
Functional Activity in the Effect of Transcranial Magnetic Stimulation Therapy for Patients with Depression: A Meta-Analysis

Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Study Characteristics
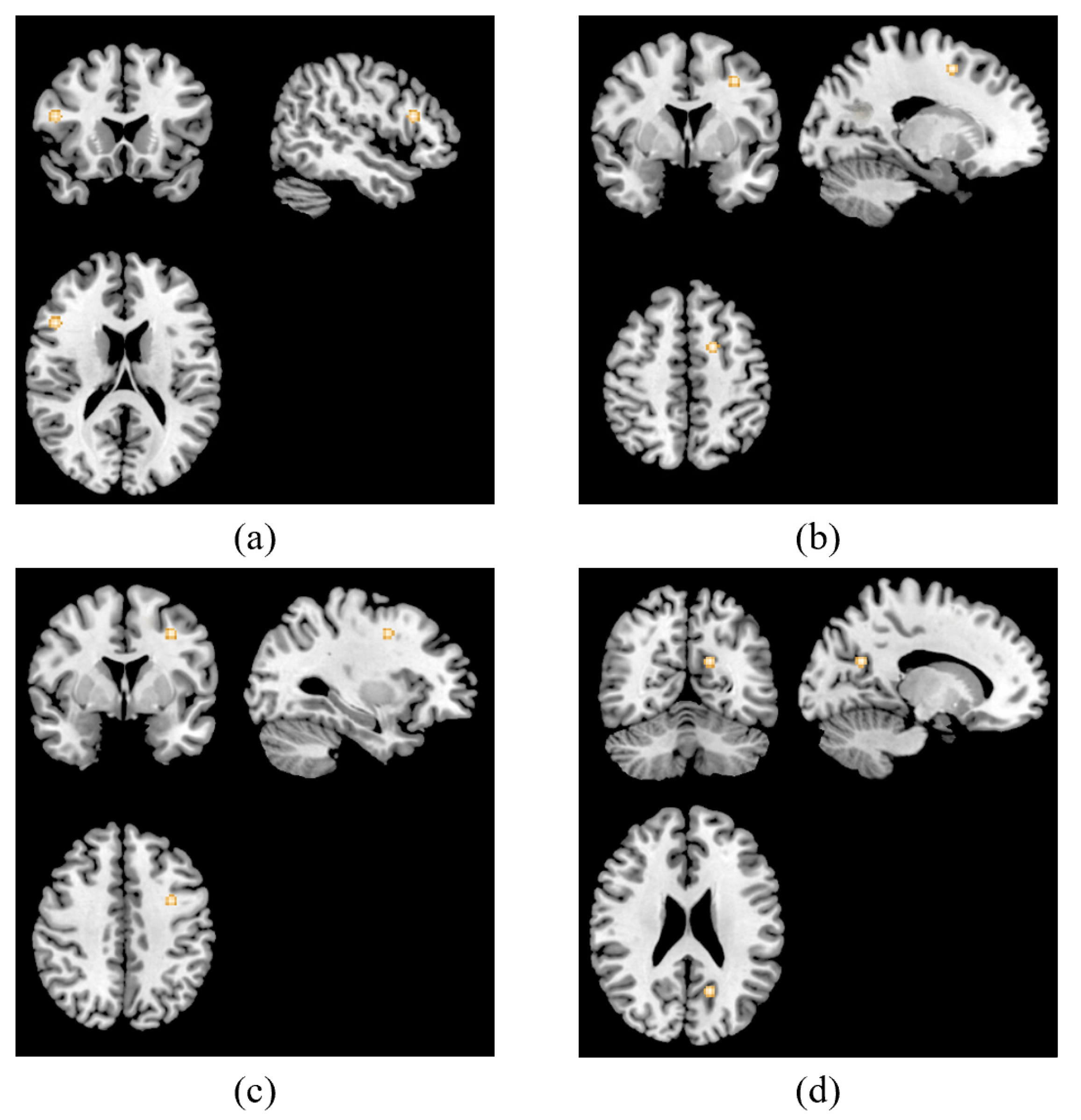
3.2. ALE Meta-Analysis Results
4. Discussion
5. Limitations and Future Directions
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Depression: Overview. Available online: https://www.who.int/health-topics/depression (accessed on 4 February 2021).
