
Nanotechnologies in Obstetrics and Cancer during Pregnancy: A Narrative Review

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
3. Nanotechnologies and Pregnancy
4. The Placental Barrier, Therapeutic Perspectives of Nanoparticles, and Nanotoxicology
5. Point-of-Care Testing and Other Applications in Diagnostics
6. Preterm Birth
7. Preeclampsia and Fetal Growth Restriction
8. Diabetes Mellitus
9. In Utero Gene Therapy
10. Assisted Reproductive Technology
11. Cancer in Pregnancy
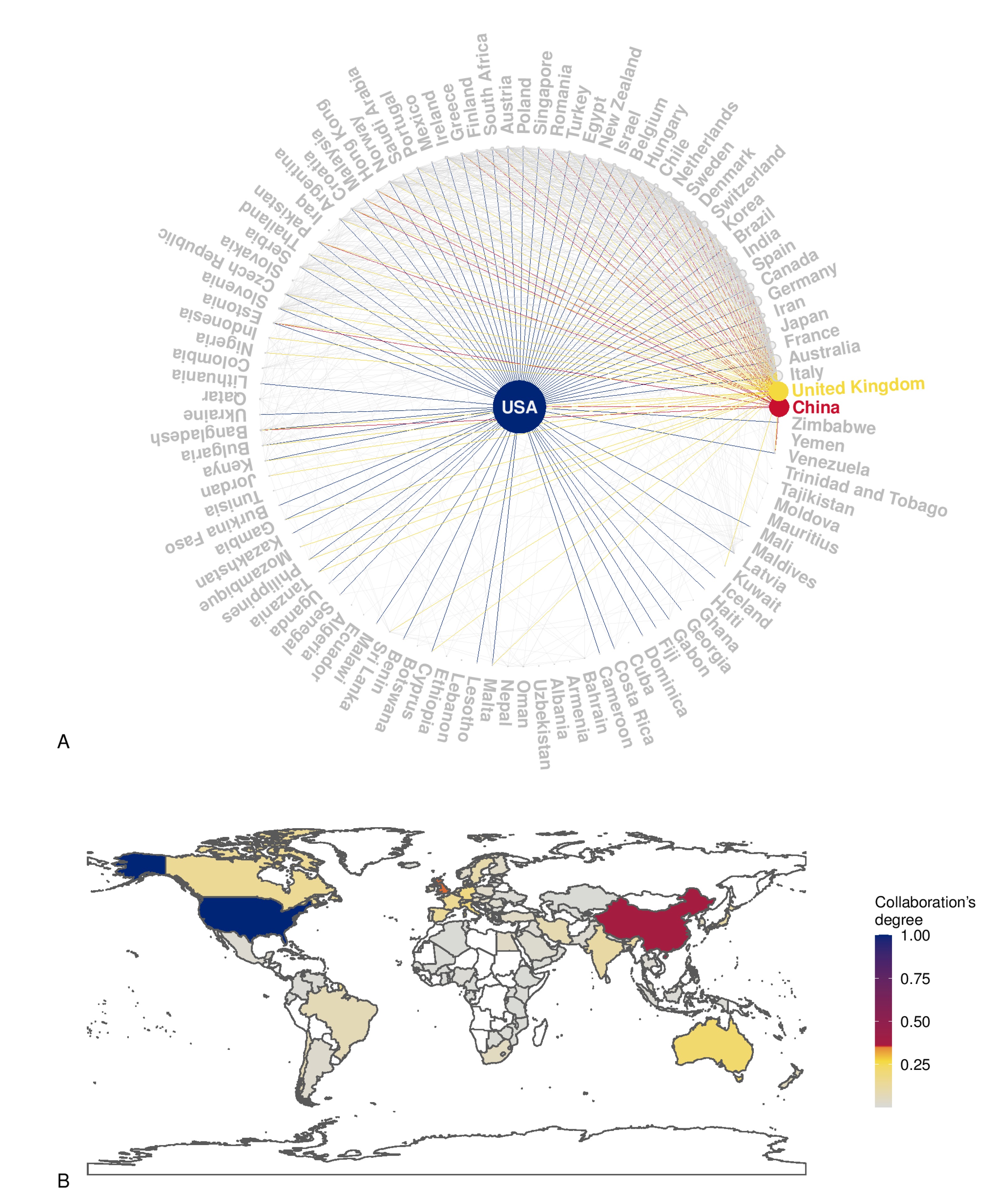
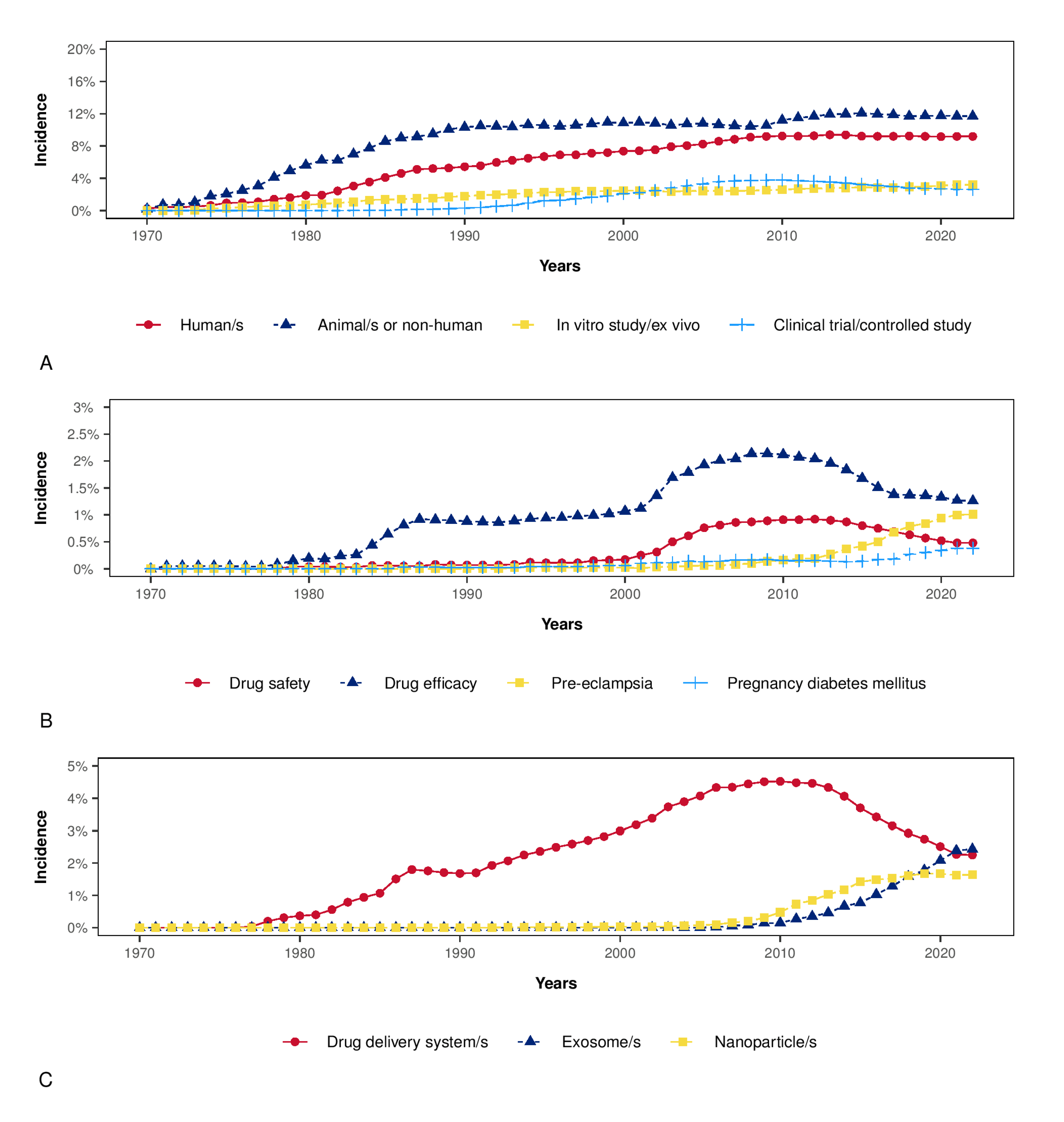
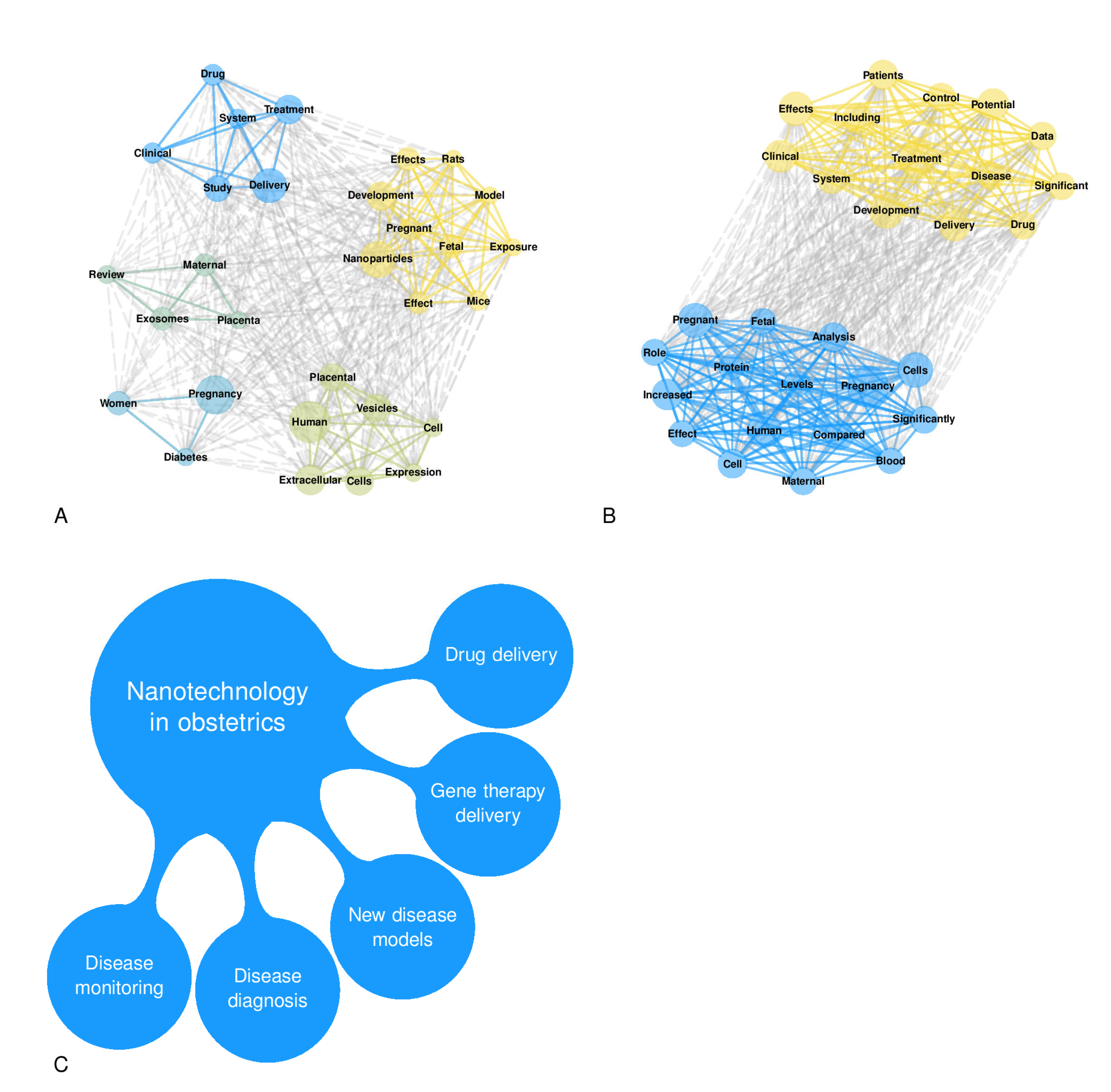
12. Bibliometric Analysis
13. Limitations
14. Implications for Clinicians and Policy-Makers/Healthcare Providers
15. Unanswered Questions and Future Research
16. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pearlman, S.A. Advancements in neonatology through quality improvement. J Perinatol. 2022, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Adane, A.A.; Bailey, H.D.; Marriott, R.; Farrant, B.M.; White, S.W.; Stanley, F.J.; Shepherd, C.C.J. Disparities between Aboriginal and non-Aboriginal perinatal mortality rates in Western Australia from 1980 to 2015. Paediatr. Perinat. Epidemiol. 2019, 33, 412–420. [Google Scholar] [CrossRef] [PubMed]
- Allen, K.M.; Smith, B.; Iliev, I.; Evans, J.; Werthammer, J. Short term cost of care for the surviving periviable neonate. J. Neonatal Perinat. Med. 2017, 10, 191–194. [Google Scholar] [CrossRef] [PubMed]
- Khan, K.A.; Petrou, S.; Dritsaki, M.; Johnson, S.J.; Manktelow, B.; Draper, E.S.; Smith, L.K.; Seaton, S.E.; Marlow, N.; Dorling, J.; et al. Economic costs associated with moderate and late preterm birth: A prospective population-based study. BJOG 2015, 122, 1495–1505. [Google Scholar] [CrossRef] [PubMed]
- Chawanpaiboon, S.; Vogel, J.P.; Moller, A.-B.; Lumbiganon, P.; Petzold, M.; Hogan, D.; Landoulsi, S.; Jampathong, N.; Kongwattanakul, K.; Laopaiboon, M.; et al. Global, regional, and national estimates of levels of preterm birth in 2014: A systematic review and modelling analysis. Lancet Glob. Health 2019, 7, e37–e46. [Google Scholar] [CrossRef]
