
The Impact of the COVID-19 Pandemic on Postpartum Maternal Mental Health

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
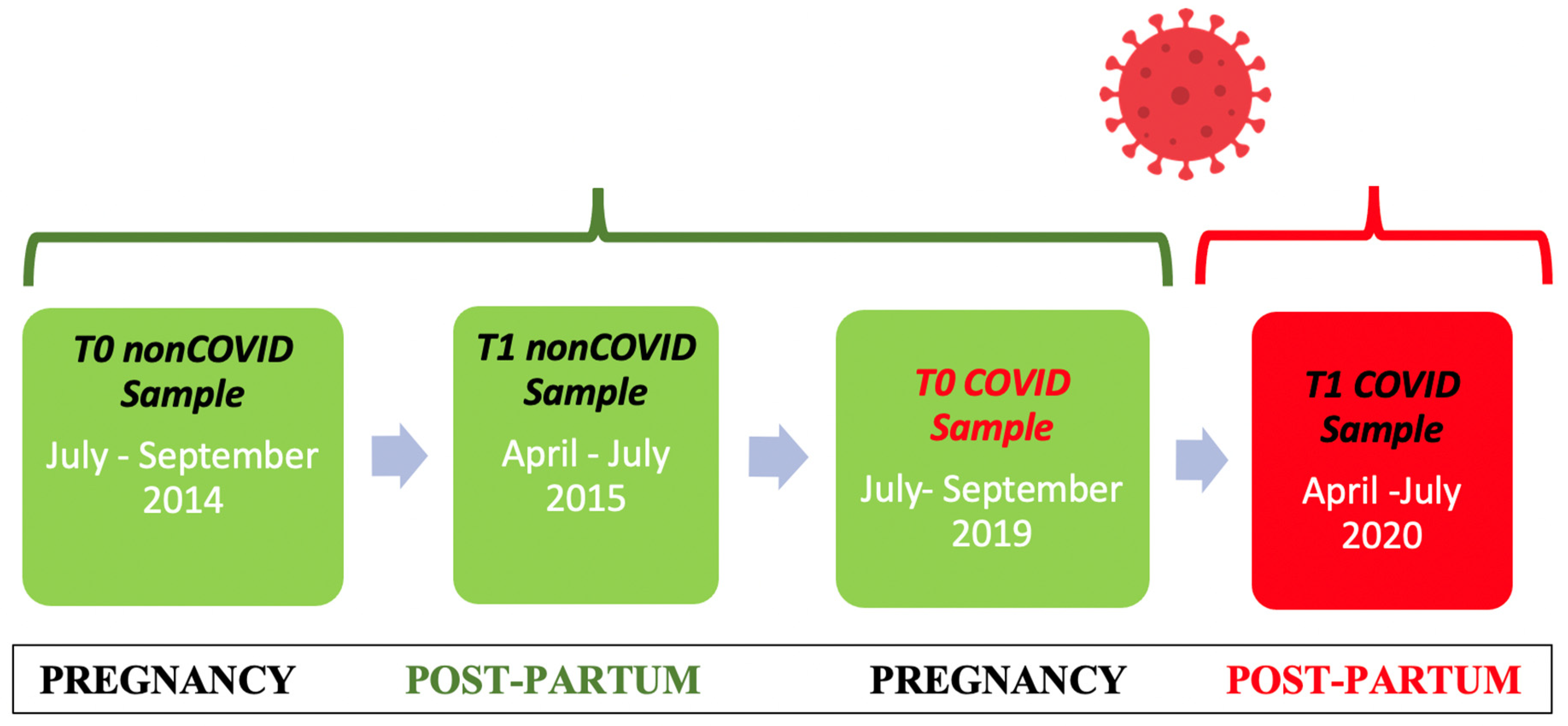
2.1. Research Setting
2.2. Participants
2.3. Measures
2.4. Statistical Analysis
3. Results
3.1. Descriptive Statistics
3.2. Non-COVID Sample
3.3. COVID Sample
3.4. Comparisons between COVID and Non-COVID Samples
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Xu, B.; Gutierrez, B.; Mekaru, S.; Sewalk, K.; Goodwin, L.; Loskill, A.; Cohn, E.L.; Hswen, Y.; Hill, S.C.; Cobo, M.M.; et al. Epidemiological data from the COVID-19 outbreak, real-time case information. Sci. Data 2020, 7, 106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Velavan, T.P.; Meyer, C.G. The COVID-19 epidemic. Trop. Med. Int. Health 2020, 25, 278–280. [Google Scholar] [CrossRef] [Green Version]
- Prati, G.; Mancini, A.D. The psychological impact of COVID-19 pandemic lockdowns: A review and meta-analysis of longitudinal studies and natural experiments. Psychol. Med. 2021, 51, 201–211. [Google Scholar] [CrossRef] [PubMed]
- Landi, G.; Pakenham, K.I.; Boccolini, G.; Grandi, S.; Tossani, E. Health Anxiety and Mental Health Outcome during COVID-19 Lockdown in Italy: The Mediating and Moderating Roles of Psychological Flexibility. Front. Psychol. 2020, 11, 2195. [Google Scholar] [CrossRef] [PubMed]
- Montalbani, B.; Bargagna, P.; Mastrangelo, M.; Sarubbi, S.; Imbastaro, B.; De Luca, G.P.; Anibaldi, G.; Erbuto, D.; Pompili, M.; Comparelli, A. The COVID-19 Outbreak and Subjects with Mental Disorders Who Presented to an Italian Psychiatric Emergency Department. J. Nerv. Ment. Dis. 2021, 209, 246–250. [Google Scholar] [CrossRef] [PubMed]
- Kotlar, B.; Gerson, E.; Petrillo, S.; Langer, A.; Tiemeier, H. The impact of the COVID-19 pandemic on maternal and perinatal health: A scoping review. Reprod. Health 2021, 18, 10. [Google Scholar] [CrossRef] [PubMed]
- Fiorillo, A.; Sampogna, G.; Giallonardo, V.; Del Vecchio, V.; Luciano, M.; Albert, U.; Carmassi, C.; Carrà, G.; Cirulli, F.; Dell’Osso, B.; et al. Effects of the lockdown on the mental health of the general population during the COVID-19 pandemic in Italy: Results from the COMET collaborative network. Eur. Psychiatry 2020, 63, e87. [Google Scholar] [CrossRef]
- Rossi, R.; Socci, V.; Talevi, D.; Mensi, S.; Niolu, C.; Pacitti, F.; Di Marco, A.; Rossi, A.; Siracusano, A.; Di Lorenzo, G. COVID-19 Pandemic and Lockdown Measures Impact on Mental Health Among the General Population in Italy. Front. Psychiatry 2020, 11, 790. [Google Scholar] [CrossRef]
- Moccia, L.; Janiri, D.; Pepe, M.; Dattoli, L.; Molinaro, M.; De Martin, V.; Chieffo, D.; Janiri, L.; Fiorillo, A.; Sani, G.; et al. Affective temperament, attachment style, and the psychological impact of the COVID-19 outbreak: An early report on the Italian general population. Brain Behav. Immun. 2020, 87, 75–79. [Google Scholar] [CrossRef]
- Fiorenzato, E.; Zabberoni, S.; Costa, A.; Cona, G. Cognitive and mental health changes and their vulnerability factors related to COVID-19 lockdown in Italy. PLoS ONE 2021, 16, e0246204. [Google Scholar] [CrossRef]
