
Preoperative Immunocite-Derived Ratios Predict Surgical Complications Better when Artificial Neural Networks Are Used for Analysis—A Pilot Comparative Study
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Design
2.2. Perioperative Management
2.3. Data Extraction
2.4. Statistical Analysis
2.5. Artificial Neural Network
3. Results
3.1. Patient Characteristics
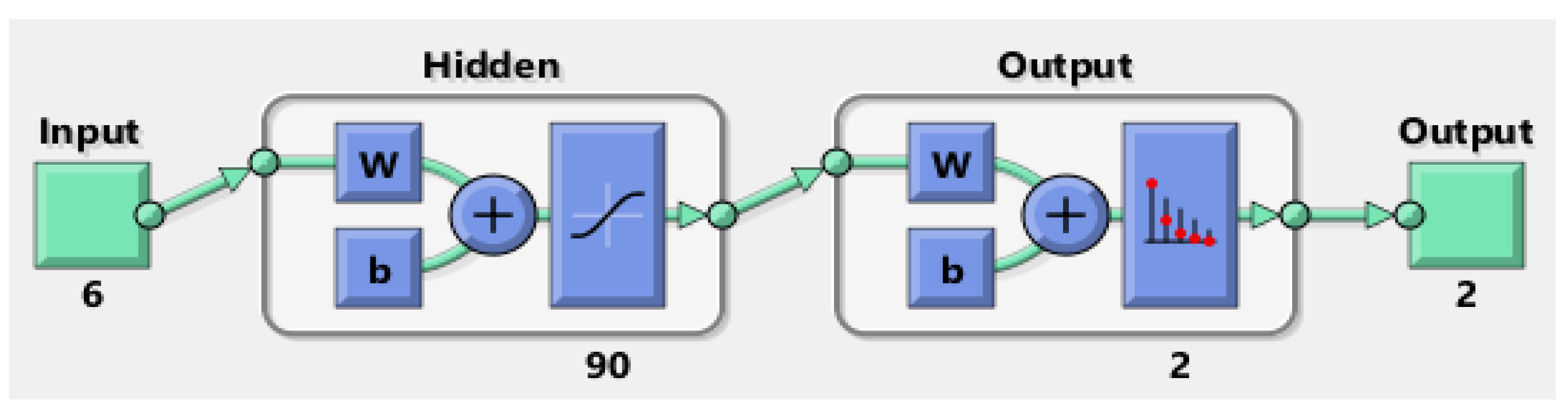
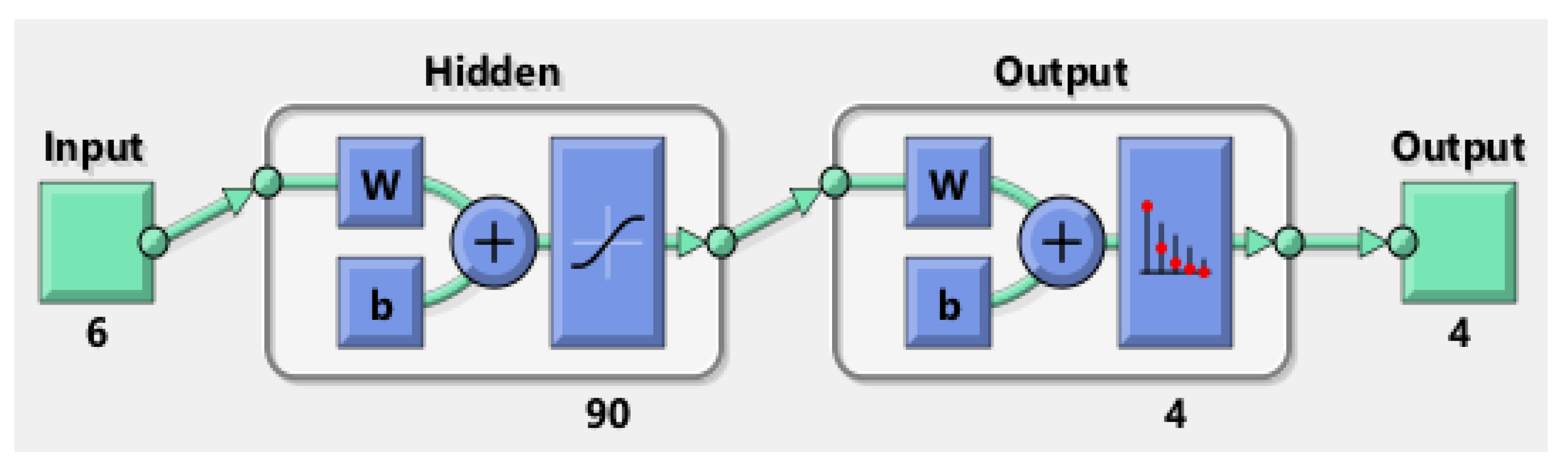
3.2. MLP Neural Networks
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mantovani, A.; Allavena, P.; Sica, A.; Balkwill, F. Cancer-related inflammation. Nature 2008, 454, 436–444. [Google Scholar] [CrossRef]
- Terzić, J.; Grivennikov, S.; Karin, E.; Karin, M. Inflammation and Colon Cancer. Gastroenterology 2010, 138, 2101–2114.e5. [Google Scholar] [CrossRef]
- Rumba, R.; Cipkina, S.; Cukure, F.; Vanags, A. Systemic and local inflammation in colorectal cancer. Acta Med. Litu. 2018, 25, 185–196. [Google Scholar] [CrossRef] [Green Version]
- Holmgren, K.; Jonsson, P.; Lundin, C.; Matthiessen, P.; Rutegård, J.; Sund, M.; Rutegård, M. Preoperative biomarkers related to inflammation may identify high-risk anastomoses in colorectal cancer surgery: Explorative study. BJS Open 2022, 6, zrac072. [Google Scholar] [CrossRef]
- Diakos, C.I.; Charles, K.A.; McMillan, D.C.; Clarke, S.J. Cancer-related inflammation and treatment effectiveness. Lancet Oncol. 2014, 15, e493–e503. [Google Scholar] [CrossRef] [PubMed]
- Josse, J.M.; Cleghorn, M.C.; Ramji, K.M.; Jiang, H.; Elnahas, A.; Jackson, T.D.; Okrainec, A.; Quereshy, F.A. The neutrophil/lymphocyte ratio predicts major perioperative complications in patients undergoing colorectal surgery. Color. Dis. 2016, 18, O236–O242. [Google Scholar] [CrossRef]
- Cook, E.J.; Walsh, S.; Farooq, N.; Alberts, J.C.; Justin, T.A.; Keeling, N.J. Post-operative neutrophil–lymphocyte ratio predicts complications following colorectal surgery. Int. J. Surg. 2007, 5, 27–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, J.C.Y.; Diakos, C.I.; Chan, D.L.H.; Engel, A.; Pavlakis, N.; Gill, A.; Clarke, S.J. A Longitudinal Investigation of Inflammatory Markers in Colorectal Cancer Patients Perioperatively Demonstrates Benefit in Serial Remeasurement. Ann. Surg. 2018, 267, 1119–1125. [Google Scholar] [CrossRef] [PubMed]