- Liu, L.; Oza, S.; Hogan, D.; Perin, J.; Rudan, I.; Lawn, J.E.; Cousens, S.; Mathers, C.; Black, R.E. Global, regional, and national causes of child mortality in 2000-13, with projections to inform post-2015 priorities: An updated systematic analysis. Lancet 2015, 385, 430–440. [Google Scholar] [CrossRef]
- Driul, L.; Londero, A.P.; Adorati-Menegato, A.; Vogrig, E.; Bertozzi, S.; Fachechi, G.; Forzano, L.; Cacciaguerra, G.; Perin, E.; Miceli, A.; et al. Therapy side-effects and predictive factors for preterm delivery in patients undergoing tocolysis with atosiban or ritodrine for threatened preterm labour. J. Obstet. Gynaecol. 2014, 34, 684–689. [Google Scholar] [CrossRef]
- Fruscalzo, A.; Londero, A.P.; Orsaria, M.; Marzinotto, S.; Driul, L.; Di Loreto, C.; Mariuzzi, L. Placental fibronectin staining is unaffected in pregnancies complicated by late-onset intrauterine growth restriction and small for gestational age fetuses. Int. J. Gynaecol. Obstet. 2020, 148, 253–260. [Google Scholar] [CrossRef]
- Xodo, S.; Cecchini, F.; Celante, L.; Novak, A.; Rossetti, E.; Baccarini, G.; Londero, A.P.; Driul, L. Preeclampsia and low sodium: A retrospective cohort analysis and literature review. Pregnancy Hypertens. 2021, 23, 169–173. [Google Scholar] [CrossRef]
- Visentin, S.; Londero, A.P.; Camerin, M.; Grisan, E.; Cosmi, E. A possible new approach in the prediction of late gestational hypertension: The role of the fetal aortic intima-media thickness. Medicine 2017, 96, e5515. [Google Scholar] [CrossRef]
- Visentin, S.; Londero, A.P.; Grumolato, F.; Trevisanuto, D.; Zanardo, V.; Ambrosini, G.; Cosmi, E. Timing of delivery and neonatal outcomes for small-for-gestational-age fetuses. J. Ultrasound Med. 2014, 33, 1721–1728. [Google Scholar] [CrossRef] [PubMed]
- Fruscalzo, A.; Cividino, A.; Rossetti, E.; Maurigh, A.; Londero, A.P.; Driul, L. First trimester PAPP-A serum levels and long-term metabolic outcome of mothers and their offspring. Sci. Rep. 2020, 10, 5131. [Google Scholar] [CrossRef] [PubMed]
- Fruscalzo, A.; Londero, A.P.; Driul, L.; Henze, A.; Tonutti, L.; Ceraudo, M.; Zanotti, G.; Berni, R.; Schweigert, F.J.; Raila, J. First trimester concentrations of the TTR-RBP4-retinol complex components as early markers of insulin-treated gestational diabetes mellitus. Clin. Chem. Lab. Med. 2015, 53, 1643–1651. [Google Scholar] [CrossRef] [PubMed]
