
Practical Aspects of Esophageal Pressure Monitoring in Patients with Acute Respiratory Distress Syndrome

Abstract
:1. Introduction
2. Transpulmonary Pressure, Pleural Pressure, and Esophageal Pressure

{kind=link}
{kind=link}
| Parameter | Method | Computation |
|---|---|---|
| End-inspiratory PL, | Elastance-derived | PL = Pplat x EL/Ers = Pplat x [(Pplat − Pesplat) − (PawPEEP − PesPEEP)]/(Pplat − PawPEEP) |
| End-inspiratory PL (reference method) | Release-derived | PL = (Pplat − PawATM) − (Pesplat − PesATM) |
| End-expiratory PL | Direct method | PL = PawPEEP − PesPEEP |
| Driving PL | Direct method | DPL = (Pplat − Pesplat) − (PawPEEP − PesPEEP), or DPL = (Pplat − PawPEEP) − (Pesplat − PesPEEP) |
3. Technical Aspects of Esophageal Pressure Measurement
3.1. Ballon Catheter Insertion and Positioning
3.2. Ballon Filling and Validation Testing
3.3. Artifacts, Errors, and Rules during the Pes Measurement
4. Ventilatory Setting Based on Transpulmonary Pressure in Passive ARDS Patients
4.1. PEEP Setting Targeting Expiratory Transpulmonary Pressure
4.2. PEEP Setting Targeting Inspiratory Transpulmonary Pressure
4.3. Transpulmonary Driving Pressure and Safety
5. The Other Possible Use for Measuring Esophageal Pressure in ARDS Patients
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mauri, T.; Yoshida, T.; Bellani, G.; Goligher, E.C.; Carteaux, G.; Rittayamai, N.; Mojoli, F.; Chiumello, D.; Piquilloud, L.; Grasso, S.; et al. PLeUral pressure working Group (PLUG—Acute Respiratory Failure section of the European Society of Intensive Care Medicine). Esophageal and transpulmonary pressure in the clinical setting: Meaning, usefulness and perspectives. Intensive Care Med. 2016, 42, 1360–1373. [Google Scholar] [CrossRef] [PubMed]
- Gattinoni, L.; Giosa, L.; Bonifazi, M.; Pasticci, I.; Busana, M.; Macri, M.; Romitti, F.; Vassalli, F.; Quintel, M. Targeting transpulmonary pressure to prevent ventilator-induced lung injury. Expert Rev. Respir. Med. 2019, 13, 737–746. [Google Scholar] [CrossRef] [PubMed]
