
The Use of the 6MWT for Rehabilitation in Children with Cerebral Palsy: A Narrative Review
 ,
,
Abstract
:1. Introduction
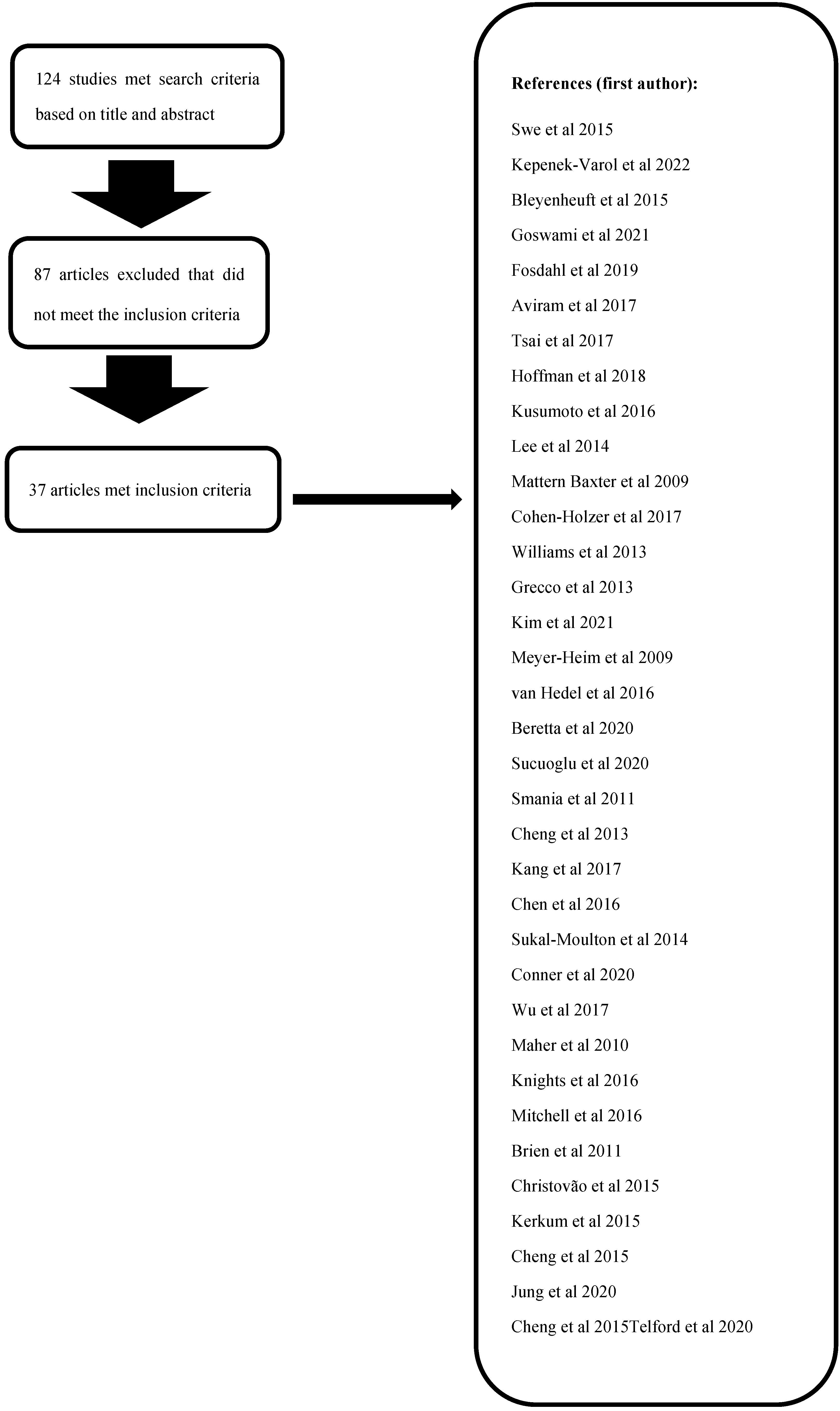
2. Methods
2.1. Search Criteria
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Data Extraction and Analysis
2.4.1. Studies Assessing Possible Changes in 6MWT in CP before/after Physiotherapy
2.4.2. Studies Assessing Possible Changes in 6MWT in CP before/after Medical or Surgical Intervention
2.4.3. Studies Assessing Possible Changes in 6MWT in CP before/after Robotics
2.4.4. Studies Assessing Possible Changes in 6MWT in CP before/after Other Types of Intervention
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Baxter, P.; Morris, C.; Rosenbaum, P.; Paneth, N.; Leviton, A.; Goldstein, M.; Bax, M.; Colver, A.; Damiano, D.; Graham, H.K.; et al. The definition and classification of cerebral palsy. Dev. Med. Child Neurol. 2007, 49 (Suppl. 109), 1–44. [Google Scholar]
- Thompson, P.; Beath, T.; Bell, J.; Jacobson, G.; Phair, T.; Salbach, N.M.; Wright, F.V. Test-retest reliability of the 10-metre fast walk test and 6-minute walk test in ambulatory school-aged children with cerebral palsy. Dev. Med. Child Neurol. 2008, 50, 370–376. [Google Scholar] [CrossRef]
- Novak, I.; Morgan, C.; Adde, L.; Blackman, J.; Boyd, R.N.; Brunstrom-Hernandez, J.; Cioni, G.; Damiano, D.; Darrah, J.; Ann-Eliasson, A.; et al. Early, Accurate Diagnosis and Early Intervention in Cerebral Palsy: Advances in Diagnosis and Treatment. JAMA Pediatr. 2017, 171, 897–907. [Google Scholar] [CrossRef]
- Morgan, C.; Fetters, L.; Adde, L.; Badawi, N.; Bancale, A.; Boyd, R.N.; Chorna, O.; Cioni, G.; Damiano, D.L.; Darrah, J.; et al. Early Intervention for Children Aged 0 to 2 Years With or at High Risk of Cerebral Palsy: International Clinical Practice Guideline Based on Systematic Reviews. JAMA Pediatr. 2021, 175, 846–858. [Google Scholar] [CrossRef] [PubMed]
- Wallard, L.; Dietrich, G.; Kerlirzin, Y.; Bredin, J. Robotic-assisted gait training improves walking abilities in diplegic children with cerebral palsy. Eur. J. Paediatr. Neurol. 2017, 21, 557–564. [Google Scholar] [CrossRef] [PubMed]
- Maghini, C.; Romei, M.; Morganti, R.; Piccinini, L.; Turconi, A.C. Robotic gait training in children affected with Cerebral Palsy: Effects on motor function, gait pattern and posture. Gait Posture 2014, 40, S8–S9. [Google Scholar] [CrossRef]
- Martakis, K.; Stark, C.; Rehberg, M.; Semler, O.; Duran, I.; Schoenau, E. Reference Centiles to Monitor the 6-minute-walk Test in Ambulant Children with Cerebral Palsy and Identification of Effects after Rehabilitation Utilizing Whole-body Vibration. Dev. Neurorehabilit. 2021, 24, 45–55. [Google Scholar] [CrossRef] [PubMed]
- Nsenga Leunkeu, A.; Shephard, R.J.; Ahmaidi, S. Six-minute walk test in children with cerebral palsy gross motor function classification system levels I and II: Reproducibility, validity, and training effects. Arch. Phys. Med. Rehabil. 2012, 93, 233. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Sullivan, M.J.; Thompson, P.J.; Fallen, E.L.; Pugsley, S.O.; Taylor, D.W.; Berman, L.B. The 6-minute walk: A new measure of exercise capacity in patients with chronic heart failure. Can. Med. Assoc. J. 1985, 132, 919–923. [Google Scholar]
- Geiger, R.; Strasak, A.; Treml, B.; Gasser, K.; Kleinsasser, A.; Fischer, V.; Geiger, H.; Loeckinger, A.; Stein, J.I. Six-minute walk test in children and adolescents. J. Pediatr. 2007, 150, 395–399. [Google Scholar] [CrossRef]
- Fitzgerald, D.; Hickey, C.; Delahunt, E.; Walsh, M.; O’Brien, T. Six-Minute Walk Test in Children With Spastic Cerebral Palsy and Children Developing Typically. Pediatr. Phys. Ther. 2016, 28, 192–199. [Google Scholar] [CrossRef]
- Swe, N.; Sendhilnnathan, S.; van Den Berg, M.; Barr, C. Over ground walking and body weight supported walking improve mobility equally in cerebral palsy: A randomized controlled trial. Clin. Rehabil. 2015, 29, 1108–1116. [Google Scholar] [CrossRef] [PubMed]
