
Better Oral Hygiene Is Associated with a Decreased Risk of Meniere’s Disease: A Nationwide Cohort Study

Abstract
:1. Introduction
2. Methods
2.1. Data Source
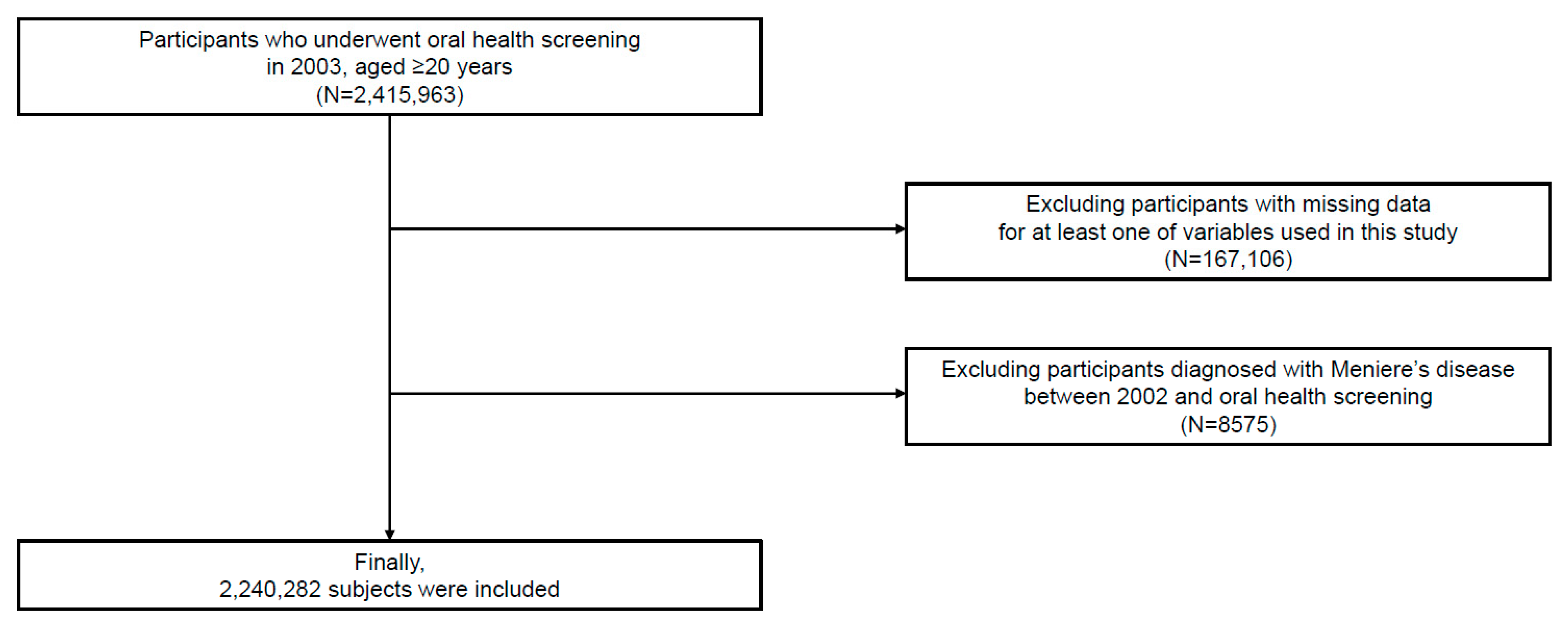
2.2. Study Population
2.3. Definition and Variables
2.4. Study Outcomes
2.5. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Definition of Comorbidities
Appendix B. Treatment Codes Related to Periodontitis
| Code | Procedure |
| U2232 | Removal of dental calculus (one third of the dental arch) |
| U2240 | Root planning |
| U2233 | Removal of dental calculus (whole dental arch) |
| U2221 | Dressing after periodontal treatment (removal of dental calculus, root planning, or curettage) |
| U1010 | Curettage (one third of the dental arch) |
| U2211 | Dressing after dental surgery (simple) |
| U4454 | Incision and drainage (gingival abscess or pericoronal abscess) |
| U2222 | Dressing after periodontal treatment (other than the removal of dental calculus, root planning, or curettage) |
| U0010 | Simple dressing |
| U1051 | Periodontal flap operation (simple) |
| U1052 | Periodontal flap operation (complicated) |
| U4455 | Incision and drainage (periodontal abscess or palatal abscess) |
| U1060 | Root conditioning |
| U2231 | Oral prophylaxis |
| U1040 | Gingivectomy (one third of the dental arch) |
| U4660 | Crown lengthening procedure with gingivectomy |
References
- Lee, K.; Lee, J.S.; Kim, J.; Lee, H.; Chang, Y.; Woo, H.G.; Kim, J.W.; Song, T.J. Oral health and gastrointestinal cancer: A nationwide cohort study. J. Clin. Periodontol. 2020, 47, 796–808. [Google Scholar] [CrossRef]
- Chang, Y.; Lee, J.S.; Woo, H.G.; Ryu, D.R.; Kim, J.W.; Song, T.J. Improved oral hygiene care and chronic kidney disease occurrence: A nationwide population-based retrospective cohort study. Medicine 2021, 100, e27845. [Google Scholar] [CrossRef]
- Woo, H.G.; Chang, Y.; Lee, J.S.; Song, T.J. Association of tooth loss with new-onset parkinson’s disease: A nationwide population-based cohort study. Park. Dis. 2020, 2020, 4760512. [Google Scholar] [CrossRef]
- Kim, J.; Kim, H.J.; Jeon, J.; Song, T.J. Association between oral health and cardiovascular outcomes in patients with hypertension: A nationwide cohort study. J. Hypertens. 2022, 40, 374–381. [Google Scholar] [CrossRef]