- Sahetya, S.K.; Brower, R.G. The promises and problems of transpulmonary pressure measurements in acute respiratory distress syndrome. Curr. Opin. Crit. Care 2016, 22, 7–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gattinoni, L.; Carlesso, E.; Caironi, P. Stress and strain within the lung. Curr. Opin. Crit. Care 2012, 18, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Talmor, D.; Sarge, T.; Malhotra, A.; O’Donnell, C.R.; Ritz, R.; Lisbon, A.; Novack, V.; Loring, S.H. Mechanical ventilation guided by esophageal pressure in acute lung injury. N. Engl. J. Med. 2008, 359, 2095–2104. [Google Scholar] [CrossRef] [Green Version]
- Yoshida, T.; Grieco, D.L.; Brochard, L.; Fujino, Y. Patient self-inflicted lung injury and positive end-expiratory pressure for safe spontaneous breathing. Curr. Opin. Crit. Care 2020, 26, 59–65. [Google Scholar] [CrossRef]
- Mauri, T.; Bellani, G.; Confalonieri, A.; Tagliabue, P.; Turella, M.; Coppadoro, A.; Citerio, G.; Patroniti, N.; Pesenti, A. Topographic distribution of tidal ventilation in acute respiratory distress syndrome: Effects of positive end-expiratory pressure and pressure support. Crit. Care Med. 2013, 41, 1664–1673. [Google Scholar] [CrossRef]
- Yoshida, T.; Amato, M.B.P.; Grieco, D.L.; Chen, L.; Lima, C.A.S.; Roldan, R.; Morais, C.C.A.; Gomes, S.; Costa, E.L.V.; Cardoso, P.F.G.; et al. Esophageal Manometry and Regional Transpulmonary Pressure in Lung Injury. Am. J. Respir. Crit. Care Med. 2018, 197, 1018–1026. [Google Scholar] [CrossRef]
- Mietto, C.; Malbrain, M.L.; Chiumello, D. Transpulmonary pressure monitoring during mechanical ventilation: A bench-to-bedside review. Anaesthesiol. Intensive Ther. 2015, 8, 27–37. [Google Scholar] [CrossRef]
- Gattinoni, L.; Chiumello, D.; Carlesso, E.; Valenza, F. Bench-to-bedside review: Chest wall elastance in acute lung injury/acute respiratory distress syndrome patients. Crit. Care 2004, 8, 350–355. [Google Scholar] [CrossRef] [Green Version]
- Grieco, D.L.; Chen, L.; Brochard, L. Transpulmonary pressure: Importance and limits. Ann. Transl. Med. 2017, 5, 285. [Google Scholar] [CrossRef] [Green Version]
- Mojoli, F.; Torriglia, F.; Orlando, A.; Bianchi, I.; Arisi, E.; Pozzi, M. Technical aspects of bedside respiratory monitoring of transpulmonary pressure. Ann. Transl. Med. 2018, 6, 377. [Google Scholar] [CrossRef] [PubMed]
- Mojoli, F.; Chiumello, D.; Pozzi, M.; Algieri, I.; Bianzina, S.; Luoni, S.; Volta, C.A.; Braschi, A.; Brochard, L. Esophageal pressure measurements under different conditions of intrathoracic pressure. An in vitro study of second generation balloon catheters. Minerva Anestesiol. 2015, 81, 855–864. [Google Scholar] [PubMed]