- Hessami, K.; Romanelli, C.; Chiurazzi, M.; Cozzolino, M. COVID-19 pandemic and maternal mental health: A systematic review and meta-analysis. J. Matern. Fetal Neonatal Med. 2022, 35, 4014–4021. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Zhang, C.; Liu, H.; Duan, C.; Li, C.; Fan, J.; Li, H.; Chen, L.; Xu, H.; Li, X.; et al. Perinatal depressive and anxiety symptoms of pregnant women during the coronavirus disease 2019 outbreak in China. Am. J. Obstet. Gynecol. 2020, 223, 240.e1–240.e9. [Google Scholar] [CrossRef] [PubMed]
- Fallon, V.; Davies, S.M.; Silverio, S.A.; Jackson, L.; De Pascalis, L.; Harrold, J.A. Psychosocial experiences of postnatal women during the COVID-19 pandemic. A UK-wide study of prevalence rates and risk factors for clinically relevant depression and anxiety. J. Psychiatr. Res. 2021, 136, 157–166. [Google Scholar] [CrossRef] [PubMed]
- Harrison, V.; Moulds, M.L.; Jones, K. Support from friends moderates the relationship between repetitive negative thinking and postnatal wellbeing during COVID-19. J. Reprod. Infant Psychol. 2021, 40, 516–531. [Google Scholar] [CrossRef]
- Pariente, G.; Broder, O.W.; Sheiner, E.; Battat, T.L.; Mazor, E.; Salem, S.Y.; Kosef, T.; Wainstock, T. Risk for probable post-partum depression among women during the COVID-19 pandemic. Arch. Women’s Ment. Health 2020, 23, 767–773. [Google Scholar] [CrossRef]
- Spinola, O.; Liotti, M.; Speranza, A.M.; Tambelli, R. Effects of COVID-19 Epidemic Lockdown on Postpartum Depressive Symptoms in a Sample of Italian Mothers. Front. Psychiatry 2020, 11, 589916. [Google Scholar] [CrossRef]
- Orsolini, L.; Pompili, S.; Mauro, A.; Salvi, V.; Volpe, U. Fear and anxiety related to COVID-19 pandemic may predispose to perinatal depression in Italy. Front. Psychiatry 2022, 13, 977681. [Google Scholar] [CrossRef]
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. Br. J. Psychiatry 1987, 150, 782–786. [Google Scholar] [CrossRef] [Green Version]
- Benvenuti, P.; Ferrara, M.; Niccolai, C.; Valoriani, V.; Cox, J.L. The Edinburgh Postnatal Depression Scale: Validation for an Italian sample. J. Affect. Disord. 1999, 53, 137–141. [Google Scholar] [CrossRef]
- Murray, D.; Cox, J.L. Screening for depression during pregnancy with the edinburgh depression scale (EPDS). J. Reprod. Infant Psychol. 1990, 8, 99–107. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence [NICE]. Antenatal and Postnatal Mental Health: Clinical Management and Service Guidance. Clinical Guideline [CG192]. Published: 17 December 2014. Last Updated: 11 February 2020. Available online: https://www.nice.org.uk/guidance/cg192/resources/antenatal-and-postnatal-mental-health-clinical-management-and-service-guidance-pdf-35109869806789 (accessed on 29 May 2021).
- American College of Obstetricians and Gynecologists (ACOG). ACOG publications: October 2018. Practice guidelines. Obstet. Gynecol. 2018, 132, 1075–1076. [Google Scholar] [CrossRef]
- Murray, L.; Carothers, A.D. The Validation of the Edinburgh Post-natal Depression Scale on a Community Sample. Br. J. Psychiatry 1990, 157, 288–290. [Google Scholar] [CrossRef]