- Song, T.J.; Chang, Y.; Jeon, J.; Kim, J. Oral health and longitudinal changes in fasting glucose levels: A nationwide cohort study. PLoS ONE 2021, 16, e0253769. [Google Scholar] [CrossRef]
- Harcourt, J.; Barraclough, K.; Bronstein, A.M. Meniere’s disease. BMJ 2014, 349, g6544. [Google Scholar] [CrossRef]
- Frejo, L.; Lopez-Escamez, J.A. Cytokines and inflammation in meniere disease. Clin. Exp. Otorhinolaryngol. 2022, 15, 49–59. [Google Scholar] [CrossRef]
- Nakae, K.; Komatuzaki, K. Epidemiological study of meniere’s disease. Pract. Otol. (Kyoto) 1984, 69, 1783–1788. [Google Scholar] [CrossRef]
- Kotimäki, J.; Sorri, M.; Aantaa, E.; Nuutinen, J.J.T.L. Prevalence of meniere disease in finland. Laryngoscope 1999, 109, 748–753. [Google Scholar] [CrossRef]
- Tyrrell, J.S.; Whinney, D.J.; Ukoumunne, O.C.; Fleming, L.E.; Osborne, N.J. Prevalence, associated factors, and comorbid conditions for ménière’s disease. Ear Hear. 2014, 35, e162–e169. [Google Scholar] [CrossRef]
- Eidelman, D. Meniere’s disease may be caused by common intraosseous dental pathology--diagnosis using the comparative compression sign. Med. Hypotheses. 2007, 68, 389–392. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.; Woo, H.G.; Park, J.; Lee, J.S.; Song, T.J. Improved oral hygiene care is associated with decreased risk of occurrence for atrial fibrillation and heart failure: A nationwide population-based cohort study. Eur. J. Prev Cardiol. 2020, 27, 1835–1845. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Kwoen, M.J.; Lee, J.R.; Kim, K.S.; Lee, H.J.; Kim, J.W.; Lee, H. Gradual, but not sudden, dose-dependent increase of onj risk with bisphosphonate exposure: A nationwide cohort study in women with osteoporosis. Front. Endocrinol. 2021, 12, 774820. [Google Scholar] [CrossRef] [PubMed]
- Park, S.Y.; Kim, S.H.; Kang, S.H.; Yoon, C.H.; Lee, H.J.; Yun, P.Y.; Youn, T.J.; Chae, I.H. Improved oral hygiene care attenuates the cardiovascular risk of oral health disease: A population-based study from korea. Eur. Heart J. 2019, 40, 1138–1145. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.; Lee, J.S.; Lee, K.J.; Woo, H.G.; Song, T.J. Improved oral hygiene is associated with decreased risk of new-onset diabetes: A nationwide population-based cohort study. Diabetologia 2020, 63, 924–933. [Google Scholar] [CrossRef]
