
Long-Term Outcomes of Liver Transplantation for the Management of Neuroendocrine Neoplasms: A Systematic Review

Abstract
:1. Introduction
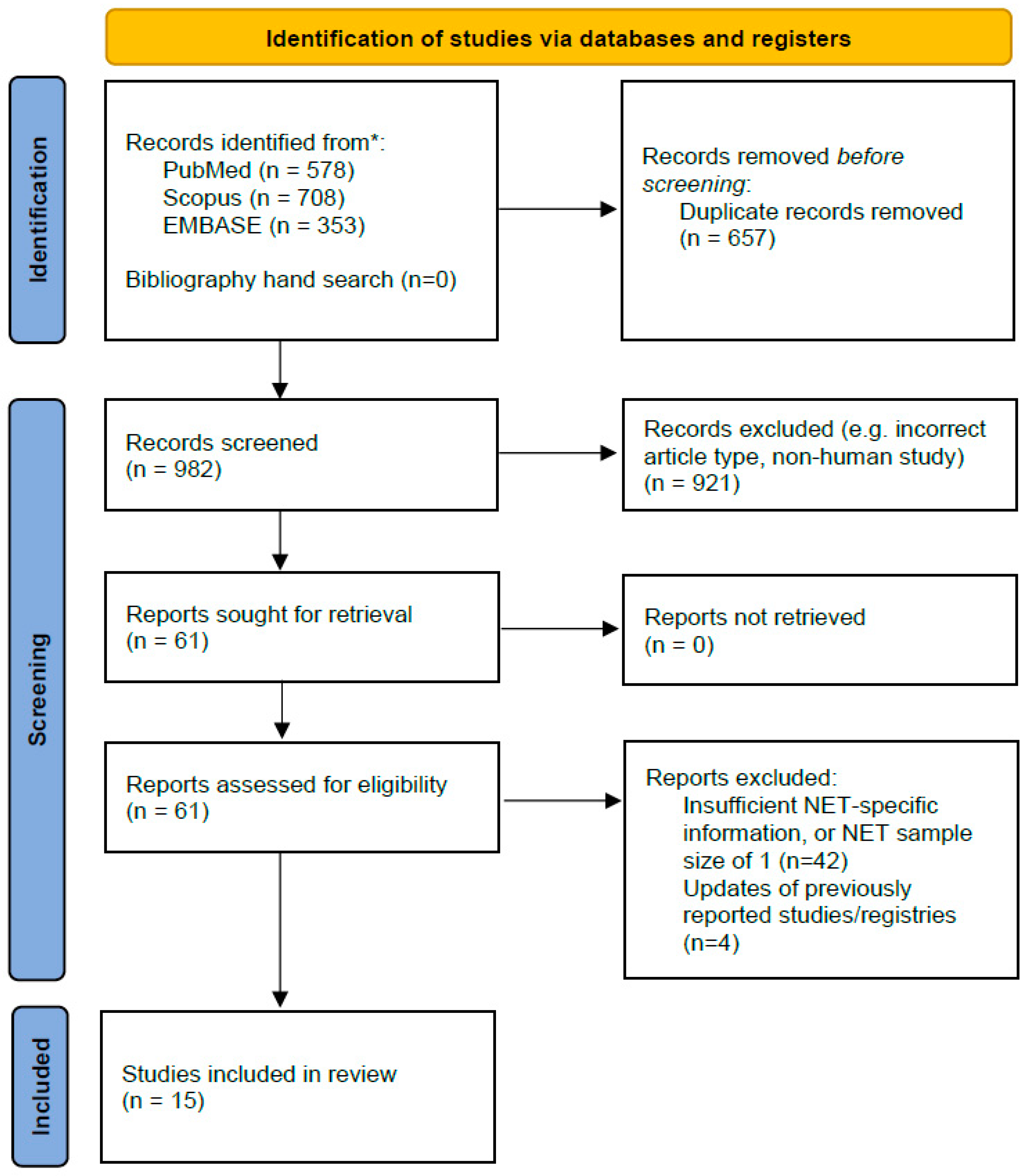
2. Materials and Methods
2.1. Protocol Registration and Study Conduct
- Population: patients with advanced neuroendocrine neoplasms (liver metastases);
- Intervention: liver transplantation, either alone (orthotopic) or part of a multivisceral graft;
- Comparison: other, non-transplant treatment strategies (data availability permitting);
- Outcome: overall and disease-free survival at 1-, 3-, 5-, 10-, and 10+ years.