- Xodo, S.; Londero, A.P.; D’Agostin, M.; Novak, A.; Galasso, S.; Pittini, C.; Baccarini, G.; Grimaldi, F.; Driul, L. Is Glycated Hemoglobin A1c Level Associated with Adverse Pregnancy Outcomes of Women Affected by Pre-Gestational Diabetes? Medicina 2021, 57, 461. [Google Scholar] [CrossRef]
- Londero, A.P.; Rossetti, E.; Pittini, C.; Cagnacci, A.; Driul, L. Maternal age and the risk of adverse pregnancy outcomes: A retrospective cohort study. BMC Pregnancy Childbirth 2019, 19, 261. [Google Scholar] [CrossRef]
- Johansson, A.L.; Fredriksson, I.; Mellemkjaer, L.; Stensheim, H.; Lähteenmäki, P.; Winther, J.F.; Ullenhag, G.J.; Lundberg, F.E. Cancer survival in women diagnosed with pregnancy-associated cancer: An overview using nationwide registry data in Sweden 1970–2018. Eur. J. Cancer 2021, 155, 106–115. [Google Scholar] [CrossRef]
- Wolters, V.; Heimovaara, J.; Maggen, C.; Cardonick, E.; Boere, I.; Lenaerts, L.; Amant, F. Management of pregnancy in women with cancer. Int. J. Gynecol. Cancer 2021, 31, 314–322. [Google Scholar] [CrossRef]
- Kannan, R.M.; Kannan, S. Emerging nanomedicine approaches in obstetrics. Am. J. Obstet. Gynecol. 2017, 216, 201–203. [Google Scholar] [CrossRef]
- Tesarova, P.; Pavlista, D.; Parizek, A. Is It Possible to Personalize the Diagnosis and Treatment of Breast Cancer during Pregnancy? J. Pers. Med. 2020, 11, 18. [Google Scholar] [CrossRef]
- Patel, S.P.; Patel, P.B.; Parekh, B.B. Application of nanotechnology in cancers prevention, early detection and treatment. J. Cancer Res. Ther. 2014, 10, 479–486. [Google Scholar]
- Barkalina, N.; Charalambous, C.; Jones, C.; Coward, K. Nanotechnology in reproductive medicine: Emerging applications of nanomaterials. Nanomedicine 2014, 10, 921–938. [Google Scholar] [CrossRef] [PubMed]
- Cerqueira, B.B.S.; Lasham, A.; Shelling, A.N.; Al-Kassas, R. Nanoparticle therapeutics: Technologies and methods for overcoming cancer. Eur. J. Pharm. Biopharm. 2015, 97, 140–151. [Google Scholar] [CrossRef] [PubMed]
