
Urine-Based Detection of Biomarkers Indicative of Chronic Kidney Disease in a Patient Cohort from Ghana
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Cytokine Assay Experiments
2.3. Image Analysis of Cytokine Assays
2.4. Data Analysis of Cytokine Assays
3. Results
3.1. Patient Characteristics
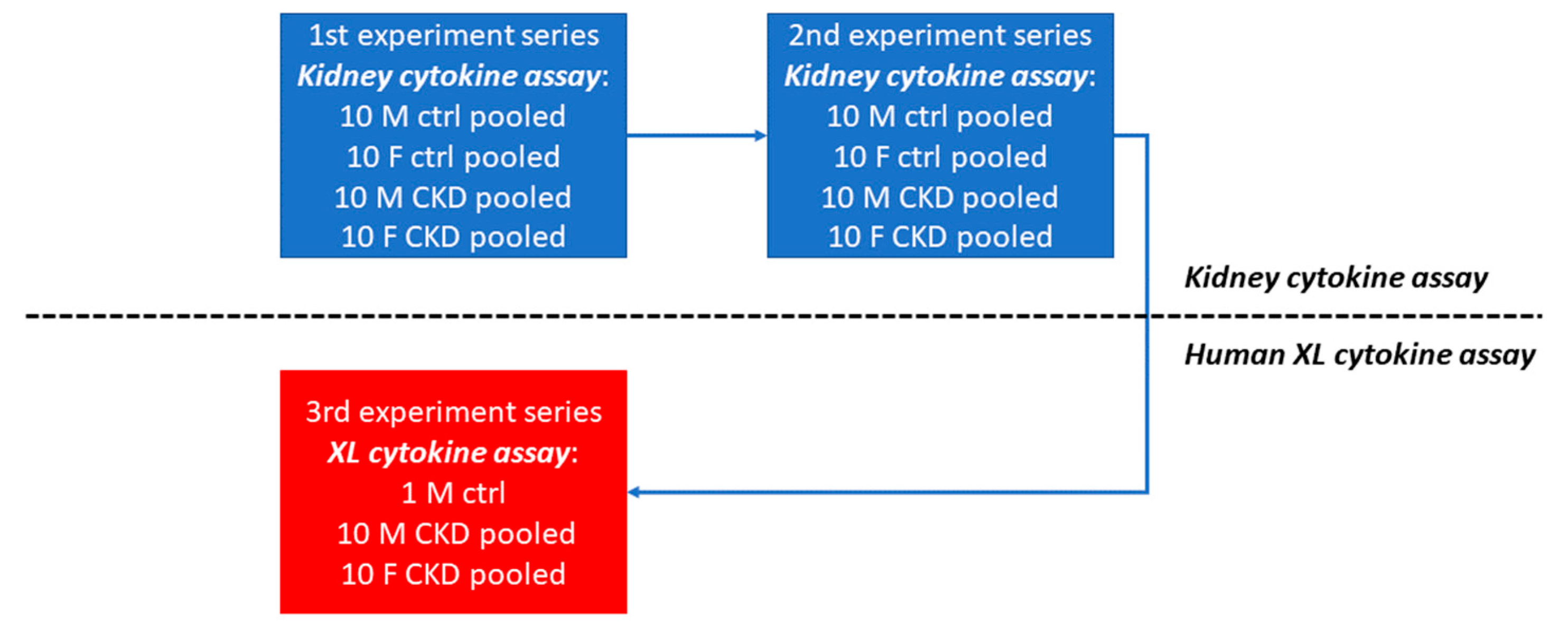
3.2. Strategy for the Identification of CKD Markers
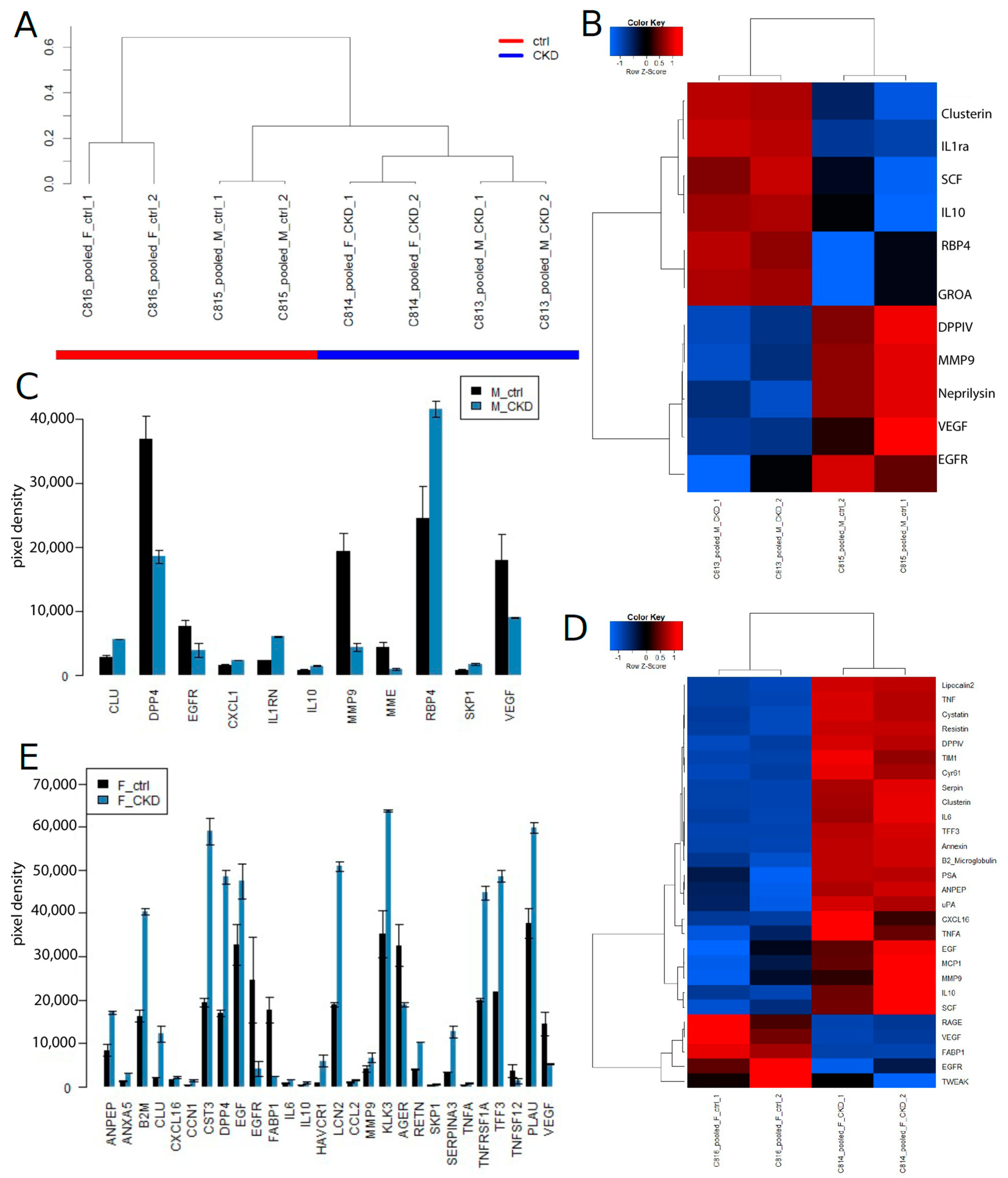
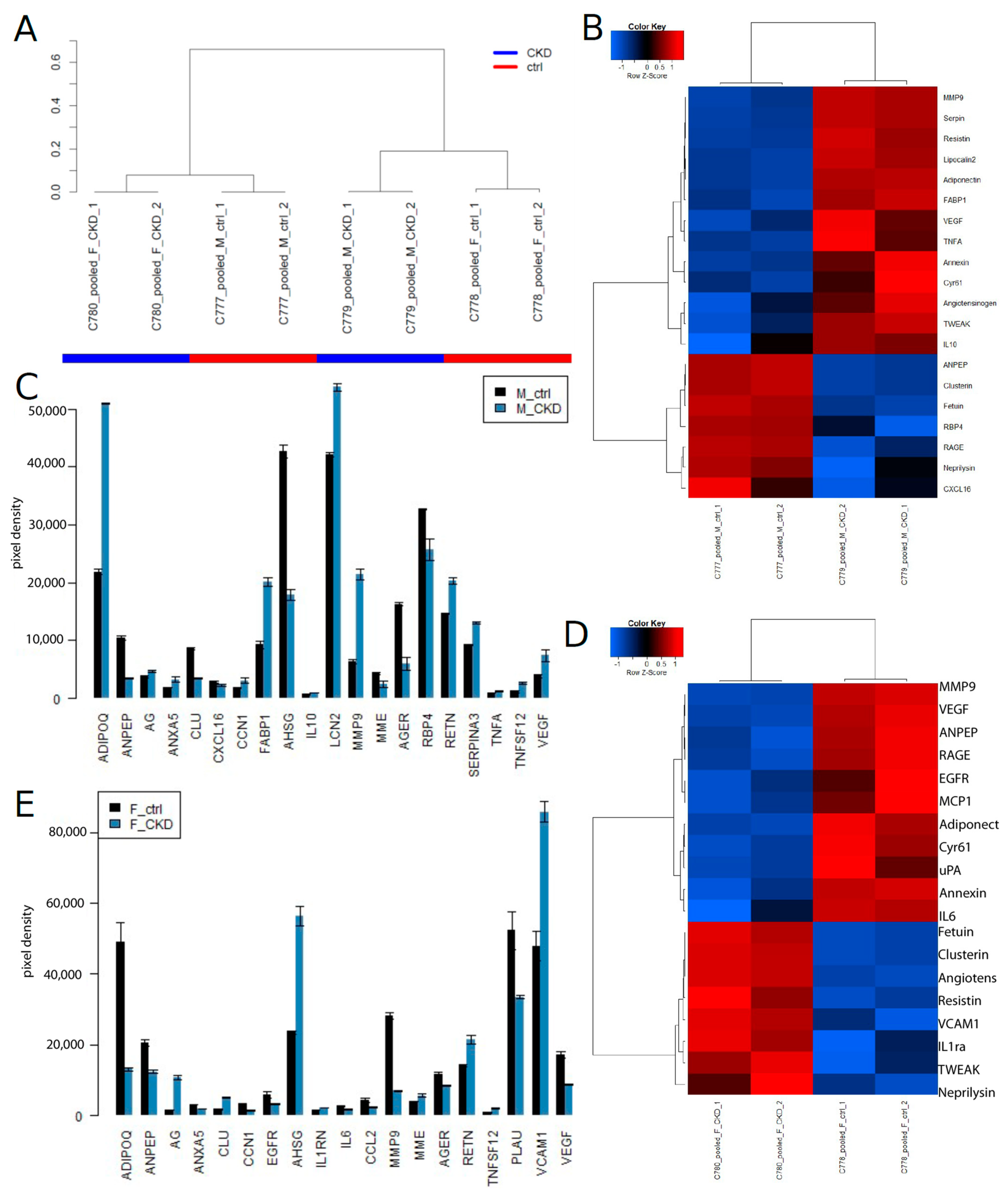
3.3. Identification of CKD Biomarkers Using the Human Kidney Biomarker Array
3.4. Summary of the Identified CKD Biomarkers in Experiment Series 1 and 2
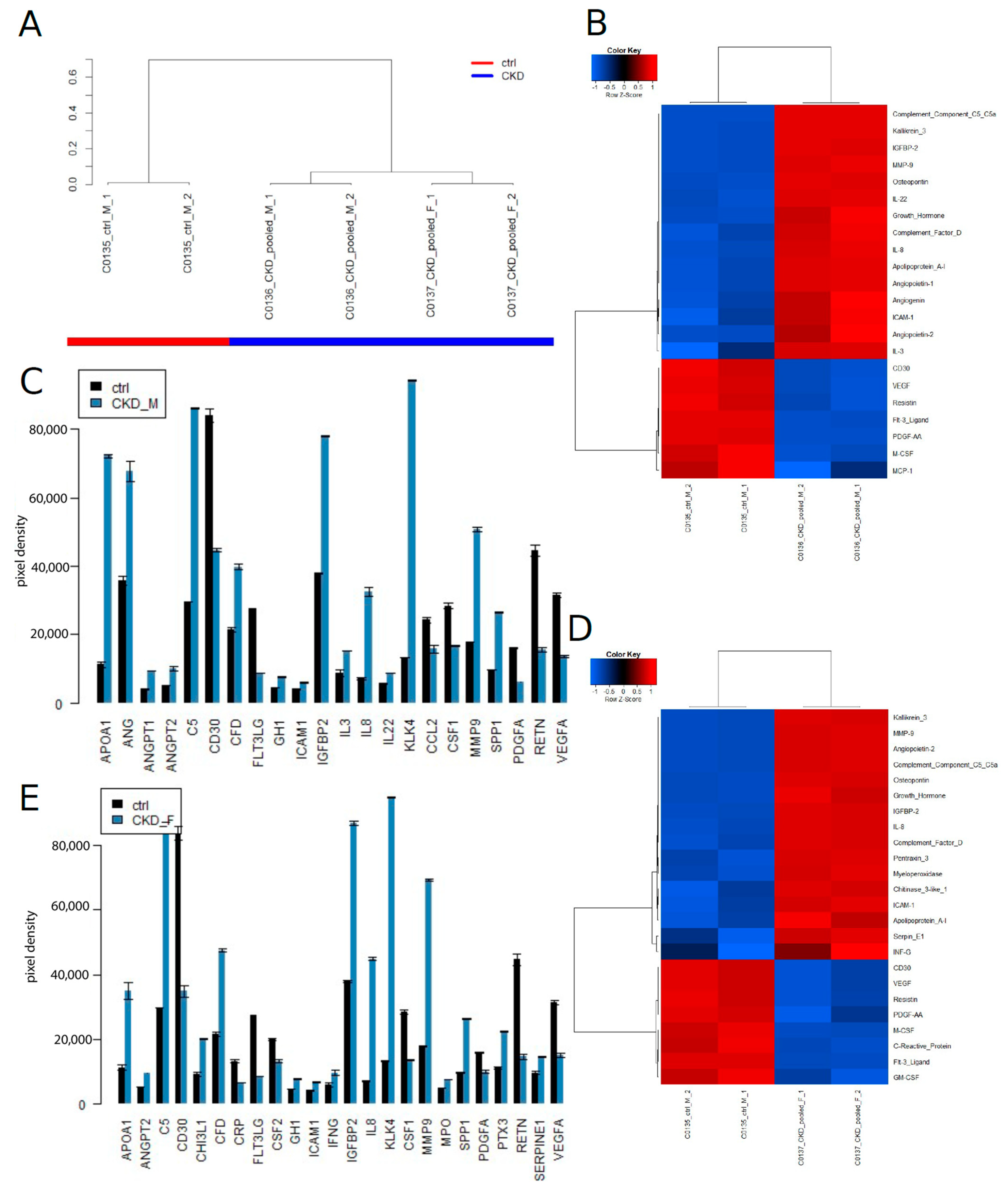
3.5. Identification of CKD Biomarkers on the Human XL Cytokine Assay
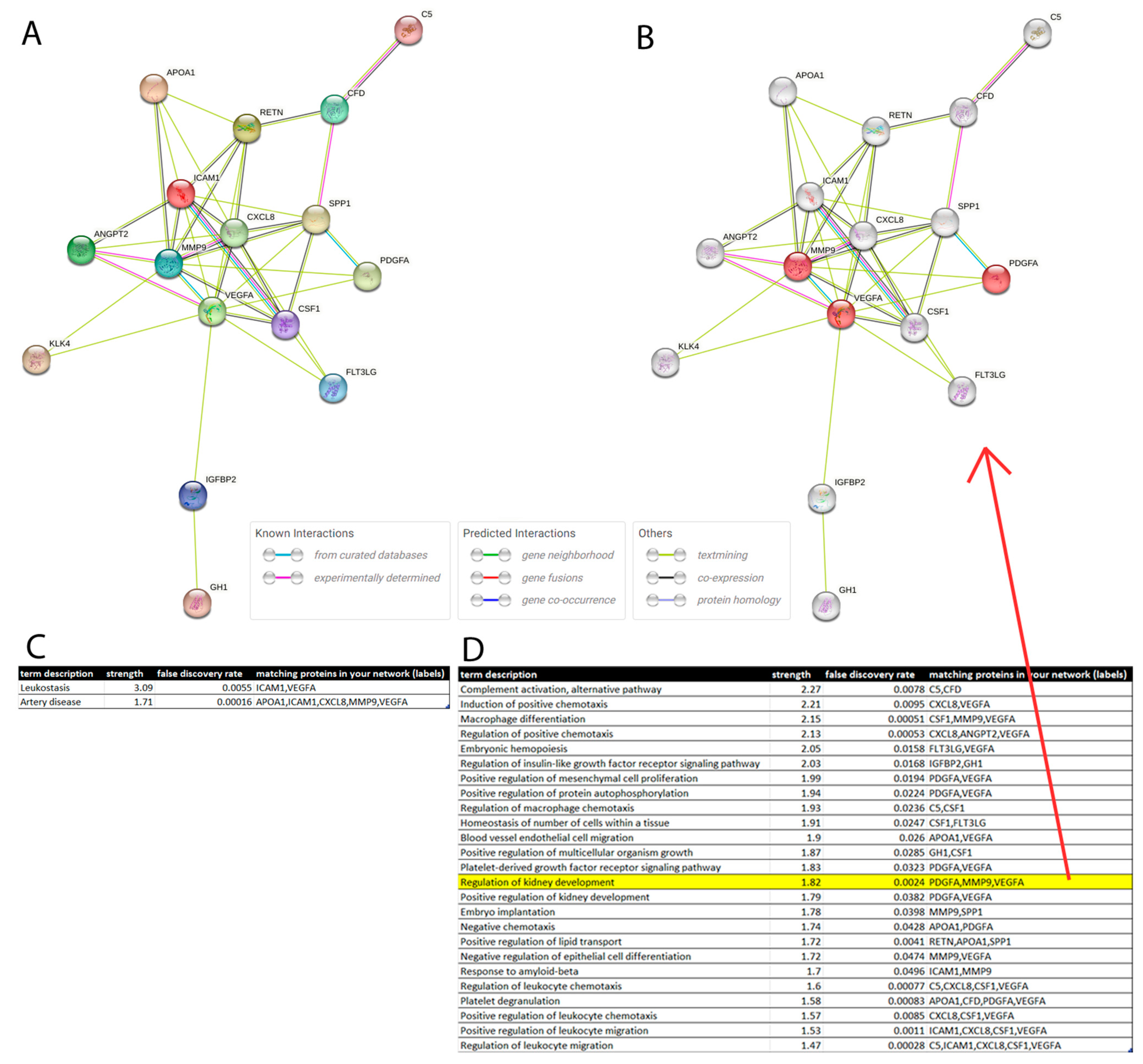
3.6. Protein Interaction Network
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Levey, A.S.; Coresh, J. Chronic Kidney Disease. Lancet 2012, 379, 165–180. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Coresh, J.; Balk, E.; Kausz, A.T.; Levin, A.; Steffes, M.W.; Hogg, R.J.; Perrone, R.D.; Lau, J.; Eknoyan, G.; et al. National Kidney Foundation Practice Guidelines for Chronic Kidney Disease: Evaluation, Classification, and Stratification. Ann. Intern. Med. 2003, 139, 137–147. [Google Scholar] [CrossRef]
- D’Amico, G.; Bazzi, C. Pathophysiology of Proteinuria. Kidney Int. 2003, 63, 809–825. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schena, F.P.; Gesualdo, L. Pathogenetic Mechanisms of Diabetic Nephropathy. J. Am. Soc. Nephrol. 2005, 16, S30–S33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Webster, A.C.; Nagler, E.V.; Morton, R.L.; Masson, P. Chronic Kidney Disease. Lancet 2017, 389, 1238–1252. [Google Scholar] [CrossRef]
- Remuzzi, G. Mechanisms of Progression and Regression of Renal Lesions of Chronic Nephropathies and Diabetes. J. Clin. Investig. 2006, 116, 288–296. [Google Scholar] [CrossRef] [Green Version]
- The Diabetes Control and Complications (DCCT) Research Group. Effect of Intensive Therapy on the Development and Progression of Diabetic Nephropathy in the Diabetes Control and Complications Trial. Kidney Int. 1995, 47, 1703–1720. [Google Scholar] [CrossRef] [Green Version]
- Dronavalli, S.; Duka, I.; Bakris, G.L. The Pathogenesis of Diabetic Nephropathy. Nat. Clin. Pract. Endocrinol. Metab. 2008, 4, 444–452. [Google Scholar] [CrossRef]
