
Three-Dimensional Accuracy and Stability of Personalized Implants in Orthognathic Surgery: A Systematic Review and a Meta-Analysis
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Eligibility Criteria
2.3. Search Strategy
2.4. Data Collection
2.5. Risk of Bias Assessment
2.6. Meta-Analysis
3. Results
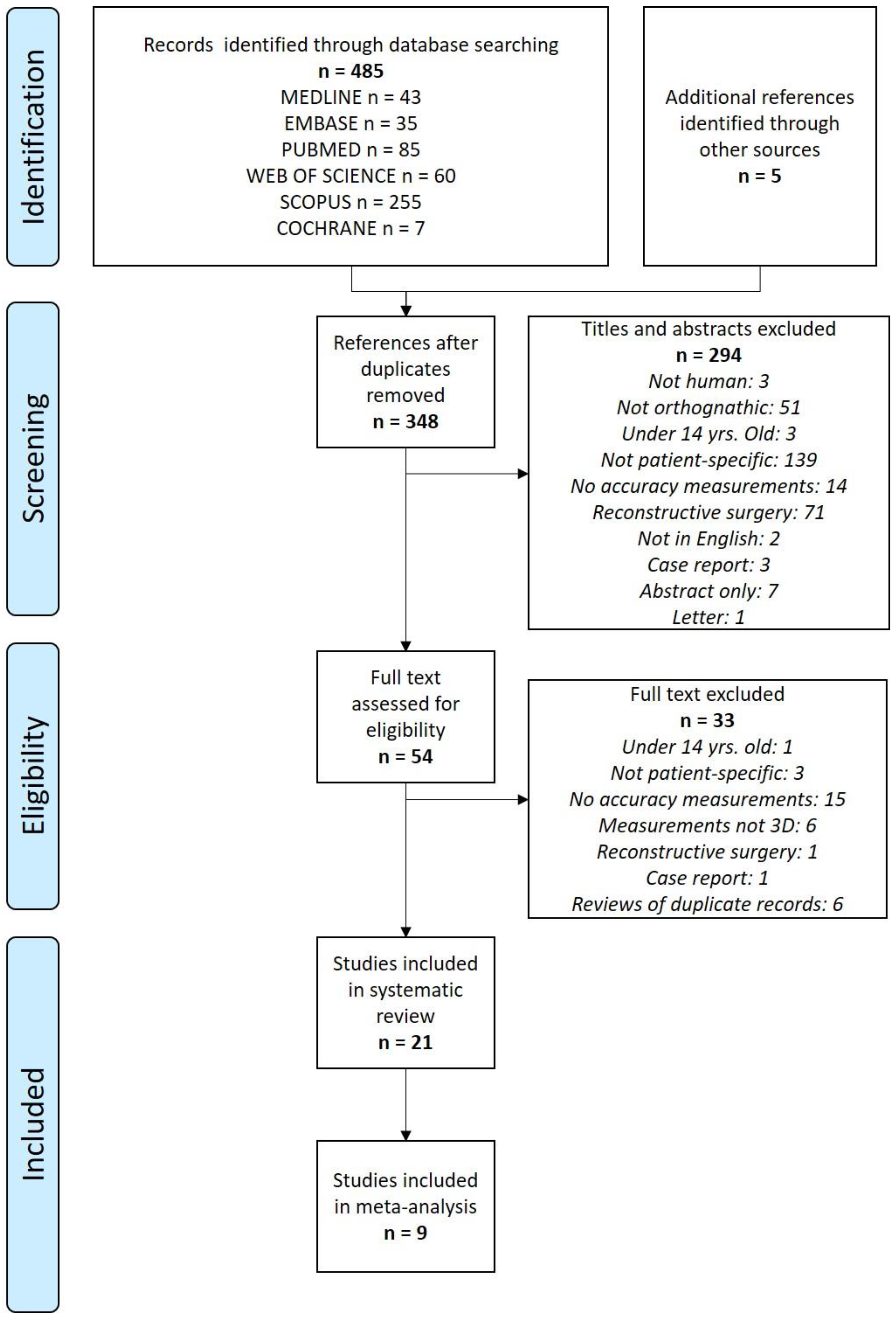
3.1. Liteature Search
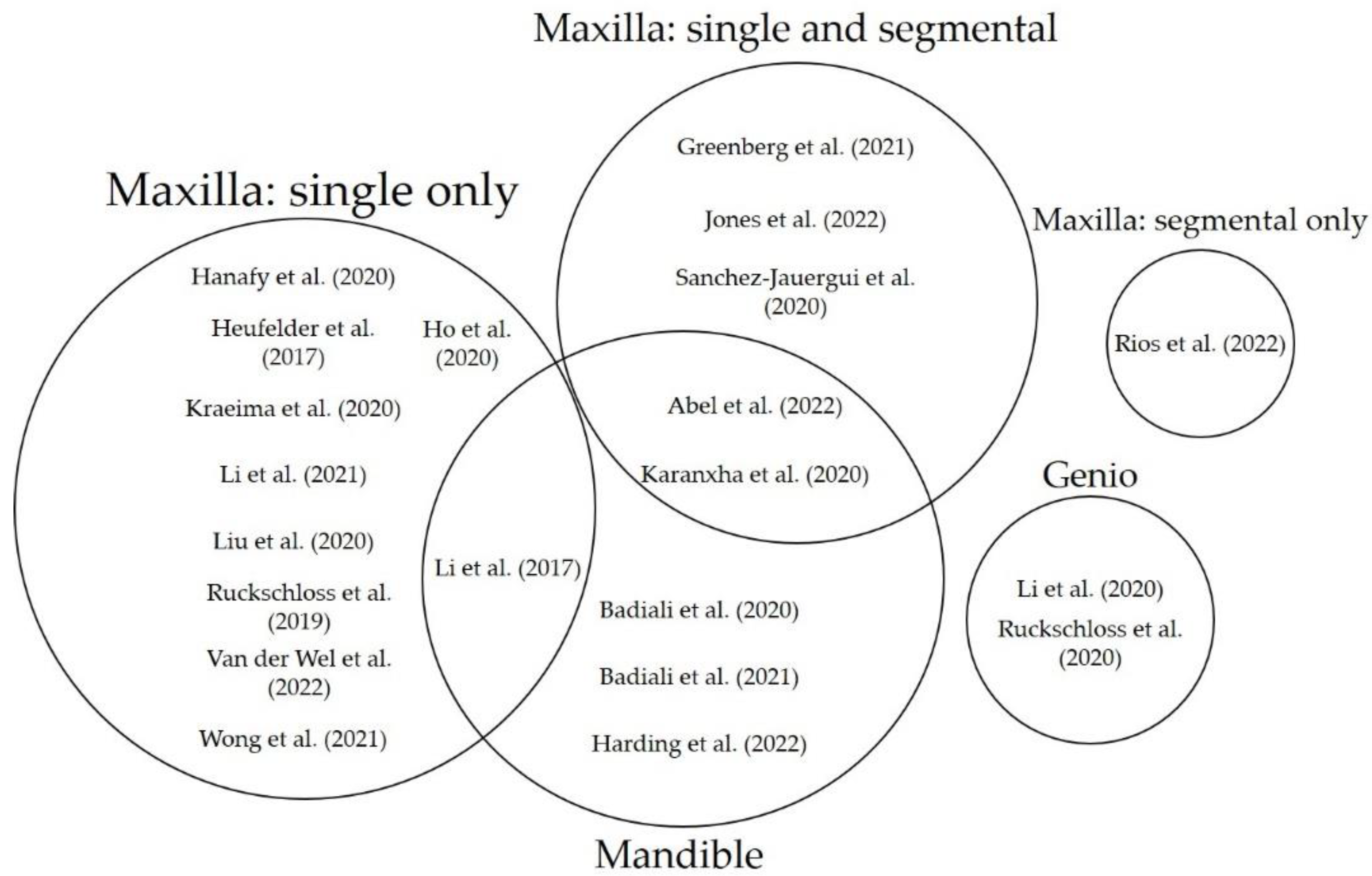
3.2. Characteristics of Eligible Studies
3.3. Risk of Bias
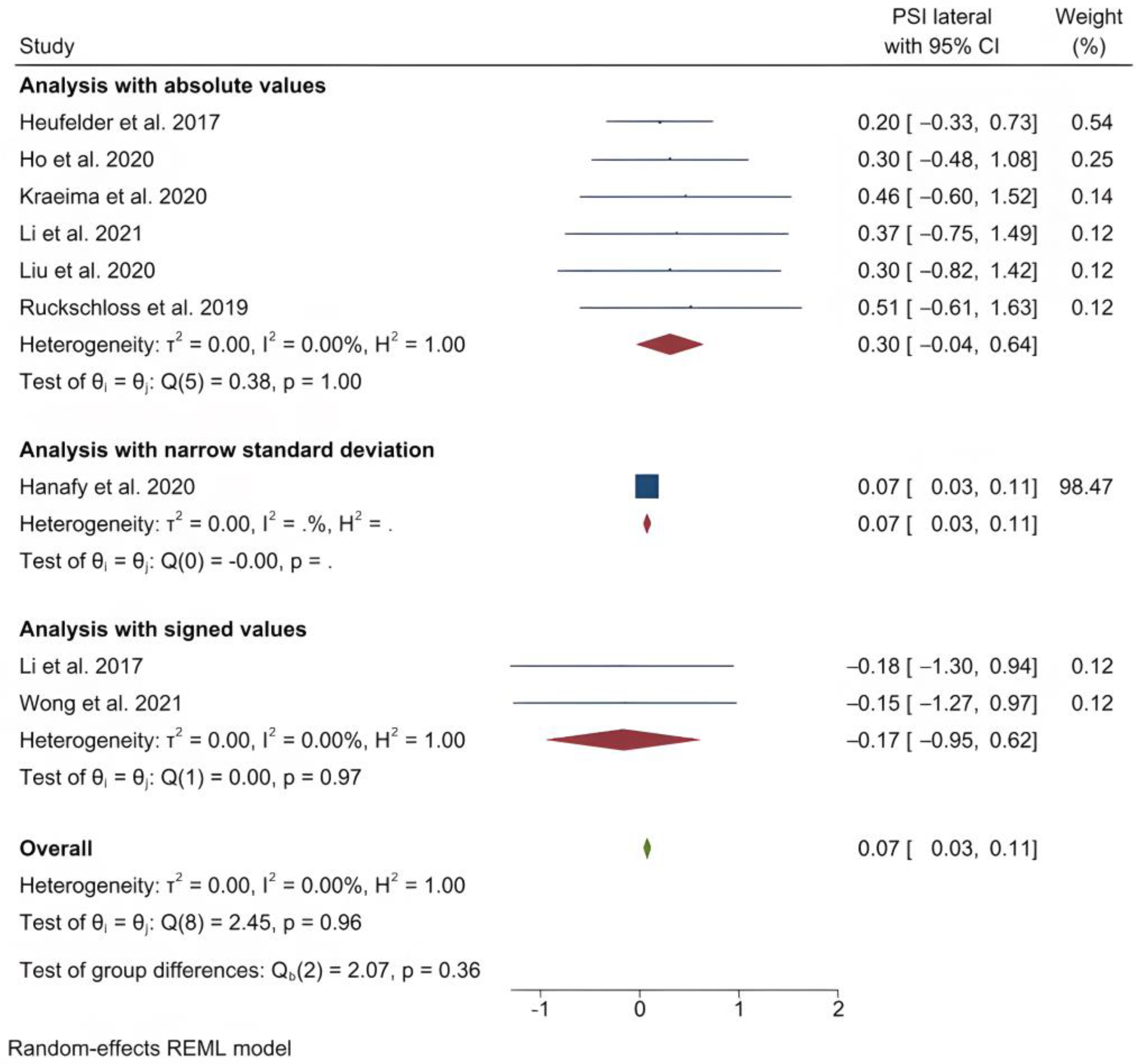
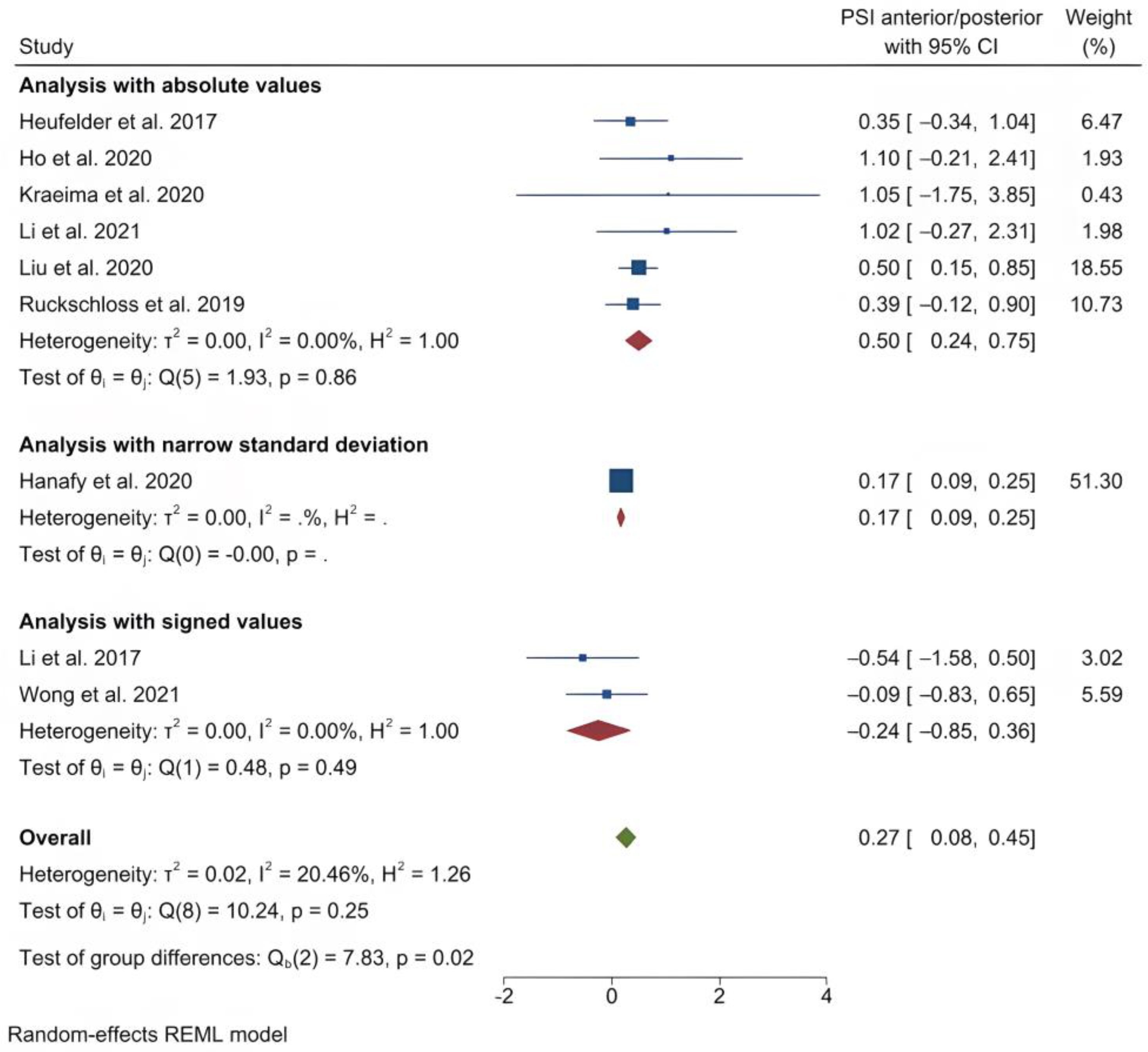
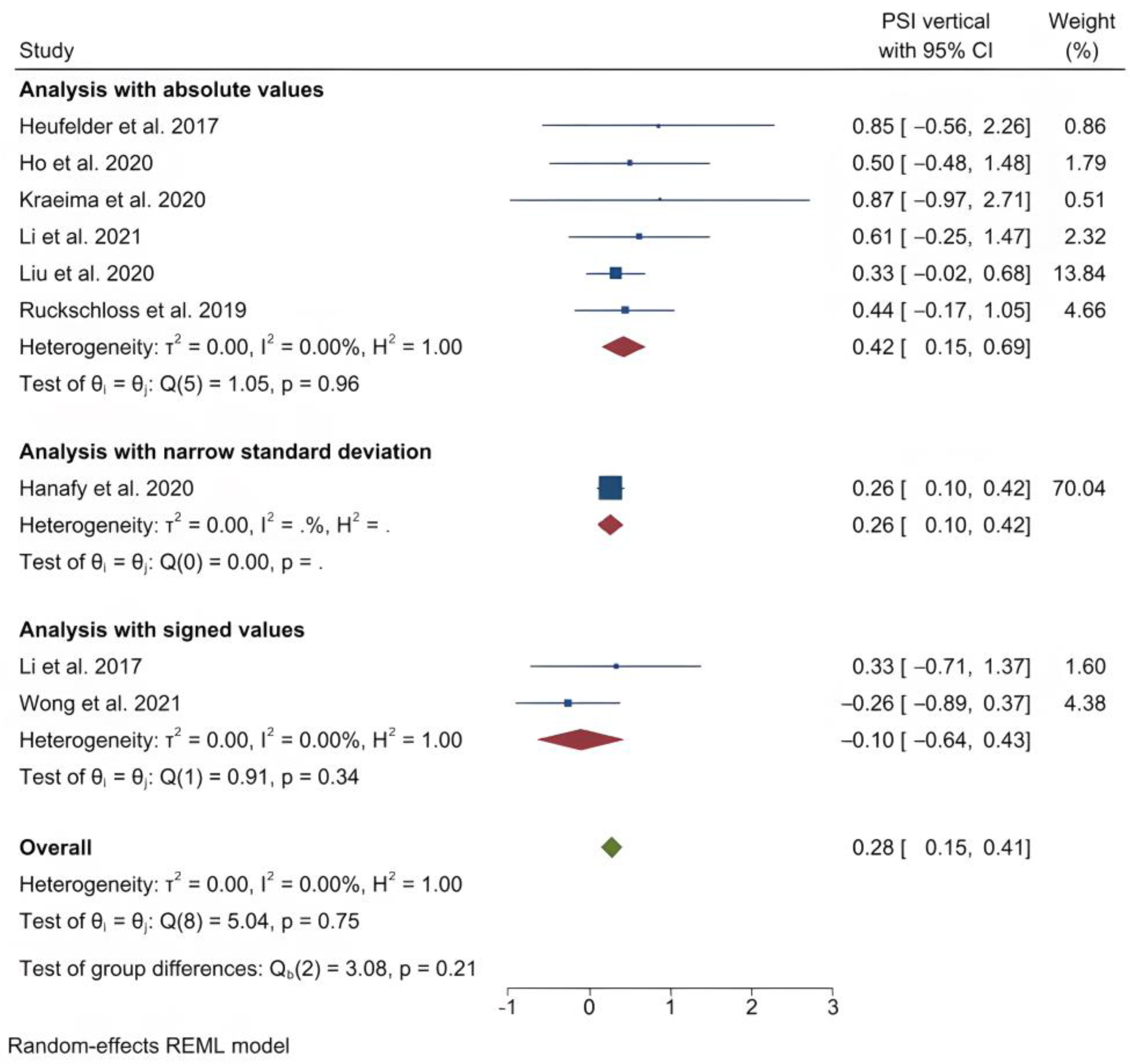
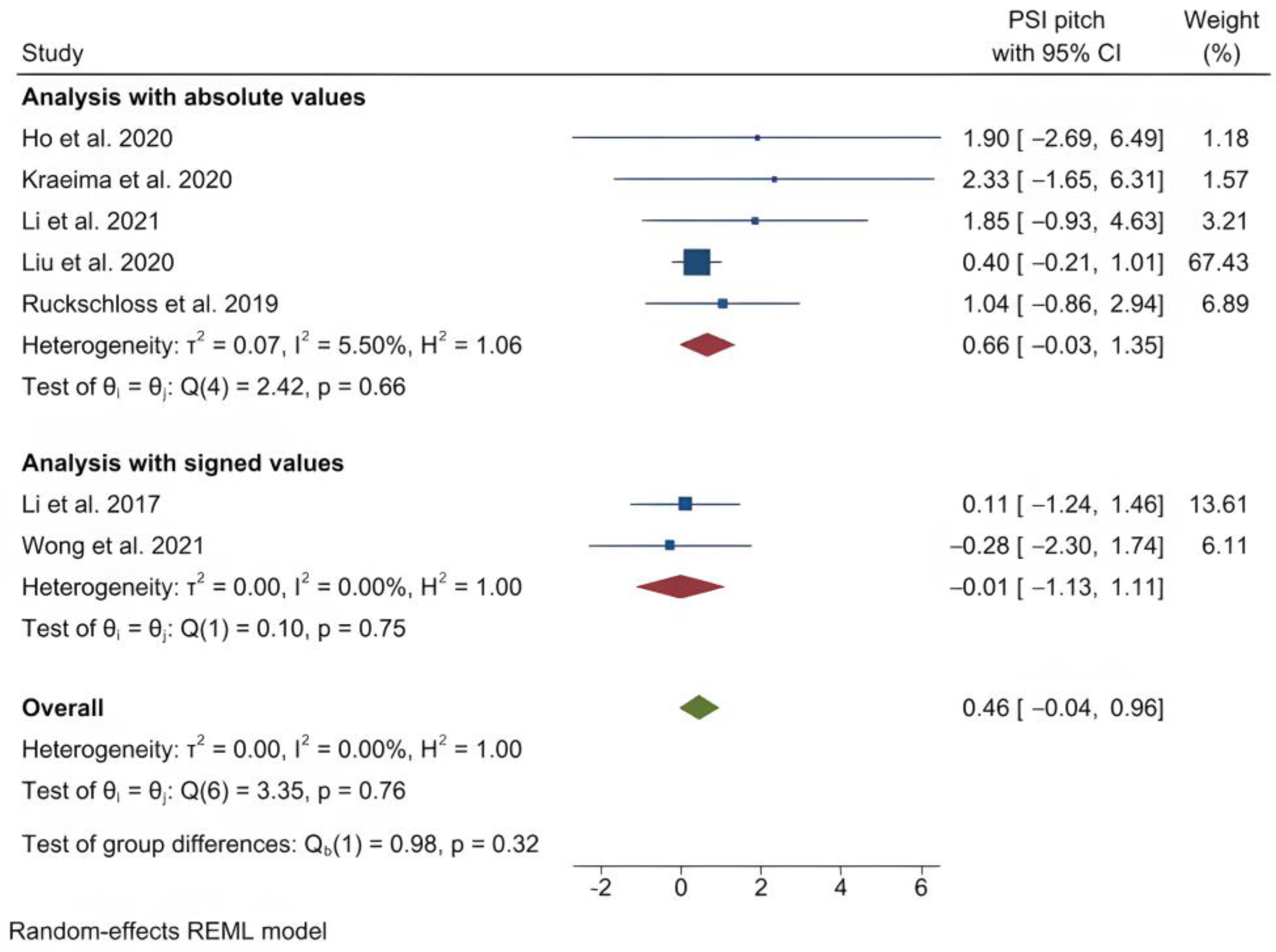
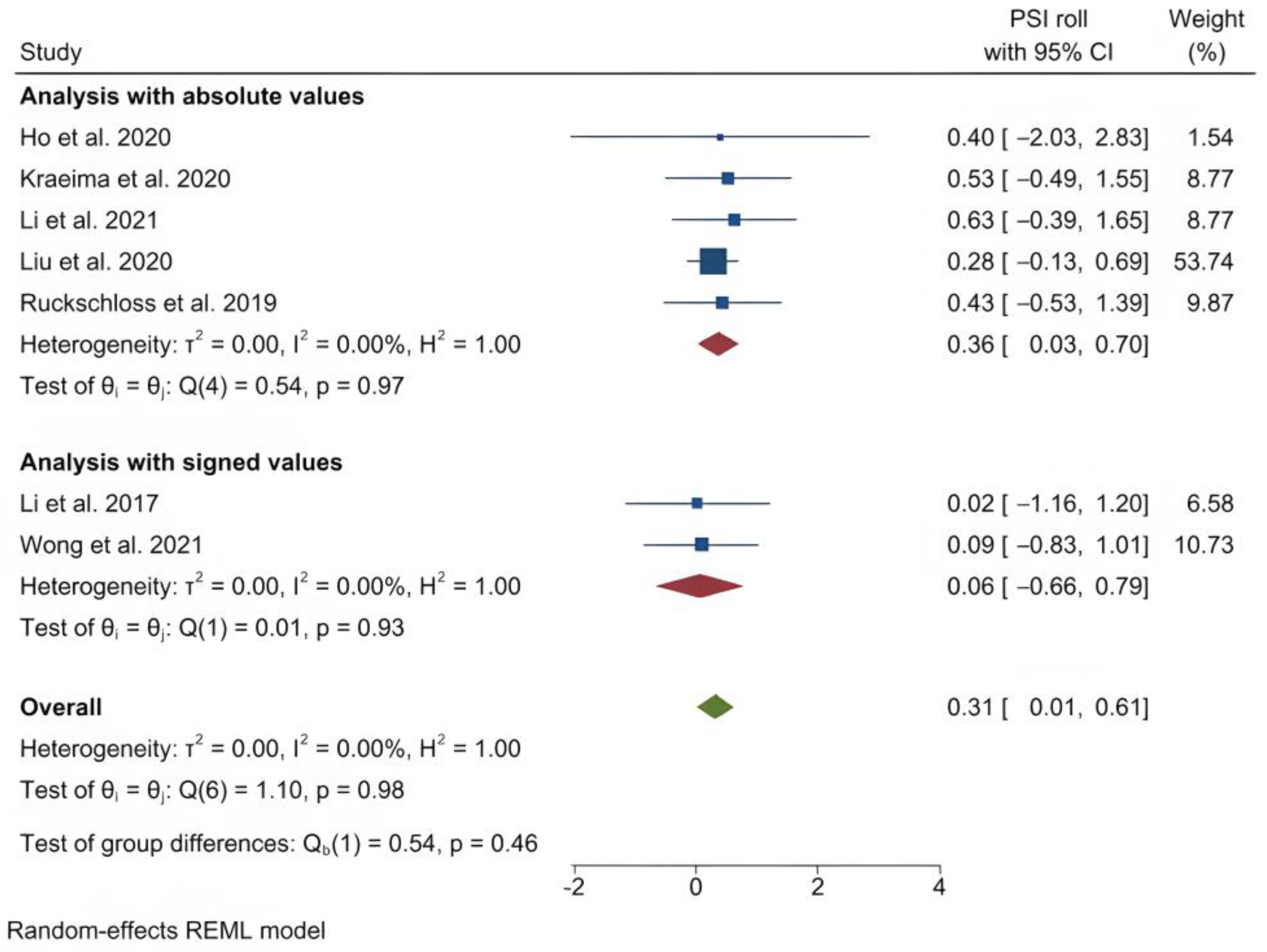
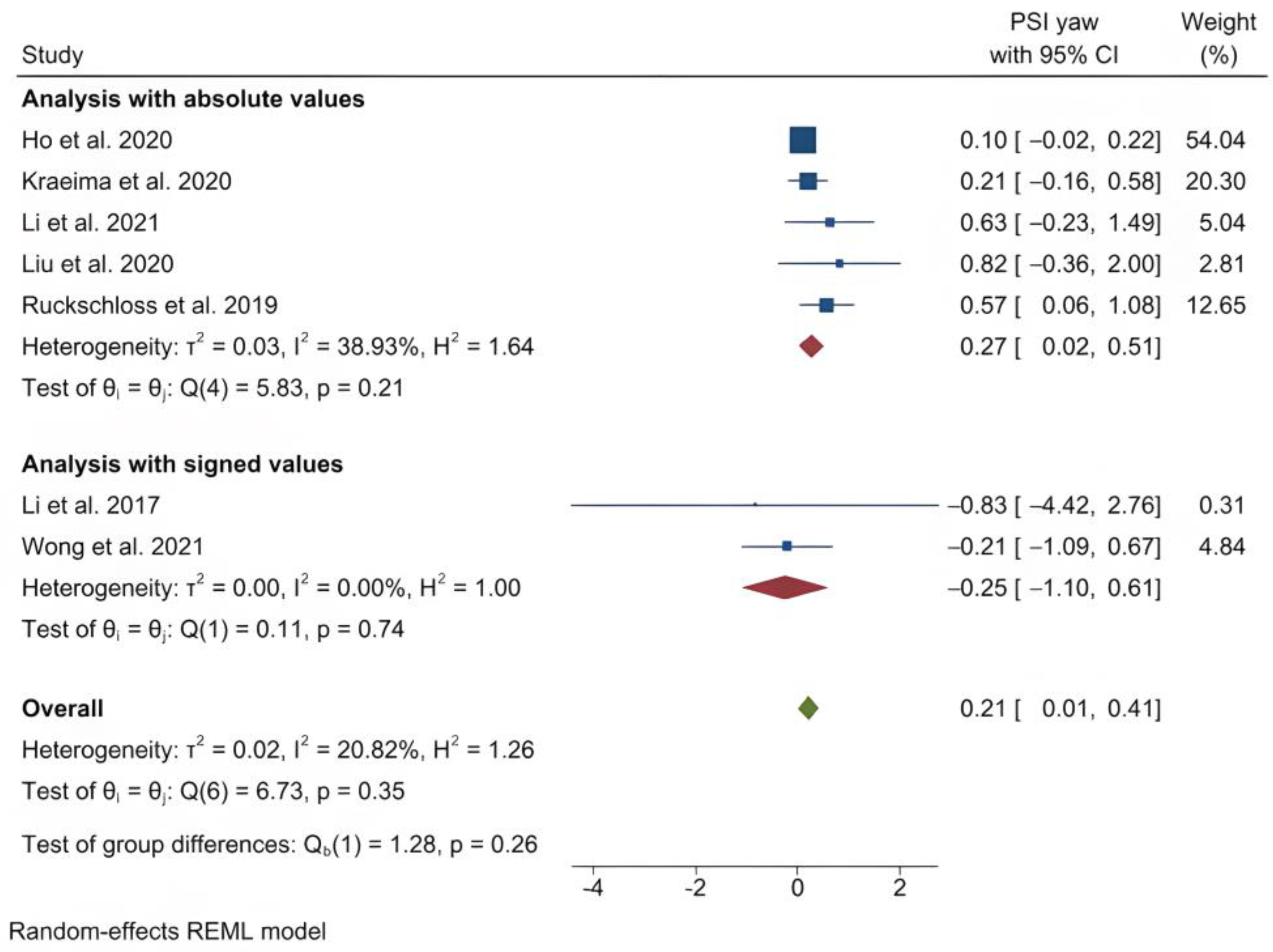
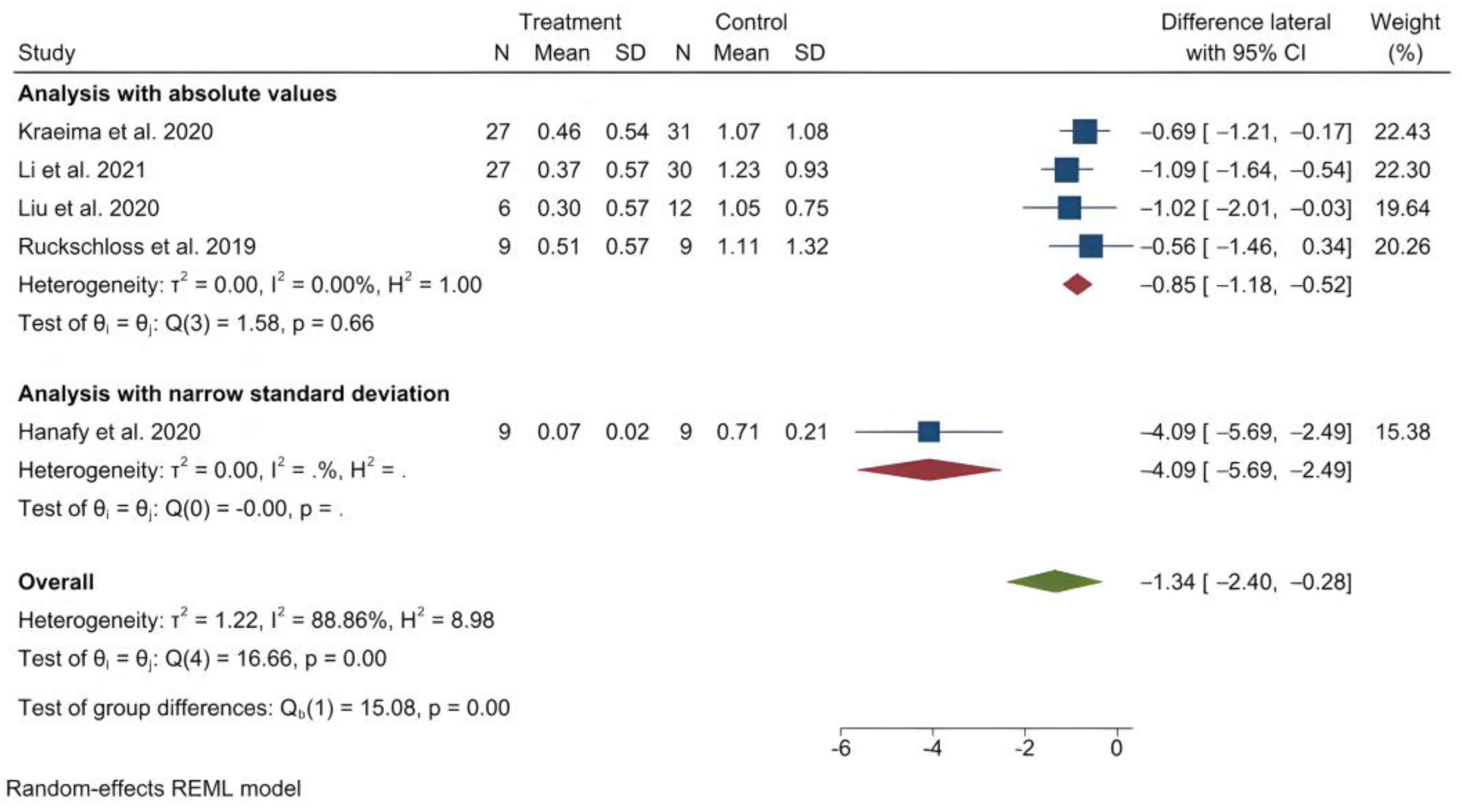
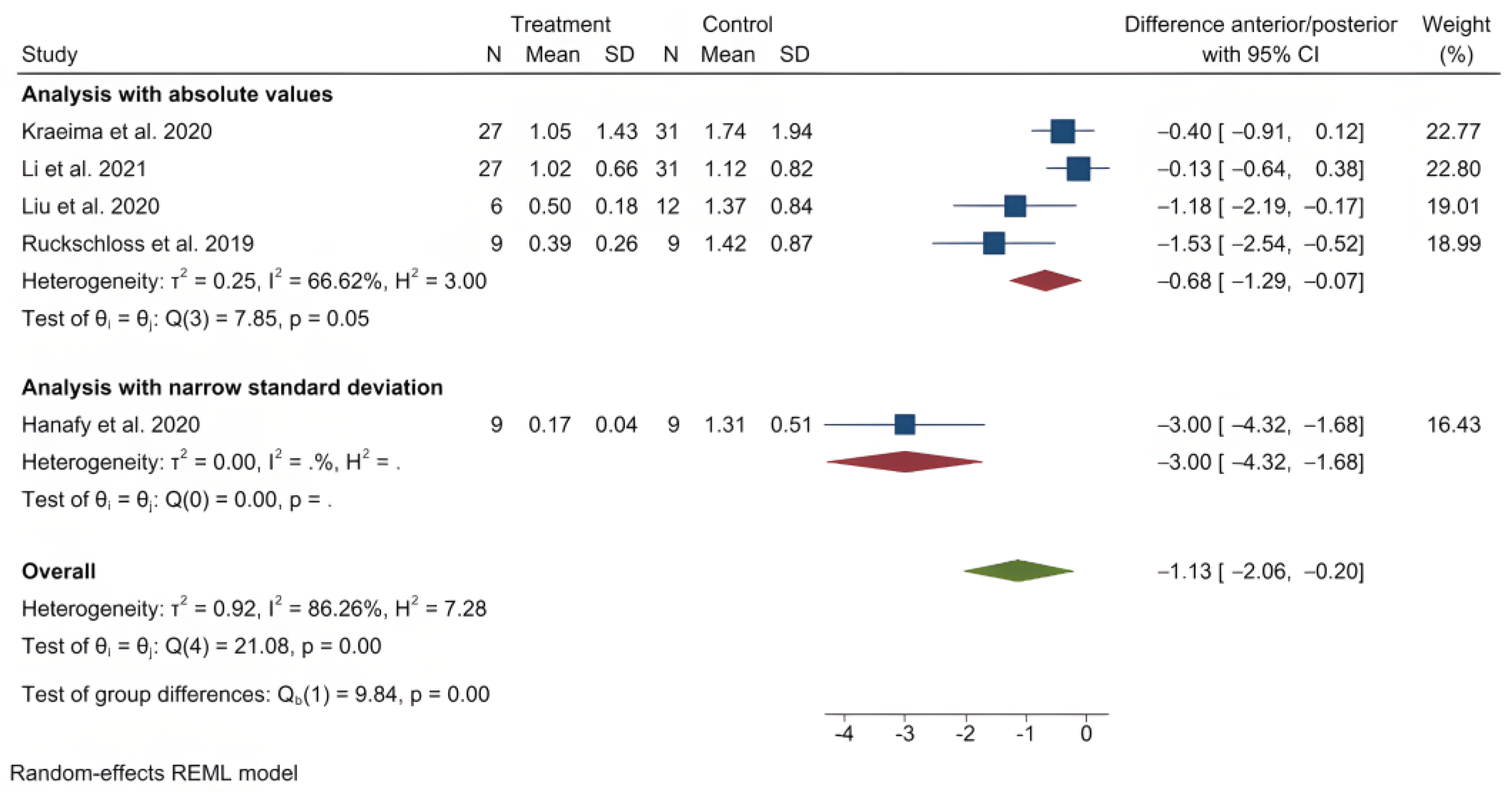
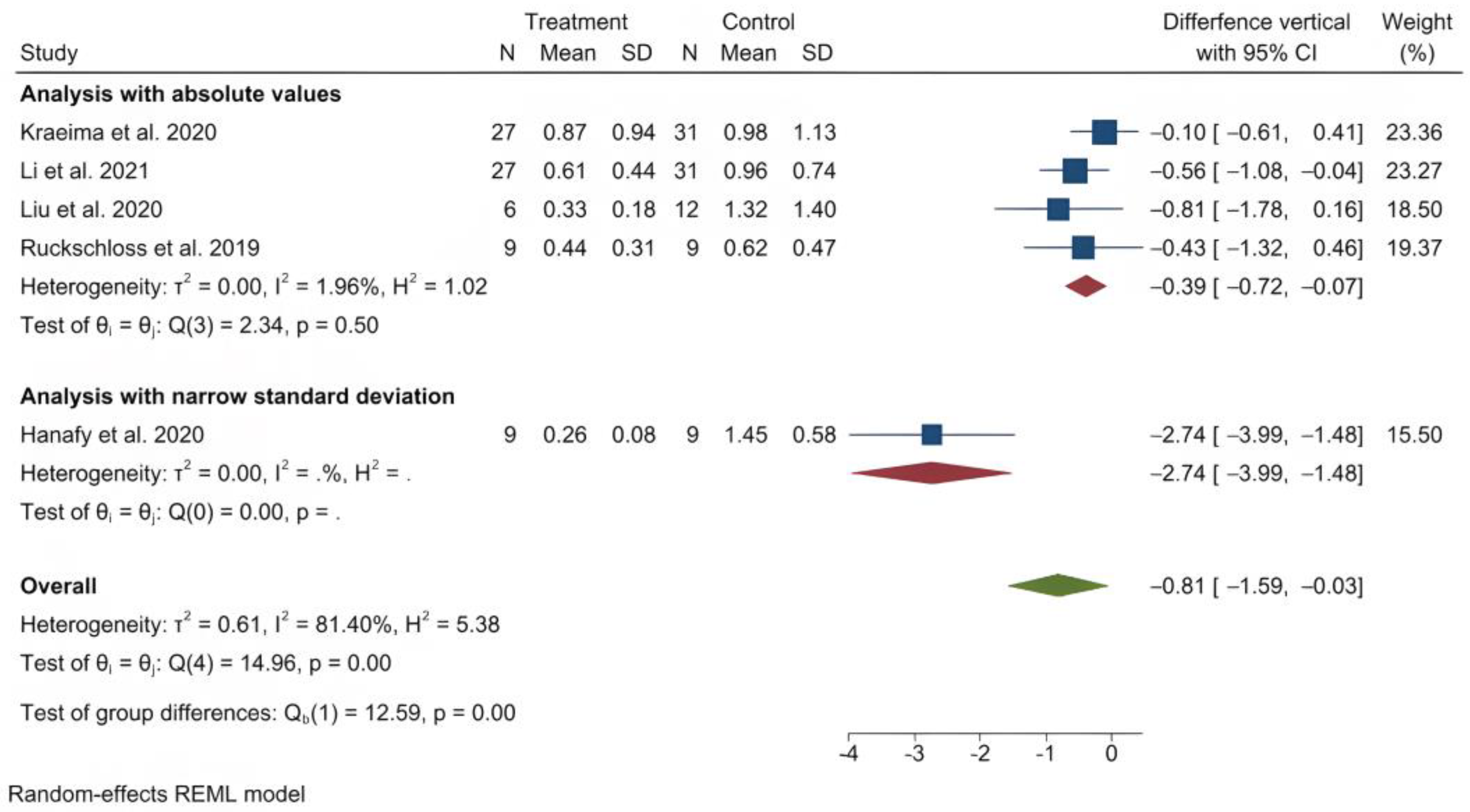
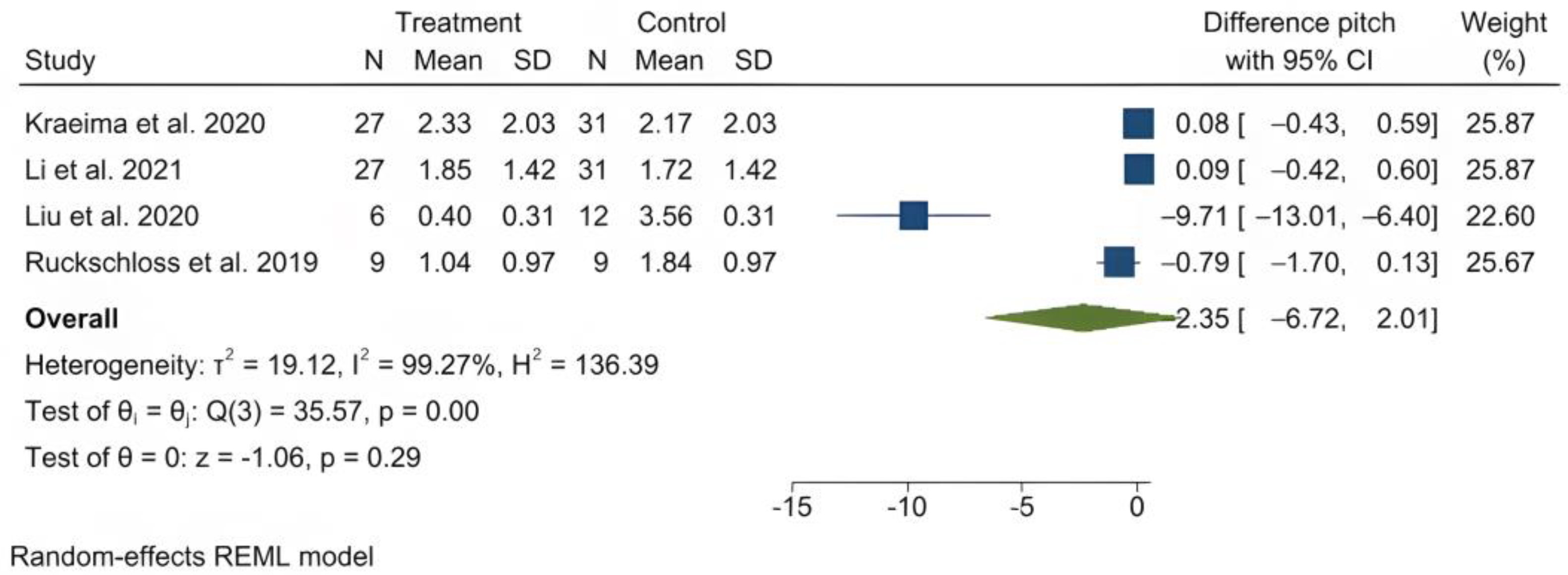
3.4. Meta-Analysis: PSI Accuracy in Single Le Fort I Osteotomy Procedures
3.5. Mixed Le Fort I Procedures
3.6. Segmental Le Fort I
3.7. Mandibular Osteotomy Procedures
3.8. Genioplasty Procedures
3.9. Stability
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Database Search Strings

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Database | Search phrase |
|---|---|
| Ovid Embase | (exp “orthognathic surgery”/OR exp “orthognathic surgical procedures”/OR genioplasty) AND (accuracy OR precision OR stability) AND (((“patient specific” OR patient-specific OR customized) AND (implant OR instrument)) OR PSI OR splintless OR waferless) |
| Ovid Medline | (exp “orthognathic surgery”/OR exp “orthognathic surgical procedures”/OR genioplasty) AND (accuracy OR precision OR stability) AND (((“patient specific” OR patient-specific OR customized) AND (implant OR instrument)) OR PSI OR splintless OR waferless) |
| PubMed | (“orthognathic surgery”[Mesh] OR “orthognathic surgical procedures”[Mesh] OR genioplasty) AND (accuracy OR precision OR stability) AND (((“patient specific” OR patient-specific OR customized) AND (implant OR instrument)) OR PSI OR splintless OR waferless) |
| Web of Science | ALL = ((“orthognathic surgery” OR “orthognathic surgical procedures” OR genioplasty) AND (accuracy OR precision OR stability) AND (((“patient specific” OR patient-specific OR customized) AND (implant OR instrument)) OR PSI OR splintless OR waferless)) |
| Scopus | (INDEXTERMS(“orthognathic surgery”) OR INDEXTERMS(“orthognathic surgical procedures”) OR genioplasty) AND (accuracy OR precision OR stability) AND (((“patient specific” OR patient-specific OR customized) AND (implant OR instrument)) OR PSI OR splintless OR waferless) |
| Cochrane Library | [mh “orthognathic surgery”] OR [mh “orthognathic surgical procedures”] OR genioplasty AND accuracy OR precision OR stability AND ((“patient specific” OR patient-specific OR customized) AND (implant OR instrument)) OR PSI OR splintless OR waferless |
Appendix B. Risk of Bias Assessment with Author’s Judgement
| Bias | Author’s Judgement | Support for Judgement |
|---|---|---|
| Random sequence generation | Low risk | “The patients were divided randomly into two equal groups using computer software” (p. 64) |
| Allocation concealment | Low risk | “numbers were concealed in closed envelopes” (p. 64) |
| Blinding of participants | Low risk | “Only the patients and the statistician were blinded, as the operator and the assessor would know the group allocation from the shape of the plate.” (p. 64) It is unlikely any present bias would affect the outcome. |
| Blinding of outcome | Low risk | “Only the patients and the statistician were blinded, as the operator and the assessor would know the group allocation from the shape of the plate.” (p. 64) It is unlikely any preset bias would affect the objective 3D measurements. |
| Incomplete outcome data addressed | Low risk | No loss of participants. |
| Selective reporting | Low risk | All pre-specified outcomes reported. |
| Bias | Author’s Judgement | Support for Judgement |
|---|---|---|
| Random sequence generation | Low risk | “Included patients were assigned to either the control group or the intervention group by means of blocked randomization.” (p. 455) |
| Allocation concealment | Unclear | Allocation concealment is unclear and may present a low risk of bias. |
| Blinding of participants | Unclear | It is unspecified whether there was blinding. However, any present bias is unlikely to affect the outcome of the procedure. |