- Aria, M.; Cuccurullo, C. Bibliometrix: An R-tool for comprehensive science mapping analysis. J. Informetr. 2017, 11, 959–975. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022. [Google Scholar]
- Glover, D.D.; Amonkar, M.; Rybeck, B.F.; Tracy, T.S. Prescription, over-the-counter, and herbal medicine use in a rural, obstetric population. Am. J. Obstet. Gynecol. 2003, 188, 1039–1045. [Google Scholar] [CrossRef]
- Lee, E.; Maneno, M.K.; Smith, L.; Weiss, S.R.; Zuckerman, I.H.; Wutoh, A.K.; Xue, Z. National patterns of medication use during pregnancy. Pharmacoepidemiol. Drug Saf. 2006, 15, 537–545. [Google Scholar] [CrossRef]
- Refuerzo, J.S.; Blackwell, S.C.; Sokol, R.J.; Lajeunesse, L.; Firchau, K.; Kruger, M.; Sorokin, Y. Use of over-the-counter medications and herbal remedies in pregnancy. Am. J. Perinatol. 2005, 22, 321–324. [Google Scholar] [CrossRef]
- Joshi, M.D. Drug delivery during pregnancy: How can nanomedicine be used? Ther. Deliv. 2017, 8, 1023–1025. [Google Scholar] [CrossRef]
- Irvin-Choy, N.S.; Nelson, K.M.; Gleghorn, J.P.; Day, E.S. Design of nanomaterials for applications in maternal/fetal medicine. J. Mater. Chem. B 2020, 8, 6548–6561. [Google Scholar] [CrossRef]
- Pritchard, N.; Kaitu’u-Lino, T.; Harris, L.; Tong, S.; Hannan, N. Nanoparticles in pregnancy: The next frontier in reproductive therapeutics. Hum. Reprod. Update 2021, 27, 280–304. [Google Scholar] [CrossRef]
- Keelan, J.A.; Leong, J.W.; Ho, D.; Iyer, K.S. Therapeutic and safety considerations of nanoparticle-mediated drug delivery in pregnancy. Nanomedicine 2015, 10, 2229–2247. [Google Scholar] [CrossRef]
- Wick, P.; Malek, A.; Manser, P.; Meili, D.; Maeder-Althaus, X.; Diener, L.; Diener, P.-A.; Zisch, A.; Krug, H.F.; Von Mandach, U. Barrier capacity of human placenta for nanosized materials. Environ. Health Perspect. 2010, 118, 432–436. [Google Scholar] [CrossRef] [PubMed]
- de Araújo, T.E.; Milián, I.C.B.; de Souza, G.; da Silva, R.J.; Rosini, A.M.; Guirelli, P.M.; Franco, P.S.; Barbosa, B.F.; Ferro, E.A.V.; da Costa, I.N. Experimental models of maternal-fetal interface and their potential use for nanotechnology applications. Cell Biol. Int. 2020, 44, 36–50. [Google Scholar] [CrossRef] [PubMed]