- Tibubos, A.N.; Brähler, E.; Ernst, M.; Baumgarten, C.; Wiltink, J.; Burghardt, J.; Michal, M.; Ghaemi Kerahrodi, J.; Schulz, A.; Wild, P.S.; et al. Course of depressive symptoms in men and women: Differential effects of social, psychological, behavioral and somatic predictors. Sci. Rep. 2019, 9, 18929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lépine, J.P.; Briley, M. The increasing burden of depression. Neuropsychiatr. Dis. Treat. 2011, 7, 3–7. [Google Scholar] [PubMed] [Green Version]
- Joo, J. From depression to disability. Int. Psychogeriatr. 2017, 29, 883. [Google Scholar] [CrossRef] [PubMed]
- Porter, R.J.; Douglas, K.M. Cognitive impairment in people remitted from major depression. Lancet Psychiatry 2019, 6, 799–800. [Google Scholar] [CrossRef]
- Kahl, K.G.; Stapel, B.; Frieling, H. Link between depression and cardiovascular diseases due to epigenomics and proteomics: Focus on energy metabolism. Prog. Neuropsychopharmacol. Biol. Psychiatry 2019, 89, 146–157. [Google Scholar] [CrossRef]
- Leone, M.; Kuja-Halkola, R.; Leval, A.; D’Onofrio, B.M.; Larsson, H.; Lichtenstein, P.; Bergen, S.E. Association of Youth Depression with Subsequent Somatic Diseases and Premature Death. JAMA Psychiatry 2021, 78, 302–310. [Google Scholar] [CrossRef]
- Fridell, M.; Bäckström, M.; Hesse, M.; Krantz, P.; Perrin, S.; Nyhlén, A. Prediction of psychiatric comorbidity on premature death in a cohort of patients with substance use disorders: A 42-year follow-up. BMC Psychiatry 2019, 19, 150. [Google Scholar] [CrossRef] [Green Version]
- Carpenter, L.L.; Janicak, P.G.; Aaronson, S.T.; Boyadjis, T.; Brock, D.G.; Cook, I.A.; Dunner, D.L.; Lanocha, K.; Solvason, H.B.; Demitrack, M.A. Transcranial magnetic stimulation (TMS) for major depression: A multisite, naturalistic, observational study of acute treatment outcomes in clinical practice. Depress. Anxiety 2012, 29, 587–596. [Google Scholar] [CrossRef]
- Blumberger, D.M.; Vila-Rodriguez, F.; Thorpe, K.E.; Feffer, K.; Noda, Y.; Giacobbe, P.; Knyahnytska, Y.; Kennedy, S.H.; Lam, R.W.; Daskalakis, Z.J.; et al. Effectiveness of theta burst versus high-frequency repetitive transcranial magnetic stimulation in patients with depression (THREE-D): A randomised non-inferiority trial. Lancet 2018, 391, 1683–1692. [Google Scholar] [CrossRef]
- Cantone, M.; Bramanti, A.; Lanza, G.; Pennisi, M.; Bramanti, P.; Pennisi, G.; Bella, R. Cortical Plasticity in Depression. ASN Neuro 2017, 9, 1759091417711512. [Google Scholar] [CrossRef] [Green Version]
- Di Gregorio, F.; La Porta, F.; Petrone, V.; Battaglia, S.; Orlandi, S.; Ippolito, G.; Romei, V.; Piperno, R.; Lullini, G. Accuracy of EEG Biomarkers in the Detection of Clinical Outcome in Disorders of Consciousness after Severe Acquired Brain Injury: Preliminary Results of a Pilot Study Using a Machine Learning Approach. Biomedicines 2022, 10, 1897. [Google Scholar] [CrossRef]
- Ippolito, G.; Bertaccini, R.; Tarasi, L.; Di Gregorio, F.; Trajkovic, J.; Battaglia, S.; Romei, V. The Role of Alpha Oscillations among the Main Neuropsychiatric Disorders in the Adult and Developing Human Brain: Evidence from the Last 10 Years of Research. Biomedicines 2022, 10, 3189. [Google Scholar] [CrossRef]
- Linhartová, P.; Látalová, A.; Kóša, B.; Kašpárek, T.; Schmahl, C.; Paret, C. fMRI neurofeedback in emotion regulation: A literature review. Neuroimage 2019, 193, 75–92. [Google Scholar] [CrossRef]
- Ridding, M.C.; Rothwell, J.C. Is there a future for therapeutic use of transcranial magnetic stimulation? Nat. Rev. Neurosci. 2007, 8, 559–567. [Google Scholar] [CrossRef]
- Zis, P.; Shafique, F.; Hadjivassiliou, M.; Blackburn, D.; Venneri, A.; Iliodromiti, S.; Mitsikostas, D.D.; Sarrigiannis, P.G. Safety, Tolerability, and Nocebo Phenomena During Transcranial Magnetic Stimulation: A Systematic Review and Meta-Analysis of Placebo-Controlled Clinical Trials. Neuromodulation 2020, 23, 291–300. [Google Scholar] [CrossRef] [Green Version]