- Song, T.J.; Kim, J.W.; Kim, J. Oral health and changes in lipid profile: A nationwide cohort study. J. Clin. Periodontol. 2020, 47, 1437–1445. [Google Scholar] [CrossRef]
- Kim, S.Y.; Lee, C.H.; Min, C.; Park, I.S.; Choi, H.G. Bidirectional analysis of the association between ménière’s disease and depression: Two longitudinal follow-up studies using a national sample cohort. Clin. Otolaryngol. 2020, 45, 687–694. [Google Scholar] [CrossRef]
- Lee, D.-H.; Han, J.; Jang, M.-j.; Suh, M.-W.; Lee, J.H.; Oh, S.H.; Park, M.K. Association between meniere’s disease and air pollution in south korea. Sci. Rep. 2021, 11, 13128. [Google Scholar] [CrossRef]
- Geismar, K.; Stoltze, K.; Sigurd, B.; Gyntelberg, F.; Holmstrup, P. Periodontal disease and coronary heart disease. J. Periodontol. 2006, 77, 1547–1554. [Google Scholar] [CrossRef]
- Bengtsson, V.W.; Persson, G.R.; Berglund, J.S.; Renvert, S. Periodontitis related to cardiovascular events and mortality: A long-time longitudinal study. Clin. Oral Investig. 2021, 25, 4085–4095. [Google Scholar] [CrossRef]
- Xu, K.; Yu, W.; Li, Y.; Li, Y.; Wan, Q.; Chen, L.; Dong, Y.; Tay, F.R.; Niu, L. Association between tooth loss and hypertension: A systematic review and meta-analysis. J. Dent. 2022, 123, 104178. [Google Scholar] [CrossRef] [PubMed]
- Guo, T.; Wang, Y.; Jiang, Q. Tooth loss and the incidence of ischemic stroke and transient ischemic attack: A systematic review and meta-analysis. J. Healthc. Eng. 2022, 2022, 1088371. [Google Scholar] [CrossRef] [PubMed]
- Iwai, T. Periodontal bacteremia and various vascular diseases. J. Periodontal. Res. 2009, 44, 689–694. [Google Scholar] [CrossRef] [PubMed]
- Loos, B.G. Systemic markers of inflammation in periodontitis. J. Periodontol. 2005, 76, 2106–2115. [Google Scholar] [CrossRef] [PubMed]
- Chung, Y.H.; Kuo, H.C.; Liu, H.Y.; Wu, M.Y.; Chang, W.J.; Chen, J.T.; Cherng, Y.G.; Chen, T.J.; Dai, Y.X.; Wu, H.L.; et al. Association between dental scaling and reduced risk of end-stage renal disease: A nationwide matched cohort study. Int. J. Environ. Res. Public Health 2021, 18, 8910. [Google Scholar] [CrossRef] [PubMed]