- Kepenek-Varol, B.; Gürses, H.N.; İçağasıoğlu, D.F. Effects of Inspiratory Muscle and Balance Training in Children with Hemiplegic Cerebral Palsy: A Randomized Controlled Trial. Dev. Neurorehabilit. 2022, 25, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Bleyenheuft, Y.; Arnould, C.; Brandao, M.B.; Bleyenheuft, C.; Gordon, A.M. Hand and Arm Bimanual Intensive Therapy Including Lower Extremity (HABIT-ILE) in Children With Unilateral Spastic Cerebral Palsy: A Randomized Trial. Neurorehabil. Neural Repair 2015, 29, 645–657. [Google Scholar] [CrossRef] [PubMed]
- Goswami, J.N.; Sankhyan, N.; Singhi, P. Add-on Home-Centered Activity-Based Therapy vs Conventional Physiotherapy in Improving Walking Ability at 6-Months in Children With Diplegic Cerebral Palsy: A Randomized Controlled Trial. Indian Pediatr. 2021, 58, 826–832. [Google Scholar] [CrossRef]
- Fosdahl, M.A.; Jahnsen, R.; Kvalheim, K.; Holm, I. Effect of a Combined Stretching and Strength Training Program on Gait Function in Children with Cerebral Palsy, GMFCS Level I & II: A Randomized Controlled Trial. Medicina 2019, 55, 250. [Google Scholar]
- Aviram, R.; Harries, N.; Namourah, I.; Amro, A.; Bar-Haim, S. Effects of a group circuit progressive resistance training program compared with a treadmill training program for adolescents with cerebral palsy. Dev. Neurorehabilit. 2017, 20, 347–354. [Google Scholar] [CrossRef]
- Tsai, L.C.; Ren, Y.; Gaebler-Spira, D.J.; Revivo, G.A.; Zhang, L.Q. Effects of an Off-Axis Pivoting Elliptical Training Program on Gait Function in Persons With Spastic Cerebral Palsy: A Preliminary Study. Am. J. Phys. Med. Rehabil. 2017, 96, 515–522. [Google Scholar] [CrossRef]
- Hoffman, R.M.; Corr, B.B.; Stuberg, W.A.; Arpin, D.J.; Kurz, M.J. Changes in lower extremity strength may be related to the walking speed improvements in children with cerebral palsy after gait training. Res. Dev. Disabil. 2018, 73, 14–20. [Google Scholar] [CrossRef]
- Kusumoto, Y.; Nitta, O.; Takaki, K. Impact of loaded sit-to-stand exercises at different speeds on the physiological cost of walking in children with spastic diplegia: A single-blind randomized clinical trial. Res. Dev. Disabil. 2016, 57, 85–91. [Google Scholar] [CrossRef]
- Lee, Y.S.; Kim, W.B.; Park, J.W. The effect of exercise using a sliding rehabilitation machine on the gait function of children with cerebral palsy. J. Phys. Ther. Sci. 2014, 26, 1667–1669. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mattern-Baxter, K.; Bellamy, S.; Mansoor, J.K. Effects of intensive locomotor treadmill training on young children with cerebral palsy. Pediatr. Phys. Ther. 2009, 21, 308–318. [Google Scholar] [CrossRef]
- Cohen-Holzer, M.; Sorek, G.; Schweizer, M.; Katz-Leurer, M. The influence of a constraint and bimanual training program using a variety of modalities on endurance and on the cardiac autonomic regulation system of children with unilateral cerebral palsy: A self-control clinical trial. NeuroRehabilitation 2017, 41, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Williams, S.A.; Reid, S.; Elliott, C.; Shipman, P.; Valentine, J. Muscle volume alterations in spastic muscles immediately following botulinum toxin type-A treatment in children with cerebral palsy. Dev. Med. Child Neurol. 2013, 55, 813–820. [Google Scholar] [CrossRef] [PubMed]
- Grecco, L.A.C.; de Freitas, T.; Satie, J.; Bagne, E.; Oliveira, C.S.; de Souza, D.R. Treadmill Training Following Orthopedic Surgery in Lower Limbs of Children With Cerebral Palsy. Pediatr. Phys. Ther. 2013, 25, 187–192. [Google Scholar] [CrossRef]
- Kim, S.K.; Park, D.; Yoo, B.; Shim, D.; Choi, J.O.; Choi, T.Y.; Park, E.S. Overground Robot-Assisted Gait Training for Pediatric Cerebral Palsy. Sensors 2021, 21, 2087. [Google Scholar] [CrossRef]