2.2. Search Strategy, Data Sources and Inclusion
2.3. Data Extraction and Summary
2.4. Synthesis and Meta-Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Dasari, A.; Shen, C.; Halperin, D.; Zhao, B.; Zhou, S.; Xu, Y.; Shih, T.; Yao, J.C. Trends in the Incidence, Prevalence, and Survival Outcomes in Patients With Neuroendocrine Tumors in the United States. JAMA Oncol. 2017, 3, 1335. [Google Scholar] [CrossRef]
- Frilling, A.; Clift, A.K. Therapeutic strategies for neuroendocrine liver metastases. Cancer 2015, 121, 1172–1186. [Google Scholar] [CrossRef] [PubMed]
- Miller, H.C.; Drymousis, P.; Flora, R.; Goldin, R.; Spalding, D.; Frilling, A. Role of Ki-67 proliferation index in the assessment of patients with neuroendocrine neoplasias regarding the stage of disease. World J. Surg. 2014, 38, 1353–1361. [Google Scholar] [CrossRef] [PubMed]
- Riihimäki, M.; Hemminki, A.; Sundquist, K.; Sundquist, J.; Hemminki, K. The epidemiology of metastases in neuroendocrine tumors. Int. J. Cancer 2016, 139, 2679–2686. [Google Scholar] [CrossRef] [PubMed]
- Panzuto, F.; Boninsegna, L.; Fazio, N.; Campana, D.; Brizzi, M.P.; Capurso, G.; Scarpa, A.; De Braud, F.; Dogliotti, L.; Tomassetti, P.; et al. Metastatic and locally advanced pancreatic endocrine carcinomas: Analysis of factors associated with disease progression. J. Clin. Oncol. 2011, 29, 2372–2377. [Google Scholar] [CrossRef] [PubMed]
- Pavel, M.; Öberg, K.; Falconi, M.; Krenning, E.P.; Sundin, A.; Perren, A.; Berruti, A. Gastroenteropancreatic neuroendocrine neoplasms: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020, 31, 844–860. [Google Scholar] [CrossRef]
- Elias, D.; Lefevre, J.H.; Duvillard, P.; Goéré, D.; Dromain, C.; Dumont, F.; Baudin, E. Hepatic metastases from neuroendocrine tumors with a ‘thin slice’ pathological examination: They are many more than you think. Ann. Surg. 2010, 251, 307–310. [Google Scholar] [CrossRef]
- Frilling, A.; Modlin, I.M.; Kidd, M.; Russell, C.; Breitenstein, S.; Salem, R.; Kwekkeboom, D.; Lau, W.-Y.; Klersy, C.; Vilgrain, V.; et al. Recommendations for management of patients with neuroendocrine liver metastases. Lancet Oncol. 2014, 15, e8–e21. [Google Scholar] [CrossRef]
- Caplin, M.E.; Pavel, M.; Ćwikła, J.B.; Phan, A.T.; Raderer, M.; Sedláčková, E.; Cadiot, G.; Wolin, E.M.; Capdevila, J.; Wall, L.; et al. Lanreotide in metastatic enteropancreatic neuroendocrine tumors. N. Engl. J. Med. 2014, 371, 224–233. [Google Scholar] [CrossRef]
- Strosberg, J.; El-Haddad, G.; Wolin, E.; Hendifar, A.; Yao, J.; Chasen, B.; Mittra, E.; Kunz, P.L.; Kulke, M.H.; Jacene, H.; et al. Phase 3 Trial of 177Lu-Dotatate for Midgut Neuroendocrine Tumors. N. Engl. J. Med. 2017, 376, 125–135. [Google Scholar] [CrossRef]
- Raymond, E.; Dahan, L.; Raoul, J.-L.; Bang, Y.-J.; Borbath, I.; Lombard-Bohas, C.; Valle, J.; Metrakos, P.; Smith, D.; Vinik, A.; et al. Sunitinib malate for the treatment of pancreatic neuroendocrine tumors. N. Engl. J. Med. 2011, 364, 501–513. [Google Scholar] [CrossRef] [PubMed]
- Yao, J.C.; Lombard-Bohas, C.; Baudin, E.; Kvols, L.K.; Rougier, P.; Ruszniewski, P.; Hoosen, S.; Peter, J.S.; Haas, T.; Lebwohl, D.; et al. Daily oral everolimus activity in patients with metastatic pancreatic neuroendocrine tumors after failure of cytotoxic chemotherapy: A phase II trial. J. Clin. Oncol. 2010, 28, 69–76. [Google Scholar] [CrossRef]