- Leelapatana, P.; Limpuangthip, N. Association between oral health and atrial fibrillation: A systematic review. Heliyon 2022, 8, e09161. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.; Li, Z.; He, T.; Bo, C.; Chang, J.; Li, L.; He, Y.; Liu, J.; Charbonneau, D.; Li, R.; et al. Microbiota-based signature of gingivitis treatments: A randomized study. Sci. Rep. 2016, 6, 24705. [Google Scholar] [CrossRef] [Green Version]
- Teeuw, W.J.; Slot, D.E.; Susanto, H.; Gerdes, V.E.; Abbas, F.; D’Aiuto, F.; Kastelein, J.J.; Loos, B.G. Treatment of periodontitis improves the atherosclerotic profile: A systematic review and meta-analysis. J. Clin. Periodontol. 2014, 41, 70–79. [Google Scholar] [CrossRef]
- Arboleda, S.; Vargas, M.; Losada, S.; Pinto, A. Review of obesity and periodontitis: An epidemiological view. Br. Dent. J. 2019, 227, 235–239. [Google Scholar] [CrossRef]
- Billings, M.; Holtfreter, B.; Papapanou, P.N.; Mitnik, G.L.; Kocher, T.; Dye, B.A. Age-dependent distribution of periodontitis in two countries: Findings from nhanes 2009 to 2014 and ship-trend 2008 to 2012. J. Clin. Periodontol. 2018, 45 (Suppl. S20), S130–S148. [Google Scholar] [CrossRef]
- Sabharwal, A.; Stellrecht, E.; Scannapieco, F.A. Associations between dental caries and systemic diseases: A scoping review. BMC Oral Health 2021, 21, 472. [Google Scholar] [CrossRef] [PubMed]
- Jeong, E.; Park, J.B.; Park, Y.G. Evaluation of the association between periodontitis and risk of parkinson’s disease: A nationwide retrospective cohort study. Sci. Rep. 2021, 11, 16594. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.; Woo, H.G.; Lee, J.S.; Song, T.J. Better oral hygiene is associated with lower risk of stroke. J. Periodontol. 2021, 92, 87–94. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Total | Periodontitis (−) | Periodontitis (+) | p-Value | Standardized Difference |
|---|---|---|---|---|---|
| Number of participants (%) | 2,240,282 | 2,178,787 (97.3) | 61,495 (2.7) | ||
| Age, years | 42.29 ± 12.77 | 42.13 ± 12.72 | 48.18 ± 13.11 | <0.001 | 0.47 |
| Sex | <0.001 | 0.09 | |||
| Male | 1,487,062 (66.4) | 1,443,774 (66.3) | 43,288 (70.4) | ||
| Female | 753,220 (33.6) | 735013 (33.7) | 18,207 (29.6) | ||
| Body mass index (kg/m2) | 23.55 ± 14.05 | 23.54 ± 14.23 | 23.80 ± 4.27 | <0.001 | 0.02 |