- Zelkowitz, P.; Tamara, H.M. Screening for Post-Partum Depression in a Community Sample. Can. J. Psychiatry 1995, 40, 80–86. [Google Scholar] [CrossRef]
- Carpiniello, B.; Pariante, C.M.; Serri, F.; Costa, G.; Carta, M.G. Validation of the Edinburgh Postnatal Depression Scale in Italy. J. Psychosom. Obstet. Gynecol. 1997, 18, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Matthey, S. Using the Edinburgh Postnatal Depression Scale to screen for anxiety disorders. Depress. Anxiety 2008, 25, 926–931. [Google Scholar] [CrossRef] [PubMed]
- Swalm, D.; Brooks, J.; Doherty, D.; Nathan, E.; Jacques, A. Using the Edinburgh postnatal depression scale to screen for perinatal anxiety. Arch. Women’s Ment. Health 2010, 13, 515–522. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Mondo, M.; Sechi, C.; Cabras, C. Psychometric evaluation of three versions of the Italian Perceived Stress Scale. Curr. Psychol. 2019, 40, 1884–1892. [Google Scholar] [CrossRef]
- Angst, J.; Adolfsson, R.; Benazzi, F.; Gamma, A.; Hantouche, E.; Meyer, T.D.; Skeppar, P.; Vieta, E.; Scott, J. The HCL-32: Towards a self-assessment tool for hypomanic symptoms in outpatients. J. Affect. Disord. 2005, 88, 217–233. [Google Scholar] [CrossRef]
- Carta, M.G.; Hardoy, M.C.; Cadeddu, M.; Murru, A.; Campus, A.; Morosini, P.L.; Gamma, A.; Angst, J. The accuracy of the Italian version of the Hypomania Checklist (HCL-32) for the screening of bipolar disorders and comparison with the Mood Disorder Questionnaire (MDQ) in a clinical sample. Clin. Pract. Epidemiol. Ment. Health 2006, 2, 2. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F., III; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef] [PubMed]
- Curcio, G.G.; Tempesta, D.; Scarlata, S.; Marzano, C.; Moroni, F.; Rossini, P.M.; Ferrara, M.; De Gennaro, L. Validity of the Italian Version of the Pittsburgh Sleep Quality Index (PSQI). Neurol. Sci. 2012, 34, 511–519. [Google Scholar] [CrossRef] [PubMed]
- Zung, W.W. A Rating Instrument For Anxiety Disorders. J. Psychosom. Res. 1971, 12, 371–379. [Google Scholar] [CrossRef] [PubMed]
- Zung, W.W.K. The Measurement of Affects: Depression and Anxiety. Mod. Probl. Pharm. 1974, 7, 170–188. [Google Scholar] [CrossRef]
- Dunstan, D.A.; Scott, N. Norms for Zung’s Self-rating Anxiety Scale. BMC Psychiatry 2020, 20, 90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunstan, D.A.; Scott, N.; Todd, A.K. Screening for anxiety and depression: Reassessing the utility of the Zung scales. BMC Psychiatry 2017, 17, 329. [Google Scholar] [CrossRef]
- Tanaka-Matsumi, J.; Kameoka, V.A. Reliabilities and concurrent validities of popular self-report measures of depression, anxiety, and social desirability. J. Consult. Clin. Psychol. 1986, 54, 328–333. [Google Scholar] [CrossRef]
- Shapiro, S.S.; Wilk, M.B. An analysis of variance test for normality (complete samples). Biometrika 1965, 52, 591–611. [Google Scholar] [CrossRef]