- Braat, A.J.A.T.; Bruijnen, R.C.G.; van Rooij, R.; Braat, M.N.; Wessels, F.J.; van Leeuwaarde, R.S.; van Treijen, M.J.C.; de Herder, W.W.; Hofland, J.; Tesselaar, M.E.T.; et al. Additional holmium-166 radioembolisation after lutetium-177-dotatate in patients with neuroendocrine tumour liver metastases (HEPAR PLuS): A single-centre, single-arm, open-label, phase 2 study. Lancet Oncol. 2020, 21, 561–570. [Google Scholar] [CrossRef] [PubMed]
- Strosberg, J.R.; Caplin, M.E.; Kunz, P.L.; Ruszniewski, P.B.; Bodei, L.; Hendifar, A.; Mittra, E.; Wolin, E.M.; Yao, J.C.; Pavel, M.E.; et al. 177Lu-Dotatate plus long-acting octreotide versus high-dose long-acting octreotide in patients with midgut neuroendocrine tumours (NETTER-1): Final overall survival and long-term safety results from an open-label, randomised, controlled, phase 3 trial. Lancet Oncol. 2021, 22, 1752–1763. [Google Scholar] [CrossRef]
- Frilling, A.; Clift, A.K. Surgical approaches to the management of neuroendocrine liver metastases. Endocr. Metab. Clin. North. Am. 2018, 47, 627–643. [Google Scholar] [CrossRef] [PubMed]
- Saxena, A.; Chua, T.C.; Perera, M.; Chu, F.; Morris, D.L. Surgical resection of hepatic metastases from neuroendocrine neoplasms: A systematic review. Surg. Oncol. 2012, 21, e131–e141. [Google Scholar] [CrossRef]
- Moris, D.; Tsilimigras, D.I.; Ntanasis-Stathopoulos, I.; Beal, E.W.; Felekouras, E.; Vernadakis, S.; Fung, J.J.; Pawlik, T.M. Liver transplantation in patients with liver metastases from neuroendocrine tumors: A systematic review. Surgery 2017, 162, 525–536. [Google Scholar] [CrossRef]
- Mrzljak, A.; Kocman, B.; Skrtic, A.; Furac, I.; Popic, J.; Franusic, L.; Zunec, R.; Mayer, D.; Mikulic, D. Liver re-transplantation for donor-derived neuroendocrine tumor: A case report. World J. Clin. Cases 2019, 7, 2794–2801. [Google Scholar] [CrossRef]
- Nikeghbalian, S.; Eshraghian, A.; Kazemi, K.; Shamsaeefar, A.; Hosseinzadeh, M.; Geramizadeh, B.; Malek-Hosseini, S.A. Liver Transplantation for High-Grade Primary Hepatic Neuroendocrine Tumor with Diffuse Liver Metastasis. J. Gastrointest. Cancer 2020, 51, 304–306. [Google Scholar] [CrossRef]
- Sher, L.S.; Levi, D.M.; Wecsler, J.S.; Lo, M.; Petrovic, L.M.; Groshen, S.; Ji, L.; Uso, T.D.; Tector, A.J.; Hamilton, A.S.; et al. Liver transplantation for metastatic neuroendocrine tumors: Outcomes and prognostic variables. J. Surg. Oncol. 2015, 112, 125–132. [Google Scholar] [CrossRef]
- Mangus, R.S.; Tector, A.J.; Kubal, C.A.; Fridell, J.A.; Vianna, R.M. Multivisceral transplantation: Expanding indications and improving outcomes. J. Gastrointest. Surg. 2013, 17, 179–186, discussion 186–187. [Google Scholar] [CrossRef] [PubMed]
- Fan, S.T.; Le Treut, Y.P.; Mazzaferro, V.; Burroughs, A.K.; Olausson, M.; Breitenstein, S.; Frilling, A. Liver transplantation for neuroendocrine tumour liver metastases. HPB 2015, 17, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Olausson, M.; Friman, S.; Herlenius, G.; Cahlin, C.; Nilsson, O.; Jansson, S.; Wängberg, B.; Ahlman, H. Orthotopic liver or multivisceral transplantation as treatment of metastatic neuroendocrine tumors. Liver Transpl. 2007, 13, 327–333. [Google Scholar] [CrossRef]
- Le Treut, Y.P.; Grégoire, E.; Klempnauer, J.; Belghiti, J.; Jouve, E.; Lerut, J.; Castaing, D.; Soubrane, O.; Boillot, O.; Mantion, G.; et al. Liver transplantation for neuroendocrine tumors in Europe-results and trends in patient selection: A 213-case European liver transplant registry study. Ann. Surg. 2013, 257, 807–815. [Google Scholar] [CrossRef]