- Meyer-Heim, A.; Ammann-Reiffer, C.; Schmartz, A.; Schäfer, J.; Sennhauser, F.H.; Heinen, F.; Knecht, B.; Dabrowski, E.; Borggraefe, I. Improvement of walking abilities after robotic-assisted locomotion training in children with cerebral palsy. Arch. Dis. Child. 2009, 94, 615–620. [Google Scholar] [CrossRef] [Green Version]
- van Hedel, H.J.A.; Meyer-Heim, A.; Rüsch-Bohtz, C. Robot-assisted gait training might be beneficial for more severely affected children with cerebral palsy. Dev. Neurorehabilit. 2016, 19, 410–415. [Google Scholar] [CrossRef]
- Beretta, E.; Storm, F.A.; Strazzer, S.; Frascarelli, F.; Petrarca, M.; Colazza, A.; Cordone, G.; Biffi, E.; Morganti, R.; Maghini, C.; et al. Effect of Robot-Assisted Gait Training in a Large Population of Children With Motor Impairment Due to Cerebral Palsy or Acquired Brain Injury. Arch. Phys. Med. Rehabil. 2020, 101, 106–112. [Google Scholar] [CrossRef] [Green Version]
- Sucuoglu, H. Effects of robot-assisted gait training alongside conventional therapy on the development of walking in children with cerebral palsy. J. Pediatr. Rehabil. Med. 2020, 13, 127–135. [Google Scholar] [CrossRef]
- Smania, N.; Bonetti, P.; Gandolfi, M.; Cosentino, A.; Waldner, A.; Hesse, S.; Werner, C.; Bisoffi, G.; Geroin, C.; Munari, D. Improved Gait After Repetitive Locomotor Training in Children with Cerebral Palsy. Am. J. Phys. Med. Rehabil. 2011, 90, 137–149. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.Y.K.; Ju, Y.Y.; Chen, C.L.; Chang, Y.J.; Wong, A.M.K. Managing lower extremity muscle tone and function in children with cerebral palsy via eight-week repetitive passive knee movement intervention. Res. Dev. Disabil. 2013, 34, 554–561. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.; Martelli, D.; Vashista, V.; Martinez-Hernandez, I.; Kim, H.; Agrawal, S.K. Robot-driven downward pelvic pull to improve crouch gait in children with cerebral palsy. Sci. Robot. 2017, 2, eaan2634. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.; Wu, Y.N.; Ren, Y.; Liu, L.; Gaebler-Spira, D.; Tankard, K.; Lee, J.; Song, W.; Wang, M.; Zhang, L.Q. Home-Based Versus Laboratory-Based Robotic Ankle Training for Children With Cerebral Palsy: A Pilot Randomized Comparative Trial. Arch. Phys. Med. Rehabil. 2016, 97, 1237–1243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sukal-Moulton, T.; Clancy, T.; Zhang, L.Q.; Gaebler-Spira, D. Clinical application of a robotic ankle training program for cerebral palsy compared to the research laboratory application: Does it translate to practice? Arch. Phys. Med. Rehabil. 2014, 95, 1433–1440. [Google Scholar] [CrossRef] [Green Version]
- Conner, B.C.; Remec, N.M.; Orum, E.K.; Frank, E.M.; Lerner, Z.F. Wearable Adaptive Resistance Training Improves Ankle Strength, Walking Efficiency and Mobility in Cerebral Palsy: A Pilot Clinical Trial. IEEE Open J. Eng. Med. Biol. 2020, 1, 282–289. [Google Scholar] [CrossRef]
- Wu, M.; Kim, J.; Arora, P.; Gaebler-Spira, D.J.; Zhang, Y. Effects of the integration of dynamic weight shifting training into treadmill training on walking function of children with cerebral palsy: A randomized controlled study. Am. J. Phys. Med. Rehabil. 2017, 96, 765–772. [Google Scholar] [CrossRef]
- Maher, C.A.; Williams, M.T.; Olds, T.; Lane, A.E. An internet-based physical activity intervention for adolescents with cerebral palsy: A randomized controlled trial. Dev. Med. Child Neurol. 2010, 52, 448–455. [Google Scholar] [CrossRef]
- Knights, S.; Graham, N.; Switzer, L.; Hernandez, H.; Ye, Z.; Findlay, B.; Xie, W.Y.; Wright, V.; Fehlings, D. An innovative cycling exergame to promote cardiovascular fitness in youth with cerebral palsy. Dev. Neurorehabil. 2016, 19, 135–140. [Google Scholar] [CrossRef]
- Mitchell, L.E.; Ziviani, J.; Boyd, R.N. A randomized controlled trial of web-based training to increase activity in children with cerebral palsy. Dev. Med. Child Neurol. 2016, 58, 767–773. [Google Scholar] [CrossRef] [Green Version]