- Bailon-Cuadrado, M.; Perez-Saborido, B.; Sanchez-Gonzalez, J.; Rodriguez-Lopez, M.; Mayo-Iscar, A.; Pacheco-Sanchez, D. A new dimensional-reducing variable obtained from original inflammatory scores is highly associated to morbidity after curative surgery for colorectal cancer. Int. J. Color. Dis. 2018, 33, 1225–1234. [Google Scholar] [CrossRef] [PubMed]
- Curtis, N.J.; Dennison, G.; Salib, E.; Hashimoto, D.A.; Francis, N.K. Artificial Neural Network Individualised Prediction of Time to Colorectal Cancer Surgery. Gastroenterol. Res. Pr. 2019, 2019, 1285931. [Google Scholar] [CrossRef]
- Francis, N.K.; Luther, A.; Salib, E.; Allanby, L.; Messenger, D.; Allison, A.S.; Smart, N.; Ockrim, J.B. The use of artificial neural networks to predict delayed discharge and readmission in enhanced recovery following laparoscopic colorectal cancer surgery. Tech. Coloproctol. 2015, 19, 419–428. [Google Scholar] [CrossRef]
- Peng, J.-H.; Fang, Y.-J.; Li, C.-X.; Ou, Q.-J.; Jiang, W.; Lu, S.-X.; Lu, Z.-H.; Li, P.-X.; Yun, J.-P.; Zhang, R.-X.; et al. A scoring system based on artificial neural network for predicting 10-year survival in stage II A colon cancer patients after radical surgery. Oncotarget 2016, 7, 22939–22947. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kavitha, M.S.; Gangadaran, P.; Jackson, A.; Venmathi Maran, B.A.; Kurita, T.; Ahn, B.C. Deep Neural Network Models for Colon Cancer Screening. Cancers 2022, 14, 3707. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Jonnagaddala, J.; Cen, M.; Zhang, H.; Xu, S. Colorectal Cancer Survival Prediction Using Deep Distribution Based Multiple-Instance Learning. Entropy 2022, 24, 1669. [Google Scholar] [CrossRef] [PubMed]
- Jansen-Winkeln, B.; Barberio, M.; Chalopin, C.; Schierle, K.; Diana, M.; Köhler, H.; Gockel, I.; Maktabi, M. Feedforward Artificial Neural Network-Based Colorectal Cancer Detection Using Hyperspectral Imaging: A Step towards Automatic Optical Biopsy. Cancers 2021, 13, 967. [Google Scholar] [CrossRef]
- Song, J.H.; Hong, Y.; Kim, E.R.; Kim, S.H.; Sohn, I. Utility of artificial intelligence with deep learning of hematoxylin and eosin-stained whole slide images to predict lymph node metastasis in T1 colorectal cancer using endoscopically resected specimens; prediction of lymph node metastasis in T1 colorectal cancer. J. Gastroenterol. 2022, 57, 654–666. [Google Scholar] [CrossRef]
- Leng, X.; Uddin, K.M.S.; Chapman, W., Jr.; Luo, H.; Kou, S.; Amidi, E.; Yang, G.; Chatterjee, D.; Shetty, A.; Hunt, S.; et al. Assessing Rectal Cancer Treatment Response Using Coregistered Endorectal Photoacoustic and US Imaging Paired with Deep Learning. Radiology 2021, 299, 349–358. [Google Scholar] [CrossRef]