- Gedaly, R.; Daily, M.F.; Davenport, D.; McHugh, P.P.; Koch, A.; Angulo, P.; Hundley, J.C. Liver transplantation for the treatment of liver metastases from neuroendocrine tumors: An analysis of the UNOS database. Arch. Surg. 2011, 146, 953–958. [Google Scholar] [CrossRef]
- Vilchez, V.; Gedaly, R. Liver transplantation for the treatment of neuroendocrine liver metastases. Best. Pract. Res. Clin. Endocrinol. Metab. 2016, 30, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, N.T.T.; Harring, T.R.; Goss, J.A.; O’Mahony, C.A. Neuroendocrine Liver Metastases and Orthotopic Liver Transplantation: The US Experience. Int. J. Hepatol. 2011, 2011, 742890. [Google Scholar] [CrossRef]
- Mazzaferro, V.; Sposito, C.; Coppa, J.; Miceli, R.; Bhoori, S.; Bongini, M.; Camerini, T.; Milione, M.; Regalia, E.; Spreafico, C.; et al. The Long-Term Benefit of Liver Transplantation for Hepatic Metastases From Neuroendocrine Tumors. Am. J. Transplant. 2016, 16, 2892–2902. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Dousset, B.; Saint-Marc, O.; Pitre, J.; Soubrane, O.; Houssin, D.; Chapuis, Y. Metastatic endocrine tumors: Medical treatment, surgical resection, or liver transplantation. World J. Surg. 1996, 20, 908–915. [Google Scholar] [CrossRef]
- Le Treut, Y.P.; Delpero, J.R.; Dousset, B.; Cherqui, D.; Segol, P.; Mantion, G.; Hannoun, L.; Benhamou, G.; Launois, B.; Boillot, O.; et al. Results of liver transplantation in the treatment of metastatic neuroendocrine tumors. A 31-case French multicentric report. Ann. Surg. 1997, 225, 355–364. [Google Scholar] [CrossRef] [PubMed]
- Le Treut, Y.P.; Grégoire, E.; Belghiti, J.; Boillot, O.; Soubrane, O.; Mantion, G.; Cherqui, D.; Castaing, D.; Ruszniewski, P.; Wolf, P.; et al. Predictors of long-term survival after liver transplantation for metastatic endocrine tumors: An 85-case French multicentric report. Am. J. Transplant. 2008, 8, 1205–1213. [Google Scholar] [CrossRef] [PubMed]
- Routley, D.; Ramage, J.K.; McPeake, J.; Tan, K.-C.; Williams, R. Orthotopic liver transplantation in the treatment of metastatic neuroendocrine tumors of the liver. Liver Transpl. Surg. 1995, 1, 118–121. [Google Scholar] [CrossRef] [PubMed]
- Rosenau, J.; Bahr, M.J.; Wasielewski, V.; Mengel, M.; Schmidt, H.H.J.; Nashan, B.; Lang, H.; Klempnauer, J.; Manns, M.P.; Boeker, K.H.W. Ki67, E-cadherin, and p53 as prognostic indicators of long-term outcome after liver transplantation for metastatic neuroendocrine tumors. Transplantation 2002, 73, 386–394. [Google Scholar] [CrossRef]
- Florman, S.; Toure, B.; Kim, L.; Gondolesi, G.; Roayaie, S.; Krieger, N.; Fishbein, T.; Emre, S.; Miller, C.; Schwartz, M. Liver transplantation for neuroendocrine tumors. J. Gastrointest. Surg. 2004, 8, 208–212. [Google Scholar] [CrossRef]
- van Vilsteren, F.G.; Baskin-Bey, E.S.; Nagorney, D.M.; Sanderson, S.O.; Kremers, W.K.; Rosen, C.B.; Gores, G.J.; Hobday, T.J. Liver transplantation for gastroenteropancreatic neuroendocrine cancers: Defining selection criteria to improve survival. Liver Transpl. 2006, 12, 448–456. [Google Scholar] [CrossRef]
- Marín, C.; Robles, R.; Fernández, J.; Bueno, F.; Ramírez, P.; Miras, M.; Parrilla, P. Role of liver transplantation in the management of unresectable neuroendocrine liver metastases. Transplant. Proc. 2007, 39, 2302–2303. [Google Scholar] [CrossRef]