- D’Agati, V.D.; Kaskel, F.J.; Falk, R.J. Focal Segmental Glomerulosclerosis. N. Engl. J. Med. 2011, 365, 2398–2411. [Google Scholar] [CrossRef] [Green Version]
- Cobo, G.; Hecking, M.; Port, F.K.; Exner, I.; Lindholm, B.; Stenvinkel, P.; Carrero, J.J. Sex and Gender Differences in Chronic Kidney Disease: Progression to End-Stage Renal Disease and Haemodialysis. Clin. Sci. 2016, 130, 1147–1163. [Google Scholar] [CrossRef]
- Iseki, K. Gender Differences in Chronic Kidney Disease. Kidney Int. 2008, 74, 415–417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carrero, J.J. Gender Differences in Chronic Kidney Disease: Underpinnings and Therapeutic Implications. Kidney Blood Press. Res. 2010, 33, 383–392. [Google Scholar] [CrossRef] [PubMed]
- Goek, O.-N.; Döring, A.; Gieger, C.; Heier, M.; Koenig, W.; Prehn, C.; Römisch-Margl, W.; Wang-Sattler, R.; Illig, T.; Suhre, K.; et al. Serum Metabolite Concentrations and Decreased GFR in the General Population. Am. J. Kidney Dis. 2012, 60, 197–206. [Google Scholar] [CrossRef]
- Saulnier, P.-J.; Darshi, M.; Wheelock, K.M.; Looker, H.C.; Fufaa, G.D.; Knowler, W.C.; Weil, E.J.; Tanamas, S.K.; Lemley, K.V.; Saito, R.; et al. Urine Metabolites Are Associated with Glomerular Lesions in Type 2 Diabetes. Metabolomics 2018, 14, 84. [Google Scholar] [CrossRef] [PubMed]
- Posada-Ayala, M.; Zubiri, I.; Martin-Lorenzo, M.; Sanz-Maroto, A.; Molero, D.; Gonzalez-Calero, L.; Fernandez-Fernandez, B.; de la Cuesta, F.; Laborde, C.M.; Barderas, M.G.; et al. Identification of a Urine Metabolomic Signature in Patients with Advanced-Stage Chronic Kidney Disease. Kidney Int. 2014, 85, 103–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abbasi, F.; Moosaie, F.; Khaloo, P.; Firouzabadi, F.D.; Abhari, S.M.F.; Atainia, B.; Ardeshir, M.; Nakhjavani, M.; Esteghamati, A. Neutrophil Gelatinase-Associated Lipocalin and Retinol-Binding Protein-4 as Biomarkers for Diabetic Kidney Disease. Kidney Blood Press. Res. 2020, 45, 222–232. [Google Scholar] [CrossRef]
- Peralta, C.A.; Katz, R.; Bonventre, J.V.; Sabbisetti, V.; Siscovick, D.; Sarnak, M.; Shlipak, M.G. Associations of Urinary Levels of Kidney Injury Molecule 1 (KIM-1) and Neutrophil Gelatinase-Associated Lipocalin (NGAL) with Kidney Function Decline in the Multi-Ethnic Study of Atherosclerosis (MESA). Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2012, 60, 904–911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feldreich, T.; Carlsson, A.C.; Helmersson-Karlqvist, J.; Risérus, U.; Larsson, A.; Lind, L.; Ärnlöv, J. Urinary Osteopontin Predicts Incident Chronic Kidney Disease, While Plasma Osteopontin Predicts Cardiovascular Death in Elderly Men. Cardiorenal Med. 2017, 7, 245–254. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.-C.; Zhang, L.; Lv, L.-L.; Wang, Y.; Liu, D.; Zhang, X. Application of Antibody Array Technology in the Analysis of Urinary Cytokine Profiles in Patients with Chronic Kidney Disease. Am. J. Nephrol. 2006, 26, 483–490. [Google Scholar] [CrossRef]
- Schwartz, G.J.; Muñoz, A.; Schneider, M.F.; Mak, R.H.; Kaskel, F.; Warady, B.A.; Furth, S.L. New Equations to Estimate GFR in Children with CKD. J. Am. Soc. Nephrol. JASN 2009, 20, 629–637. [Google Scholar] [CrossRef]
- Madhavan, S.M.; O’Toole, J.F. The Biology of APOL1 with Insights into the Association between APOL1 Variants and Chronic Kidney Disease. Clin. Exp. Nephrol. 2013, 18, 238–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneider, C.A.; Rasband, W.S.; Eliceiri, K.W. NIH Image to ImageJ: 25 Years of Image Analysis. Nat. Methods 2012, 9, 671–675. [Google Scholar] [CrossRef]
- Steinfath, M.; Wruck, W.; Seidel, H.; Lehrach, H.; Radelof, U.; O’Brien, J. Automated Image Analysis for Array Hybridization Experiments. Bioinformatics 2001, 17, 634–641. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gentleman, R.C.; Carey, V.J.; Bates, D.M.; Bolstad, B.; Dettling, M.; Dudoit, S.; Ellis, B.; Gautier, L.; Ge, Y.; Gentry, J.; et al. Bioconductor: Open Software Development for Computational Biology and Bioinformatics. Genome Biol. 2004, 5, R80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du, P.; Kibbe, W.A.; Lin, S.M. Lumi: A Pipeline for Processing Illumina Microarray. Bioinformatics 2008, 24, 1547–1548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smyth, G.K. Linear Models and Empirical Bayes Methods for Assessing Differential Expression in Microarray Experiments. Stat. Appl. Genet. Mol. Biol. 2004, 3, 1–25. [Google Scholar] [CrossRef]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. J. R. Stat. Soc. Ser. B Methodol. 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Warnes, G.R.; Bolker, B.; Bonebakker, L.; Gentleman, R.; Liaw, W.H.A.; Lumley, T.; Maechler, M.; Magnusson, A.; Moeller, S.; Schwartz, M.; et al. Gplots: Various R Programming Tools for Plotting Data. R Package Ver. 2015. [Google Scholar]