- Hardy, N.P.; Mac Aonghusa, P.; Neary, P.M.; Cahill, R.A. Intraprocedural Artificial Intelligence for Colorectal Cancer Detection and Characterisation in Endoscopy and Laparoscopy. Surg Innov. 2021, 28, 768–775. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of Surgical Complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Rahbari, N.N.; Weitz, J.; Hohenberger, W.; Heald, R.J.; Moran, B.; Ulrich, A.; Holm, T.; Wong, W.D.; Tiret, E.; Moriya, Y.; et al. Definition and grading of anastomotic leakage following anterior resection of the rectum: A proposal by the International Study Group of Rectal Cancer. Surgery 2010, 147, 339–351. [Google Scholar] [CrossRef]
- Belciug, S.; Gorunescu, F. Intelligent Decision Support Systems—A Journey to Smarter Healthcare; Springer International Publishing: Cham, Switzerland, 2020; pp. 130–137. [Google Scholar]
- Tuomisto, A.E.; Mäkinen, M.J.; Väyrynen, J.P. Systemic inflammation in colorectal cancer: Underlying factors, effects, and prognostic significance. World J. Gastroenterol. 2019, 25, 4383–4404. [Google Scholar] [CrossRef] [PubMed]
- McMillan, D.C. Systemic inflammation, nutritional status and survival in patients with cancer. Curr. Opin. Clin. Nutr. Metab. Care 2009, 12, 223–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bopanna, S.; Ananthakrishnan, A.N.; Kedia, S.; Yajnik, V.; Ahuja, V. Risk of colorectal cancer in Asian patients with ulcerative colitis: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2017, 2, 269–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keller, D.S.; Windsor, A.; Cohen, R.; Chand, M. Colorectal cancer in inflammatory bowel disease: Review of the evidence. Tech. Coloproctol. 2019, 23, 3–13. [Google Scholar] [CrossRef]
- Garg, S.K.; Velayos, F.S.; Kisiel, J.B. Intestinal and Nonintestinal Cancer Risks for Patients with Crohn’s Disease. Gastroenterol. Clin. N. Am. 2017, 46, 515–529. [Google Scholar] [CrossRef]
- Kantola, T.; Klintrup, K.; Väyrynen, J.P.; Vornanen, J.; Bloigu, R.; Karhu, T.; Herzig, K.-H.; Näpänkangas, J.; Mäkelä, J.; Karttunen, T.J.; et al. Stage-dependent alterations of the serum cytokine pattern in colorectal carcinoma. Br. J. Cancer 2012, 107, 1729–1736. [Google Scholar] [CrossRef] [Green Version]
- Birgisson, H.; Tsimogiannis, K.; Freyhult, E.; Kamali-Moghaddam, M. Plasma Protein Profiling Reveal Osteoprotegerin as a Marker of Prognostic Impact for Colorectal Cancer. Transl. Oncol. 2018, 11, 1034–1043. [Google Scholar] [CrossRef]