- Brien, M.; Sveistrup, H. An Intensive Virtual Reality Program Improves Functional Balance and Mobility of Adolescents With Cerebral Palsy. Pediatr. Phys. Ther. 2011, 23, 258–266. [Google Scholar] [CrossRef] [PubMed]
- Christovão, T.C.L.; Pasini, H.; Grecco, L.A.C.; Ferreira, L.A.B.; Duarte, N.A.C.; Oliveira, C.S. Effect of postural insoles on static and functional balance in children with cerebral palsy: A randomized controlled study. Braz. J. Phys. Ther. 2015, 19, 44–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kerkum, Y.L.; Buizer, A.I.; van den Noort, J.C.; Becher, J.G.; Harlaar, J.; Brehm, M.A. The Effects of Varying Ankle Foot Orthosis Stiffness on Gait in Children with Spastic Cerebral Palsy Who Walk with Excessive Knee Flexion. PLoS ONE 2015, 10, e0142878. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.Y.K.; Yu, Y.C.; Wong, A.M.K.; Tsai, Y.S.; Ju, Y.Y. Effects of an eight-week whole body vibration on lower extremity muscle tone and function in children with cerebral palsy. Res. Dev. Disabil. 2015, 38, 256–261. [Google Scholar] [CrossRef] [PubMed]
- Jung, Y.; Chung, E.J.; Chun, H.L.; Lee, B.H. Effects of whole-body vibration combined with action observation on gross motor function, balance, and gait in children with spastic cerebral palsy: A preliminary study. J. Exerc. Rehabil. 2020, 16, 249–257. [Google Scholar] [CrossRef]
- Cheng, H.Y.; Ju, Y.Y.; Chen, C.L.; Chuang, L.L.; Cheng, C.H. Effects of whole body vibration on spasticity and lower extremity function in children with cerebral palsy. Hum. Mov. Sci. 2015, 39, 65–72. [Google Scholar] [CrossRef]
- Telford, D.; Vesey, R.M.; Hofman, P.L.; Gusso, S. The Effect of Vibration Therapy on Walking Endurance in Children and Young People With Cerebral Palsy: Do Age and Gross Motor Function Classification System Matter? Arch. Rehabil. Res. Clin. Transl. 2020, 2, 100068. [Google Scholar] [CrossRef]
- Beckung, E.; Hagberg, G. Neuroimpairments, activity limitations, and participation restrictions in children with cerebral palsy. Dev. Med. Child Neurol. 2002, 44, 309–316. [Google Scholar] [CrossRef]
- LaForme Fiss, A.; McCoy, S.W.; Bartlett, D.; Avery, L.; Hanna, S.E.; On Track Study Team. Developmental Trajectories for the Early Clinical Assessment of Balance by Gross Motor Function Classification System Level for Children With Cerebral Palsy. Phys. Ther. 2019, 99, 217–228. [Google Scholar] [CrossRef] [Green Version]
- Tyson, S.; Connell, L. The psychometric properties and clinical utility of measures of walking and mobility in neurological conditions: A systematic review. Clin. Rehabil. 2009, 23, 1018–1033. [Google Scholar] [CrossRef]
- de Almeida Carvalho Duarte, N.; Collange Grecco, L.A.; Zanon, N.; Galli, M.; Fregni, F.; Santos Oliveira, C. Motor cortex plasticity in children with spastic cerebral palsy: A systematic review. J. Mot. Behav. 2017, 49, 355–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- You, S.H.; Jang, S.H.; Kim, Y.; Kwon, Y.; Barrow, I.; Hallett, M. Cortical reorganization induced by virtual reality therapy in a child with hemiparetic cerebral palsy. Dev. Med. Child Neurol. 2005, 47, 628–635. [Google Scholar] [CrossRef] [PubMed]
- Rauch, F. Vibration therapy. Dev. Med. Child Neurol. 2009, 51, 166–168. [Google Scholar] [CrossRef] [PubMed]
- Hanna, S.E.; Rosenbaum, P.L.; Bartlett, D.J.; Palisano, R.J.; Walter, S.D.; Avery, L.; Russell, D.J. Stability and decline in gross motor function among children and youth with cerebral palsy aged 2 to 21 years. Dev. Med. Child Neurol. 2009, 51, 295–302. [Google Scholar] [CrossRef]
- Beckung, E.; Hagberg, G.; Uldall, P.; Cans, C.; Surveillance of Cerebral Palsy in Europe. Probability of walking in children with cerebral palsy in Europe. Pediatrics 2008, 121, e187–e192. [Google Scholar] [CrossRef]


{kind=link}