| Blinding of outcome | Unclear | It is unspecified whether there was blinding. However, it is unlikely any preset bias would affect the objective 3D measurements. |
| Incomplete outcome data addressed | Low risk | “A total of 64 patients agreed to participate in the study and provided informed consent. However, only 58 completed the study protocol. Six patients were excluded from the PP analysis due to late changes in surgical planning (n = 1); damaged or in complete guides or PSO materials after sterilization (n = 4); and perioperative conversion to the control group protocol (n = 1).” (p. 457) Acceptable loss of 7%. |
| Selective reporting | Low risk | All pre-specified outcomes reported. |
| Bias | Author’s Judgement | Support for Judgement |
|---|---|---|
| Random sequence generation | Low risk | “The patients were assigned randomly by means of a block randomization procedure with the use of a computer-generated list of random numbers” (p. 1102) |
| Allocation concealment | Low risk | “The allocation sequence was concealed from the surgeons, enrolled patients, and the researcher” (p. 1102) |
| Blinding of participants | Low risk | “It was impossible to blind the patient and surgeon to the treatment group for the whole study, espe- cially during the operation. However, the surgeons and researchers were blinded to the treatment group during the virtual planning phase.” (p. 1102) |
| Blinding of outcome | Low risk | “The doctor performing the clinical examination after the operation was also blinded to the grouping” (p. 1102) |
| Incomplete outcome data addressed | Low risk | “A total of 64 patients were recruited and assigned randomly and equally to both groups. After exclud- ing those lost to follow-up (n = 1) and those who refused the operation (n = 5), 58 patients were included in the primary analysis (27 in the patient-specific implant group and 31 in the control group).” (p. 1106) Acceptable loss of 7% |
| Selective reporting | Low risk | All pre-specified outcomes reported. |
| Bias | Author’s Judgement | Support for Judgement |
|---|---|---|
| Random sequence generation | Low risk | “The included patients were divided into two groups by means of block randomization” (p. 2) |
| Allocation concealment | Unclear | Allocation concealment is unclear and may present a low risk of bias. |
| Blinding of participants | Unclear | It is unspecified whether there was blinding. However, any present bias is unlikely to affect the out- come of the procedure. |
| Blinding of outcome | Unclear | It is unspecified whether there was blinding. However, any present bias is unlikely to affect the accuracy measurements. |
| Incomplete outcome data addressed | High risk | “A total of 64 patients provided informed consent to participate in the RCT. Fifty-eight patients completed the protocol for the 2-week postoperative analysis, but unfortunately only 27 patients completed the 1-year follow-up study protocol. Reasons for drop-out between the 2-week and 1-year protocol were as follows: no CBCT dataset available due to ‘no show’ of the patient (n = 25) or CBCT scan was per- formed outside the follow up period (n = 6).” (pp. 3,4) “the statistical comparison between the directional and rotational sub-groups suffered from the skewed ness in group sizes. Considering the prevalence of relapse, the skewedness in group sizes might have influenced the results of the statistical comparison. Generally, the results of this study are limited by a relatively small sample size due to the large number of patients lost during follow-up.” (p. 6) At the one-year time point, a loss of 31 patients is reported. This is difficult to oversee and it may pre- sent a high risk of attrition bias. The previously established adequate sample size not achieved. At the two-week time point, the results for 31 patients are omitted in order to enable the comparison with the one-year time point. As such, it is incomplete outcome data, deemed as high risk of bias. |
| Selective reporting | Low risk | All pre-specified outcomes reported. |
References