| Household income | <0.001 | −0.05 | |||
| Q1, lowest | 586,530 (26.2) | 568,702 (26.1) | 17,828 (29.0) | ||
| Q2 | 811,773 (36.2) | 790,161 (36.3) | 21,612 (35.1) | ||
| Q3 | 586,086 (26.2) | 570,748 (26.2) | 15,338 (24.9) | ||
| Q4, highest | 255,893 (11.4) | 249,176 (11.4) | 6717 (10.9) | ||
| Smoking status | <0.001 | 0.08 | |||
| Never | 1,254,512 (56.0) | 1,222,430 (56.1) | 32,082 (52.2) | ||
| Former | 240,678 (10.7) | 233,620 (10.7) | 7058 (11.5) | ||
| Current | 745,092 (33.3) | 722,737 (33.2) | 22,355 (36.4) | ||
| Alcohol consumption (days/week) | <0.001 | 0.13 | |||
| None | 1,497,928 (66.9) | 1,459,550 (67.0) | 38,378 (62.4) | ||
| 1–4 | 684,064 (30.5) | 664,299 (30.5) | 19,765 (32.1) | ||
| ≥5 | 58,290 (2.6) | 54,938 (2.5) | 3352 (5.5) | ||
| Regular physical activity (days/week) | <0.001 | −0.03 | |||
| None | 1,166,662 (52.1) | 1,132,845 (52.0) | 33,817 (55.0) | ||
| 1–4 | 912,225 (40.7) | 889,655 (40.8) | 22,570 (36.7) | ||
| ≥5 | 161,395 (7.2) | 156,287 (7.2) | 5108 (8.3) | ||
| Comorbidities | |||||
| Hypertension | 417,652 (18.6) | 401,892 (18.5) | 15,760 (25.6) | <0.001 | 0.17 |
| Diabetes mellitus | 169,243 (7.6) | 161,746 (7.4) | 7497 (12.2) | <0.001 | 0.16 |
| Dyslipidemia | 282,256 (12.6) | 273,443 (12.6) | 8813 (14.3) | <0.001 | 0.05 |
| Atrial fibrillation | 3723 (0.2) | 3567 (0.2) | 156 (0.3) | <0.001 | 0.02 |
| Cancer | 20,587 (0.9) | 19,823 (0.9) | 764 (1.2) | <0.001 | 0.03 |
| Renal disease | 11,176 (0.5) | 10,746 (0.5) | 430 (0.7) | <0.001 | 0.03 |
| Oral health status | |||||
| Number of missing teeth | <0.001 | 0.35 | |||
| 0 | 1,842,344 (82.2) | 1,800,866 (82.7) | 41,478 (67.5) | ||
| 1–7 | 364,530 (16.3) | 347,147 (15.9) | 17,383 (28.3) | ||
| 8–14 | 19,451 (0.9) | 17,510 (0.8) | 1941 (3.2) | ||
| ≥15 | 13,957 (0.6) | 13,264 (0.6) | 693 (1.1) | ||
| Oral hygiene behaviors | |||||
| Frequency of tooth brushing (times/day) | <0.001 | −0.20 | |||
| 0–1 | 278,065 (12.4) | 267,510 (12.3) | 10,555 (17.2) | ||
| 2 | 1,038,556 (46.4) | 1,007,626 (46.3) | 30,930 (50.3) | ||
| ≥3 | 923,661 (41.2) | 903,651 (41.5) | 20,010 (32.5) | ||
| Dental scaling | <0.001 | −0.11 | |||
| No | 1,727,449 (77.1) | 1,677,403 (77.0) | 50,046 (81.4) | ||
| Yes | 512,833 (22.9) | 501,384 (23.0) | 11,449 (18.6) |