- Adewuya, A.O.; Ola, B.A.; Dada, A.O.; Fasoto, O.O. Validation of the Edinburgh Postnatal Depression Scale as a screening tool for depression in late pregnancy among Nigerian women. J. Psychosom. Obstet. Gynecol. 2006, 27, 267–272. [Google Scholar] [CrossRef]
- Su, K.-P.; Chiu, T.-H.; Huang, C.-L.; Ho, M.; Lee, C.-C.; Wu, P.-L.; Lin, C.-Y.; Liau, C.-H.; Liao, C.-C.; Chiu, W.-C.; et al. Different cutoff points for different trimesters? The use of Edinburgh Postnatal Depression Scale and Beck Depression Inventory to screen for depression in pregnant Taiwanese women. Gen. Hosp. Psychiatry 2007, 29, 436–441. [Google Scholar] [CrossRef]
- Brunelli, A.; Silvestrini, G.; Palestini, L.; Vitali, P.; Nanni, R.; Belluzzi, A.; Ciambra, R.; De Logu, M.; Degli Angeli, M.; Dessì, F.L.; et al. Impatto del lockdown sui bambini e sulle famiglie: un’indagine dei pediatri di famiglia all’interno di una comunità [Impact of the lockdown on children and families: A survey of family pediatricians within a community]. Recenti. Prog. Med. 2021, 112, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Istat (Istituto Nazionale di Statistica). Informazioni Sulla Rilevazione. Indagine Multiscopo Sulle Famiglie: Aspetti della vita quotidiana. Periodo di riferimento: Anno 2020. Data di Pubblicazione: 9 marzo 2021. Istat: Roma, Italy, 2021. Available online: https://www.istat.it/it/archivio/91926 (accessed on 22 June 2021).
- Pieh, C.; O’rourke, T.; Budimir, S.; Probst, T. Relationship quality and mental health during COVID-19 lockdown. PLoS ONE 2020, 15, e0238906. [Google Scholar] [CrossRef] [PubMed]
- Matthies, L.M.; Müller, M.; Doster, A.; Sohn, C.; Wallwiener, M.; Reck, C.; Wallwiener, S. Maternal–fetal attachment protects against postpartum anxiety: The mediating role of postpartum bonding and partnership satisfaction. Arch. Gynecol. Obstet. 2020, 301, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Mari, E.; Fraschetti, A.; Lausi, G.; Pizzo, A.; Baldi, M.; Paoli, E.; Giannini, A.M.; Avallone, F. Forced Cohabitation during Coronavirus Lockdown in Italy: A Study on Coping, Stress and Emotions among Different Family Patterns. J. Clin. Med. 2020, 9, 3906. [Google Scholar] [CrossRef]
- Killgore, W.D.S.; Taylor, E.C.; Cloonan, S.A.; Dailey, N.S. Psychological resilience during the COVID-19 lockdown. Psychiatry Res. 2020, 291, 113216. [Google Scholar] [CrossRef]
- Kinser, P.A.; Jallo, N.; Amstadter, A.B.; Thacker, L.R.; Jones, E.; Moyer, S.; Rider, A.; Karjane, N.; Salisbury, A.L. Depression, Anxiety, Resilience, and Coping: The Experience of Pregnant and New Mothers During the First Few Months of the COVID-19 Pandemic. J. Women’s Health 2021, 30, 654–664. [Google Scholar] [CrossRef]
- Khatri, G.K.; Tran, T.D.; Baral, S.; Fisher, J. Effect of the 2015 Nepal Earthquakes on symptoms of common mental disorders among women who are pregnant. J. Affect. Disord. 2018, 228, 238–247. [Google Scholar] [CrossRef]
- Harville, E.W.; Xiong, X.; Pridjian, G.; Elkind-Hirsch, K.; Buekens, P. Postpartum mental health after Hurricane Katrina: A cohort study. BMC Pregnancy Childbirth 2009, 9, 21. [Google Scholar] [CrossRef] [Green Version]