- Xu, J.; Ye, Y.; Zhang, H.; Szmitkowski, M.; Mäkinen, M.J.; Li, P.; Xia, D.; Yang, J.; Wu, Y.; Wu, H. Diagnostic and Prognostic Value of Serum Interleukin-6 in Colorectal Cancer. Medicine 2016, 95, e2502. [Google Scholar] [CrossRef]
- Su’a, B.U.; Mikaere, H.L.; Rahiri, J.L.; Bissett, I.; Hill, A.G. Systematic review of the role of biomarkers in diagnosing anastomotic leakage following colorectal surgery. Br. J. Surg. 2017, 104, 503–512. [Google Scholar] [CrossRef]
- Dimitriou, N.; Felekouras, E.; Karavokyros, I.; Alexandrou, A.; Pikoulis, E.; Griniatsos, J. Neutrophils to lymphocytes ratio as a useful prognosticator for stage II colorectal cancer patients. BMC Cancer 2018, 18, 1202. [Google Scholar] [CrossRef] [Green Version]
- Dell’Aquila, E.; Cremolini, C.; Zeppola, T.; Lonardi, S.; Bergamo, F.; Masi, G.; Stellato, M.; Marmorino, F.; Schirripa, M.; Urbano, F.; et al. Prognostic and predictive role of neutrophil/lymphocytes ratio in metastatic colorectal cancer: A retrospective analysis of the TRIBE study by GONO. Ann. Oncol. 2018, 29, 924–930. [Google Scholar] [CrossRef]
- Clarke, S.J.; Burge, M.; Feeney, K.; Gibbs, P.; Jones, K.; Marx, G.; Molloy, M.P.; Price, T.; Reece, W.H.H.; Segelov, E.; et al. The prognostic role of inflammatory markers in patients with metastatic colorectal cancer treated with bevacizumab: A translational study [ASCENT]. PLoS ONE 2020, 15, e0229900. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yilmaz, H.; Cakmak, M.; Inan, O.; Darcin, T.; Akcay, A. Can neutrophil–lymphocyte ratio be independent risk factor for predicting acute kidney injury in patients with severe sepsis? Ren. Fail. 2015, 37, 225–229. [Google Scholar] [CrossRef] [PubMed]
- Suppiah, A.; Malde, D.; Arab, T.; Hamed, M.; Allgar, V.; Smith, A.M.; Morris-Stiff, G. The Prognostic Value of the Neutrophil–Lymphocyte Ratio (NLR) in Acute Pancreatitis: Identification of an Optimal NLR. J. Gastrointest. Surg. 2013, 17, 675–681. [Google Scholar] [CrossRef]
- Liu, C.-C.; Ko, H.-J.; Liu, W.-S.; Hung, C.-L.; Hu, K.-C.; Yu, L.-Y.; Shih, S.-C. Neutrophil-to-lymphocyte ratio as a predictive marker of metabolic syndrome. Medicine 2019, 98, e17537. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.-H.; Zhai, E.-T.; Yuan, Y.; Wu, K.-M.; Xu, J.-B.; Peng, J.-J.; Chen, C.-Q.; He, Y.-L.; Cai, S.-R. Systemic immune-inflammation index for predicting prognosis of colorectal cancer. World J. Gastroenterol. 2017, 23, 6261–6272. [Google Scholar] [CrossRef]