- Niknam, J.; Chandra, A.; Adams, A.B.; Nahum, A.; Ravenscraft, S.A.; Marini, J.J. Effect of a nasogastric tube on esophageal pressure measurement in normal adults. Chest 1994, 106, 137–141. [Google Scholar] [CrossRef] [Green Version]
- Mojoli, F.; Iotti, G.A.; Torriglia, F.; Pozzi, M.; Volta, C.A.; Bianzina, S.; Braschi, A.; Brochard, L. In vivo calibration of esophageal pressure in the mechanically ventilated patient makes measurements reliable. Crit. Care 2016, 20, 98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Y.L.; He, X.; Sun, X.M.; Chen, H.; Shi, Z.H.; Xu, M.; Chen, G.Q.; Zhou, J.X. Optimal esophageal balloon volume for accurate estimation of pleural pressure at end-expiration and end-inspiration: An in vitro bench experiment. Intensive Care Med. Exp. 2017, 5, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, X.M.; Chen, G.Q.; Huang, H.W.; He, X.; Yang, Y.L.; Shi, Z.H.; Xu, M.; Zhou, J.X. Use of esophageal balloon pressure-volume curve analysis to determine esophageal wall elastance and calibrate raw esophageal pressure: A bench experiment and clinical study. BMC Anesthesiol. 2018, 18, 21. [Google Scholar] [CrossRef]
- Kassis, E.B.; Talmor, D. Clinical application of esophageal manometry: How I do it. Crit. Care 2021, 25, 6. [Google Scholar] [CrossRef]
- Jiang, J.; Su, L.; Cheng, W.; Wang, C.; Rui, X.; Tang, B.; Zhang, H.; He, H.; Long, Y. The calibration of esophageal pressure by proper esophageal balloon filling volume: A clinical study. Front. Med. 2022, 9, 986982. [Google Scholar] [CrossRef]
- Kumaresan, A.; Gerber, R.; Mueller, A.; Loring, S.H.; Talmor, D. Effects of Prone Positioning on Transpulmonary Pressures and End-expiratory Volumes in Patients without Lung Disease. Anesthesiology 2018, 128, 1187–1192. [Google Scholar] [CrossRef]
- Beitler, J.R.; Sarge, T.; Banner-Goodspeed, V.M.; Gong, M.N.; Cook, D.; Novack, V.; Loring, S.H.; Talmor, D.; EPVent-2 Study Group. Effect of Titrating Positive End-Expiratory Pressure (PEEP) With an Esophageal Pressure-Guided Strategy vs an Empirical High PEEP-Fio2 Strategy on Death and Days Free From Mechanical Ventilation Among Patients With Acute Respiratory Distress Syndrome: A Randomized Clinical Trial. JAMA 2019, 321, 