
Increasing Trend in Violence-Related Trauma and Suicide Attempts among Pediatric Trauma Patients: A 6-Year Analysis of Trauma Mechanisms and the Effects of the COVID-19 Pandemic
 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Epidemiological Analysis over Time
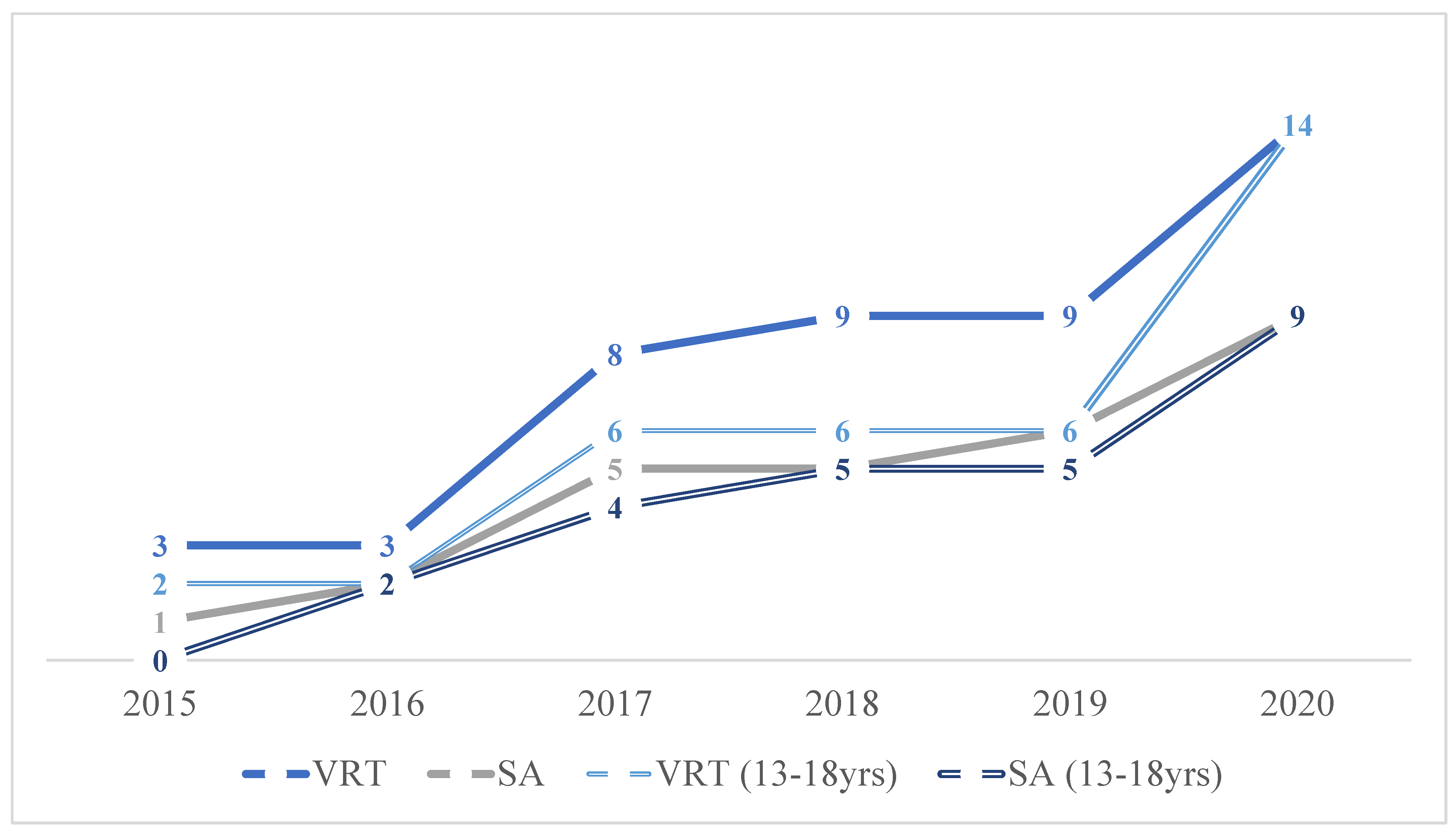
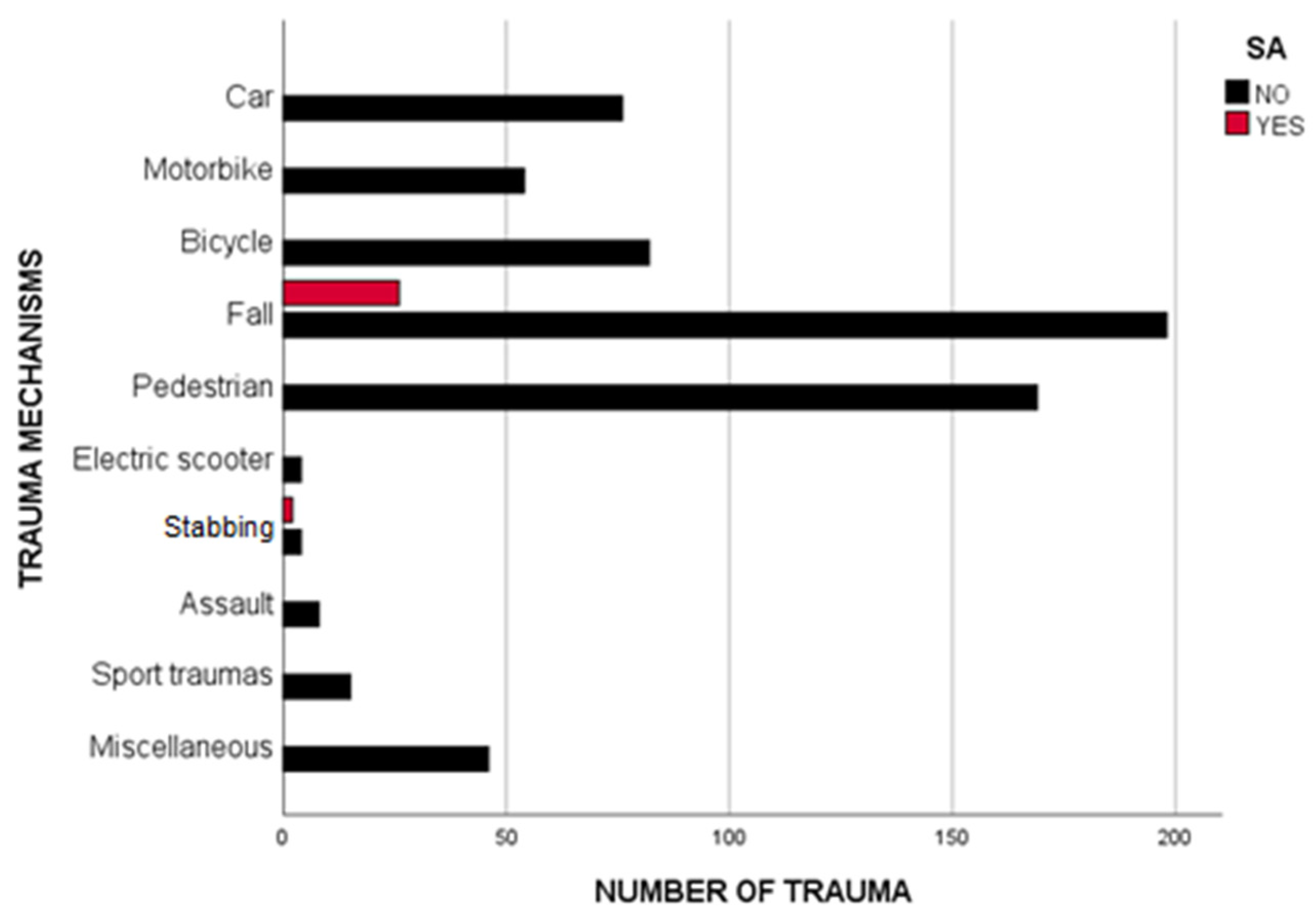
3.2. Major Trauma: Trend over Time and Predominant Mechanisms
3.3. Emergency Department Management
3.4. Surgical Intervention
3.5. Subgroup Analysis: 0–12 Years Old vs. 13–18 Years Old
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| PT | pediatric trauma |
| VRT | violence-related trauma |
| SA | suicide attempt |
| NTC | Niguarda Trauma Center |
| COVID-19 | COVID-19 |
| ED | Emergency Department |
| DCS | Damage Control Strategy |
| SI | Shock Index |
| ISS | Injury Severity Score |
| AIS15 | Abbreviated Injury Scale 2015 Revision |
| SD | standard deviation |
| IQR | interquartile range |
| EPP | extraperitoneal pelvic packing |
| TBI | traumatic brain injuries |
| UNICEF | United Nation International Children’s Emergency Fund |
| EAP | European Academy of Pediatrics |
| ECPCP | European Confederation of Primary Care Pediatricians |