- Tong, Y.-S.; Tan, J.; Zhou, X.-L.; Song, Y.-Q.; Song, Y.-J. Systemic immune-inflammation index predicting chemoradiation resistance and poor outcome in patients with stage III non-small cell lung cancer. J. Transl. Med. 2017, 15, 221. [Google Scholar] [CrossRef]
- Chen, J.; Chen, M.-H.; Li, S.; Guo, Y.-L.; Zhu, C.-G.; Xu, R.-X.; Zhang, Y.; Sun, J.; Qing, P.; Liu, G.; et al. Usefulness of the neutrophil-to-lymphocyte ratio in predicting the severity of coronary artery disease: A Gensini Score Assessment. J. Atheroscler. Thromb. 2014, 21, 1271–1282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, J.; Li, S.; Zhang, S.; Liu, Y.; Ma, L.; Zhu, J.; Xin, Y.; Wang, Y.; Yang, C.; Cheng, Y. Systemic immune-inflammation index, neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio can predict clinical outcomes in patients with metastatic non-small-cell lung cancer treated with nivolumab. J. Clin. Lab. Anal. 2019, 33, e22964. [Google Scholar] [CrossRef]
- Kamonvarapitak, T.; Matsuda, A.; Matsumoto, S.; Jamjittrong, S.; Sakurazawa, N.; Kawano, Y.; Yamada, T.; Suzuki, H.; Miyashita, M.; Yoshida, H. Preoperative lymphocyte-to-monocyte ratio predicts postoperative infectious complications after laparoscopic colorectal cancer surgery. Int. J. Clin. Oncol. 2020, 25, 633–640. [Google Scholar] [CrossRef]
- Wen, J.; Pan, T.; Yuan, Y.-C.; Huang, Q.-S.; Shen, J. Nomogram to predict postoperative infectious complications after surgery for colorectal cancer: A retrospective cohort study in China. World J. Surg. Oncol. 2021, 19, 204. [Google Scholar] [CrossRef] [PubMed]
- Paliogiannis, P.; Deidda, S.; Maslyankov, S.; Paycheva, T.; Farag, A.; Mashhour, A.; Misiakos, E.; Papakonstantinou, D.; Mik, M.; Losinska, J.; et al. Blood cell count indexes as predictors of anastomotic leakage in elective colorectal surgery: A multicenter study on 1432 patients. World J. Surg. Oncol. 2020, 18, 89. [Google Scholar] [CrossRef] [PubMed]
- Renganathan, V. Overview of artificial neural network models in the biomedical domain. Bratisl. Lek. Listy 2019, 120, 536–540. [Google Scholar] [CrossRef]
- Que, S.-J.; Chen, Q.-Y.; Liu, Z.-Y.; Wang, J.-B.; Lin, J.-X.; Lu, J.; Cao, L.-L.; Lin, M.; Tu, R.-H.; Huang, Z.-N.; et al. Application of preoperative artificial neural network based on blood biomarkers and clinicopathological parameters for predicting long-term survival of patients with gastric cancer. World J. Gastroenterol. 2019, 25, 6451–6464. [Google Scholar] [CrossRef]