- Caporale, N.; Leemans, M.; Birgersson, L.; Germain, P.-L.; Cheroni, C.; Borbély, G.; Engdahl, E.; Lindh, C.; Bressan, R.B.; Cavallo, F.; et al. From cohorts to molecules: Adverse impacts of endocrine disrupting mixtures. Science 2022, 375, eabe8244. [Google Scholar] [CrossRef] [PubMed]
- Fliedel, L.; Alhareth, K.; Mignet, N.; Fournier, T.; Andrieux, K. Placental Models for Evaluation of Nanocarriers as Drug Delivery Systems for Pregnancy Associated Disorders. Biomedicines 2022, 10, 936. [Google Scholar] [CrossRef]
- Shojaei, S.; Ali, M.S.; Suresh, M.; Upreti, T.; Mogourian, V.; Helewa, M.; Labouta, H.I. Dynamic placenta-on-a-chip model for fetal risk assessment of nanoparticles intended to treat pregnancy-associated diseases. Biochim. Biophys. Acta Mol. Basis Dis. 2021, 1867, 166131. [Google Scholar] [CrossRef]
- Tutar, R.; Çelebi-Saltik, B. Modeling of Artificial 3D Human Placenta. Cells Tissues Organs 2021, 1–10. [Google Scholar] [CrossRef]
- Viola, L.; Marzinotto, S.; Bertacchi, M.; Londero, A.P.; Orsaria, M.; Bertozzi, S.; Driul, L.; Di Loreto, C.; Studer, M.; Mariuzzi, L.; et al. COUP-TFI deletion affects angiogenesis and apoptosis related gene expression in mouse placenta: Results of an explorative study. Clin. Exp. Obstet. Gynecol. 2022, 49, 1. [Google Scholar] [CrossRef]
- Al-Enazy, S.; Ali, S.; Albekairi, N.; El-Tawil, M.; Rytting, E. Placental control of drug delivery. Adv. Drug Deliv. Rev. 2017, 116, 63–72. [Google Scholar] [CrossRef]
- Rattanapinyopituk, K.; Shimada, A.; Morita, T.; Sakurai, M.; Asano, A.; Hasegawa, T.; Inoue, K.; Takano, H. Demonstration of the clathrin- and caveolin-mediated endocytosis at the maternal-fetal barrier in mouse placenta after intravenous administration of gold nanoparticles. J. Vet. Med. Sci. 2014, 76, 377–387. [Google Scholar] [CrossRef]
- Kloet, S.K.; Walczak, A.P.; Louisse, J.; van den Berg, H.H.; Bouwmeester, H.; Tromp, P.; Fokkink, R.G.; Rietjens, I.M. Translocation of positively and negatively charged polystyrene nanoparticles in an in vitro placental model. Toxicol. In Vitro 2015, 29, 1701–1710. [Google Scholar] [CrossRef]