846–857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarge, T.; Baedorf-Kassis, E.; Banner-Goodspeed, V.; Novack, V.; Loring, S.H.; Gong, M.N.; Cook, D.; Talmor, D.; Beitler, J.R.; EPVent-2 Study Group. Effect of Esophageal Pressure-guided Positive End-Expiratory Pressure on Survival from Acute Respiratory Distress Syndrome: A Risk-based and Mechanistic Reanalysis of the EPVent-2 Trial. Am. J. Respir. Crit. Care Med. 2021, 204, 1153–1163. [Google Scholar] [CrossRef] [PubMed]
- Amato, M.B.; Meade, M.O.; Slutsky, A.S.; Brochard, L.; Costa, E.L.; Schoenfeld, D.A.; Stewart, T.E.; Briel, M.; Talmor, D.; Mercat, A.; et al. Driving pressure and survival in the acute respiratory distress syndrome. N. Engl. J. Med. 2015, 372, 747–755. [Google Scholar] [CrossRef] [Green Version]
- Writing Group for the Alveolar Recruitment for Acute Respiratory Distress Syndrome Trial (ART) Investigators; Cavalcanti, A.B.; Suzumura, É.A.; Laranjeira, L.N.; Paisani, D.M.; Damiani, L.P.; Guimarães, H.P.; Romano, E.R.; Regenga, M.M.; Taniguchi, L.N.T.; et al. Effect of Lung Recruitment and Titrated Positive End-Expiratory Pressure (PEEP) vs Low PEEP on Mortality in Patients With Acute Respiratory Distress Syndrome: A Randomized Clinical Trial. JAMA 2017, 318, 1335–1345. [Google Scholar] [CrossRef]
- Gattinoni, L.; Marini, J.J. In search of the Holy Grail: Identifying the best PEEP in ventilated patients. Intensive Care Med. 2022, 48, 728–731. [Google Scholar] [CrossRef] [PubMed]
- Grasso, S.; Terragni, P.; Birocco, A.; Urbino, R.; Del Sorbo, L.; Filippini, C.; Mascia, L.; Pesenti, A.; Zangrillo, A.; Gattinoni, L.; et al. ECMO criteria for influenza A (H1N1)-associated ARDS: Role of transpulmonary pressure. Intensive Care Med. 2012, 38, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Bugedo, G.; Retamal, J.; Bruhn, A. Driving pressure: A marker of severity, a safety limit, or a goal for mechanical ventilation? Crit. Care 2017, 21, 199. [Google Scholar] [CrossRef] [Green Version]
- Pelosi, P.; Ball, L.; Barbas, C.S.V.; Bellomo, R.; Burns, K.E.A.; Einav, S.; Gattinoni, L.; Laffey, J.G.; Marini, J.J.; Myatra, S.N.; et al. Personalized mechanical ventilation in acute respiratory distress syndrome. Crit. Care 2021, 25, 250. [Google Scholar] [CrossRef]
- Goligher, E.C.; Dres, M.; Patel, B.K.; Sahetya, S.K.; Beitler, J.R.; Telias, I.; Yoshida, T.; Vaporidi, K.; Grieco, D.L.; Schepens, T.; et al. Lung- and Diaphragm-Protective Ventilation. Am. J. Respir. Crit. Care Med. 2020, 202, 950–961. [Google Scholar] [CrossRef]