- Wise, E.S.; Amateau, S.K.; Ikramuddin, S.; Leslie, D.B. Prediction of thirty-day morbidity and mortality after laparoscopic sleeve gastrectomy: Data from an artificial neural network. Surg. Endosc. 2020, 34, 3590–3596. [Google Scholar] [CrossRef]
- Van den Bosch, T.; Warps, A.L.K.; tot Babberich, M.P.D.N.; Stamm, C.; Geerts, B.F.; Vermeulen, L.; Wouters, M.W.J.M.; Dekker, J.W.T.; Tollenaar, R.A.E.M.; Tanis, P.J.; et al. Predictors of 30-Day Mortality among Dutch Patients Undergoing Colorectal Cancer Surgery, 2011–2016. JAMA Netw. Open 2021, 4, e217737. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Factor | Subtype/Measurement | n (281) | Percentage (%) |
|---|---|---|---|
| Age | Mean ± SD | 68.70 ± 10.55 | |
| Range (y) | 27–96 | ||
| Sex | M | 160 | 56.9% |
| F | 121 | 43.1% | |
| Localization | Right colon | 72 | 25.62% |
| Transverse colon | 14 | 4.98% | |
| Descendent colon | 24 | 8.54% | |
| Sigmoid colon | 67 | 23.84% | |
| Rectosigmoid junction Rectum | 23 81 | 8.18% 28.82% | |
| Comorbidities | Cardiovascular diseases | 151 | 53.7% |
| Diabetes mellitus | 38 | 13.5% | |
| Obesity | 29 | 10.3% | |
| Staging | T4 | 91 | 32.4% |
| T3 | 139 | 49.5% | |
| T2 | 42 | 14.9% | |
| T1 | 9 | 3.2% | |
| N0 | 109 | 38.8% | |
| N1 | 99 | 35.2% | |
| N2 | 73 | 26.0% | |
| M1 | 51 | 18.1% | |
| Postoperative complications | 87 | 30.9% | |
| Anastomotic leakage | 24 | 8.5% | |
| Wound | 31 | 11.0% | |
| Sepsis | 12 | 4.3% | |
| Cardiovascular event Other | 17 24 | 6.0% 8.5% | |
| Complication grade (Clavien–Dindo grade) | Mild complications (1–II) | 39 | 13.8% |
| Moderately severe complications (III–IV) | 27 | 9.6% | |
| Severe complications (V) | 21 | 7.47% |
| Variable | Avg ± SD | 95% CI |
|---|---|---|
| Hb | 10.92 ± 2.44 | 10.64–11.20 |
| Platelet | 283.62 ± 119.84 | 269.77–297.47 |
| Neutrophils | 6.276 ± 4.45 | 5.76–6.79 |
| SII | 1301.99 ± 1441.31 | 1132.73–1471.24 |
| NLR | 4.47 ± 4.09 | 3.78–4.98 |
| LMR | 3.45 ± 3.00 | 3.10–3.80 |
| PLR | 194.82 ± 131.73 | 179.60–210.05 |
| Mean ± SD | 95% CI | p (t-Test) | R (Pearson) | |
|---|---|---|---|---|
| SII | ||||
| Without AL (n = 164) | 993.35 ± 878.94 | 857.82 to 1128.87 | 0.001 | 0.251 |
| With AL (n = 22) | 1913.19 ± 2368 | 863.17 to 2963.20 | ||
| NLR | ||||
| Without AL (n = 164) | 3.17 ± 1.70 | 2.91 to 3.43 | 0.001 | 0.42 |