- Figueiredo, C.E.; Paranhos, L.R.; da Silva, R.P.; Herval, Á.M.; Blumenberg, C.; Zanetta-Barbosa, D. Accuracy of orthognathic surgery with customized titanium plates—Systematic review. J. Stomatol. Oral Maxillofac. Surg. 2021, 122, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Williams, A.; Walker, K.; Hughes, D.; Goodson, A.M.C.; Mustafa, S.F. Accuracy and cost effectiveness of a waferless osteotomy approach, using patient specific guides and plates in orthognathic surgery: A systematic review. Br. J. Oral Maxillofac. Surg. 2022, 60, 537–546. [Google Scholar] [CrossRef] [PubMed]
- Huang, M.F.; Alfi, D.; Alfi, J.; Huang, A.T. The Use of Patient-Specific Implants in Oral and Maxillofacial Surgery. Oral Maxillofac. Surg. Clin. N. Am. 2019, 31, 593–600. [Google Scholar] [CrossRef]
- Pascal, E.; Majoufre, C.; Bondaz, M.; Courtemanche, A.; Berger, M.; Bouletreau, P. Current status of surgical planning and transfer methods in orthognathic surgery. J. Stomatol. Oral Maxillofac. Surg. 2018, 119, 245–248. [Google Scholar] [CrossRef]
- Van den Bempt, M.; Liebregts, J.; Maal, T.; Bergé, S.; Xi, T. Toward a higher accuracy in orthognathic surgery by using intraoperative computer navigation, 3D surgical guides, and/or customized osteosynthesis plates: A systematic review. J. Cranio-Maxillofac. Surg. 2018, 46, 2108–2119. [Google Scholar] [CrossRef]
- Zavattero, E.; Gerbino, G.; Borbon, C.; Ramieri, G. Conformity of the Virtual Surgical Plan to the Actual Result Comparing Five Craniofacial Procedure Types. Plast. Reconstr. Surg. 2022, 150, 484e–485e. [Google Scholar] [CrossRef] [PubMed]
- Cevidanes, L.H.; Styner, M.A.; Proffit, W.R. Image analysis and superimposition of 3-dimensional cone-beam computed tomography models. Am. J. Orthod. Dentofac. Orthop. 2006, 129, 611–618. [Google Scholar] [CrossRef] [Green Version]
- Maes, F.; Collignon, A.; Vandermeulen, D.; Marchal, G.; Suetens, P. Multimodality image registration by maximization of mutual information. IEEE Trans. Med. Imaging 1997, 16, 187–198. [Google Scholar] [CrossRef] [Green Version]
- Andriola, F.O.; Junior, O.L.H.; Guijarro-Martínez, R.; Hernández-Alfaro, F.; de Oliveira, R.B.; Pagnoncelli, R.M.; Swennen, G.R. Computed tomography imaging superimposition protocols to assess outcomes in orthognathic surgery: A systematic review with comprehensive recommendations. Dentomaxillofac. Radiol. 2022, 51, 20210340. [Google Scholar] [CrossRef]
- Apostolakis, D.; Michelinakis, G.; Kamposiora, P.; Papavasiliou, G. The current state of computer assisted orthognathic surgery: A narrative review. J. Dent. 2022, 119, 104052. [Google Scholar] [CrossRef]
- Zoabi, A.; Redenski, I.; Oren, D.; Kasem, A.; Zigron, A.; Daoud, S.; Moskovich, L.; Kablan, F.; Srouji, S. 3D Printing and Virtual Surgical Planning in Oral and Maxillofacial Surgery. J. Clin. Med. 2022, 11, 2385. [Google Scholar] [CrossRef]
- Hsu, S.S.; Gateno, J.; Bell, R.B.; Hirsch, D.L.; Markiewicz, M.R.; Teichgraeber, J.F.; Zhou, X.; Xia, J.J. Accuracy of a computer-aided surgical simulation protocol for orthognathic surgery: A prospective multicenter study. J. Oral Maxillofac. Surg. 2013, 71, 128–142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, B.; Shen, S.; Jiang, W.; Li, J.; Jiang, T.; Xia, J.J.; Shen, S.G.; Wang, X. A new approach of splint-less orthognathic surgery using a personalized orthognathic surgical guide system: A preliminary study. Int. J. Oral Maxillofac. Surg. 2017, 46, 1298–1305. [Google Scholar] [CrossRef] [Green Version]
- Shaheen, E.; Shujaat, S.; Saeed, T.; Jacobs, R.; Politis, C. Three-dimensional planning accuracy and follow-up protocol in orthognathic surgery: A validation study. Int. J. Oral Maxillofac. Surg. 2019, 48, 71–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tondin, G.M.; Leal, M.; Costa, S.T.; Grillo, R.; Jodas, C.R.P.; Teixeira, R.G. Evaluation of the accuracy of virtual planning in bimaxillary orthognathic surgery: A systematic review. Br. J. Oral Maxillofac. Surg. 2022, 60, 412–421. [Google Scholar] [CrossRef]
- Tonin, R.H.; Filho, L.I.; Yamashita, A.L.; Ferraz, F.W.D.S.; Tolentino, E.D.S.; Previdelli, I.T.D.S.; Brum, B.; Iwaki, L.C.V. Accuracy of 3D virtual surgical planning for maxillary positioning and orientation in orthognathic surgery. Orthod. Craniofac. Res. 2020, 23, 229–236. [Google Scholar] [CrossRef]