- Galili, T. Dendextend: An R Package for Visualizing, Adjusting and Comparing Trees of Hierarchical Clustering. Bioinforma. Oxf. Engl. 2015, 31, 3718–3720. [Google Scholar] [CrossRef] [Green Version]
- Levey, A.S.; Becker, C.; Inker, L.A. Glomerular Filtration Rate and Albuminuria for Detection and Staging of Acute and Chronic Kidney Disease in Adults: A Systematic Review. JAMA 2015, 313, 837–846. [Google Scholar] [CrossRef] [Green Version]
- Szklarczyk, D.; Franceschini, A.; Wyder, S.; Forslund, K.; Heller, D.; Huerta-Cepas, J.; Simonovic, M.; Roth, A.; Santos, A.; Tsafou, K.P.; et al. STRING V10: Protein-Protein Interaction Networks, Integrated over the Tree of Life. Nucleic Acids Res. 2015, 43, D447–D452. [Google Scholar] [CrossRef] [PubMed]
- Cañadas-Garre, M.; Anderson, K.; Cappa, R.; Skelly, R.; Smyth, L.J.; McKnight, A.J.; Maxwell, A.P. Genetic Susceptibility to Chronic Kidney Disease–Some More Pieces for the Heritability Puzzle. Front. Genet. 2019, 10, 453. [Google Scholar] [CrossRef] [PubMed]
- Abeysekera, R.A.; Healy, H.G.; Wang, Z.; Cameron, A.L.; Hoy, W.E. Heterogeneity in Patterns of Progression of Chronic Kidney Disease. Intern. Med. J. 2021, 51, 220–228. [Google Scholar] [CrossRef] [PubMed]
- Mårtensson, J.; Bellomo, R. The Rise and Fall of NGAL in Acute Kidney Injury. Blood Purif. 2014, 37, 304–310. [Google Scholar] [CrossRef]
- Sinuani, I.; Beberashvili, I.; Averbukh, Z.; Sandbank, J. Role of IL-10 in the Progression of Kidney Disease. World J. Transplant. 2013, 3, 91–98. [Google Scholar] [CrossRef]
- Zhang, D.; Gu, T.; Forsberg, E.; Efendic, S.; Brismar, K.; Gu, H.F. Genetic and Functional Effects of Membrane Metalloendopeptidase on Diabetic Nephropathy Development. Am. J. Nephrol. 2011, 34, 483–490. [Google Scholar] [CrossRef]
- Fritz, I.B.; Murphy, B. Clusterin Insights into a Multifunctional Protein. Trends Endocrinol. Metab. TEM 1993, 4, 41–45. [Google Scholar] [CrossRef]
- Rogulska, K.; Wojciechowska-Koszko, I.; Dołęgowska, B.; Kwiatkowska, E.; Roszkowska, P.; Kapczuk, P.; Kosik-Bogacka, D. The Most Promising Biomarkers of Allogeneic Kidney Transplant Rejection. J. Immunol. Res. 2022, 2022, 6572338. [Google Scholar] [CrossRef]
- Guo, J.; Guan, Q.; Liu, X.; Wang, H.; Gleave, M.E.; Nguan, C.Y.C.; Du, C. Relationship of Clusterin with Renal Inflammation and Fibrosis after the Recovery Phase of Ischemia-Reperfusion Injury. BMC Nephrol. 2016, 17, 133. [Google Scholar] [CrossRef] [Green Version]