| With AL (n = 22) | 6.73 ± 5.54 | 4.27 to 9.19 | ||
| LMR | ||||
| Without AL (n = 164) | 4.04 ± 3.48 | 3.51 to 4.58 | 0.06 | |
| With AL (n = 22) | 2.50 ± 1.65 | 1.77 to 3.24 | 0.04 | |
| PLR | ||||
| Without AL (n = 164) | 177.32 ± 86.10 | 164.04 to 190.60 | 0.14 | |
| With AL (n = 22) | 195.66 ± 125.97 | 139.80 to 251.51 | 0.37 |
| Grade of Complication | Avg ± St Dev | 95% CI | p (ANOVA) | r (Pearson) |
|---|---|---|---|---|
| SII | ||||
| No complications (n = 194) | 897.99 ± 571.60 | 817.05 to 978.93 | 0.001 | 0.341 |
| Mild complications (n = 39) | 2331.28 ± 2064.51 | 1662.04 to 3000.52 | ||
| Moderately severe complications (n = 27) | 2224.32 ± 2427.79 | 1263.92 to 3184.72 | ||
| Severe complications (n = 21) | 1936.72 ± 2224.67 | 924.06 to 2949.38 | ||
| NLR | ||||
| No complications (n = 194) | 3.15 ± 1.58 | 2.92 to 3.37 | 0.001 | 0.412 |
| Mild complications (n = 39) | 7.57 ± 4.62 | 6.08 to 9.07 | ||
| Moderately severe complications (n = 27) | 7.66 ± 6.55 | 5.07 to 10.25 | ||
| Severe complications (n = 21) | 6.69 ± 6.90 | 3.55 to 9.84 | ||
| LMR | ||||
| No complications (n = 194) | 4.50 ± 9.71 | 3.13 to 5.88 | 0.107 | 0.096 |
| Mild complications (n = 39) | 2.09 ± 1.15 | 1.71 to 2.46 | ||
| Moderately severe complications (n = 27) | 2.61 ± 1.59 | 1.98 to 3.25 | ||
| Severe complications (n = 21) | 2.70 ± 1.84 | 1.86 to 3.55 | ||
| PLR | ||||
| No complications (n = 194) | 175.67 ± 81.30 | 164.15 to 187.18 | 0.002 | 0.188 |
| Mild complications (n = 39) | 246.81 ± 139.02 | 201.75 to 291.88 | ||
| Moderately severe complications (n = 27) | 211.09 ± 133.46 | 158.29 to 263.89 | ||
| Severe complications (n = 21) | 250.46 ± 315.77 | 106.73 to 394.20 | ||
| Variable | Odds Ratio (OR) | 95% CI | p Value | |
|---|---|---|---|---|
| Age | 1.067 | 0.989 | 1.151 | 0.093 |
| Obesity | 76.149 | 0.096 | 60,360.412 | 0.203 |
| Diabetes | 0.197 | 0.021 | 1.836 | 0.154 |
| Local tumor extension (T) | 0.652 | |||
| T 1 | 6.744 | 0.010 | 4477.042 | 0.565 |
| T 2 | 2.245 | 0.207 | 24.303 | 0.506 |
| T 3 | 2.958 | 0.531 | 16.483 | 0.216 |
| Lymph-node extension (n) | 0.233 | |||
| n 1 | 0.618 | 0.051 | 7.462 | 0.705 |
| n 2 | 2.702 | 0.306 | 23.849 | 0.371 |
| Metastasis (M) | 0.400 | 0.072 | 2.226 | 0.296 |
| Hb | 1.531 | 1.043 | 2.247 | 0.030 |
| Thrombocytes | 1.002 | 0.989 | 1.015 | 0.806 |
| NLR | 3.159 | 1.328 | 7.517 | 0.009 |
| SII | 0.998 | 0.996 | 1.001 | 0.136 |
| PLR | 0.999 | 0.986 | 1.012 | 0.857 |