- Gershon, A.A.; Dannon, P.N.; Grunhaus, L. Transcranial magnetic stimulation in the treatment of depression. Am. J. Psychiatry 2003, 160, 835–845. [Google Scholar] [CrossRef] [Green Version]
- Corlier, J.; Wilson, A.; Hunter, A.M.; Vince-Cruz, N.; Krantz, D.; Levitt, J.; Minzenberg, M.J.; Ginder, N.; Cook, I.A.; Leuchter, A.F. Changes in Functional Connectivity Predict Outcome of Repetitive Transcranial Magnetic Stimulation Treatment of Major Depressive Disorder. Cereb. Cortex. 2019, 29, 4958–4967. [Google Scholar] [CrossRef]
- Concerto, C.; Lanza, G.; Cantone, M.; Ferri, R.; Pennisi, G.; Bella, R.; Aguglia, E. Repetitive transcranial magnetic stimulation in patients with drug-resistant major depression: A six-month clinical follow-up study. Int. J. Psychiatry Clin. Pract. 2015, 19, 252–258. [Google Scholar] [CrossRef]
- Spampinato, C.; Aguglia, E.; Concerto, C.; Pennisi, M.; Lanza, G.; Bella, R.; Cantone, M.; Pennisi, G.; Kavasidis, I.; Giordano, D. Transcranial magnetic stimulation in the assessment of motor cortex excitability and treatment of drug-resistant major depression. IEEE Trans. Neural Syst. Rehabil. Eng. 2013, 21, 391–403. [Google Scholar] [CrossRef]
- Noda, Y.; Zomorrodi, R.; Vila-Rodriguez, F.; Downar, J.; Farzan, F.; Cash, R.F.H.; Rajji, T.K.; Daskalakis, Z.J.; Blumberger, D.M. Impaired neuroplasticity in the prefrontal cortex in depression indexed through paired associative stimulation. Depress. Anxiety 2018, 35, 448–456. [Google Scholar] [CrossRef]
- Biswal, B.B.; Mennes, M.; Zuo, X.N.; Gohel, S.; Kelly, C.; Smith, S.M.; Beckmann, C.F.; Adelstein, J.S.; Buckner, R.L.; Colcombe, S.; et al. Toward discovery science of human brain function. Proc. Natl. Acad. Sci. USA 2010, 107, 4734–4739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neacsiu, A.D.; Luber, B.M.; Davis, S.W.; Bernhardt, E.; Strauman, T.J.; Lisanby, S.H. On the Concurrent Use of Self-System Therapy and Functional Magnetic Resonance Imaging-Guided Transcranial Magnetic Stimulation as Treatment for Depression. J. ECT 2018, 34, 266–273. [Google Scholar] [CrossRef] [PubMed]
- Hadas, I.; Sun, Y.; Lioumis, P.; Zomorrodi, R.; Jones, B.; Voineskos, D.; Downar, J.; Fitzgerald, P.B.; Blumberger, D.M.; Daskalakis, Z.J. Association of Repetitive Transcranial Magnetic Stimulation Treatment with Subgenual Cingulate Hyperactivity in Patients with Major Depressive Disorder: A Secondary Analysis of a Randomized Clinical Trial. JAMA Netw. Open 2019, 2, e195578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eickhoff, S.B.; Bzdok, D.; Laird, A.R.; Kurth, F.; Fox, P.T. Activation likelihood estimation meta-analysis revisited. Neuroimage 2012, 59, 2349–2361. [Google Scholar] [CrossRef] [Green Version]
- Turkeltaub, P.E.; Eickhoff, S.B.; Laird, A.R.; Fox, M.; Wiener, M.; Fox, P. Minimizing within-experiment and within-group effects in Activation Likelihood Estimation meta-analyses. Hum. Brain Mapp. 2012, 33, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Eickhoff, S.B.; Laird, A.R.; Grefkes, C.; Wang, L.E.; Zilles, K.; Fox, P.T. Coordinate-based activation likelihood estimation meta-analysis of neuroimaging data: A random-effects approach based on empirical estimates of spatial uncertainty. Hum Brain Mapp. 2009, 30, 2907–2926. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Deng, Y.; Li, W.; Zhang, B. Neuroimaging in the effect of transcranial magnetic stimulation therapy for patient with depression: A protocol for a coordinate-based meta-analysis. BMJ Open 2020, 10, e038099. [Google Scholar] [CrossRef]
- Mutz, J.; Edgcumbe, D.R.; Brunoni, A.R.; Fu, C.H.Y. Efficacy and acceptability of non-invasive brain stimulation for the treatment of adult unipolar and bipolar depression: A systematic review and meta-analysis of randomised sham-controlled trials. Neurosci. Biobehav. Rev. 2018, 92, 291–303. [Google Scholar] [CrossRef] [Green Version]