References
- Cunningham, R.M.; Walton, M.A.; Carter, P.M. The Major Causes of Death in Children and Adolescents in the United States. N. Engl. J. Med. 2018, 379, 2468–2475. [Google Scholar] [CrossRef] [PubMed]
- Sanford, E.L.; Zagory, J.; Blackwell, J.; Szmuk, P.; Rayan, M.; Ambardekar, A. Changes in pediatric trauma during COVID-19 stay-at-home epoch at a tertiary pediatric hospital. J. Pediatr. Surg. 2021, 56, 918–922. [Google Scholar] [CrossRef] [PubMed]
- Schlegel, C.; Greeno, A.; Chen, H.; Raees, M.A.; Collins, K.F.; Chung, D.H.; Lovvorn, H.N., III. Evolution of a level I pediatric trauma center: Changes in injury mechanisms and improved outcomes. Surgery 2018, 163, 1173–1177. [Google Scholar] [CrossRef] [PubMed]
- Oliver, J.; Avraham, J.; Frangos, S.; Tomita, S.; DiMaggio, C. The epidemiology of inpatient pediatric trauma in United States hospitals 2000 to 2011. J. Pediatr. Surg. 2018, 53, 758–764. [Google Scholar] [CrossRef]
- Bessoff, K.E.; Han, R.W.; Cho, M.; Stroud, M.; Urrechaga, E.M.; Thorson, C.M.; Russell, K.W.; Rohan, A.; Acker, S.N.; Swain, S.; et al. Epidemiology of pediatric trauma during the COVID-19 pandemic shelter in place. Surg. Open Sci. 2021, 6, 5–9. [Google Scholar] [CrossRef]