| LMR | 1.040 | 0.790 | 1.368 | 0.779 |
| Proteins | 0.691 | 0.280 | 1.707 | 0.423 |
| Variable | Odds Ratio (OR) | 95% CI | p Value | |
|---|---|---|---|---|
| Age | 1.015 | 0.977 | 1.054 | 0.452 |
| Sex | 2.020 | 0.891 | 4.579 | 0.092 |
| Obesity | 1.666 | 0.348 | 7.983 | 0.523 |
| Diabetes | 0.960 | 0.300 | 3.071 | 0.945 |
| Local tumor extension (T) | 0.916 | |||
| T 1 | 0.624 | 0.031 | 12.734 | 0.759 |
| T 2 | 0.782 | 0.212 | 2.884 | 0.712 |
| T 3 | 0.726 | 0.296 | 1.783 | 0.485 |
| Lymph-node extension (n) | 0.476 | |||
| n 1 | 0.517 | 0.174 | 1.539 | 0.236 |
| n 2 | 0.618 | 0.222 | 1.717 | 0.356 |
| Metastasis (M) | 1.113 | 0.415 | 2.983 | 0.832 |
| Hb | 1.020 | 0.830 | 1.252 | 0.852 |
| Thrombocytes | 0.990 | 0.982 | 0.999 | 0.023 |
| NLR | 1.104 | 0.628 | 1.626 | 0.648 |
| SII | 1.002 | 0.723 | 1.686 | 0.051 |
| PLR | 0.999 | 1.000 | 1.003 | 0.503 |
| LMR | 0.986 | 0.995 | 1.003 | 0.898 |
| Proteins | 1.010 | 0.799 | 1.217 | 0.966 |
| Predicted Classes | |||||
|---|---|---|---|---|---|
| Anastomotic Leakage | Complication | ||||
| Yes | No | Yes | No | ||
| True classes | Yes | 257 | 41 | 144 | 34 |
| No | 0 | 216 | 50 | 160 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patrascu, S.; Cotofana-Graure, G.-M.; Surlin, V.; Mitroi, G.; Serbanescu, M.-S.; Geormaneanu, C.; Rotaru, I.; Patrascu, A.-M.; Ionascu, C.M.; Cazacu, S.; et al. Preoperative Immunocite-Derived Ratios Predict Surgical Complications Better when Artificial Neural Networks Are Used for Analysis—A Pilot Comparative Study. J. Pers. Med. 2023, 13, 101. https://doi.org/10.3390/jpm13010101
Patrascu S, Cotofana-Graure G-M, Surlin V, Mitroi G, Serbanescu M-S, Geormaneanu C, Rotaru I, Patrascu A-M, Ionascu CM, Cazacu S, et al. Preoperative Immunocite-Derived Ratios Predict Surgical Complications Better when Artificial Neural Networks Are Used for Analysis—A Pilot Comparative Study. Journal of Personalized Medicine. 2023; 13(1):101. https://doi.org/10.3390/jpm13010101
Chicago/Turabian StylePatrascu, Stefan, Georgiana-Maria Cotofana-Graure, Valeriu Surlin, George Mitroi, Mircea-Sebastian Serbanescu, Cristiana Geormaneanu, Ionela Rotaru, Ana-Maria Patrascu, Costel Marian Ionascu, Sergiu Cazacu, and et al. 2023. "Preoperative Immunocite-Derived Ratios Predict Surgical Complications Better when Artificial Neural Networks Are Used for Analysis—A Pilot Comparative Study" Journal of Personalized Medicine 13, no. 1: 101. https://doi.org/10.3390/jpm13010101