- Iwabuchi, S.J.; Krishnadas, R.; Li, C.; Auer, D.P.; Radua, J.; Palaniyappan, L. Localized connectivity in depression: A meta-analysis of resting state functional imaging studies. Neurosci. Biobehav. Rev. 2015, 51, 77–86. [Google Scholar] [CrossRef]
- Sulpizio, S.; Del Maschio, N.; Fedeli, D.; Abutalebi, J. Bilingual language processing: A meta-analysis of functional neuroimaging studies. Neurosci. Biobehav. Rev. 2020, 108, 834–853. [Google Scholar] [CrossRef]
- Laird, A.R.; Robinson, J.L.; McMillan, K.M.; Tordesillas-Gutiérrez, D.; Moran, S.T.; Gonzales, S.M.; Ray, K.L.; Franklin, C.; Glahn, D.C.; Fox, P.T.; et al. Comparison of the disparity between Talairach and MNI coordinates in functional neuroimaging data: Validation of the Lancaster transform. Neuroimage 2010, 51, 677–683. [Google Scholar] [CrossRef] [Green Version]
- Fitzgerald, P.B.; Sritharan, A.; Daskalakis, Z.J.; de Castella, A.R.; Kulkarni, J.; Egan, G. A functional magnetic resonance imaging study of the effects of low frequency right prefrontal transcranial magnetic stimulation in depression. J. Clin. Psychopharmacol. 2007, 27, 488–492. [Google Scholar] [CrossRef]
- Li, X.; Nahas, Z.; Kozel, F.A.; Anderson, B.; Bohning, D.E.; George, M.S. Acute left prefrontal transcranial magnetic stimulation in depressed patients is associated with immediately increased activity in prefrontal cortical as well as subcortical regions. Biol. Psychiatry 2004, 55, 882–890. [Google Scholar] [CrossRef]
- Zheng, A.; Yu, R.; Du, W.; Liu, H.; Zhang, Z.; Xu, Z.; Xiang, Y.; Du, L. Two-week rTMS-induced neuroimaging changes measured with fMRI in depression. J. Affect Disord. 2020, 270, 15–21. [Google Scholar] [CrossRef]
- Zhou, B. Brain Functional Magnetic Resonance Imaging Study of rTMS in the Treatment of Depression. Ph.D. Thesis, Kunming Medical University, Kunming, China, 2021. Available online: http://cdmd.cnki.com.cn/Article/CDMD-10678-1021144024.htm (accessed on 28 January 2022).
- Liang, S.; Xue, K.; Wang, W.; Yu, W.; Ma, X.; Luo, S.; Zhang, J.; Sun, X.; Luo, X.; Liu, F.; et al. Altered brain function and clinical features in patients with first-episode, drug naïve major depressive disorder: A resting-state fMRI study. Psychiatry Res. Neuroimaging 2020, 303, 111134. [Google Scholar] [CrossRef]
- Liu, P.; Tu, H.; Zhang, A.; Yang, C.; Liu, Z.; Lei, L.; Wu, P.; Sun, N.; Zhang, K. Brain functional alterations in MDD patients with somatic symptoms: A resting-state fMRI study. J. Affect Disord. 2021, 295, 788–796. [Google Scholar] [CrossRef]
- Yoshino, A.; Okamoto, Y.; Kunisato, Y.; Yoshimura, S.; Jinnin, R.; Hayashi, Y.; Kobayakawa, M.; Doi, M.; Oshita, K.; Nakamura, R.; et al. Distinctive spontaneous regional neural activity in patients with somatoform pain disorder: A preliminary resting-state fMRI study. Psychiatry Res. 2014, 221, 246–248. [Google Scholar] [CrossRef]
- Ho, N.S.; Wong, M.M.; Lee, T.M. Neural connectivity of alexithymia: Specific association with major depressive disorder. J. Affect Disord. 2016, 193, 362–372. [Google Scholar] [CrossRef]
- Lee, M.; Kim, S.E.; Kim, W.S.; Han, J.; Kim, H.J.; Kim, B.S.; Kim, J.Y.; Hong, S.B.; Kim, B.G.; Lee, H.W. Cortico-cortical modulation induced by 1-Hz repetitive transcranial magnetic stimulation of the temporal cortex. J. Clin. Neurol. 2013, 9, 75–82. [Google Scholar] [CrossRef] [Green Version]
- Boccia, M.; Piccardi, L.; Guariglia, P. How treatment affects the brain: Meta-analysis evidence of neural substrates underpinning drug therapy and psychotherapy in major depression. Brain Imaging Behav. 2016, 10, 619–627. [Google Scholar] [CrossRef] [PubMed]