- Tran, N.H.; Tantidhnazet, S.; Raocharernporn, S.; Kiattavornchareon, S.; Pairuchvej, V.; Wongsirichat, N. Accuracy of Three-Dimensional Planning in Surgery-First Orthognathic Surgery: Planning Versus Outcome. J. Clin. Med. Res. 2018, 10, 429–436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, N.; Liu, S.; Hu, Z.; Hu, J.; Zhu, S.; Li, Y. Accuracy of virtual surgical planning in two-jaw orthognathic surgery: Comparison of planned and actual results. Oral Surgery Oral Med. Oral Pathol. Oral Radiol. 2016, 122, 143–151. [Google Scholar] [CrossRef]
- Alkhayer, A.; Piffko, J.; Lippold, C.; Segatto, E. Accuracy of virtual planning in orthognathic surgery: A systematic review. Head Face Med. 2020, 16, 34. [Google Scholar] [CrossRef] [PubMed]
- Gaber, R.M.; Shaheen, E.; Falter, B.; Araya, S.; Politis, C.; Swennen, G.R.; Jacobs, R. A Systematic Review to Uncover a Universal Protocol for Accuracy Assessment of 3-Dimensional Virtually Planned Orthognathic Surgery. J. Oral Maxillofac. Surg. 2017, 75, 2430–2440. [Google Scholar] [CrossRef]
- Baan, F.; Sabelis, J.F.; Schreurs, R.; van de Steeg, G.; Xi, T.; van Riet, T.C.T.; Becking, A.G.; Maal, T.J.J. Validation of the OrthoGnathicAnalyser 2.0-3D accuracy assessment tool for bimaxillary surgery and genioplasty. PLoS ONE 2021, 16, e0246196. [Google Scholar] [CrossRef] [PubMed]
- da Senior, O.C.; Vaes, L.; Mulier, D.; Jacobs, R.; Politis, C.; Shaheen, E. Three dimensional assessment of segmented Le Fort I osteotomy planning and follow-up: A validation study. J. Dent. 2021, 111, 103707. [Google Scholar] [CrossRef] [PubMed]
- Holte, M.B.; Diaconu, A.; Ingerslev, J.; Thorn, J.J.; Pinholt, E.M. Virtual Analysis of Segmental Bimaxillary Surgery: A Validation Study. J. Oral Maxillofac. Surg. 2021, 79, 2320–2333. [Google Scholar] [CrossRef]
- Holte, M.B.; Diaconu, A.; Ingerslev, J.; Thorn, J.J.; Pinholt, E.M. Virtual surgical analysis: Long-term cone beam computed tomography stability assessment of segmental bimaxillary surgery. Int. J. Oral Maxillofac. Surg. 2022, 51, 1188–1196. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Luo, D.; Wan, X.; Liu, J.; Tong, T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat. Methods Med. Res. 2018, 27, 1785–1805. [Google Scholar] [CrossRef] [Green Version]
- Badiali, G.; Bevini, M.; Lunari, O.; Lovero, E.; Ruggiero, F.; Bolognesi, F.; Feraboli, L.; Bianchi, A.; Marchetti, C. PSI-Guided Mandible-First Orthognathic Surgery: Maxillo-Mandibular Position Accuracy and Vertical Dimension Adjustability. J. Pers. Med. 2021, 11, 1237. [Google Scholar] [CrossRef] [PubMed]
- Badiali, G.; Bevini, M.; Ruggiero, F.; Cercenelli, L.; Lovero, E.; De Simone, E.; Marchetti, C. Validation of a patient-specific system for mandible-first bimaxillary surgery: Ramus and implant positioning precision assessment and guide design comparison. Sci. Rep. 2020, 10, 13317. [Google Scholar] [CrossRef]
- Hanafy, M.; Akoush, Y.; Abou-ElFetouh, A.; Mounir, R.M. Precision of orthognathic digital plan transfer using patient-specific cutting guides and osteosynthesis versus mixed analogue-digitally planned surgery: A randomized controlled clinical trial. Int. J. Oral Maxillofac. Surg. 2020, 49, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Heufelder, M.; Wilde, F.; Pietzka, S.; Mascha, F.; Winter, K.; Schramm, A.; Rana, M. Clinical accuracy of waferless maxillary positioning using customized surgical guides and patient specific osteosynthesis in bimaxillary orthognathic surgery. J. Cranio-Maxillofac. Surg. 2017, 45, 1578–1585. [Google Scholar] [CrossRef]
- Karanxha, L.; Rossi, D.; Hamanaka, R.; Giannì, A.B.; Baj, A.; Moon, W.; Del Fabbro, M.; Romano, M. Accuracy of splint vs splintless technique for virtually planned orthognathic surgery: A voxel-based three-dimensional analysis. J. Cranio-Maxillofac. Surg. 2021, 49, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kraeima, J.; Schepers, R.H.; Spijkervet, F.K.L.; Maal, T.J.J.; Baan, F.; Witjes, M.J.H.; Jansma, J. Splintless surgery using patient-specific osteosynthesis in Le Fort I osteotomies: A randomized controlled multi-centre trial. Int. J. Oral Maxillofac. Surg. 2020, 49, 454–460. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Wang, S.; Wei, H.; Zeng, F.; Wang, X. The use of patient-specific implants in genioplasty and its clinical accuracy: A preliminary study. Int. J. Oral Maxillofac. Surg. 2020, 49, 461–465. [Google Scholar] [CrossRef]