- Dhupar, R.; De Vera, M.E.; Marsh, J.W.; Fontes, P.A.; Steel, J.L.; Zeh, H.J.; Gamblin, T.C. Simultaneous pancreatectomy and liver transplantation: A single-institution experience. HPB 2009, 11, 242–246. [Google Scholar] [CrossRef]
- Frilling, A.; Li, J.; Malamutmann, E.; Schmid, K.-W.K.-W.; Bockisch, A.; Broelsch, C.E. Treatment of liver metastases from neuroendocrine tumours in relation to the extent of hepatic disease. Br. J. Surg. 2009, 96, 175–184. [Google Scholar] [CrossRef]
- Bonaccorsi-Riani, E.; Apestegui, C.; Jouret-Mourin, A.; Sempoux, C.; Goffette, P.; Ciccarelli, O.; Borbath, I.; Hubert, C.; Gigot, J.F.; Hassoun, Z.; et al. Liver transplantation and neuroendocrine tumors: Lessons from a single centre experience and from the literature review. Transpl. Int. 2010, 23, 668–678. [Google Scholar] [CrossRef]
- Korda, D.; Doros, A.; Piros, L.; Gerlei, Z.; Haboub-Sandil, A.; Mándli, T.; Fazakas, J.; Deák, P.; Máthé, Z. Liver Transplant for Metastatic Neuroendocrine Tumors: A Single-Center Experience in Hungary. Transplant. Proc. 2019, 51, 1251–1253. [Google Scholar] [CrossRef] [PubMed]
- Valvi, D.; Mei, X.; Gupta, M.; Shah, M.B.; Ancheta, A.; Marti, F.; Gedaly, R. Younger Age Is Associated with Improved Survival in Patients Undergoing Liver Transplantation Alone for Metastatic Neuroendocrine Tumors. J. Gastrointest. Surg. 2021, 25, 1487–1493. [Google Scholar] [CrossRef] [PubMed]
- Sposito, C.; Rossi, R.E.; Monteleone, M.; Coppa, J.; Bongini, M.; Milione, M.; Bhoori, S.; Mazzaferro, V. Postrecurrence Survival After Liver Transplantation for Liver Metastases From Neuroendocrine Tumors. Transplantation 2021, 105, 2579–2586. [Google Scholar] [CrossRef] [PubMed]
- Moons, K.G.M.; Altman, D.G.; Reitsma, J.B.; Ioannidis, J.P.A.; Macaskill, P.; Steyerberg, E.W.; Vickers, A.J.; Ransohoff, D.F.; Collins, G.S. Transparent Reporting of a multivariable prediction model for Individual Prognosis Or Diagnosis (TRIPOD): Explanation and Elaboration. Ann. Intern. Med. 2015, 162, W1. [Google Scholar] [CrossRef]
- Shah, T.; Moore, J.; Venkataraman, H.; Caplin, M.; Smith, S.; O’Toole, D.; Hoti, E.; Dasari, B.; Ford, S.; Mazzaferro, V.; et al. Setting up of a national liver transplant programme for neuroendocrine tumour liver metastases in UK and Ireland: Opportunities for clinical study and research. Endocr. Abstr. 2021, 80, P1. [Google Scholar] [CrossRef]
- Modlin, I.M.; Bodei, L.; Kidd, M. Neuroendocrine tumor biomarkers: From monoanalytes to transcripts and algorithms. Best. Pract. Res. Clin. Endocrinol. Metab. 2016, 30, 59–77. [Google Scholar] [CrossRef]
- Oberg, K.; Modlin, I.M.; De Herder, W.; Pavel, M.; Klimstra, D.; Frilling, A.; Metz, D.C.; Heaney, A.; Kwekkeboom, D.J.; Strosberg, J.R.; et al. Consensus on biomarkers for neuroendocrine tumour disease. Lancet Oncol. 2015, 16, e435–e446. [Google Scholar] [CrossRef]


{kind=link}
| First Author | Year of Publication | Study Period | Country/Ies | Study Design | Sample Size | Median Age | Gender (M:F) | Median Follow-Up | 1-Year OS | 3-Year OS | 5-Year OS | 10-Year OS | 1-Year DFS | 3-Year DFS | 5-Year DFS | 10-Year DFS |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Routley [33] | 1995 | 1983–1997 | United Kingdom | Multicentre, retrospective case series | 11 | NR | 6:5 | NR | 82% | 57% | ||||||
| Rosenau [34] | 2002 | 1982–1997 | Germany | Single centre, retrospective case series | 19 | Median 47 years (range 18–61) | 9:10 | Mean 59 months (0.5–146) | 89% | 80% | 50% | 56% | 21% | 21% | ||