- Sheridan, G.A.; Nagle, M.; Russell, S.; Varghese, S.; O’Loughlin, P.F.; Boran, S.; Taylor, C.; Harty, J.A. Pediatric Trauma and the COVID-19 Pandemic: A 12-Year Comparison in a Level-1 Trauma Center. HSS J. 2020, 16, 92–96. [Google Scholar] [CrossRef]
- Ruzzini, L.; De Salvatore, S.; Lamberti, D.; Maglione, P.; Piergentili, I.; Crea, F.; Ossella, C.; Costici, P. COVID-19 changed the incidence and the pattern of pediatric traumas: A single-centre study in a pediatric emergency department. Int. J. Environ. Res. Public Health 2021, 18, 6573. [Google Scholar] [CrossRef]
- Zee-Cheng, J.E.; McCluskey, C.K.; Klein, M.J.; Scanlon, M.C.; Rotta, A.T.; Shein, S.L.; Pineda, J.A.; Remy, K.E.; Carroll, C.L. Changes in Pediatric ICU Utilization and Clinical Trends During the Coronavirus Pandemic. Chest 2021, 160, 529–537. [Google Scholar] [CrossRef]
- Rady, M.Y.; Nightingale, P.; Little, R.A.; Edwards, J.D. Shock index: A re-evaluation in acute circulatory failure. Resuscitation 1992, 23, 227–234. [Google Scholar] [CrossRef]
- Nice. Major trauma: Assessment and initial management. Natl. Inst. Health Care Excell. 2018, 197–201. Available online: www.nice.org.uk (accessed on 1 October 2022).