- Sade, S.; Sheiner, E.; Wainstock, T.; Hermon, N.; Salem, S.Y.; Kosef, T.; Battat, T.L.; Oron, S.; Pariente, G. Risk for Depressive Symptoms among Hospitalized Women in High-Risk Pregnancy Units during the COVID-19 Pandemic. J. Clin. Med. 2020, 9, 2449. [Google Scholar] [CrossRef]
- Dsouza, D.D.; Quadros, S.; Hyderabadwala, Z.J.; Mamun, M.A. Aggregated COVID-19 suicide incidences in India: Fear of COVID-19 infection is the prominent causative factor. Psychiatry Res. 2020, 290, 113145. [Google Scholar] [CrossRef]
- Bonanno, G.A.; Galea, S.; Bucciarelli, A.; Vlahov, D. Psychological Resilience After Disaster: New York City in the aftermath of the September 11th terrorist attack. Psychol. Sci. 2006, 17, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Klein, M. A contribution to the psychogenesis of manic-depressive states (1935). In The Writings of Melanie Klein, Vol. 1: Love, Guilt and Reparation and Other Works, 1921–1945; Hogarth Press: London, UK, 1975; pp. 262–289, 432–438, 439–443. [Google Scholar]
- Janiri, D.; Carfì, A.; Kotzalidis, G.D.; Bernabei, R.; Landi, F.; Sani, G. Gemelli Against COVID-19 Post-Acute Care Study Group Posttraumatic Stress Disorder in Patients After Severe COVID-19 Infection. JAMA Psychiatry 2021, 78, 567–569. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ettman, C.K.; Abdalla, S.M.; Cohen, G.H.; Sampson, L.; Vivier, P.M.; Galea, S. Low assets and financial stressors associated with higher depression during COVID-19 in a nationally representative sample of US adults. J. Epidemiol. Community Health 2020, 75, 501–508. [Google Scholar] [CrossRef]
- McGinty, E.E.; Presskreischer, R.; Anderson, K.E.; Han, H.; Barry, C.L. Psychological Distress and COVID-19–Related Stressors Reported in a Longitudinal Cohort of US Adults in April and July 2020. JAMA 2020, 324, 2555–2557. [Google Scholar] [CrossRef]
- Glynn, L.M.; Wadhwa, P.D.; Dunkel-Schetter, C.; Chicz-DeMet, A.; Sandman, C.A. When stress happens matters: Effects of earthquake timing on stress responsivity in pregnancy. Am. J. Obstet. Gynecol. 2001, 184, 637–642. [Google Scholar] [CrossRef] [Green Version]
- Ehrlich, M.; Harville, E.; Xiong, X.; Buekens, P.; Pridjian, G.; Elkind-Hirsch, K. Loss of Resources and Hurricane Experience as Predictors of Postpartum Depression Among Women in Southern Louisiana. J. Women’s Health 2010, 19, 877–884. [Google Scholar] [CrossRef]
- Xiong, X.; Harville, E.W.; Mattison, D.R.; Elkind-Hirsch, K.; Pridjian, G.; Buekens, P. Hurricane Katrina experience and the risk of post-traumatic stress disorder and depression among pregnant women. Am. J. Disaster. Med. 2010, 5, 181–187, Erratum in Am. J. Disaster. Med. 2010, 5, 360. [Google Scholar] [CrossRef]
- Kildea, S.; Simcock, G.; Liu, A.; Elgbeili, G.; Laplante, D.P.; Kahler, A.; Austin, M.-P.; Tracy, S.; Kruske, S.; Tracy, M.; et al. Continuity of midwifery carer moderates the effects of prenatal maternal stress on postnatal maternal wellbeing: The Queensland flood study. Arch. Women’s Ment. Health 2018, 21, 203–214. [Google Scholar] [CrossRef]