- Soininen, S.K.; Repo, J.K.; Karttunen, V.; Auriola, S.; Vähäkangas, K.H.; Ruponen, M. Human placental cell and tissue uptake of doxorubicin and its liposomal formulations. Toxicol. Lett. 2015, 239, 108–114. [Google Scholar] [CrossRef] [PubMed]
- Cureton, N.; Korotkova, I.; Baker, B.; Greenwood, S.; Wareing, M.; Kotamraju, V.R.; Teesalu, T.; Cellesi, F.; Tirelli, N.; Ruoslahti, E.; et al. Selective Targeting of a Novel Vasodilator to the Uterine Vasculature to Treat Impaired Uteroplacental Perfusion in Pregnancy. Theranostics 2017, 7, 3715–3731. [Google Scholar] [CrossRef]
- Ali, S.; Rytting, E. Influences of nanomaterials on the barrier function of epithelial cells. Adv. Exp. Med. Biol. 2014, 811, 45–54. [Google Scholar]
- Rytting, E.; Cartwright, L.; Poulsen, M.S.; Nielsen, H.M.; Pojana, G.; Knudsen, L.E.; Saunders, M. In vitro placental model optimization for nanoparticle transport studies. Int. J. Nanomed. 2012, 7, 497–510. [Google Scholar] [CrossRef] [PubMed]
- Brown, D.M.; Wilson, M.R.; MacNee, W.; Stone, V.; Donaldson, K. Size-dependent proinflammatory effects of ultrafine polystyrene particles: A role for surface area and oxidative stress in the enhanced activity of ultrafines. Toxicol. Appl. Pharmacol. 2001, 175, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, S.J.; Crompton, L.A.; Sood, A.; Saunders, M.; Boyle, N.T.; Buckley, A.; Minogue, A.M.; McComish, S.F.; Jiménez-Moreno, N.; Cordero-Llana, O.; et al. Nanoparticle-induced neuronal toxicity across placental barriers is mediated by autophagy and dependent on astrocytes. Nat. Nanotechnol. 2018, 13, 427–433. [Google Scholar] [CrossRef]
- Menjoge, A.R.; Rinderknecht, A.L.; Navath, R.S.; Faridnia, M.; Kim, C.J.; Romero, R.; Miller, R.K.; Kannan, R.M. Transfer of PAMAM dendrimers across human placenta: Prospects of its use as drug carrier during pregnancy. J. Control. Release 2011, 150, 326–338. [Google Scholar] [CrossRef]
- Poulsen, M.S.; Mose, T.; Maroun, L.L.; Mathiesen, L.; Knudsen, L.E.; Rytting, E. Kinetics of silica nanoparticles in the human placenta. Nanotoxicology 2015, 9 (Suppl 1), 79–86. [Google Scholar] [CrossRef]
- Odijk, M.; van der Meer, A.D.; Levner, D.; Kim, H.J.; van der Helm, M.W.; Segerink, L.I.; Frimat, J.-P.; Hamilton, G.A.; Ingber, D.E.; Berg, A.V.D. Measuring direct current trans-epithelial electrical resistance in organ-on-a-chip microsystems. Lab Chip 2015, 15, 745–752. [Google Scholar] [CrossRef]