- Axelsson, J.; Bergsten, A.; Qureshi, A.R.; Heimbürger, O.; Bárány, P.; Lönnqvist, F.; Lindholm, B.; Nordfors, L.; Alvestrand, A.; Stenvinkel, P. Elevated Resistin Levels in Chronic Kidney Disease Are Associated with Decreased Glomerular Filtration Rate and Inflammation, but Not with Insulin Resistance. Kidney Int. 2006, 69, 596–604. [Google Scholar] [CrossRef] [Green Version]
- Curran, C.S.; Kopp, J.B. RAGE Pathway Activation and Function in Chronic Kidney Disease and COVID-19. Front. Med. 2022, 9, 970423. [Google Scholar] [CrossRef] [PubMed]
- Rayego-Mateos, S.; Rodrigues-Diez, R.; Morgado-Pascual, J.L.; Valentijn, F.; Valdivielso, J.M.; Goldschmeding, R.; Ruiz-Ortega, M. Role of Epidermal Growth Factor Receptor (EGFR) and Its Ligands in Kidney Inflammation and Damage. Mediat. Inflamm. 2018, 2018, 8739473. [Google Scholar] [CrossRef] [Green Version]
- Sabolić, I.; Asif, A.R.; Budach, W.E.; Wanke, C.; Bahn, A.; Burckhardt, G. Gender Differences in Kidney Function. Pflüg. Arch.-Eur. J. Physiol. 2007, 455, 397–429. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Z.; Limbu, M.H.; Wang, Z.; Liu, J.; Liu, L.; Zhang, X.; Chen, P.; Liu, B. MMP-2 and 9 in Chronic Kidney Disease. Int. J. Mol. Sci. 2017, 18, 776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schrijvers, B.F.; Flyvbjerg, A.; De Vriese, A.S. The Role of Vascular Endothelial Growth Factor (VEGF) in Renal Pathophysiology. Kidney Int. 2004, 65, 2003–2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimada, K.; Baba, T.; Neugebauer, S.; Onozaki, A.; Yamada, D.; Midorikawa, S.; Sato, W.; Watanabe, T. Plasma Vascular Endothelial Growth Factor in Japanese Type 2 Diabetic Patients with and without Nephropathy. J. Diabetes Complicat. 2002, 16, 386–390. [Google Scholar] [CrossRef]
- Köttgen, A.; Pattaro, C.; Böger, C.A.; Fuchsberger, C.; Olden, M.; Glazer, N.L.; Parsa, A.; Gao, X.; Yang, Q.; Smith, A.V.; et al. New Loci Associated with Kidney Function and Chronic Kidney Disease. Nat. Genet. 2010, 42, 376–384. [Google Scholar] [CrossRef] [Green Version]
- Böger, C.A.; Gorski, M.; Li, M.; Hoffmann, M.M.; Huang, C.; Yang, Q.; Teumer, A.; Krane, V.; O’Seaghdha, C.M.; Kutalik, Z.; et al. Association of EGFR-Related Loci Identified by GWAS with Incident CKD and ESRD. PLoS Genet. 2011, 7, e1002292. [Google Scholar] [CrossRef] [Green Version]