- Williams, R.J.; Brown, E.C.; Clark, D.L.; Pike, G.B.; Ramasubbu, R. Early post-treatment blood oxygenation level-dependent responses to emotion processing associated with clinical response to pharmacological treatment in major depressive disorder. Brain Behav. 2021, 11, e2287. [Google Scholar] [CrossRef] [PubMed]
- Broyd, S.J.; Demanuele, C.; Debener, S.; Helps, S.K.; James, C.J.; Sonuga-Barke, E.J. Default-mode brain dysfunction in mental disorders: A systematic review. Neurosci. Biobehav. Rev. 2009, 33, 279–296. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Q.; Swati, Z.N.K.; Metmer, H.; Sang, X.; Lu, J. Investigating executive control network and default mode network dysfunction in major depressive disorder. Neurosci. Lett. 2019, 701, 154–161. [Google Scholar] [CrossRef]
- Rolls, E.T. The cingulate cortex and limbic systems for emotion, action, and memory. Brain Struct. Funct. 2019, 224, 3001–3018. [Google Scholar] [CrossRef] [Green Version]
- Cheng, W.; Rolls, E.T.; Qiu, J.; Xie, X.; Wei, D.; Huang, C.C.; Yang, A.C.; Tsai, S.J.; Li, Q.; Meng, J.; et al. Increased functional connectivity of the posterior cingulate cortex with the lateral orbitofrontal cortex in depression. Transl. Psychiatry 2018, 8, 90. [Google Scholar] [CrossRef] [Green Version]
- Monkul, E.S.; Silva, L.A.; Narayana, S.; Peluso, M.A.; Zamarripa, F.; Nery, F.G.; Najt, P.; Li, J.; Lancaster, J.L.; Fox, P.T.; et al. Abnormal resting state corticolimbic blood flow in depressed unmedicated patients with major depression: A (15)O-H(2)O PET study. Hum. Brain Mapp. 2012, 33, 272–279. [Google Scholar] [CrossRef] [Green Version]
- Zhong, S.; Chen, G.; Zhao, L.; Jia, Y.; Chen, F.; Qi, Z.; Huang, L.; Wang, Y. Correlation between Intrinsic Brain Activity and Thyroid-Stimulating Hormone Level in Unmedicated Bipolar II Depression. Neuroendocrinology 2019, 108, 232–243. [Google Scholar] [CrossRef]
- Mayberg, H.S.; Brannan, S.K.; Tekell, J.L.; Silva, J.A.; Mahurin, R.K.; McGinnis, S.; Jerabek, P.A. Regional metabolic effects of fluoxetine in major depression: Serial changes and relationship to clinical response. Biol. Psychiatry 2000, 48, 830–843. [Google Scholar] [CrossRef]
- Mayberg, H.S.; Lozano, A.M.; Voon, V.; McNeely, H.E.; Seminowicz, D.; Hamani, C.; Schwalb, J.M.; Kennedy, S.H. Deep brain stimulation for treatment-resistant depression. Neuron 2005, 45, 651–660. [Google Scholar] [CrossRef] [Green Version]
- Teneback, C.C.; Nahas, Z.; Speer, A.M.; Molloy, M.; Stallings, L.E.; Spicer, K.M.; Risch, S.C.; George, M.S. Changes in prefrontal cortex and paralimbic activity in depression following two weeks of daily left prefrontal TMS. J. Neuropsychiatry Clin. Neurosci. 1999, 11, 426–435. [Google Scholar] [CrossRef]
- Belden, A.C.; Pagliaccio, D.; Murphy, E.R.; Luby, J.L.; Barch, D.M. Neural Activation During Cognitive Emotion Regulation in Previously Depressed Compared to Healthy Children: Evidence of Specific Alterations. J. Am. Acad. Child. Adolesc. Psychiatry 2015, 54, 771–781. [Google Scholar] [CrossRef] [Green Version]
- Guo, W.B.; Liu, F.; Xue, Z.M.; Xu, X.J.; Wu, R.R.; Ma, C.Q.; Wooderson, S.C.; Tan, C.L.; Sun, X.L.; Chen, J.D.; et al. Alterations of the amplitude of low-frequency fluctuations in treatment-resistant and treatment-response depression: A resting-state fMRI study. Prog. Neuropsychopharmacol. Biol. Psychiatry 2012, 37, 153–160. [Google Scholar] [CrossRef]
- Huang, M.; Lu, S.; Yu, L.; Li, L.; Zhang, P.; Hu, J.; Zhou, W.; Hu, S.; Wei, N.; Huang, J.; et al. Altered fractional amplitude of low frequency fluctuation associated with cognitive dysfunction in first-episode drug-naïve major depressive disorder patients. BMC Psychiatry 2017, 17, 11. [Google Scholar] [CrossRef] [Green Version]
- Kaichi, Y.; Okada, G.; Takamura, M.; Toki, S.; Akiyama, Y.; Higaki, T.; Matsubara, Y.; Okamoto, Y.; Yamawaki, S.; Awai, K. Changes in the regional cerebral blood flow detected by arterial spin labeling after 6-week escitalopram treatment for major depressive disorder. J. Affect Disord. 2016, 194, 135–143. [Google Scholar] [CrossRef] [Green Version]