- Parenti, N.; Manfredi, R.; Bacchi Reggiani, M.L.; Sangiorgi, D.; Lenzi, T. Reliability and validity of an Italian four-level emergency triage system. Bologna Emerg. Med. J. 2010, 27, 495–498. [Google Scholar] [CrossRef]
- Van Ditshuizen, J.C.; Sewalt, C.A.; Palmer, C.S.; Van Lieshout, E.M.M.; Verhofstad, M.H.J.; Den Hartog, D. The definition of major trauma using different revisions of the abbreviated injury scale. Scand. J. Trauma Resusc. Emerg. Med. 2021, 29, 1–10. [Google Scholar] [CrossRef]
- Committee on Medical Aspects of Automotive Safety. Rating the Severity of Tissue Damage: I. The Abbreviated Scale. JAMA 1972, 215, 277–280. [Google Scholar]
- Spahn, D.R.; Bouillon, B.; Cerny, V.; Duranteau, J.; Filipescu, D.; Hunt, B.J. The European guideline on management of major bleeding and coagulopathy following trauma: Fifth edition. Crit. Care 2019, 23, 1–74. [Google Scholar]
- Olasveengen, T.M.; Semeraro, F.; Ristagno, G.; Castren, M.; Handley, A.; Kuzovlev, A.; Monsieurs, K.G.; Raffay, V.; Smyth, M.; Soar, M.; et al. Basic life support: European Resuscitation Council Guidelines 2021. Notf. Und Rett. 2021, 24, 386–405. [Google Scholar] [CrossRef]
- Mikrogianakis, A.; Grant, V. The Kids Are Alright: Pediatric Trauma Pearls. Emerg. Med. Clin. N. Am. 2018, 36, 237–257. [Google Scholar] [CrossRef]
- Chiara, O.; Cimbanassi, S. Protocolli per la Gestione Intraospedaliera del Trauma Maggiore; Elsevier: Amsterdam, The Netherlands, 2008. [Google Scholar]
- Hamill, J. Damage control surgery in children. Injury 2004, 35, 707–711. [Google Scholar] [CrossRef]
- Sherman, W.F.; Khadra, H.S.; Kale, N.N.; Wu, V.J.; Gladden, P.B.; Lee, O.C. How Did the Number and Type of Injuries in Patients Presenting to a Regional Level I Trauma Center Change During the COVID-19 Pandemic with a Stay-at-home Order? Clin. Orthop. Relat. Res. 2021, 479, 266–275. [Google Scholar] [CrossRef]
- Hatchimonji, J.S.; Swendiman, R.A.; Seamon, M.J.; Nance, M.L. Trauma Does not Quarantine: Violence During the COVID-19 Pandemic. Ann. Surg. 2020, 272, e53–e54. [Google Scholar] [CrossRef]
- Sidpra, J.; Abomeli, D.; Hameed, B. Rise in the incidence of abusive head trauma during the COVID-19 pandemic. BMJ Arch. Dis. Child. 2021, 106, 1. [Google Scholar] [CrossRef]
- Giudici, R.; Lancioni, A.; Gay, H.; Bassi, G.; Chiara, O.; Mare, C.; Latronico, N.; Pesenti, A.; Faccincani, R.; Cabrini, L.; et al. Impact of the COVID-19 outbreak on severe trauma trends and healthcare system reassessment in Lombardia, Italy: An analysis from the regional trauma registry. World J. Emerg. Surg. 2021, 16, 1–8. [Google Scholar] [CrossRef]
- Theodorou, C.M.; Yamashiro, K.J.; Stokes, S.C.; Salcedo, E.S.; Hirose, S.; Beres, A.L. Pediatric suicide by violent means: A cry for help and a call for action. Inj. Epidemiol. 2022, 9, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Sisler, S.M.; Schapiro, N.A.; Nakaishi, M.; Steinbuchel, P. Suicide assessment and treatment in pediatric primary care settings. J. Child Adolesc. Psychiatr. Nurs. 2020, 33, 187–200. [Google Scholar] [CrossRef] [PubMed]