- Li, B.; Wei, H.; Jiang, T.; Qian, Y.; Zhang, T.; Yu, H.; Zhang, L.; Wang, X. Randomized Clinical Trial of the Accuracy of Patient-Specific Implants versus CAD/CAM Splints in Orthognathic Surgery. Plast. Reconstr. Surg. 2021, 148, 1101–1110. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Jauregui, E.; Baranda-Manterola, E.; Ranz-Colio, A.; de Vicente, A.B.; Acero-Sanz, J. Custom made cutting guides and osteosynthesis plates versus CAD/CAM occlusal splints in positioning and fixation of the maxilla in orthognathic surgery: A prospective randomized study. J. Cranio Maxillofac. Surg. 2022, 50, 609–614. [Google Scholar] [CrossRef] [PubMed]
- van der Wel, H.; Kraeima, J.; Spijkervet, F.K.L.; Schepers, R.H.; Jansma, J. Postoperative skeletal stability at the one-year follow-up after splintless Le Fort I osteotomy using patient-specific osteosynthesis versus conventional osteosynthesis: A randomized controlled trial. Int. J. Oral Maxillofac. Surg. 2022. [Google Scholar] [CrossRef]
- Ho, J.P.T.F.; Schreurs, R.; Baan, F.; de Lange, J.; Becking, A.G. Splintless orthognathic surgery in edentulous patients—A pilot study. Int. J. Oral Maxillofac. Surg. 2020, 49, 587–594. [Google Scholar] [CrossRef]
- Jones, J.P.; Amarista, F.J.; Jeske, N.A.; Szalay, D.; Ellis, E. Comparison of the Accuracy of Maxillary Positioning with Interim Splints Versus Patient-Specific Guides and Plates in Executing a Virtual Bimaxillary Surgical Plan. J. Oral Maxillofac. Surg. 2022, 80, 827–837. [Google Scholar] [CrossRef]
- Abel, A.R.; Ho, K.; Neugarten, J.M. What Is the Accuracy of Bimaxillary Orthognathic Surgery Using Occlusally and Patient-Specific Fixation in Both Jaws? A Cohort Study and Discussion of Surgical Techniques. J. Oral Maxillofac. Surg. 2022, 80, 1912–1926. [Google Scholar] [CrossRef]
- Greenberg, S.; Buchbinder, D.; Turner, M.D.; Dhillon, P.; Afshar, A.A. Three-Dimensional Repositioning of the Maxilla in Orthognathic Surgery Using Patient-Specific Titanium Plates: A Case Series. J. Oral Maxillofac. Surg. 2021, 79, 902–913. [Google Scholar] [CrossRef] [PubMed]
- Liu, K.; Sun, H.; Zhang, L.; Li, B.; Chakraborty, S.; Wang, X. Do patient-specific cutting guides and plates improve the accuracy of maxillary repositioning in hemifacial microsomia? Br. J. Oral Maxillofac. Surg. 2020, 58, 590–596. [Google Scholar] [CrossRef]
- Rios, O.; Lerhe, B.; Chamorey, E.; Savoldelli, C. Accuracy of Segmented Le Fort I Osteotomy with Virtual Planning in Orthognathic Surgery Using Patient-Specific Implants: A Case Series. J. Clin. Med. 2022, 11, 5495. [Google Scholar] [CrossRef] [PubMed]
- Ruckschloss, T.; Ristow, O.; Muller, M.; Kuhle, R.; Zingler, S.; Engel, M.; Hoffmann, J.; Freudlsperger, C. Accuracy of patient-specific implants and additive-manufactured surgical splints in orthognathic surgery—A three-dimensional retrospective study. J. Cranio-Maxillofac. Surg. 2019, 47, 847–853. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.; Goonewardene, M.S.; Allan, B.P.; Mian, A.S.; Rea, A. Accuracy of maxillary repositioning surgery using CAD/CAM customized surgical guides and fixation plates. Int. J. Oral Maxillofac. Surg. 2021, 50, 494–500. [Google Scholar] [CrossRef]
- Harding, J.; Hartsfield, J.K., Jr.; Mian, A.S.; Allan, B.P.; Naoum, S.; Lee, R.J.H.; Goonewardene, M.S. Accuracy of mandibular proximal segment position using virtual surgical planning and custom osteosynthesis plates. Int. J. Oral Maxillofac. Surg. 2022, 51, 219–225. [Google Scholar] [CrossRef]
- Ruckschloss, T.; Ristow, O.; Kuhle, R.; Weichel, F.; Roser, C.; Aurin, K.; Engel, M.; Hoffmann, J.; Freudlsperger, C. Accuracy of laser-melted patient-specific implants in genioplasty—A three-dimensional retrospective study. J. Cranio-Maxillofac. Surg. 2020, 48, 653–660. [Google Scholar] [CrossRef]
- Besl, P.J.; McKay, N.D. A method for registration of 3-D shapes. IEEE Trans. Pattern Anal. 1992, 14, 239–256. [Google Scholar] [CrossRef] [Green Version]
- Cassoni, A.; Manganiello, L.; Barbera, G.; Priore, P.; Fadda, M.T.; Pucci, R.; Valentini, V. Three-Dimensional Comparison of the Maxillary Surfaces through ICP-Type Algorithm: Accuracy Evaluation of CAD/CAM Technologies in Orthognathic Surgery. Int. J. Environ. Res. Public Health 2022, 19, 11834. [Google Scholar] [CrossRef] [PubMed]
- Marliere, D.A.A.; Demetrio, M.S.; Verner, F.S.; Asprino, L.; Netto, H.D.M.C. Feasibility of iterative closest point algorithm for accuracy between virtual surgical planning and orthognathic surgery outcomes. J. Cranio-Maxillofac. Surg. 2019, 47, 1031–1040. [Google Scholar] [CrossRef] [PubMed]