| Author Year | Type of Study | Sample N Male/Female | Age of Assessment Years (y) Mean ± SD | Type of CP | Type of Intervention | Outcome | |
|---|---|---|---|---|---|---|---|
| 1 | Swe et al., 2015 [12] | Randomized controlled study | 30 (20/10) | 13.2 (±3.39) | CP (GMFCS II–III) | Physiotherapy: Partial body weight supported treadmill training/over-ground training (2-times 30 min sessions of walking training per week for 8 weeks) | Significant improvements in the 6MWT performances after a period of 4–8 weeks for both partial body weight supported treadmill training and over-ground training without significant differences between them |
| 2 | Kepenek-Varol et al., 2021 [13] | Case–control | 30 | 7–16 | Hemiplegia (GMFCS I–II) | Physiotherapy: Inspiratory muscle training/conventional physiotherapy versus conventional physiotherapy alone | 6MWT values were significantly increased after the training in both groups No significant differences between groups |
| 3 | Bleyenheuft et al., 2014 [14] | Interventional study | 24 (12/12) | 6–13 | Unilateral spastic cerebral palsy | Physiotherapy: 2 groups HABIT-ILE: immediate HABIT-ILE group (IHG, initially receiving HABIT-ILE, 10 days = 90 h), and a delayed HABIT-ILE group (DHG), which continued their conventional/ongoing treatment for an intended total duration of 90 h. Phase 2: children in the DHG were crossed over to receive HABIT-ILE, and children of the IHG were followed in their ongoing conventional therapy | Significant improvements in the 6MWT between the pre- and post-HABIT-ILE No significant differences were observed following conventional treatment |
| 4 | Goswami et al., 2021 [15] | Open-label, randomized controlled study | 59 (43/16) | 5–12 | Spastic diplegia (GMFCS II–III) | Physiotherapy: Home-centered activity-based rehabilitation (walking, standing, squatting, climbing upstairs/downstairs, kicking a ball, dancing, riding a tricycle/bicycle) and institutional physiotherapy versus conventional physiotherapy | No significant differences in the 6MWT in children performing home activity compared with those who have followed a conventional physiotherapy |
| 5 | Fosdahl et al., 2019 [16] | Randomized case–control, interventional study | 37 (21/16) | 10.2 (±2.3) | Spastic CP (GMFCS I–III) | Physiotherapy: A 16-week combined stretching and progressive resistance exercise (PRE) program, followed by a 16-week maintenance program (n = 17) compared to traditional physiotherapy program (n = 20) | Significant improvements in the 6MWT between baseline and after 16 weeks No differences between the 2 groups |
| 6 | Aviram et al., 2017 [17] | Matched controlled study | 95 (61/34) | 14–21 | Spastic CP (GMFCS II–III) | Physiotherapy: Circuit progressive resistance exercise training and treadmill training intervention for 30 biweekly 1 h training | Significant improvements in the 6MWT in both groups |
| 7 | Tsai et al., 2017 [18] | Interventional study | 8 | 15.5 (± 4.1) | Not specified (GMFCS I–III) | Physiotherapy: Off-axis elliptical training on gait function improvement for a total of 18 training sessions (approximately 45–60 min/session) within 6 to 10 weeks (average, 8.2 ± 1.1 weeks) | No statistically significant increase in 6MWT distance |
| 8 | Hoffman et al., 2018 [19] | Exploratory study | 11 (10/1) | 12 ± 1 | Spastic CP (10 diplegic, 1 hemiplegic) | Physiotherapy: Gait training program with 30 min of treadmill locomotion performed 3 days a week for 6 weeks, with a minimum of 1 day of rest between the training sessions | Significant improvements in the 6MWT after training |
| 9 | Kusumoto et al., 2016 [20] | Single-blind randomized clinical trial | 16 (16/0) | 12–18 | Spastic diplegia (GMFCS I–III) | Physiotherapy: Loaded STS exercises at different speeds (slow-loaded STS training group and arbitrarily loaded STS training group); loaded sit-to-stand exercise was conducted at home for 15 min, 4 sets per day, 3–4 days per week, for 6 weeks | Significant improvements in the 6MWT in the slow-loaded STS training group |