- Yamashita, K.; Yoshioka, Y.; Higashisaka, K.; Mimura, K.; Morishita, Y.; Nozaki, M.; Yoshida, T.; Ogura, T.; Nabeshi, H.; Nagano, K.; et al. Silica and titanium dioxide nanoparticles cause pregnancy complications in mice. Nat. Nanotechnol. 2011, 6, 321–328. [Google Scholar] [CrossRef]
- Zalgeviciene, V.; Kulvietis, V.; Bulotiene, D.; Didziapetriene, J.; Rotomskis, R. The effect of nanoparticles in rats during critical periods of pregnancy. Medicina 2012, 48, 256–264. [Google Scholar] [CrossRef] [PubMed]
- Austin, C.A.; Hinkley, G.K.; Mishra, A.R.; Zhang, Q.; Umbreit, T.H.; Betz, M.W.; Wildt, B.E.; Casey, B.J.; Francke-Carroll, S.; Hussain, S.M.; et al. Distribution and accumulation of 10 nm silver nanoparticles in maternal tissues and visceral yolk sac of pregnant mice, and a potential effect on embryo growth. Nanotoxicology 2016, 10, 654–661. [Google Scholar] [CrossRef] [PubMed]
- Ema, M.; Okuda, H.; Gamo, M.; Honda, K. A review of reproductive and developmental toxicity of silver nanoparticles in laboratory animals. Reprod. Toxicol. 2017, 67, 149–164. [Google Scholar] [CrossRef]
- Zhang, X.F.; Park, J.H.; Choi, Y.J.; Kang, M.H.; Gurunathan, S.; Kim, J.H. Silver nanoparticles cause complications in pregnant mice. Int. J. Nanomed. 2015, 10, 7057–7071. [Google Scholar]
- Salim, E.I.; Abdel-Halim, K.Y.; Abu-Risha, S.E.; Abdel-Latif, A.S. Induction of 8-hydroxydeoxyguanosine and ultrastructure alterations by silver nanoparticles attributing to placental transfer in pregnant rats and fetuses. Hum. Exp. Toxicol. 2019, 38, 734–745. [Google Scholar] [CrossRef] [PubMed]
- Campagnolo, L.; Massimiani, M.; Vecchione, L.; Piccirilli, D.; Toschi, N.; Magrini, A.; Bonanno, E.; Scimeca, M.; Castagnozzi, L.; Buonanno, G.; et al. Silver nanoparticles inhaled during pregnancy reach and affect the placenta and the foetus. Nanotoxicology 2017, 11, 687–698. [Google Scholar] [CrossRef]
- Wang, Z.; Zhang, C.; Liu, X.; Huang, F.; Wang, Z.; Yan, B. Oral intake of ZrO2 nanoparticles by pregnant mice results in nanoparticles’ deposition in fetal brains. Ecotoxicol. Environ. Saf. 2020, 202, 110884. [Google Scholar] [CrossRef]