- Koechlin, E.; Hyafil, A. Anterior prefrontal function and the limits of human decision-making. Science 2007, 318, 594–598. [Google Scholar] [CrossRef]
- Zhang, K.; Liu, Z.; Cao, X.; Yang, C.; Xu, Y.; Xu, T.; Xu, C.; Yang, Z. Amplitude of low-frequency fluctuations in first-episode, drug-naïve depressive patients: A 5-year retrospective study. PLoS ONE 2017, 12, e0174564. [Google Scholar] [CrossRef] [Green Version]
- Yang, C.; Zhang, A.; Jia, A.; Ma, J.X.; Sun, N.; Wang, Y.; Li, X.; Liu, Z.; Liu, S.; Xu, Y.; et al. Identify abnormalities in resting-state brain function between first-episode, drug-naive major depressive disorder and remitted individuals: A 3-year retrospective study. Neuroreport 2018, 29, 907–916. [Google Scholar] [CrossRef]
- Ogura, A.; Morinobu, S.; Kawakatsu, S.; Totsuka, S.; Komatani, A. Changes in regional brain activity in major depression after successful treatment with antidepressant drugs. Acta Psychiatr. Scand. 1998, 98, 54–59. [Google Scholar] [CrossRef]
- Lemogne, C.; le Bastard, G.; Mayberg, H.; Volle, E.; Bergouignan, L.; Lehéricy, S.; Allilaire, J.F.; Fossati, P. In search of the depressive self: Extended medial prefrontal network during self-referential processing in major depression. Soc. Cogn. Affect Neurosci. 2009, 4, 305–312. [Google Scholar] [CrossRef] [Green Version]
- Colich, N.L.; Ho, T.C.; Foland-Ross, L.C.; Eggleston, C.; Ordaz, S.J.; Singh, M.K.; Gotlib, I.H. Hyperactivation in Cognitive Control and Visual Attention Brain Regions During Emotional Interference in Adolescent Depression. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2017, 2, 388–395. [Google Scholar] [CrossRef] [PubMed]
- Geng, J.; Yan, R.; Shi, J.; Chen, Y.; Mo, Z.; Shao, J.; Wang, X.; Yao, Z.; Lu, Q. Altered regional homogeneity in patients with somatic depression: A resting-state fMRI study. J. Affect Disord. 2019, 246, 498–505. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Liu, S.; Jiang, X.; Yu, H.; Ding, S.; Lu, Y.; Li, W.; Zhang, H.; Liu, B.; Cui, Y.; et al. Common and Specific Functional Activity Features in Schizophrenia, Major Depressive Disorder, and Bipolar Disorder. Front. Psychiatry 2019, 10, 52. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Tang, Y.; Zhu, Y.; Li, Y.; Tong, S. Study of functional brain homogeneity in female patients with major depressive disorder. In Proceedings of the 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; pp. 2562–2565. [Google Scholar]
- Peng, H.; Zheng, H.; Li, L.; Liu, J.; Zhang, Y.; Shan, B.; Zhang, L.; Yin, Y.; Liu, J.; Li, W.; et al. High-frequency rTMS treatment increases white matter FA in the left middle frontal gyrus in young patients with treatment-resistant depression. J. Affect Disord. 2012, 136, 249–257. [Google Scholar] [CrossRef] [PubMed]
- Choi, K.M.; Choi, S.H.; Lee, S.M.; Jang, K.I.; Chae, J.H. Three Weeks of rTMS Treatment Maintains Clinical Improvement but Not Electrophysiological Changes in Patients With Depression: A 6-Week Follow-Up Pilot Study. Front. Psychiatry 2019, 10, 351. [Google Scholar] [CrossRef] [Green Version]
- Choi, K.M.; Jang, K.M.; Jang, K.I.; Um, Y.H.; Kim, M.S.; Kim, D.W.; Shin, D.; Chae, J.H. The effects of 3 weeks of rTMS treatment on P200 amplitude in patients with depression. Neurosci. Lett. 2014, 577, 22–27. [Google Scholar] [CrossRef]
- Cullen, K.R.; Klimes-Dougan, B.; Vu, D.P.; Westlund Schreiner, M.; Mueller, B.A.; Eberly, L.E.; Camchong, J.; Westervelt, A.; Lim, K.O. Neural Correlates of Antidepressant Treatment Response in Adolescents with Major Depressive Disorder. J Child Adolesc. Psychopharmacol. 2016, 26, 705–712. [Google Scholar] [CrossRef] [Green Version]
- Lai, C.H. Patterns of cortico-limbic activations during visual processing of sad faces in depression patients: A coordinate-based meta-analysis. J. Neuropsychiatry Clin. Neurosci. 2014, 26, 34–43. [Google Scholar] [CrossRef]