- Lousa, I.; Reis, F.; Beirão, I.; Alves, R.; Belo, L.; Santos-Silva, A. New Potential Biomarkers for Chronic Kidney Disease Management—A Review of the Literature. Int. J. Mol. Sci. 2020, 22, 43. [Google Scholar] [CrossRef]
- Levey, A.S.; Perrone, R.D.; Madias, N.E. Serum Creatinine and Renal Function. Annu. Rev. Med. 1988, 39, 465–490. [Google Scholar] [CrossRef]
- Coresh, J.; Selvin, E.; Stevens, L.A.; Manzi, J.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Levey, A.S. Prevalence of Chronic Kidney Disease in the United States. JAMA 2007, 298, 2038–2047. [Google Scholar] [CrossRef] [PubMed]
- Kodgirwar, P.S.; Jajoo, S.U.; Jajoo, U.N.; Taksande, B.A.; Gupta, S.S. Nonalbuminuric Chronic Kidney Disease: A Dominant Presentation in Noncommunicable Disease Population of Rural Central India. J. Fam. Med. Prim. Care 2018, 7, 442–446. [Google Scholar] [CrossRef]
- Koye, D.N.; Magliano, D.J.; Reid, C.M.; Jepson, C.; Feldman, H.I.; Herman, W.H.; Shaw, J.E. Risk of Progression of Nonalbuminuric CKD to End-Stage Kidney Disease in People with Diabetes: The CRIC (Chronic Renal Insufficiency Cohort) Study. Am. J. Kidney Dis. 2018, 72, 653–661. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group 1 | |||||||||||||||
| Control female | Control male | CKD female | CKD male | ||||||||||||
| Age | eGFR (mL/min per 1-73 m²) | number | Albumine creatine ratio (g/mmol) | Age | eGFR (mL/min per 1-73 m²) | number | Albumine creatine ratio (g/mmol) | Age | eGFR (mL/min per 1-73 m²) | number | Albumine creatine ratio (g/mmol) | Age | eGFR (mL/min per 1-73 m²) | number | Albumine creatine ratio (g/mmol) |
| 39 | 169.45 | 52815 | 0.68 | 11 | 70.77 | 52803 | 0.4 | 69 | 3 | 52866 | 107.25 | 24 | 84.05 | 52852 | 123.34 |
| 39 | 94.85 | 21206 | 1.11 | 26 | 153.98 | 52833 | 1.6 | 28 | 29 | 21245 | 8.27 | 41 | 123.38 | 52840 | 10.61 |
| 46 | 131.85 | 52855 | 0.85 | 46 | 92.64 | 52856 | 0.95 | 65 | 49 | 52838 | 1.67 | 28 | 153.97 | 52829 | 1925.38 |
| 47 | 145.27 | 52805 | 0.47 | 47 | 120.56 | 52839 | 1.06 | 49 | 51 | 52973 | 30.68 | 25 | 181.34 | 52830 | 17.89 |
| 20 | 134.71 | 21227 | 0.81 | 47 | 85.62 | 52839 | 1.06 | 38 | 75 | 52845 | 13.79 | 48 | 11.04 | 52842 | 2.69 |
| 24 | 74.53 | 21246 | 0.51 | 57 | 160.36 | 52777 | 1.03 | 39 | 92 | 21240 | 119.93 | 47 | 30.99 | 52875 | 0.91 |
| 25 | 113.26 | 21216 | 0.19 | 57 | 136.93 | 52823 | 0.48 | 25 | 93 | 52854 | 3.76 | 48 | 11.04 | 52842 | 2.69 |