- Han, G.; Li, J.; Wang, S.; Wang, L.; Zhou, Y.; Liu, Y. A comparison of voxel- and surface-based cone-beam computed tomography mandibular superimposition in adult orthodontic patients. J. Int. Med. Res. 2021, 49, 300060520982708. [Google Scholar] [CrossRef] [PubMed]
- Ghoneima, A.; Cho, H.; Farouk, K.; Kula, K. Accuracy and reliability of landmark-based, surface-based and voxel-based 3D cone-beam computed tomography superimposition methods. Orthod. Craniofac. Res. 2017, 20, 227–236. [Google Scholar] [CrossRef]
- Almukhtar, A.; Ju, X.; Khambay, B.; McDonald, J.; Ayoub, A. Comparison of the accuracy of voxel based registration and surface based registration for 3D assessment of surgical change following orthognathic surgery. PLoS ONE 2014, 9, e93402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holte, M.B.; Saederup, H.; Pinholt, E.M. Comparison of surface- and voxel-based registration on the mandibular ramus for long-term three-dimensional assessment of condylar remodelling following orthognathic surgery. Dentomaxillofac. Radiol. 2022, 51, 20210499. [Google Scholar] [CrossRef]
- Verhelst, P.J.; Shaheen, E.; Vasconcelos, K.D.F.; Van der Cruyssen, F.; Shujaat, S.; Coudyzer, W.; Salmon, B.; Swennen, G.; Politis, C.; Jacobs, R. Validation of a 3D CBCT-based protocol for the follow-up of mandibular condyle remodeling. Dentomaxillofac. Radiol. 2020, 49, 20190364. [Google Scholar] [CrossRef]














| Author, Year | Study Design | N | Mean Age (Range) | Treatment | PSI Component |
|---|---|---|---|---|---|
| Abel et al. (2022) | Cohort (retrospective) | 49 | F: 24 M: 25.6 | Bimaxillary osteotomy | Maxilla (single or split) and mandible |
| Badiali et al. (2021) | Cohort (prospective) | 22 * | 26 (18–43) | Bimaxillary osteotomy | Mandible |
| Badiali et al. (2020) | Cohort (prospective) | 22 | 26 (18–43) | Bimaxillary osteotomy | Mandible |
| Greenberg et al. (2021) | Series (retrospective) | 10 | 25.7 | Bimaxillary osteotomy | Maxilla (single or segmental) |
| Hanafy et al. (2020) | RCT (prospective) | 18 | 21.2 (19–24) | Bimaxillary osteotomy | Maxilla (single) |
| Harding et al. (2022) | Cohort (retrospective) | 55 | PSI: 28.0 (16–52) Splint: 25.9 (16–47) | Bimaxillary osteotomy | Mandible |
| Heufelder et al. (2017) | Series (prospective) | 22 | NS (17–59) | Bimaxillary osteotomy | Maxilla (single) |
| Ho et al. (2020) | Cohort (retrospective) | 4 | 55 (48–62) | Bimaxillary osteotomy bilateral sagittal split osteotomy | Maxilla (single) |
| Jones et al. (2022) | Cohort (retrospective) | 82 | 23.2 (14–54) | Bimaxillary osteotomy | Maxilla (single or segmental) |
| Karanxha et al. (2021) | Cohort (prospective) | 16 | 26.4 | Bimaxillary osteotomy | Maxilla (single or segmental) and mandible |
| Kraeima et al. (2020) | RCMCT (prospective) | 58 | 27.6 (19–60) | Le Fort I osteotomy | Maxilla (single) |
| Li et al. (2017) | Series (prospective) | 10 | NS (18–27) | Bimaxillary osteotomy | Maxilla (single) and mandible |
| Li et al. (2020) | Cohort (prospective) | 15 | NS (18–30) | Genioplasty, with or without simultaneous Le Fort I and/or bilateral sagittal split osteotomy | Chin |
| Li et al. (2021) | RCT (prospective) | 58 | PSI: 23.8 (19–32) Splint: 23.6 (19–33) | Bimaxillary osteotomy | Maxilla (single) |
| Liu et al. (2020) | Cohort (retrospective) | 18 | NS (17–30) | Bimaxillary osteotomy | Maxilla (single) |
| Rios et al. (2022) | Series (retrospective) | 22 | 27.4 | Bimaxillary osteotomy | Maxilla (segmental) |
| Ruckschloss et al. (2020) | Cohort (retrospective) | 29 | 24.2 | Bimaxillary osteotomy | Chin |
| Ruckschloss et al. (2019) | Cohort (retrospective) | 18 | F: 23.3 M: 19.8 | Le Fort I osteotomy (single) or bimaxillary osteotomy | Maxilla (single) |
| Sanchez-Jauregui et al. (2020) | Cohort (prospective) | 30 | NS | Le Fort I osteotomy (single or split) | Maxilla (single or segmental) |
| van der Wel et al. (2022) | RCMCT (prospective) | 27 † | PSI: 28.6 (9.7) Splint: 26.8 (6.9) | Le Fort I osteotomy (single) with or without mandibular osteotomy | Maxilla (single) |
| Wong et al. (2021) | Series (retrospective) | 30 | F: 25.5 M: 29.2 | Le Fort I osteotomy (single) with or without mandibular osteotomy and genioplasty | Maxilla (single) |
| Author, Year | PSI Component (s) | Translation | Rotation |
|---|---|---|---|