| 10 | Lee et al., 2014 [21] | Interventional study | 13 (9/4) | 6–18 | 4 diplegia, 6 hemiplegia, 3 quadriplegia (GMFCS I–III) | Physiotherapy: Sliding rehabilitation machine for 8 weeks (30 min/day, 2 times/week) | Significant improvements in the 6MWT after training |
| 11 | Mattern-Baxter et al., 2009 [22] | Interventional study | 6 (3/3) | 2.5–3.9 | 3 spastic diplegia, 1 spastic quadriplegia, 1 dystonic quadriplegia, 1 hypotonic CP (GMFCS I–IV) | Physiotherapy: A 4-week intensive locomotor treadmill training (3 times per week for 1 h sessions consisting of 2 individualized treadmill walks) | Significant improvements in the 6MWT between baseline and 1-month follow-up |
| 12 | Cohen-Holzer et al., 2017 [23] | Interventional study | 24 | 6–11 | Unilateral cerebral palsy | Physiotherapy: Short-term, intensive intervention program combining constraint and bimanual training | Significant improvements in the 6MWT at post- and 3 months postintervention |
| 13 | Williams et al. 2013 [24] | Cross-sectional study | 15 (10/5) | 5–11 8.5 (±1.10) | Spastic diplegia (GMFCS I–II) | Pharmacological therapy: BoNT-A in the gastrocnemius muscle; 5 participants also received BoNT-A bilaterally to the medial hamstring muscles | No statistically significant increase in the 6MWT after 5 weeks from injections, neither in children receiving BoNT-A treatment in the gastrocnemius muscles nor in those who received BoNT-A treatment in the gastrocnemius and medial hamstring muscles |
| 14 | Grecco et al. 2013 [25] | Prospective study | 15 | 8–15 | Not specified (GMFCS II–III) | Surgery: Surgery intervention (Group 1: soft tissue versus Group 2: soft tissue and bone surgery) and 12 weeks of treadmill training | Significant improvements in the 6MWT in both groups on the post-training |
| 15 | Kim et al., 2021 [26] | Interventional study | 3 (1/2) | 9–16 | Bilateral spastic cerebral palsy (GMFCS II–IV) | Robotics: RAGT using a wearable torque-assisted exoskeletal (Angel Legs) conducted for 17~20 sessions (60 min per session) and conventional rehabilitation program | Significant improvements in the 6MWT and in gross motor function after RAGT |
| 16 | Meyer-Heim et al., 2009 [27] | Single-case experimental | 22 (13/9) | 4.6–11.7 (8.6) | Bilateral spastic CP (GMFCS II–IV) | Robotics: RAGT with Lokomat (3–5 sessions of 45–60 min/week during a 3–5-week period) | No statistically significant increase in the 6MWT |
| 17 | Van Hedel et al., 2015 [28] | Retrospective study | 67 (41/26) | 3.9–19.9 | Bilateral spastic CP: 57; unilateral spastic CP: 2; ataxic CP: 6; dystonic CP: 2 (GMFCS II–IV) | Robotics: Intensive locomotor training program using RAGT with Lokomat and conventional physiotherapy | No statistically significant increase in the 6MWT |
| 18 | Beretta et al., 2019 [29] | Retrospective study | 182 | 4–18 | 110 with acquired brain injury (ABI) and 72 with cerebral palsy | Robotics: Combined treatment of RAGT with Lokomat and physical therapy (20 sessions + 20 sessions) | Significant improvements in the 6MWT in both ABI and CP |
| 19 | Sucuoglu et al., 2020 [30] | Cross-sectional study | 38 (23/15) | 7.8 (± 3.8) | Spastic CP (hemiplegic, diplegic, tetraplegic, n = 33); ataxic, n = 2; hypotonic, n = 2; mixed, n = 1 (GMFCS I–IV) | Robotics: RAGT in combination with a conventional treatment program (30 sessions of 60 min over 8–10 weeks) | Significant improvements in the 6MWT after RAGT in combination with a conventional treatment program in children with mild to moderate CP (GMFCS I–III) |
| 20 | Smania et al. 2011 [31] | Randomized controlled study | 18 | 10–18 | Diplegia or quadriplegia (GMFCS II–IV) | Robotics: 30 min repetitive locomotor training with an electromechanical gait trainer (gait trainer) versus 40 min of conventional physiotherapy. A total of 10 treatment sessions were performed over a 2-week period | Significant improvements in the 6MWT in gait trainer group |