- Khatri, G.K.; Tran, T.; Fisher, J. Prevalence and determinants of symptoms of antenatal common mental disorders among women who had recently experienced an earthquake: A systematic review. BMC Psychiatry 2019, 19, 47. [Google Scholar] [CrossRef]
- Perzow, S.E.; Hennessey, E.-M.P.; Hoffman, M.C.; Grote, N.K.; Davis, E.P.; Hankin, B.L. Mental health of pregnant and postpartum women in response to the COVID-19 pandemic. J. Affect. Disord. Rep. 2021, 4, 100123. [Google Scholar] [CrossRef] [PubMed]
- Douglas, A.J.; Brunton, P.J.; Bosch, O.J.; Russell, J.A.; Neumann, I.D. Neuroendocrine responses to stress in mice: Hyporesponsiveness in pregnancy and parturition. Endocrinology 2003, 144, 5268–5276. [Google Scholar] [CrossRef] [PubMed]
- Lonstein, J.S. Reduced anxiety in postpartum rats requires recent physical interactions with pups, but is independent of suckling and peripheral sources of hormones. Horm. Behav. 2005, 47, 241–255. [Google Scholar] [CrossRef] [PubMed]
- Slattery, D.A.; Neumann, I.D. No stress please! Mechanisms of stress hyporesponsiveness of the maternal brain. J. Physiol. 2008, 586, 377–385. [Google Scholar] [CrossRef] [PubMed]
- Seeley, W.W.; Menon, V.; Schatzberg, A.F.; Keller, J.; Glover, G.H.; Kenna, H.; Reiss, A.L.; Greicius, M.D. Dissociable intrinsic connectivity networks for salience processing and executive control. J. Neurosci. 2007, 27, 2349–2356. [Google Scholar] [CrossRef]
- Chan, A.S.W.; Ho, J.M.C.; Li, J.S.F.; Tam, H.L.; Tang, P.M.K. Impacts of COVID-19 Pandemic on Psychological Well-Being of Older Chronic Kidney Disease Patients. Front. Med. 2021, 8, 666973. [Google Scholar] [CrossRef]


{kind=link}
| Parameter | Total Group | COVID | Non-COVID | p COVID vs. Non-COVID |
|---|---|---|---|---|
| Age, in years ( ± SD) | 33.62 ± 4.68 | 33.25 ± 4.69 | 34.01 ± 4.68 | 0.337 |
| Nationality | 0.495 | |||
| Italian N (%) | 131 (93.6) | 66 (91.7) | 65 (95.6) | |
| Other N (%) | 9 (6.4) | 6 (8.3) | 3 (4.4) | |
| Educational level | 0.967 | |||
| Primary, N (%) | 0 | 0 | 0 | |
| Middle school, N (%) | 4 (2.8) | 2 (2.8) | 2 (2.9) | |
| High school, N (%) | 48 (34.3) | 24 (33.3) | 24 (35.3) | |
| College/ University, N (%) | 88 (62.9) | 46 (63.9) | 42 (61.8) | |
| Professional status | 1.000 | |||
| Employed, N (%) | 114 (81.4) | 59 (81.9) | 55 (80.9) | |
| Unemployed, N (%) | 26 (18.6) | 13 (18.1) | 13 (19.1) | |
| Active medical condition | 0.152 | |||
| Yes N (%) | 30 (21.4) | 19 (26.4) | 11 (83.8) | |
| No N (%) | 109 (77.9) | 52 (72.2) | 57 (16.2) | |
| Missing | 1 (0.7) | 1 (1.4) | 0 | |
| Medical treatment | 0.819 | |||
| Yes N (%) | 22 (15.7) | 12 (16.7) | 10 (14.7) | |
| No N (%) | 118 (84.3) | 60 (83.3) | 58 (85.3) | |
| Psychiatric history | 0.840 | |||
| Positive N (%) | 31 (22.1) | 15 (20.8) | 16 (23.5) | |
| Negative N (%) | 106 (75.7) | 54 (75) | 52 (76.5) | |
| Missing | 3 (2.1) | 3 (4.2) | 0 | |
| Past psychiatric drug treatment | 0.741 | |||
| Yes N (%) | 9 (6.4) | 4 (5.6) | 5 (7.4) | |
| No N (%) | 128 (91.4) | 66 (91.7) | 62 (91.2) | |
| Missing | 3 (2.1) | 2 (2.8) | 1 (1.5) | |
| Psychiatric drug treatment during current pregnancy | . | |||
| Yes N (%) | 0 | 0 | 0 | |
| No N (%) | 140 (100) | 72 (100) | 68 (100) | |
| Smokes | 0.116 | |||