- Japee, S.; Holiday, K.; Satyshur, M.D.; Mukai, I.; Ungerleider, L.G. A role of right middle frontal gyrus in reorienting of attention: A case study. Front. Syst. Neurosci. 2015, 9, 23. [Google Scholar] [CrossRef] [Green Version]
- Beevers, C.G.; Clasen, P.C.; Enock, P.M.; Schnyer, D.M. Attention bias modification for major depressive disorder: Effects on attention bias, resting state connectivity, and symptom change. J. Abnorm. Psychol. 2015, 124, 463–475. [Google Scholar] [CrossRef]
- Disner, S.G.; Shumake, J.D.; Beevers, C.G. Self-referential schemas and attentional bias predict severity and naturalistic course of depression symptoms. Cogn. Emot. 2017, 31, 632–644. [Google Scholar] [CrossRef]
- Liu, X.; Hou, Z.; Yin, Y.; Xie, C.; Zhang, H.; Zhang, H.; Zhang, Z.; Yuan, Y. CACNA1C Gene rs11832738 Polymorphism Influences Depression Severity by Modulating Spontaneous Activity in the Right Middle Frontal Gyrus in Patients with Major Depressive Disorder. Front. Psychiatry 2020, 11, 73. [Google Scholar] [CrossRef]
- Yu, Y.; Li, Z.; Lin, Y.; Yu, J.; Peng, G.; Zhang, K.; Jia, X.; Luo, B. Depression Affects Intrinsic Brain Activity in Patients with Mild Cognitive Impairment. Front. Neurosci. 2019, 13, 1333. [Google Scholar] [CrossRef] [Green Version]
- Zuo, X.N.; Di Martino, A.; Kelly, C.; Shehzad, Z.E.; Gee, D.G.; Klein, D.F.; Castellanos, F.X.; Biswal, B.B.; Milham, M.P. The oscillating brain: Complex and reliable. Neuroimage 2010, 49, 1432–1445. [Google Scholar] [CrossRef] [Green Version]
- Yang, H.; Long, X.Y.; Yang, Y.; Yan, H.; Zhu, C.Z.; Zhou, X.P.; Zang, Y.F.; Gong, Q.Y. Amplitude of low frequency fluctuation within visual areas revealed by resting-state functional MRI. Neuroimage 2007, 36, 144–152. [Google Scholar] [CrossRef]
- Wang, Y.; Xu, C.; Cao, X.; Gao, Q.; Li, J.; Liu, Z.; Sun, N.; Ren, Y.; Zhang, K. Effects of an antidepressant on neural correlates of emotional processing in patients with major depression. Neurosci. Lett. 2012, 527, 55–59. [Google Scholar] [CrossRef]
- Sokoloff, L. Local cerebral energy metabolism: Its relationships to local functional activity and blood flow. Bull. Schweiz. Akad. Med. Wiss. 1978, 36, 171–197. [Google Scholar]
- Wu, B.; Li, X.; Zhou, J.; Zhang, M.; Long, Q. Altered Whole-Brain Functional Networks in Drug-Naïve, First-Episode Adolescents with Major Depression Disorder. J. Magn. Reason. Imaging 2020, 52, 1790–1798. [Google Scholar] [CrossRef]
- Li, Q.; Zhao, Y.; Chen, Z.; Long, J.; Dai, J.; Huang, X.; Lui, S.; Radua, J.; Vieta, E.; Kemp, G.J.; et al. Meta-analysis of cortical thickness abnormalities in medication-free patients with major depressive disorder. Neuropsychopharmacology 2020, 45, 703–712. [Google Scholar] [CrossRef]
- Li, X.; Chu, M.Y.; Lv, Q.Y.; Hu, H.X.; Li, Z.; Yi, Z.H.; Wang, J.H.; Zhang, J.Y.; Lui, S.S.Y.; Cheung, E.F.C.; et al. The remediation effects of working memory training in schizophrenia patients with prominent negative symptoms. Cogn. Neuropsychiatry 2019, 24, 434–453. [Google Scholar] [CrossRef]
- Belujon, P.; Grace, A.A. Dopamine System Dysregulation in Major Depressive Disorders. Int. J. Neuropsychopharmacol. 2017, 20, 1036–1046. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fitzgerald, P.B.; Laird, A.R.; Maller, J.; Daskalakis, Z.J. A meta-analytic study of changes in brain activation in depression. Hum. Brain Mapp. 2008, 29, 683–695. [Google Scholar] [CrossRef] [PubMed]
- Mayberg, H.S.; Silva, J.A.; Brannan, S.K.; Tekell, J.L.; Mahurin, R.K.; McGinnis, S.; Jerabek, P.A. The functional neuroanatomy of the placebo effect. Am. J. Psychiatry 2002, 159, 728–737. [Google Scholar] [CrossRef] [PubMed]