| 21 | Cheng et al., 2013 [32] | Randomized, crossover study | 18 (10/8) | 9.5 ± 2.1 | Spastic diplegia or spastic quadriplegia | Robotics: An 8-week repetitive passive knee movement intervention program (3 times a week) and a control group. After a 4-week wash-out period, children from 1 group were crossed over to the other group | Significant improvements in the 6MWT and decrease in muscle spasticity within 3 days postintervention |
| 22 | Kang et al., 2017 [33] | Interventional study | 6 (6/0) | 9–19 | Not specified GMFCS Level II | Robotics: A robot-driven downward pelvic pull (tethered pelvic assist device (TPAD)) while walking on treadmill for 2 weeks after the last training | Significant improvements in the 6MWT |
| 23 | Chen et al., 2016 [34] | Pilot randomized comparative trial | 41 (31/10) | 7–18 8.7 ± 2.8 | Hemiplegia: 21; diplegia: 20 (GMFCS I–III) | Robotics: 6-week home-based robotic ankle training with a portable rehabilitation robot versus laboratory-based rehabilitation | Significant improvements in the 6MWT in both groups |
| 24 | Sukal-Moulton et al., 2014 [35] | Retrospective study | 28 (19/9) | 8.2 ± 3.62 | 11 diplegia, 16 hemiplegia, 1 triplegia (GMFCS I–III) | Robotics: Robotic ankle training program (IntelliStretch robotic device) in a training program combining passive stretching and active movement protocol of 1 ankle joint 2 times per week for 75 min sessions for a total of 6 weeks compared to children previously involved in a laboratory-based intervention protocol (n = 12) | Significant improvements in the 6MWT in the IntelliStretch group |
| 25 | Conner et al. 2020 [36] | Interventional study | 6 (5/1) | 14 y 11 m | 3 hemiplegic CP, 3 diplegic CP (GMFCS I–III) | Robotics: 10 training sessions in 4 weeks, consisting in walking on treadmill with a wearable resistance in strengthening walking capacity and mobility | Significant improvements in the 6MWT |
| 26 | Ming Wu et al., 2017 [37] | Randomized controlled trial | 23 (14/9) | 4–16 (10.9 ± 3.2) | Not specified (GMFCS I–IV) | Robotics: Ankle and leg robotic devices using a controlled force to the pelvis and legs and treadmill training versus treadmill training only | Significant improvements in the 6MWT after robotic training, but not after treadmill-only training |
| 27 | Maher et al., 2010 [38] | Randomized Controlled study | 41 26/15 | 13.7 (±1.8) | Unilateral or bilateral cerebral palsy (GMFCS I–III) | Others: 8-week internet-based intervention, including exercises on social cognitive theory, incorporating education, quizzes, goal-setting, self-reflection and positive role modeling | No significant improvements in the 6MWT |
| 28 | Knights et al. 2014 [39] | Prospective | 8 (6/2) | 9–18 | Bilateral spastic CP (GMFCS III) | Others: 6-week home-based internet-platform exergame cycling program (play of video games that require physical exertion) | No Significant improvements in the 6MWT |
| 29 | Mitchell et al., 2016 [40] | Case-controlled trial | 101 (52/49) | 8–17 (11 y 3 m ± 2 y 4 m) | Unilateral CP (GMFCS I–II) | Others: Individualized daily program of 30 min duration, 6 days per week for 20 weeks, with specific physical activity games (repetitive multi-joint bodyweight functional exercise) and upper-limb and visual–perceptual games versus waitlist control group | Significant improvements in the 6MWT and functional strength in experimental group compared with the control group at 20 weeks |
| 30 | Brien et al., 2011 [41] | Interventional study | 4 (4/0) | 16 (±2.25) | Spastic diplegia choreoathetosis (GMFCS level I) | Others: 1-month intensive short-duration virtual reality (VR) intervention consisting of 90 min of VR-based balance training on 5 consecutive days, in which the participants interacted with virtual objects encouraging motor abilities such as dynamic standing balance and coordination skills in walking performance, walking speed and endurance, and stair climbing | Significant improvements in the 6MWT in the interventional phase, maintained at 1-month follow-up |