- Qasim, Z.; Sjoholm, L.O.; Volgraf, J.; Sailes, S.; Nance, M.L.; Perks, D.H.; Grewal, H.; Meyer, L.K.; Walker, J.; Koenig, G.J.; et al. Trauma center activity and surge response during the early phase of the COVID-19 pandemic—The Philadelphia story. J. Trauma Acute Care Surg. 2020, 89, 821–828. [Google Scholar] [CrossRef]
- Kuok, C.I.; Chan, W.K.Y.; Kwok, A.W.L. What and who should we focus in pediatric injury prevention e An analysis of critical pediatric trauma in a major trauma center in Hong Kong. Pediatr. Neonatol. 2021, 62, 620–627. [Google Scholar]
- Cantor, R.M.; Leaming, J.M. Evaluation and management of pediatric major trauma. Emerg. Med. Clin. North Am. 1998, 16, 229–256. [Google Scholar] [CrossRef]
- Ringen, A.H.; Baksaas-aasen, K.; Skaga, N.O.; Wisborg, T.; Gaarder, C.; Naess, P.A. Close to zero preventable in-hospital deaths in pediatric trauma patients—An observational study from a major Scandinavian trauma. Injury 2022, 54, 183–188. [Google Scholar] [CrossRef]
- Paneitz, D.C.; Ahmad, S. Pediatric Trauma Update. Mo Med. 2018, 115, 438–442. [Google Scholar] [PubMed]
- Li, G.; Ling, J.; DiScala, C.; Nordenholz, K.; Sterling, S.; Baker, S.P. Characteristics and outcomes of self inflicted pediatric injuries: The role of method of suicide attempt. Inj. Prev. 1997, 3, 115–119. [Google Scholar] [CrossRef] [Green Version]
- Avdimiretz, N.; Phillips, L.; Bratu, I. Focus on pediatric intentional trauma. J. Trauma Acute Care Surg. 2012, 72, 1031–1034. [Google Scholar] [CrossRef]
- Lee, J. Mental health effects of school closures during COVID-19. Lancet 2020, 4, 421. [Google Scholar] [CrossRef]
- Bergman, A.B.; Rivara, F.P. Sweden’s experience in reducing childhood injuries. Pediatrics 1991, 1, 69–74. [Google Scholar] [CrossRef]
- UNICEF. The State of the World’s Children 2021: On My Mind--Promoting, Protecting and Caring for Children’s Mental Health; United Nations Plaza: New York, NY, USA, 2021; pp. 1–15. [Google Scholar]
- Manetti, S.; Panza, C. Repercussions of the COVID-19 Pandemic on Child and Adolescent Mental health: A matter of concern—A joint statement from EAP and ECPCP. ACP 2020, 27, 3–5. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| 2015 (N = 84) | 2016 (N = 98) | 2017 (N = 125) | 2018 (N = 119) | 2019 (N = 114) | 2020 (N = 144) | p | |
|---|---|---|---|---|---|---|---|
| Sex (male), n (%) | 63 (75) | 70 (71.4) | 83 (66.4) | 77 (64.7) | 70 (61.4) | 90 (62.5) | 0.280 |
| Age (years) | 10 (±5.4) | 9.9 (±5) | 9.6 (±5.2) | 10 (±5.2) | 9.8 (±5.1) | 10.1 (±5.2) | 0.977 |
| Mechanism of trauma, n (%)
| 45 (53.6) 30 (35.7) 2 (2.4) 7 (8.3) | 56 (57.1) 35 (35.7) 0 (0) 7 (7.1) | 72 (57.6) 42 (33.6) 4 (3.2) 7 (5.6) | 72 (60.5) 33 (27.8) 1 (0.8) 13 (10.9) | 65 (57) 37 (32.5) 1 (0.9) 11 (9.6) | 75 (52.1) 47 (32.6) 6 (4.2) 16 (11.1) | 0.808 0.830 0.168 0.112 |