| Number of Participants | Number of Events | Event Rate (%) (95% CI) | Person-Years | Incidence Rate (per 1000 Person-Years) | Adjusted HR (95% CI) | p-Value | |
|---|---|---|---|---|---|---|---|
| Oral health status | |||||||
| Periodontitis | |||||||
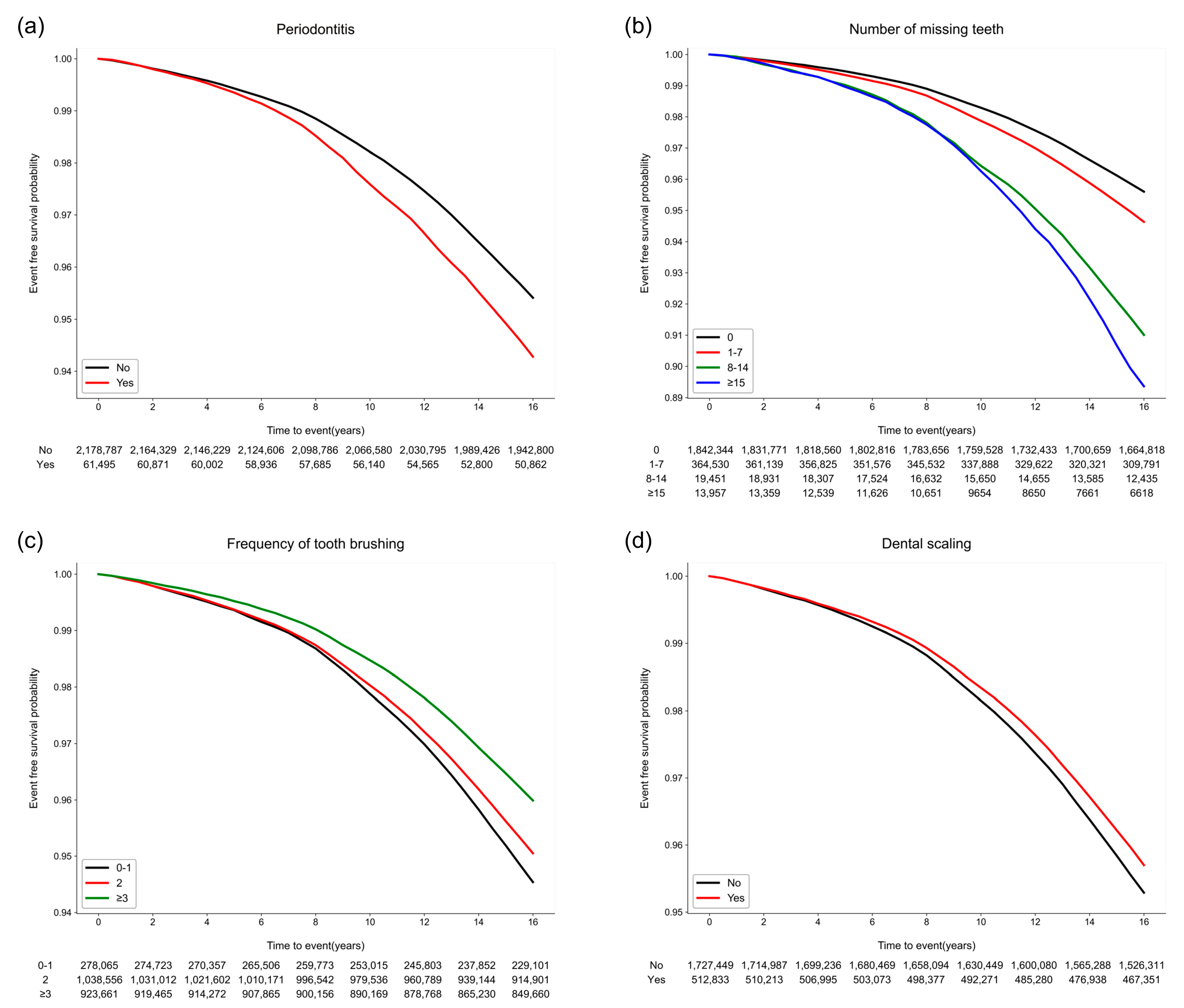
| No | 2,178,787 | 108,351 | 4.97 (4.94, 5.00) | 35,122,258.21 | 3.08 | 1 (reference) | |
| Yes | 61,495 | 3755 | 6.11 (5.91, 6.30) | 968,678.89 | 3.88 | 1.18 (1.14, 1.22) | <0.001 |
| Number of missing teeth | |||||||
| 0 | 1,842,344 | 88,285 | 4.79 (4.76, 4.82) | 29,865,626.16 | 2.96 | 1 (reference) | |
| 1–7 | 364,530 | 20,939 | 5.74 (5.67, 5.82) | 5,771,774.93 | 3.63 | 1.16 (1.15, 1.18) | <0.001 |
| 8–14 | 19,451 | 1678 | 8.63 (8.21, 9.04) | 276,464.01 | 6.07 | 1.37 (1.30, 1.44) | <0.001 |
| ≥15 | 13,957 | 1204 | 8.63 (8.14, 9.11) | 177,072.00 | 6.80 | 1.25 (1.18, 1.32) | <0.001 |
| Oral hygiene behaviors | |||||||
| Frequency of tooth brushing (times/day) | |||||||
| 0–1 | 278,065 | 16,089 | 5.79 (5.70, 5.88) | 4,342,687.69 | 3.70 | 1 (reference) | |
| 2 | 1,038,556 | 55,652 | 5.36 (5.31, 5.40) | 16,700,387.12 | 3.33 | 0.91 (0.89, 0.93) | <0.001 |
| ≥3 | 923,661 | 40,365 | 4.37 (4.33, 4.41) | 15,047,862.30 | 2.68 | 0.75 (0.73, 0.76) | <0.001 |
| Dental scaling | |||||||
| No | 1,727,449 | 88,049 | 5.10 (5.06, 5.13) | 27,749,737.61 | 3.17 | 1 (reference) | |
| Yes | 512,833 | 24,057 | 4.69 (4.63, 4.75) | 8,341,199.49 | 2.88 | 0.98 (0.97, 0.99) | 0.003 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, J.-H.; Kim, J.-W.; Lee, H.; Hong, I.; Song, T.-J. Better Oral Hygiene Is Associated with a Decreased Risk of Meniere’s Disease: A Nationwide Cohort Study. J. Pers. Med. 2023, 13, 80. https://doi.org/10.3390/jpm13010080
Park J-H, Kim J-W, Lee H, Hong I, Song T-J. Better Oral Hygiene Is Associated with a Decreased Risk of Meniere’s Disease: A Nationwide Cohort Study. Journal of Personalized Medicine. 2023; 13(1):80. https://doi.org/10.3390/jpm13010080
Chicago/Turabian StylePark, Jung-Hyun, Jin-Woo Kim, Heajung Lee, Iksun Hong, and Tae-Jin Song. 2023. "Better Oral Hygiene Is Associated with a Decreased Risk of Meniere’s Disease: A Nationwide Cohort Study" Journal of Personalized Medicine 13, no. 1: 80. https://doi.org/10.3390/jpm13010080