| 31 | Christovão et al., 2015 [42] | Randomizedcontrolled, double-blind, clinical study | 20 (10/10) Cases: 8/2 Controls: 7/3 | 4–12 | Spastic diplegia | Others: Postural insoles versus placebo insoles for 3 months | No significant improvements in the 6MWT immediately after placement of insoles and after 3 months of use Performances were similar for both groups |
| 32 | Kerkum et al. 2015 [43] | Interventional study | 15 (11/4) | 6–14 (10 ± 2) | Spastic CP (GMFCS I–III) | Others: AFOs and spring-like AFOs that enhance push-off power | Significant improvements in the 6MWT, knee flexion and energy cost in all kinds of AFOs No significant differences were found between AFOs |
| 33 | Cheng et al. 2015 [44] | Crossover study | 16 (8/8) | 9.2 (±2.1) | Spastic diplegia or spastic quadriplegia | Others: 1 group received an 8-week WBV intervention (10 min/day) followed by an 8-week control condition, with a 4-week rest; the other group began the treatment sequence with the control condition to counterbalance the order effects | Significant improvements in the 6MWT, spasticity and active joint range for at least 3 days, but the effect attenuated over time after the cease of the intervention |
| 34 | Jung et al., 2020 [45] | Randomized, interventional study | 14 (6/8) | 4-12 | Spastic CP (GMFCS I–III) | Others: 7 children underwent the WBV combined with action observation (WBVAO), performing 6 different actions demonstrated in the videos for a 4-week period; 7 children followed the same training protocols without action observation for a 4-week period. During the same period, all participants also performed physical therapy | Significant improvements in the 6MWT in both experimental (WBVAO) and control groups (WBV only) WBVAO group showed a more significant improvement |
| 35 | Martakis et al. 2020 [46] | Retrospective study | 157 (84/73) | 3–12 | Not specified (GMFCS I–II) | Others: 6-month rehabilitation program including whole-body vibration. The assessments were performed at baseline, after 6 months of combined conventional physiotherapy and WBV program and after 12 months without training | Significant improvements in the 6MWT at 6 months, while no statistically significant changes at 12 months |
| 36 | Cheng et al. 2015 [47] | Complete crossover design | 16 (9/7) | 9.8 ± 2.3 | Spastic diplegia or spastic quadriplegia | Others: 20 min WBV and control condition in a counterbalanced order on 2 separate days, 1 week apart | Significant improvements in the 6MWT in the WBV treatment |
| 37 | Telford et al. 2020 [48] | Interventional study | 59 (33/26) | 5–20 (13.8 ± 4.3) | Not specified (GMFCS II–IV) | Others: Side-alternating WBV, 9 min per day, 4 times per week for 20 weeks | Significant improvements in the 6MWT after intervention, especially for children with limited mobility (GMFCS III and IV) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romeo, D.M.; Venezia, I.; De Biase, M.; Sini, F.; Velli, C.; Mercuri, E.; Brogna, C. The Use of the 6MWT for Rehabilitation in Children with Cerebral Palsy: A Narrative Review. J. Pers. Med. 2023, 13, 28. https://doi.org/10.3390/jpm13010028
Romeo DM, Venezia I, De Biase M, Sini F, Velli C, Mercuri E, Brogna C. The Use of the 6MWT for Rehabilitation in Children with Cerebral Palsy: A Narrative Review. Journal of Personalized Medicine. 2023; 13(1):28. https://doi.org/10.3390/jpm13010028
Chicago/Turabian StyleRomeo, Domenico M., Ilaria Venezia, Margherita De Biase, Francesca Sini, Chiara Velli, Eugenio Mercuri, and Claudia Brogna. 2023. "The Use of the 6MWT for Rehabilitation in Children with Cerebral Palsy: A Narrative Review" Journal of Personalized Medicine 13, no. 1: 28. https://doi.org/10.3390/jpm13010028