| Type of trauma (blunt), n (%) | 82 (97.6) | 94 (95.9) | 123 (98.4) | 115 (96.6) | 109 (95.6) | 139 (96.5) | 0.847 |
Trauma intentionality, n (%)
| 3 (3.6) 1 (1.2) | 3 (3.1) 2 (2) | 8 (6.5) 5 (4) | 9 (7.6) 5 (4.2) | 9 (7.9) 6 (5.3) | 14 (9.8) 9 (6.2) | 0.020 0.029 |
Type of ED access, n (%)
| 7 (8.3) | 7 (7.1) | 10 (8) | 9 (7.6) | 0 (0) | 19 (13.2) | 0.020 |
Triage code, n (%)
| 7 (8.3) 70 (83.4) 7 (8.3) | 8 (8.2) 82 (83.6) 8 (8.2) | 13 (10.4) 100 (80) 12 (9.6) | 9 (7.6) 95 (79.8) 15 (12.6) | 5 (4.4) 82 (71.9) 27 (23.7) | 36 (25) 89 (61.8) 19 (13.2) | <0.001 <0.001 0.015 |
| 2015 (N = 84) | 2016 (N = 98) | 2017 (N = 125) | 2018 (N = 119) | 2019 (N = 114) | 2020 (N = 144) | p | |
|---|---|---|---|---|---|---|---|
| BP-pre (mmHg) | 120 (110–130) | 120 (110–130) | 120 (100–130) | 118 (102–130) | 116 (100–127) | 113 (105–130) | 0.064 |
| HR-pre (bpm) | 100 (90–120) | 98 (87–117) | 100 (85–120) | 100 (90–120) | 100 (82–120) | 100 (86–110) | 0.620 |
| GCS-pre | 15 | 15 | 15 | 15 | 15 | 15 | 1 |
| BP-ED (mmHg) | 120 (105–130) | 120 (110–125) | 120 (100–130) | 120 (105–127) | 119 (105–127) | 115 (103–130) | 0.903 |
| HR-ED (bpm) | 97 (80–110) | 100 (86–115) | 100 (85–115) | 100 (87–120) | 100 (85–113) | 100 (85–113) | 0.775 |
| GCS-ED | 15 | 15 | 15 | 15 | 15 | 15 | 1 |
| Head | Chest | Abdomen | Extremities | |
|---|---|---|---|---|
| Fall (n = 54) | 29 | 31 | 18 | 20 |
| Car (n = 11) | 5 | 6 | 1 | 5 |
| Motorbike (n = 16) | 3 | 6 | 3 | 7 |
| Bicycle (n = 13) | 6 | 5 | 3 | 1 |
| Pedestrian (n = 26) | 15 | 14 | 3 | 7 |
| Assault (n = 1) | 1 | 0 | 0 | 0 |
| Stab wound (n = 1) | 0 | 0 | 1 | 0 |
| Sports trauma (n = 4) | 3 | 0 | 1 | 0 |
| Miscellaneous (n = 4) | 2 | 0 | 0 | 2 |
| 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | p | ||||||||
| (n = 84) | (n = 98) | (n = 125) | (n = 117) | (n = 119) | (n = 144) | |||||||||
| <13 y | ≥13 y | <13 y | ≥13 y | <13 y | ≥13 y | <13 y | ≥13 y | <13 y | ≥13 y | <13 y | ≥13 y | |||
| (n = 51) | (n = 33) | (n = 62) | (n = 36) | (n = 79) | (n = 46) | (n = 74) | (n = 43) | (n = 69) | (n = 45) | (n = 80) | (n = 63) | |||
| Intentionality, n (%) | Accident | 50 (98) | 31 (93.9) | 61 (98.4) | 34 (94.4) | 77 (97.5) | 40 (87) | 71 (95.9) | 37 (86) | 66 (95.7) | 39 (86.7) | 80 (100) | 49 (77.8) | 0.06 |
| VRT | 1 (2) | 2 (6.1) | 1 (1.6) | 2 (5.6) | 2 (2.5) | 6 (13) | 3 (4.1) | 6 (14) | 3 (4.3) | 6 (13.3) | 0 (0) | 14 (22.2) | 0.02 | |
| SA | 1 (2) | 0 (0) | 0 (0) | 2 (5.6) | 1 (1.3) | 4 (11.5) | 0 (0) | 5 (11.6) | 1 (1.4) | 5 (11.1) | 0 (0) | 9 (14.3) | 0.03 | |
| Mechanisms, n (%) | Car | 11 (21.6) | 1 (3) | 7 (11.3) | 2 (5.6) | 12 (15.2) | 3 (6.5) | 5 (6.8) | 1 (2.3) | 11 (15.9) | 3 (6.7) | 9 (11.3) | 8 (12.7) | 0.86 |
| Motorbike | 1 (2) | 6 (18.2) | 0 (0) | 6 (16.7) | 3 (3.8) | 7(15.2) | 1 (1.4) | 14 (32.6) | 0 (0) | 8 (17.8) | 0 (0) | 8 (12.7) | 0.66 | |
| Bicycle | 0 (0) | 1 (3) | 6 (9.7) | 7 (19.4) | 6 (7.6) | 12 (26.1) | 6 (8.1) | 8 (18.6) | 7 (10.1) | 7 (15.6) | 13 (16.3) | 8 (12.7) | 0.03 | |