| Florman [35] | 2004 | 1992–2002 | United States | Single centre, retrospective case series | 11 | Mean 51.2 +/− 6.3 yrs | 4:7 | Mean 34 +/− 40 months | 73% | 36% | ||||||
| van Vilsteren [36] | 2006 | 1998–2002 | United States | Single centre, retrospective case series | 17 | Median 47 years (range 22–64) | 15:4 | Mean 22 months (range 0–84) | 87% | 77% | ||||||
| Marin [37] | 2007 | 1996–2006 | Spain | Single centre, retrospective case series | 10 | Mean 42 years (range 30–62) | 5:5 | Mean 3 years, range 1 month–6 years | 86% | 57% | ||||||
| Olausson [23] | 2007 | 1997–2001 | Sweden | Single centre, retrospective case series | 15 (10 OLT, 5 MVT) | Median 51.5 years (range 39–64) OLT. Median 43 years (range 38–57) for MVT | 11:4 | Mean 53.8 months (+/−9.5) | 90% OLT | Approx. 70% for all patients | 20% | |||||
| Dhupar [38] | 2009 | 1991–2006 | United States | Single centre, retrospective case series | 5 | Median 44 years (range 17–53) | 2:3 | NR | 100% | |||||||
| Frilling [39] | 2009 | NR | Germany | Single centre, retrospective case series | 17 | NR | NR | NR | 67% | 48% | ||||||
| Bonaccorsi-Riani [40] | 2010 | NR | Belgium | Single centre, retrospective case series | 9 | Median 54 years (range 26.6–61) | 7:2 | NR | 88% | 77% | 33% | 67% | 33% | 11% | ||
| Le Treut [24] | 2013 | 1982–2009 | Multiple in Europe | Multicentre, retrospective case series | 213 | Mean 46 years +/− 11. Median 48 years (range 16–71) | 114:99 | Mean 56 +/− 49 months (range 0–283) | 81% | 65% | 52% | 65% | 40% | 30% | ||
| Sher [20] | 2015 | 1988–2012 | United States, Canada, Europe | Multicentre, retrospective case series | 85 | Median 48 years (range 16–75) | 51:34 | Median 2.7 years (range 0.05–21.4) | 83% | 60% | 52% | |||||
| Mazzaferro [28] | 2016 | 1995 onwards | Italy | Single centre, retrospective case series | 42 | Median 40.5 (range 13–62) | 26:16 | NR | 97.2% | 88.8% | 86.9% | 86.9% | ||||
| Korda [41] | 2019 | 1995–2018 | Hungary | Single centre, retrospective case series | 10 | Median 49.5 years (range 38–62) | 4:6 | Median 33 months (range 9–104) | 89% | 71% | 80% | 43% | ||||
| Valvi [42] | 2021 | 1988–2018 | United States | Multicentre, retrospective case series | 206 | Mean 48.2 years (SD 11.7, range 19–75) | 117:89 | NR | 89% | 75.3% | 65% | 46.1% | 74.9% | 55.7% | 43.9% | |
| Post-OLT recurrence | ||||||||||||||||
| Sposito [43] | 2021 | 2004–2018 | Italy | Single centre, retrospective case series | 53 had LT; 32 recurred | At recurrence, median 55 (range 48.5–60.3) | 16:15 | Median 73.7 months after recurrence | 76.3% | 45.5% | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palaniappan, V.; Li, C.H.; Frilling, A.; Clift, A.K. Long-Term Outcomes of Liver Transplantation for the Management of Neuroendocrine Neoplasms: A Systematic Review. J. Pers. Med. 2023, 13, 1428. https://doi.org/10.3390/jpm13101428
Palaniappan V, Li CH, Frilling A, Clift AK. Long-Term Outcomes of Liver Transplantation for the Management of Neuroendocrine Neoplasms: A Systematic Review. Journal of Personalized Medicine. 2023; 13(10):1428. https://doi.org/10.3390/jpm13101428
Chicago/Turabian StylePalaniappan, Varun, Chun Hei Li, Andrea Frilling, and Ashley Kieran Clift. 2023. "Long-Term Outcomes of Liver Transplantation for the Management of Neuroendocrine Neoplasms: A Systematic Review" Journal of Personalized Medicine 13, no. 10: 1428. https://doi.org/10.3390/jpm13101428