| 70 | 134.61 | 52778 | 0.3 | 66 | 145.09 | 52818 | 0.67 | 35 | 99 | 21244 | 11.23 | 60 | 22.58 | 52828 | 87.79 |
| 51 | 150.26 | 52757 | 0.32 | 67 | 83.58 | 21241 | 0.36 | 46 | 114 | 52827 | 141.83 | 60 | 54.94 | 52862 | 3.05 |
| 50 | 119.12 | 21225 | 0.35 | 68 | 102.38 | 52861 | 1.71 | 60 | 123 | 52871 | 82.99 | 65 | 4.95 | 52832 | 0.54 |
| Group 2 | |||||||||||||||
| Control female | Control male | CKD female | CKD male | ||||||||||||
| Age | eGFR (mL/min per 1-73 m²) | number | Albumine creatine ratio (g/mmol) | Age | eGFR (mL/min per 1-73 m²) | number | Albumine creatine ratio (g/mmol) | Age | eGFR (mL/min per 1-73 m²) | number | Albumine creatine ratio (g/mmol) | Age | eGFR (mL/min per 1-73 m²) | number | Albumine creatine ratio (g/mmol) |
| 33 | 185.43 | 52768 | 1.32 | 17 | 72.7 | 21210 | 0.26 | 65 | 1 | 52865 | 0.68 | 22 | 157.26 | 52843 | 2.55 |
| 4 | 85.97 | 52811 | 0.71 | 18 | 83.16 | 21223 | 2.02 | 22 | 3 | 52877 | 0.62 | 24 | 19.68 | 52844 | 0.97 |
| 14 | 92.56 | 21213 | 0.52 | 21 | 165.3 | 21232 | 1.24 | 71 | 11 | 52834 | 0.91 | 28 | 5.37 | 52864 | 5.03 |
| 16 | 75.12 | 21214 | 0.37 | 24 | 153.06 | 21212 | 0.26 | 7 | 14 | 21237 | 0.68 | 33 | 194.92 | 52831 | 10 |
| 16 | 68.11 | 52812 | 2.51 | 33 | 217.41 | 52804 | 1.21 | 30 | 17 | 52859 | 1.04 | 35 | 24.3 | 52873 | 1.2 |
| 18 | 78.64 | 21231 | 0.86 | 37 | 151.17 | 21235 | 0.88 | 50 | 26 | 21238 | 0.6 | 37 | 13.96 | 52870 | 1.08 |
| 20 | 129.93 | 21229 | 0.76 | 48 | 123.11 | 21243 | 1.14 | 71 | 35 | 52867 | 0.53 | 39 | 5.92 | 21248 | 2.08 |
| 27 | 140.59 | 21218 | 1.92 | 49 | 68.92 | 52728 | 0.52 | 62 | 41 | 21249 | 2.78 | 39 | 8.5 | 52879 | 0.57 |
| 62 | 153.39 | 52825 | 1.84 | 59 | 85.61 | 52759 | 0.89 | 28 | 46 | 52857 | 46.4 | 44 | 5.15 | 52835 | 4.33 |
| 21 | 91.94 | 21217 | 0.78 | 63 | 87.59 | 52772 | 1.36 | 35 | 17 | 52858 | 7.2 | 59 | 3.07 | 52869 | 0.51 |
| Cytokine | CKD_M_ExpSeries1 | CKD_M_ExpSeries2 |
|---|---|---|
| ADIPOQ | up | |
| AG | up | |
| AGER | down | |
| AHSG | down | |
| ANPEP | down | |
| ANXA5 | up | |
| CCN1 | up | |
| CLU | up | down |
| CXCL1 | up | |
| CXCL16 | down | |
| DPP4 | down | |
| EGFR | down | |
| FABP1 | up | |
| IL1RN | up | |
| IL10 | up | up |
| LCN2 | up | |
| MME | down | down |
| MMP9 | down | up |
| RBP4 | up | down |
| RETN | up | |
| SERPINA3 | up | |
| SKP1 | up | |
| TNFA | up | |
| TNFSF12 | up | |
| VEGF | down | up |
| Cytokine | CKD_F_ExpSeries1 | CKD_F_ExpSeries2 |