| Yes N (%) | 7 (5) | 6 (8.6) | 1 (1.5) | |
| No N (%) | 131 (93.6) | 64 (91.4) | 67 (98.5) | |
| Missing | 2 (1.4) | 2 (2.8) | ||
| Uses alcohol | . | |||
| Yes N (%) | 0 | 0 | 0 | |
| No N (%) | 140 (100) | 72 (100) | 68 (100) | |
| Coffee, Tea or Energy drinks | < 0.001 | |||
| Yes N (%) | 54 (38.6) | 38 (52.8) | 52 (76.5) | |
| No N (%) | 86 (61.4) | 34 (47.2) | 15 (22.1) | |
| Abuses of drugs | 0.497 | |||
| Yes N (%) | 2 (1.4) | 2 (2.8) | 0 | |
| No N (%) | 138 (98.6) | 70 (97.2) | 68 (100) | |
| Premenstrual syndrome | 0.305 | |||
| Yes N (%) | 60 (42.9) | 34 (47.2) | 26 (38.2) | |
| No N (%) | 79 (56.4) | 37 (51.4) | 42 (61.8) | |
| Missing | 1 (0.7) | 1 (1.4) | 0 | |
| Psychiatric family history | 1.000 | |||
| Positive N (%) | 43 (30.7) | 22 (30.6) | 21 (30.9) | |
| Negative N (%) | 93 (66.4) | 47 (65.3) | 46 (67.6) | |
| Missing | 4 (2.9) | 3 (4.2) | 1 (1.5) | |
| Past abortions | 0.591 | |||
| Yes N (%) | 47 (33.6) | 26 (36.1) | 21 (30.9) | |
| No N (%) | 92 (65.7) | 45 (62.5) | 47 (69.1) | |
| Missing | 1 (0.7) | 1 (1.4) | 0 | |
| Primiparas | 0.726 | |||
| Yes N (%) | 87 (62.1) | 43 (59.7) | 44 (64.7) | |
| No N (%) | 52 (37.1) | 28 (38.9) | 24 (35.3) | |
| Missing | 1 (0.7) | 1 (1.4) | 0 | |
| Medically-Assisted Reproduction | 0.495 | |||
| Yes N (%) | 9 (6.4) | 6 (8.3) | 3 (4.4) | |
| No N (%) | 131 (93.6) | 66 (91.7) | 65 (95.6) | |
| Previous Perinatal psychiatric episodes | 0.392 | |||
| Yes N (%) | 6 (11.3) | 2 (6.9) | 4 (16.6) | |
| No N (%) | 47 (88.7) | 27 (93.1) | 20 (83.3) | |
| Pregnancy Complications | 0.447 | |||
| Yes N (%) | 38 (27.1) | 22 (30.6) | 16 (23.5) | |
| No N (%) | 99 (70.7) | 49 (68.1) | 50 (73.5) | |
| Missing | 3 (2.1) | 1 (1.4) | 2 (2.9) | |
| COVID N (%) | Non-COVID N (%) | p-Value | |
|---|---|---|---|
| T0 | |||
| EPDS T0 ≥ 12 | 7 (9.7) | 1 (1.5) | 0.063 |
| EPDS T0 ≥ 9 | 18 (25) | 8 (11.8) | 0.052 |
| EPDS-3A T0 ≥ 4 | 31 (43) | 16 (23.5) | 0.020 |
| Item 10 >0 T0 | 2 (2.8) | 0 | 0.497 |
| HCL 32 T0 ≥ 14 | 25 (40.3) | 24 (38.1) | 0.856 |
| PSQI T0 ≥ 5 | 51 (72.9) | 21 (72.4) | 1,000 |
| SAS T0 ≥ 36 | 22 (31.9) | 15 (51.7) | 0.073 |
| T1 | |||
| EPDS T1 ≥12 | 10 (14.1) | 3 (4.4) | 0.078 |
| EPDS T1 ≥9 | 21 (29.6) | 7 (10.3) | 0.006 |
| EPDS-3A T1 ≥4 | 12 (16.9) | 4 (5.9) | 0.061 |
| Item 10 >0 T1 | 3 (4.2) | 1 (1.5) | 0.620 |
| HCL 32 T1 ≥ 14 | 21 (29.6) | 14 (21.5) | 0.329 |
| PSQI T1 ≥ 5 | 26 (36.1) | ||
| SAS T1 ≥ 36 | 12 (16.7) |
| Sum of Squares | df | Mean Square | F | Sig. | ||
|---|---|---|---|---|---|---|
| T0 EPDS TOTAL | Between Groups | 66,275 | 1 | 66,275 | 5583 | 0.020 |
| Within Groups | 1,638,261 | 138 | 11,871 | |||
| Total | 1,704,536 | 139 | ||||
| T0 EPDS-3A | Between Groups | 20,102 | 1 | 20,102 | 6994 | 0.009 |
| Within Groups | 396,641 | 138 | 2874 | |||
| Total | 416,743 | 139 | ||||
| T0 HCL-32 TOTAL | Between Groups | 68,354 | 1 | 68,354 | 1619 | 0.206 |
| Within Groups | 5,192,318 | 123 | 42,214 | |||
| Total | 5,260,672 | 124 | ||||
| T1 EPDS TOTAL | Between Groups | 52,683 | 1 | 52,683 | 3305 | 0.071 |
| Within Groups | 2,184,022 | 137 | 15,942 | |||