- Goldapple, K.; Segal, Z.; Garson, C.; Lau, M.; Bieling, P.; Kennedy, S.; Mayberg, H. Modulation of cortical-limbic pathways in major depression: Treatment-specific effects of cognitive behavior therapy. Arch. Gen. Psychiatry 2004, 61, 34–41. [Google Scholar] [CrossRef] [Green Version]
- Lochmann, D.; Richardson, T. Selective Serotonin Reuptake Inhibitors. Handb. Exp. Pharmacol. 2019, 250, 135–144. [Google Scholar]
- Poh, E.Z.; Hahne, D.; Moretti, J.; Harvey, A.R.; Clarke, M.W.; Rodger, J. Simultaneous quantification of dopamine, serotonin, their metabolites and amino acids by LC-MS/MS in mouse brain following repetitive transcranial magnetic stimulation. Neurochem. Int. 2019, 131, 104546. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year) | Quality Score | Severity of Depression | Sample Size (F:M) | Mean Age | Combination Therapy | Duration of Disease | Assessment Scale | Mean Score 1 | Mean Score 2 | Respondents:Non-Respondents | Activity Altered Region |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Xingbao Li [35] (2004) | 15 | MDD | 14(9:5) | 38.2 | psychiatric medication | mean: 14.1 years | HRSD | 30.9 | N.A. | 4:10 | MFG_L, HIP_L, THA_B, PUT_B, PL_B,INS_B, ORB_R, TPOmid_L, and PFC_R |
| Paul B. Fitzgerald [34] (2007) | 14 | TRD | 11(5:6) | 39.6 | psychiatric medication | mean: 5.2 years | MADRS | 33.3 | 25.6 | 6:5 | MFG_B; PCUN_L |
| TRD | 15(8:7) | 42.4 | psychiatric medication | mean: 5.2 years | MADRS | 34.5 | 24.8 | 9:6 | PCUN_L; PreCG_L; PoSFG_L;MFG_L; IFG_R | ||
| Neacsiu AD [23] (2018) | 14 | MDD | 5(2:3) | 53.8 | self-system therapy | at least 8 weeks | HRSD | 19.8 | 3.4 | 5:0 | ORB_R; HIP_R |
| Anhai Zheng [36] (2020) | 17 | MDD | 27(19:8) | 41.2 | none | N.A. | HAMD | 23.9 | 14.7 | N.A. | SFG_L; LPCdor_L |
| Zhou Biao [37] (2022) | 16 | Mild to moderate depression | 20(16:4) | 30.2 | psychiatric medication | N.A. | HAMD | 18.1 | 4.9 | N.A. | PCG_R; PoCG_R |
| Region | Cluster Size (mm3) | MNI Coordinates | ALE | p Value | Z Score | BA | ||
|---|---|---|---|---|---|---|---|---|
| x | y | z | max. | |||||
| Main analysis | ||||||||
| Right precentral gyrus | 352 | 60 | 0 | 20 | 0.0078 | 0.0000201 | 4.106458 | 6 |
| Right posterior cingulate | 288 | 21 | 57 | 12 | 0.0075 | 0.0000379 | 3.957385 | 30 |
| Left inferior frontal gyrus | 288 | −46 | 12 | 22 | 0.0073 | 0.0000710 | 3.804717 | 9 |
| Left middle frontal gyrus | 288 | −16 | −18 | 62 | 0.0073 | 0.0000710 | 3.804717 | 6 |
| Resting-state studies | ||||||||
| Right precentral gyrus | 480 | 60 | 0 | 21 | 0.0078 | 0.0000137 | 4.194821 | 6 |
| Right posterior cingulate | 448 | 21 | 57 | 12 | 0.0075 | 0.0000299 | 4.013568 | 30 |
| Left inferior frontal gyrus | 448 | −46 | 12 | 22 | 0.0073 | 0.0000611 | 3.842041 | 9 |
| Left superior frontal gyrus | 448 | −15 | −18 | 63 | 0.0073 | 0.0000610 | 3.842041 | 6 |
| Task-related studies | ||||||||
| Right middle frontal gyrus | 384 | 48 | 20 | 18 | 0.0063 | 0.0000038 | 4.476675 | 46 |
| Left sub-gyrus | 360 | −18 | 4 | 52 | 0.0062 | 0.0000156 | 4.165172 | 6 |
| Left middle frontal gyrus | 352 | −32 | 2 | 42 | 0.0060 | 0.0000238 | 4.066664 | 6 |
| Left posterior cingulate | 344 | −16 | −60 | 24 | 0.0062 | 0.0000156 | 4.165172 | 31 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Deng, Y.; Li, W.; Zhang, B. Functional Activity in the Effect of Transcranial Magnetic Stimulation Therapy for Patients with Depression: A Meta-Analysis. J. Pers. Med. 2023, 13, 405. https://doi.org/10.3390/jpm13030405
Deng Y, Li W, Zhang B. Functional Activity in the Effect of Transcranial Magnetic Stimulation Therapy for Patients with Depression: A Meta-Analysis. Journal of Personalized Medicine. 2023; 13(3):405. https://doi.org/10.3390/jpm13030405
Chicago/Turabian StyleDeng, Yongyan, Wenyue Li, and Bin Zhang. 2023. "Functional Activity in the Effect of Transcranial Magnetic Stimulation Therapy for Patients with Depression: A Meta-Analysis" Journal of Personalized Medicine 13, no. 3: 405. https://doi.org/10.3390/jpm13030405