|---|---|---|
| ADIPOQ | down | |
| AG | up | |
| AGER | down | down |
| AHSG | up | |
| ANPEP | up | down |
| ANXA5 | up | down |
| B2M | up | |
| CCL2 | up | down |
| CCN1 | up | down |
| CLU | up | up |
| CST3 | up | |
| CXCL16 | up | |
| DPP4 | up | |
| EGF | up | |
| EGFR | down | down |
| FABP1 | down | |
| IL1RN | up | |
| IL6 | up | down |
| IL10 | up | |
| HAVCR1 | up | |
| KLK3 | up | |
| LCN2 | up | |
| MME | up | |
| MMP9 | up | down |
| PLAU | up | down |
| RETN | up | up |
| SERPINA3 | up | |
| SKP1 | up | |
| TNFA | up | |
| TNFSF12 | up | |
| TNFRSF1A | up | |
| TTF3 | up | |
| VCAM1 | up | |
| VEGF | down | down |
| Cytokine | CKD_mean_M_F_ExpSeries3 | CKD_M_ExpSeries3 | CKD_F_ExpSeries3 |
|---|---|---|---|
| APOA1 | up | up | up |
| ANG | up | ||
| ANGPT1 | up | ||
| ANGPT2 | up | up | up |
| C5 | up | up | up |
| CD3 | down | down | |
| CHI3L1 | up | up | |
| CFD | up | up | up |
| CRP | down | down | |
| FLT3LG | down | down | down |
| CSF2 | down | down | |
| GH1 | up | up | up |
| ICAM1 | up | up | up |
| IFNG | up | up | |
| IGFBP2 | up | up | up |
| IL3 | up | ||
| IL8 | up | up | up |
| IL22 | up | ||
| KLK4 | up | up | up |
| CCL2 | down | ||
| CSF1 | down | down | down |
| MMP9 | up | up | up |
| MPO | up | up | |
| SPP1 | up | up | up |
| PDGFA | down | down | down |
| PTX3 | up | up | |
| RETN | down | down | down |
| SERPINE1 | up | up | |
| VEGFA | down | down | down |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wruck, W.; Boima, V.; Erichsen, L.; Thimm, C.; Koranteng, T.; Kwakyi, E.; Antwi, S.; Adu, D.; Adjaye, J. Urine-Based Detection of Biomarkers Indicative of Chronic Kidney Disease in a Patient Cohort from Ghana. J. Pers. Med. 2023, 13, 38. https://doi.org/10.3390/jpm13010038
Wruck W, Boima V, Erichsen L, Thimm C, Koranteng T, Kwakyi E, Antwi S, Adu D, Adjaye J. Urine-Based Detection of Biomarkers Indicative of Chronic Kidney Disease in a Patient Cohort from Ghana. Journal of Personalized Medicine. 2023; 13(1):38. https://doi.org/10.3390/jpm13010038
Chicago/Turabian StyleWruck, Wasco, Vincent Boima, Lars Erichsen, Chantelle Thimm, Theresa Koranteng, Edward Kwakyi, Sampson Antwi, Dwomoa Adu, and James Adjaye. 2023. "Urine-Based Detection of Biomarkers Indicative of Chronic Kidney Disease in a Patient Cohort from Ghana" Journal of Personalized Medicine 13, no. 1: 38. https://doi.org/10.3390/jpm13010038