| Total | 2,236,705 | 138 | ||||
| T1 EPDS-3A | Between Groups | 5528 | 1 | 5528 | 1430 | 0.234 |
| Within Groups | 529,638 | 137 | 3866 | |||
| Total | 535,165 | 138 | ||||
| T1 HCL 32 TOTAL | Between Groups | 201,147 | 1 | 201,147 | 6743 | 0.010 |
| Within Groups | 3,997,089 | 134 | 29,829 | |||
| Total | 4,198,235 | 135 | ||||
| T0 | T1 | Sum of Squares | df | Mean Square | F | p | ||
|---|---|---|---|---|---|---|---|---|
| NON COVID | ||||||||
| EPDS TOTAL | 4.47 ± 2.657 | 4.85 ± 3.391 | Between Groups | 143,266 | 13 | 11,020 | 1805 | 0.066 |
| Within Groups | 329,675 | 54 | 6105 | |||||
| Total | 472,941 | 67 | ||||||
| EPDS-3A | 2.35 ± 1.533 | 2.56 ± 1.757 | Between Groups | 56,114 | 7 | 8016 | 4743 | <0.001 |
| Within Groups | 101,415 | 60 | 1690 | |||||
| Total | 157,529 | 67 | ||||||
| HCL 32 TOTAL | 10.70 ± 6.838 | 8.52 ± 6.362 | Between Groups | 1,301,200 | 22 | 59,145 | 1520 | 0.128 |
| Within Groups | 1439,783 | 37 | 38,913 | |||||
| Total | 2,740,983 | 59 | ||||||
| COVID | ||||||||
| EPDS TOTAL | 5.85 ± 4.051 | 6.08 ± 4.494 | Between Groups | 602,208 | 16 | 37,638 | 3614 | <0.001 |
| Within Groups | 562,383 | 54 | 10,415 | |||||
| Total | 1,164,592 | 70 | ||||||
| EPDS-3A | 3.11 ± 1.835 | 2.96 ± 2.148 | Between Groups | 57,101 | 8 | 7138 | 2432 | 0.024 |
| Within Groups | 181,998 | 62 | 2935 | |||||
| Total | 239,099 | 70 | ||||||
| HCL 32 TOTAL | 12.18 ± 6.131 | 10.96 ± 4.483 | Between Groups | 794,903 | 19 | 41,837 | 1163 | 0.332 |
| Within Groups | 1,474,507 | 41 | 35,964 | |||||
| Total | 2,269,410 | 60 | ||||||
| PSS TOTAL | 11.50 ± 5.795 | 15.51 ± 7.698 | Between Groups | 639,724 | 24 | 26,655 | 672 | 0.841 |
| Within Groups | 1,268,417 | 32 | 39,638 | |||||
| Total | 1,908,140 | 56 | ||||||
| PSQI GLOBAL | 6.74 ± 3.369 | 4.38 ± 3.040 | Between Groups | 165,501 | 10 | 16,550 | 1558 | 0.143 |
| Within Groups | 616,267 | 58 | 10,625 | |||||
| Total | 781,768 | 68 | ||||||
| SAS TOTAL | 33.78 ± 6.135 | 32.70 ± 4.451 | Between Groups | 982,774 | 16 | 61,423 | 2016 | 0.030 |
| Within Groups | 1,553,756 | 51 | 30,466 | |||||
| Total | 2,536,529 | 67 | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Chiara, L.; Angeletti, G.; Anibaldi, G.; Chetoni, C.; Gualtieri, F.; Forcina, F.; Bargagna, P.; Kotzalidis, G.D.; Callovini, T.; Bonito, M.; et al. The Impact of the COVID-19 Pandemic on Postpartum Maternal Mental Health. J. Pers. Med. 2023, 13, 56. https://doi.org/10.3390/jpm13010056
De Chiara L, Angeletti G, Anibaldi G, Chetoni C, Gualtieri F, Forcina F, Bargagna P, Kotzalidis GD, Callovini T, Bonito M, et al. The Impact of the COVID-19 Pandemic on Postpartum Maternal Mental Health. Journal of Personalized Medicine. 2023; 13(1):56. https://doi.org/10.3390/jpm13010056
Chicago/Turabian StyleDe Chiara, Lavinia, Gloria Angeletti, Gaia Anibaldi, Chiara Chetoni, Flavia Gualtieri, Francesca Forcina, Paride Bargagna, Georgios Demetrios Kotzalidis, Tommaso Callovini, Marco Bonito, and et al. 2023. "The Impact of the COVID-19 Pandemic on Postpartum Maternal Mental Health" Journal of Personalized Medicine 13, no. 1: 56. https://doi.org/10.3390/jpm13010056