| Electric scooter | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (1.3) | 3 (4.8) | 0.01 | |
| Pedestrian | 13 (25.5) | 12 (36.4) | 17 (27.4) | 11 (30.6) | 21 (26.6) | 8 (17.4) | 26 (35.1) | 9 (20.9) | 19 (27.5) | 10 (22.2) | 12 (15) | 11 (17.5) | 0.03 | |
| Fall | 22 (43.1) | 8 (24.2) | 29 (46.8) | 6 (16.7) | 33 (41.8) | 9 (19.6) | 25 (33.8) | 8 (18.6) | 28 (40.6) | 9 (20) | 30 (37.5) | 17 (27) | 0.49 | |
| Stabbing | 0 (0) | 1 (3) | 0 (0) | 0 (0) | 0 (0) | 1 (2.2) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 4 (6.3) | 0.18 | |
| Assault | 0 (0) | 1 (3) | 0 (0) | 0 (0) | 1 (1.3) | 2 (4.3) | 0 (0) | 1 (2.3) | 0 (0) | 1 (2.2) | 1 (1.3) | 1 (1.6) | 0.83 | |
| Sport trauma | 0 (0) | 2 (6.1) | 2 (3.2) | 1 (2.8) | 1 (1.3) | 3 (6.5) | 3 (4.1) | 1 (2.3) | 0 (0) | 1 (2.2) | 0 (0) | 1 (1.6) | 0.15 | |
| Other | 4 (7.8) | 1 (3) | 1 (1.6) | 3 (8.3) | 2 (2.5) | 1 (2.2) | 8 (10.8) | 1 (2.3) | 4 (5.8) | 6 (13.3) | 14 (17.5) | 1 (1.6) | 0.02 | |
| 0–12 (n = 415) | 13–18 (n = 269) | p | ||
|---|---|---|---|---|
| Head-AIS15, n (%) | 1 | 99 (23.8) | 28 (10.4) | <0.001 |
| 2 | 45 (10.8) | 51 (18.9) | ||
| 3 | 22 (5.3) | 21 (7.8) | ||
| 4 | 9 (2.2) | 7 (2.6) | ||
| 5 | 4 (0.9) | 10 (3.7) | ||
| Chest-AIS15, n (%) | 1 | 0 (0) | 0 (0) | 0.195 |
| 2 | 8 (1.9) | 15 (5.6) | ||
| 3 | 20 (4.8) | 21 (7.8) | ||
| 4 | 5 (1.2) | 13 (4.8) | ||
| 5 | 0 (0) | 3 (1.1) | ||
| Abdomen-AIS15, n (%) | 1 | 0 (0) | 1 (0.4) | 0.272 |
| 2 | 15 (3.6) | 25 (9.3) | ||
| 3 | 8 (1.9) | 10 (3.7) | ||
| 4 | 3 (0.7) | 6 (2.2) | ||
| 5 | 0 (0) | 7 (2.6) | ||
| Extremity-AIS15. N (%) | 1 | 8 (1.9) | 16 (5.9) | 0.042 |
| 2 | 64 (15.4) | 50 (18.6) | ||
| 3 | 18 (4.3) | 32 (11.9) | ||
| 4 | 5 (1.2) | 8 (2.9) | ||
| 5 | 1 (0.2) | 4 (1.5) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maina, C.; Cioffi, S.P.B.; Altomare, M.; Spota, A.; Virdis, F.; Bini, R.; Ragozzino, R.; Renzi, F.; Reitano, E.; Corasaniti, L.; et al. Increasing Trend in Violence-Related Trauma and Suicide Attempts among Pediatric Trauma Patients: A 6-Year Analysis of Trauma Mechanisms and the Effects of the COVID-19 Pandemic. J. Pers. Med. 2023, 13, 128. https://doi.org/10.3390/jpm13010128
Maina C, Cioffi SPB, Altomare M, Spota A, Virdis F, Bini R, Ragozzino R, Renzi F, Reitano E, Corasaniti L, et al. Increasing Trend in Violence-Related Trauma and Suicide Attempts among Pediatric Trauma Patients: A 6-Year Analysis of Trauma Mechanisms and the Effects of the COVID-19 Pandemic. Journal of Personalized Medicine. 2023; 13(1):128. https://doi.org/10.3390/jpm13010128
Chicago/Turabian StyleMaina, Cecilia, Stefano Piero Bernardo Cioffi, Michele Altomare, Andrea Spota, Francesco Virdis, Roberto Bini, Roberta Ragozzino, Federica Renzi, Elisa Reitano, Lucia Corasaniti, and et al. 2023. "Increasing Trend in Violence-Related Trauma and Suicide Attempts among Pediatric Trauma Patients: A 6-Year Analysis of Trauma Mechanisms and the Effects of the COVID-19 Pandemic" Journal of Personalized Medicine 13, no. 1: 128. https://doi.org/10.3390/jpm13010128