| Abel et al. (2022) | Maxilla and mandible | A-point: Lateral: 0.37 (0.45), AP: 0.57 (0.57), vertical: 0.45 (0.42) B-point: Lateral: 0.62 (0.54), AP: 1.15 (1.28), vertical: 1.14 (0.83) Pogonion: Lateral: 0.85 (0.73), AP: 1.29 (1.50), vertical: 1.24 (0.85) | |
| Badiali et al. (2021) | Mandible | Mandible: Lateral: 1.14 (1.00), AP: 1.49 (1.59), vertical: −1.05 (1.23) | Mandible: Pitch: 1.53 (1.34), roll: 0.96 (0.85), yaw: 1.13 (0.99) |
| Badiali et al. (2020) | Mandible | Rami: Lateral: 0.49 (1.05), AP: 0.32 (0.92), vertical: −0.04 (0.94) Plates: Lateral: 0.20 (0.64), AP: −0.68 (1.18), vertical: 0.26 (0.79) | Rami: Pitch: 0.52 (2.39), roll: 0.90 (2.15), yaw: −1.91 (2.70) Plates: Pitch: −1.93 (3.89), roll: 0.13 (3.04), yaw: 0.20 (1.41) |
| Greenberg et al. (2021) | Maxilla | UI: Lateral: 0.66 (0.51), AP: 0.80 (0.56), vertical: 0.48 (0.27) | |
| Hanafy et al. (2020) | Maxilla | PSI UI: Lateral: 0.07 (0.02), AP: 0.17 (0.04), vertical: 0.26 (0.08) Wafer UI: Lateral: 0.71 (0.21), AP: 1.31 (0.51), vertical: 1.45 (0.58) | |
| Harding et al. (2022) | Mandible | R ramus PSI: Lateral: 1.18, AP: 0.62, vertical: 0.58 R ramus control: Lateral: 0.83, AP: 0.78, vertical: 0.70 L ramus PSI: Lateral: 1.20, AP: 0.45, vertical: 0.44 L ramus control: Lateral: 0.83, AP: 0.68, vertical: 0.56 | R ramus PSI: Pitch: 1.00, roll: 1.43, yaw: 1.53 R ramus control: Pitch: 1.50, roll: 2.42, yaw: 2.98 L ramus PSI: Pitch: 1.32, roll: 1.62, yaw: 1.59 L ramus control: Pitch: 1.41, roll: 1.39, yaw: 2.45 |
| Heufelder et al. (2017) | Maxilla | UI: Lateral: 0.2, AP: 0.35, vertical: 0.85 | |
| Ho et al. (2020) | Maxilla | Maxilla: Lateral: 0.3, AP: 1.1, vertical: 0.5 | Maxilla: Pitch: 1.9, roll: 0.4, yaw: 0.1 |
| Jones et al. (2022) | Maxilla | PSI UI: Lateral: 0.41, AP: 0.94, vertical: 0.54 Splint UI: Lateral: 1.01, AP: 0.93, vertical: 1.23 | |
| Karanxha et al. (2021) | Maxilla and mandible | PSI UI: Lateral: 0.32 (0.27), AP: 1.43 (0.81), vertical: 0.85 (0.59) Splint UI: Lateral: 0.45 (0.43), AP: 1.53 (0.63), vertical: 1.73 (0.90) PSI LI: Lateral: 0.94 (0.74), AP: 1.99 (1.84), vertical: 1.99 (1.39) Splint LI: Lateral: 1.78 (1.11), AP: 1.34 (1.2), vertical: 3.68 (4.62) | PSI Maxilla: Pitch: 2.87 (1.52), roll: 0.49 (0.51), yaw: 0.17 (0.05) Splint maxilla: Pitch: 2.30 (1.31), roll: 1.62 (0.78), yaw: 0.63 (0.45) PSI mandible: Pitch: 2.85 (1.68), roll: 0.84 (0.82), yaw: 1.68 (1.00) Splint mandible: Pitch: 2.48 (2.30), roll: 1.54 (1.85), yaw: 1.62 (1.36) |
| Kraeima et al. (2020) | Maxilla | PSI UI: Lateral: 0.46, AP: 1.05, vertical: 0.87 Splint UI: Lateral: 1.07, AP: 1.74, vertical: 0.98 | PSI Maxilla: Pitch: 2.33, roll: 0.53, yaw: 0.21 Splint maxilla: Pitch: 2.17, roll: 0.60, yaw: 0.44 |
| Li et al. (2017) | Maxilla and mandible | UI: Lateral: −0.18 (0.35), AP: −0.54 (0.53), vertical: 0.33 (0.53) LI: Lateral: −0.33 (0.50), AP: −0.67 (0.92), vertical: 0.38 (0.72) Left ramus: Lateral: −0.10 (1.03), AP: 0.23 (0.82), vertical: −0.10 (0.79) Right ramus: Lateral: −0.18 (0.70), AP: 0.05 (0.54), vertical: −0.28 (0.94) | UI: Pitch: 0.11 (0.69), roll: 0.02 (0.60), yaw: −0.83 (1.83) LI: Pitch: 0.45 (1.67), roll: −0.07 (0.95), yaw: 0.26 (0.96) Left ramus: Pitch: 1.39 (2.12), roll: 0.01 (1.14), yaw: 0.49 (2.06) Right ramus: Pitch: −1.66 (1.85), roll: −0.59 (1.73), yaw: 0.26 (2.20) |
| Li et al. (2020) | Chin | Chin centroid: Lateral: 0.06 (0.71), AP: −0.49 (0.46), vertical: 0.39 (0.55) | Chin centroid: Pitch: 0.68 (1.68), roll: −0.10 (1.67), yaw: −0.17 (2.08) |
| Li et al. (2021) | Maxilla | PSI maxilla centroid: Lateral: 0.37 (0.40), AP: 1.02 (0.66), vertical: 0.61 (0.44) Splint maxilla centroid: Lateral: 1.23 (0.93), AP: 1.12 (0.82), vertical: 0.96 (0.74) | PSI maxilla: Pitch: 1.85 (1.42), roll: 1.63 (0.52), yaw: 0.63 (0.44) Splint maxilla: Pitch: 1.72 (1.56), roll: 1.25 (1.18), yaw: 0.88 (0.71) |
| Liu et al. (2020) | Maxilla | PSI: Lateral: 0.30 (0.18), AP: 0.50 (0.18), vertical: 0.33 (0.18) Splint: Lateral: 1.05 (0.75), AP: 1.37 (0.84), vertical: 1.32 (1.40) | PSI: Pitch: 0.40 (0.31), roll: 0.28 (0.21), yaw: 0.82 (0.60) Splint: Pitch: 3.56 (3.26), roll: 1.53 (1.05), yaw: 8.84 (7.73) |
| Rios et al. (2022) | Maxilla | UI: Lateral: 0.54 (0.44), AP: 0.74 (0.51), vertical: 0.35 (0.24) | |
| Ruckschloss et al. (2020) | Chin | Chin: Lateral: 0.25 (0.28), AP: 0.70 (0.64), vertical: 0.45 (0.38) | Chin: Pitch: 1.76 (0.98), roll: 0.89 (0.74), yaw: 0.83 (0.57) |