- Carteaux, G.; Parfait, M.; Combet, M.; Haudebourg, A.F.; Tuffet, S.; Mekontso Dessap, A. Patient-Self Inflicted Lung Injury: A Practical Review. J. Clin. Med. 2021, 10, 2738. [Google Scholar] [CrossRef]
- Bertoni, M.; Telias, I.; Urner, M.; Long, M.; Del Sorbo, L.; Fan, E.; Sinderby, C.; Beck, J.; Liu, L.; Qiu, H.; et al. A novel non-invasive method to detect excessively high respiratory effort and dynamic transpulmonary driving pressure during mechanical ventilation. Crit. Care 2019, 23, 346. [Google Scholar] [CrossRef] [PubMed] [Green Version]


| Steps | Method |
|---|---|
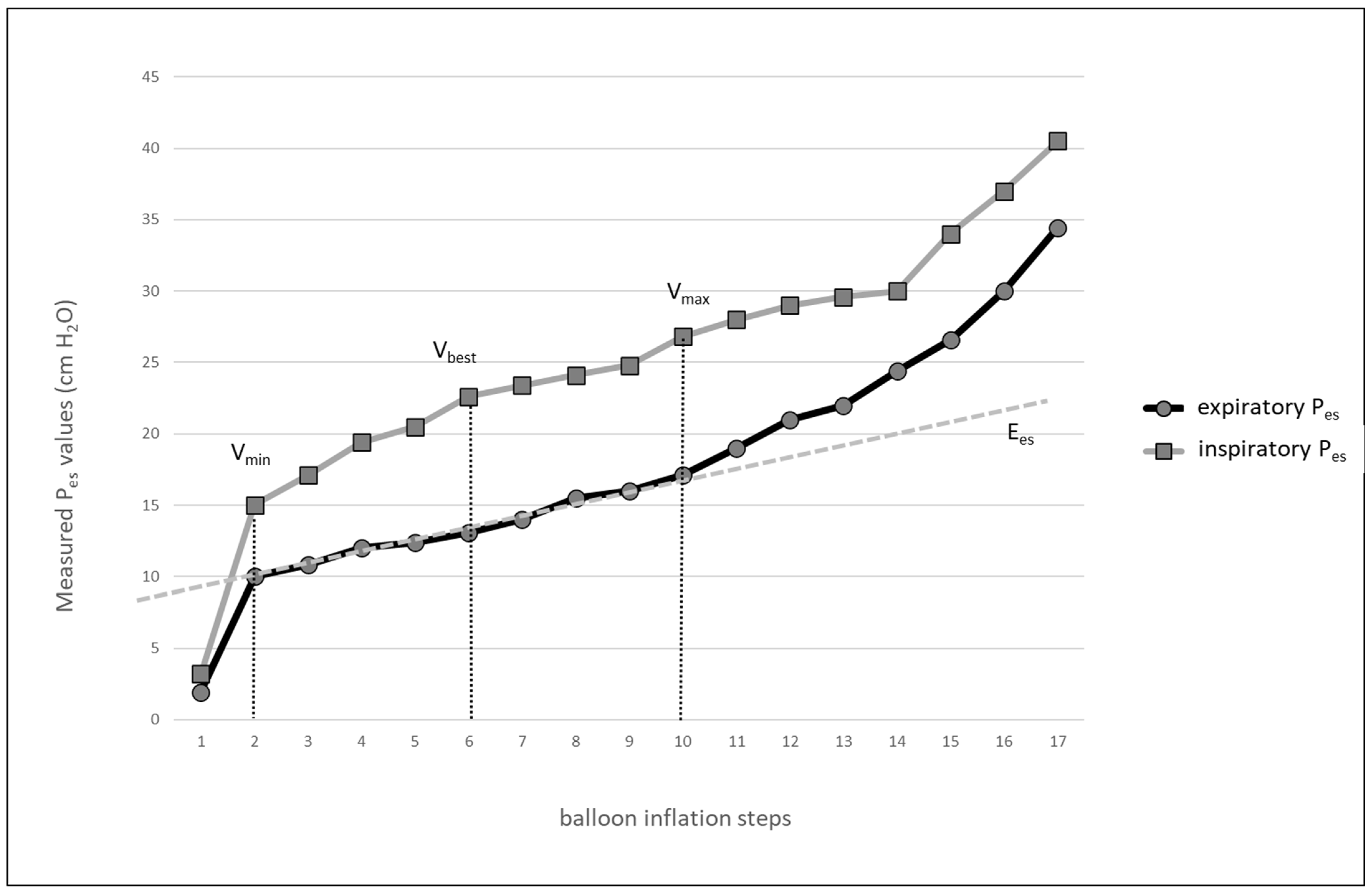
| 1st step | Perform a stepwise inflation of the balloon (0.2–1.0 mL steps, according to the balloon size), record Pes at different volumes of balloon. |
| 2nd step | Using an appropriate table calculator, create the balloon pressure-volume curve to identify a linear part of the curve with Vmin and Vmax, for further measurement select Vbest with largest tidal change of Pes. |
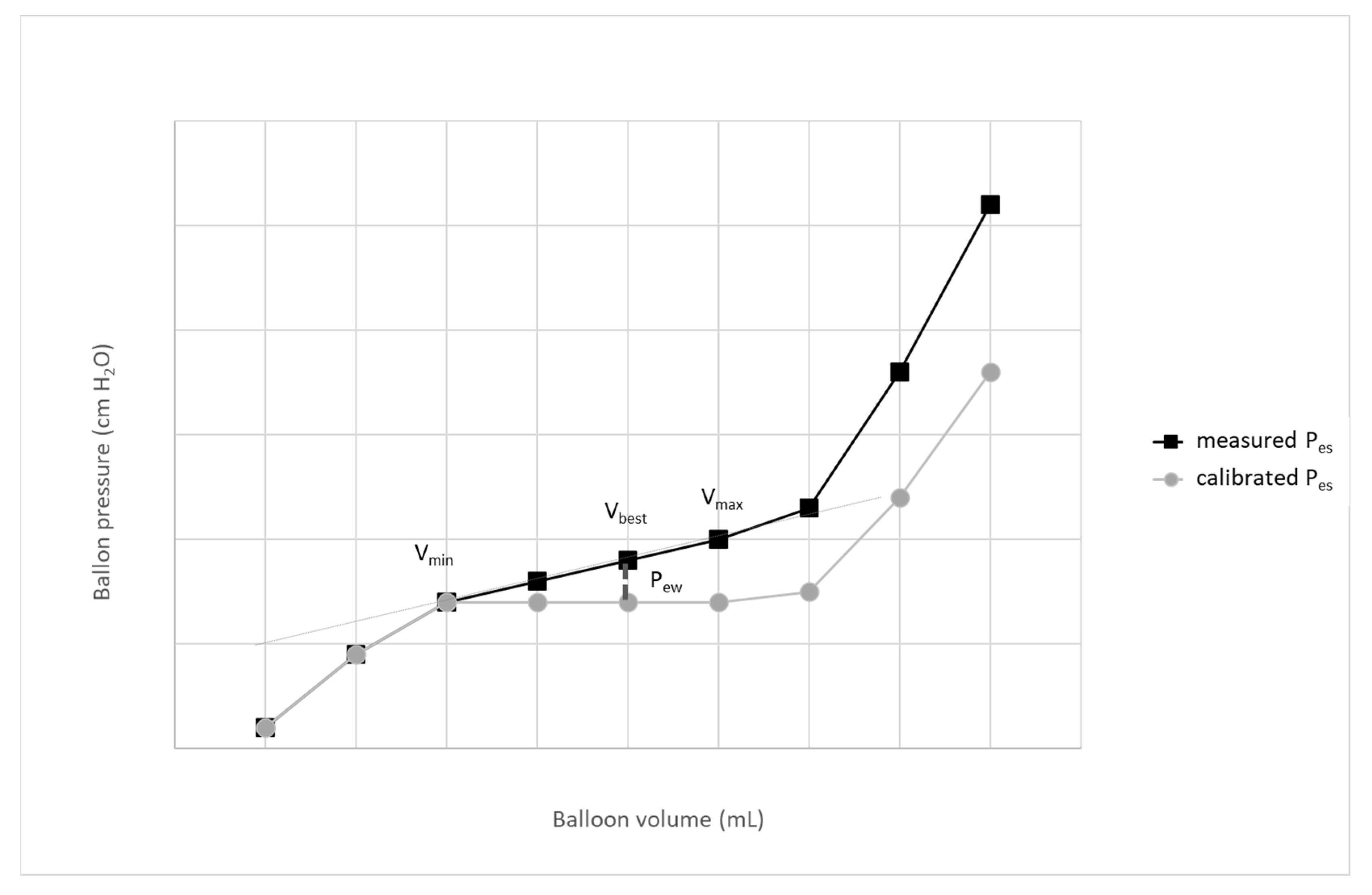
| 3rd step | Calculate the esophageal wall elastance: Ees = (PesPEEPVmax − PesPEEPVmin)/(Vmax − Vmin) |
| 4th step | Calculate the esophageal recoil pressure: PewVbest = (Vbest -Vmin) x Ees |
| 5th step | Calculate the calibrated esophageal pressure: calPes = PesVbest − PewVbest |
| Parameter | Limit |
|---|---|
| End-expiratory PL | ±2 cm H2O |
| End-inspiratory PL | <20 cm H2O |
| Driving PL | <10–12 cm H2O |
| End-inspiratory PL during recruitment maneuvers | ≤25 cm H2O |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dostal, P.; Dostalova, V. Practical Aspects of Esophageal Pressure Monitoring in Patients with Acute Respiratory Distress Syndrome. J. Pers. Med. 2023, 13, 136. https://doi.org/10.3390/jpm13010136
Dostal P, Dostalova V. Practical Aspects of Esophageal Pressure Monitoring in Patients with Acute Respiratory Distress Syndrome. Journal of Personalized Medicine. 2023; 13(1):136. https://doi.org/10.3390/jpm13010136
Chicago/Turabian StyleDostal, Pavel, and Vlasta Dostalova. 2023. "Practical Aspects of Esophageal Pressure Monitoring in Patients with Acute Respiratory Distress Syndrome" Journal of Personalized Medicine 13, no. 1: 136. https://doi.org/10.3390/jpm13010136