| Ruckschloss et al. (2019) | Maxilla | PSI: Lateral: 0.51 (0.48), AP: 0.39 (0.26), vertical: 0.37 (0.40) Splint: Lateral: 1.11 (1.32), AP: 1.42 (0.87), vertical: 0.62 (0.47) | PSI: Pitch: 1.04 (0.97), roll: 0.43 (0.49), yaw: 0.57 (0.26) Splint: Pitch: 1.84 (1.48), roll: 0.46 (0.64), yaw: 1.31 (1.11) |
| Sanchez-Jauregui et al. (2020) | Maxilla | PSI: Lateral: 0.2, AP: 0.8, vertical: 0.4 Splint: Lateral: 0.2, AP: 1.7, vertical: 1.8 | |
| van der Wel et al. (2022) | Maxilla | Accuracy: PSI UI: Lateral: 0.5, AP: 3.8, vertical: 2.1 Splint UI: Lateral: 1.2, AP: 2.8, vertical: 1.5 Stability: PSI UI: Lateral: 0.3, AP: 0.5, vertical: 0.3 Splint UI: Lateral: 0.2, AP: 0.2, vertical: 0.3 | Accuracy: PSI: Pitch: 2.6, roll: 0.7, yaw: 0.2 Splint: Pitch: 1.8, roll: 0.9, yaw: 0.6 Stability: PSI: Pitch: 0.1, roll: 0.2, yaw: 0.0 Splint: Pitch: 0.0, roll: 0.2, yaw: 0.0 |
| Wong et al. (2021) | Maxilla | UI: Lateral: −0.14 (0.22), AP: −0.09 (0.38), vertical: −0.26 (0.32) | UI: Pitch: −0.28 (1.03), roll: 0.09 (0.47), yaw: −0.21 (0.45) |
| Record | MINORS Score |
|---|---|
| Karanxha et al. (2021) | 18 |
| Harding et al. (2022) | 17 |
| Jones et al. (2022) | 16 |
| Liu et al. (2020) | 16 |
| Ruckschloss et al. (2019) | 16 |
| Heufelder et al. (2017) | 12 |
| Li et al. (2020) | 12 |
| Abel et al. (2022) | 10 |
| Ho et al. (2020) | 10 |
| Li et al. (2017) | 10 |
| Rios et al. (2022) | 10 |
| Wong et al. (2021) | 10 |
| Badiali et al. (2021) | 9 |
| Badiali et al. (2020) | 9 |
| Greenberg et al. (2021) | 9 |
| Kim et al. (2019) | 9 |
| Ruckschloss et al. (2020) | 8 |
| Record | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|
| Hanafy et al. (2020) | + | + | + | + | + | + |
| Li et al. (2021) | + | + | + | + | + | + |
| Sanchez-Jauregui et al. (2020) | + | ? | ? | ? | + | + |
| Kraeima et al. (2020) | + | ? | ? | ? | + | + |
| van der Wel et al. (2022) | + | ? | ? | ? | - * | + |
| Summarized Results | Lateral | Antero-Posterior | Vertical | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | p * | Mean | SD | p * | Mean | SD | p * | |
| Absolute values | 0.30 | 0.18 | <0.0001 | 0.50 | 0.13 | <0.0001 | 0.42 | 0.14 | <0.0001 |
| Hanafy et al. | 0.07 | 0.02 | <0.0001 | 0.17 | 0.04 | <0.0001 | 0.26 | 0.08 | <0.0001 |
| Signed values | −0.17 | 0.41 | <0.0001 | −0.24 | 0.31 | <0.0001 | −0.10 | 0.28 | <0.0001 |
| Overall | 0.07 | 0.02 | <0.0001 | 0.30 | 0.08 | <0.0001 | 0.28 | 0.07 | <0.0001 |
| Summarized Results | Pitch | Roll | Yaw | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | p * | Mean | SD | p * | Mean | SD | p * | |
| Absolute values | 0.65 | 0.35 | <0.0001 | 0.36 | 0.17 | <0.0001 | 0.26 | 0.12 | <0.0001 |
| Signed values | −0.01 | 0.57 | <0.0001 | 0.06 | 0.37 | <0.0001 | −0.24 | 0.44 | <0.0001 |
| Overall | 0.45 | 0.25 | <0.0001 | 0.15 | 0.15 | <0.0001 | 0.10 | 0.10 | <0.0001 |
| Dimension | Mean Difference (mm) | p-Value * |
|---|---|---|
| Lateral | Absolute values only: −0.852 | Absolute values only: <0.0001 |
| Overall: −0.852 | Overall: <0.0001 | |
| Antero-posterior | Absolute values only: −0.677 | Absolute values only: <0.0001 |
| Overall: −1.127 | Overall: <0.0001 | |
| Vertical | Absolute values only: −0.393 | Absolute values only: <0.0001 |
| Overall: −0.811 | Overall: <0.0001 |
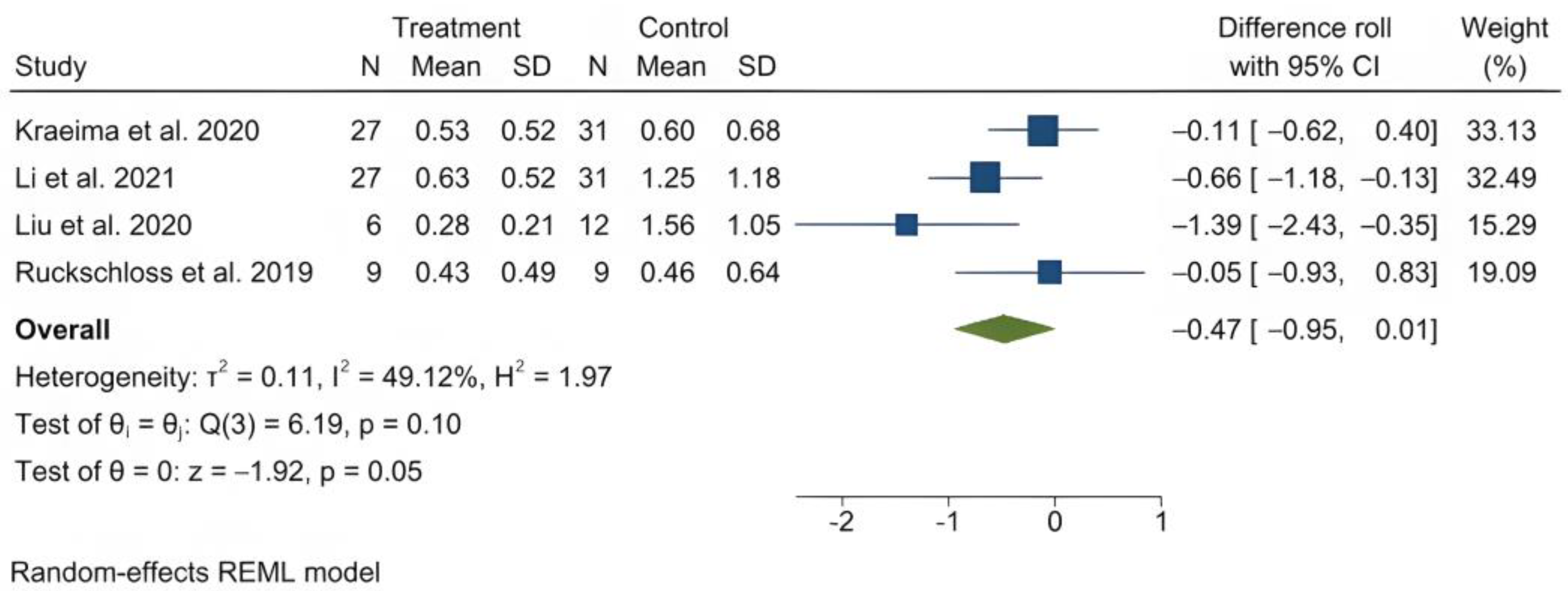
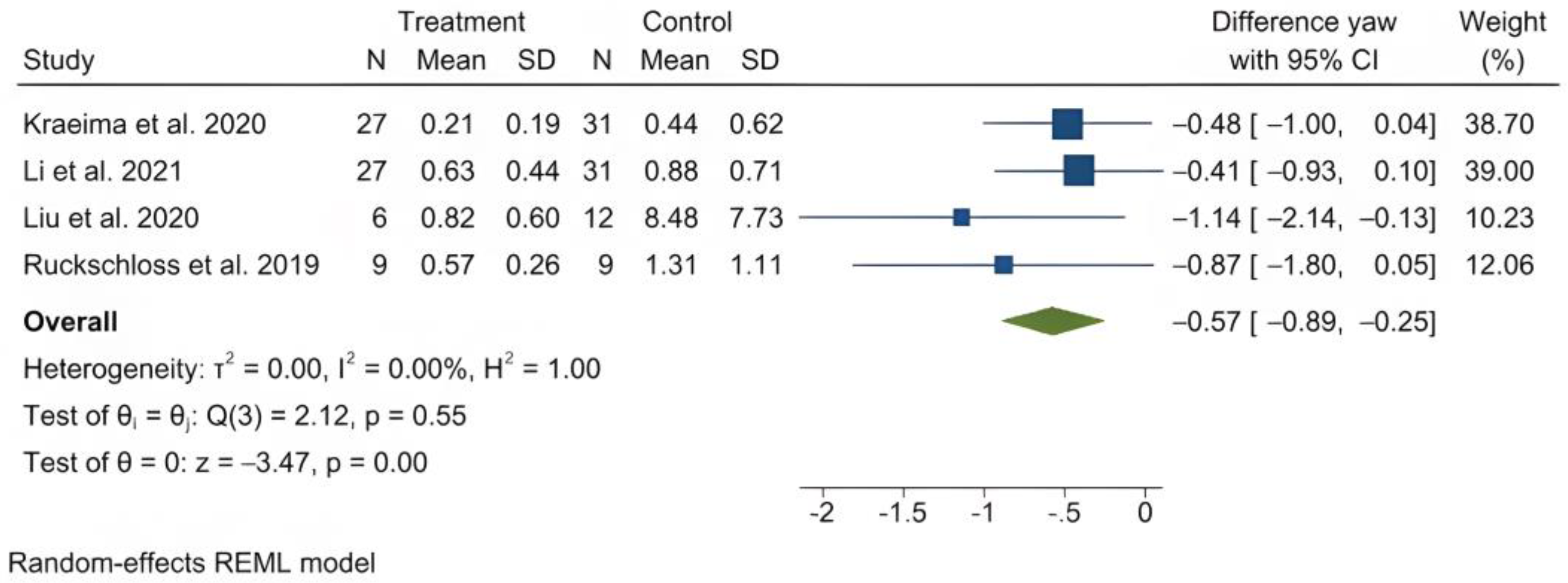
| Dimension | Mean Difference (Degrees) | p-Value * |
|---|---|---|
| Pitch | −2.352 | <0.0001 |
| Roll | −0.472 | <0.0001 |
| Yaw | −0.568 | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Diaconu, A.; Holte, M.B.; Berg-Beckhoff, G.; Pinholt, E.M. Three-Dimensional Accuracy and Stability of Personalized Implants in Orthognathic Surgery: A Systematic Review and a Meta-Analysis. J. Pers. Med. 2023, 13, 125. https://doi.org/10.3390/jpm13010125
Diaconu A, Holte MB, Berg-Beckhoff G, Pinholt EM. Three-Dimensional Accuracy and Stability of Personalized Implants in Orthognathic Surgery: A Systematic Review and a Meta-Analysis. Journal of Personalized Medicine. 2023; 13(1):125. https://doi.org/10.3390/jpm13010125
Chicago/Turabian StyleDiaconu, Alexandru, Michael Boelstoft Holte, Gabriele Berg-Beckhoff, and Else Marie Pinholt. 2023. "Three-Dimensional Accuracy and Stability of Personalized Implants in Orthognathic Surgery: A Systematic Review and a Meta-Analysis" Journal of Personalized Medicine 13, no. 1: 125. https://doi.org/10.3390/jpm13010125