- Pereira, K.V.; Giacomeli, R.; Gomes de Gomes, M.; Haas, S.E. The challenge of using nanotherapy during pregnancy: Technological aspects and biomedical implications. Placenta 2020, 100, 75–80. [Google Scholar] [CrossRef]
- Zhang, B.; Chen, Z.; Han, J.; Li, M.; Nayak, N.R.; Fan, X. Comprehensive Evaluation of the Effectiveness and Safety of Placenta-Targeted Drug Delivery Using Three Complementary Methods. J. Vis. Exp. 2018, 139, e58219. [Google Scholar] [CrossRef]
- Zhang, B.; Tan, L.; Yu, Y.; Wang, B.; Chen, Z.; Han, J.; Li, M.; Chen, J.; Xiao, T.; Ambati, B.K.; et al. Placenta-specific drug delivery by trophoblast-targeted nanoparticles in mice. Theranostics 2018, 8, 2765–2781. [Google Scholar] [CrossRef]
- Zhang, B.; Liang, R.; Zheng, M.; Cai, L.; Fan, X. Surface-Functionalized Nanoparticles as Efficient Tools in Targeted Therapy of Pregnancy Complications. Int. J. Mol. Sci. 2019, 20, 3642. [Google Scholar] [CrossRef] [PubMed]
- Refuerzo, J.S.; Leonard, F.; Bulayeva, N.; Gorenstein, D.; Chiossi, G.; Ontiveros, A.; Longo, M.; Godin, B. Uterus-targeted liposomes for preterm labor management: Studies in pregnant mice. Sci. Rep. 2016, 6, 34710. [Google Scholar] [CrossRef] [PubMed]
- Hua, S.; Vaughan, B. In vitro comparison of liposomal drug delivery systems targeting the oxytocin receptor: A potential novel treatment for obstetric complications. Int. J. Nanomed. 2019, 14, 2191–2206. [Google Scholar] [CrossRef]
- Hua, S. Synthesis and in vitro characterization of oxytocin receptor targeted PEGylated immunoliposomes for drug delivery to the uterus. J. Liposome Res. 2019, 29, 357–367. [Google Scholar] [CrossRef]
- Kalluri, R.; LeBleu, V.S. The biology, function, and biomedical applications of exosomes. Science 2020, 367, eaau6977. [Google Scholar] [CrossRef] [PubMed]
- Delorme-Axford, E.; Donker, R.B.; Mouillet, J.-F.; Chu, T.; Bayer, A.; Ouyang, Y.; Wang, T.; Stolz, D.B.; Sarkar, S.N.; Morelli, A.E.; et al. Human placental trophoblasts confer viral resistance to recipient cells. Proc. Natl. Acad. Sci. USA 2013, 110, 12048–12053. [Google Scholar] [CrossRef]
- Salomon, C.; Torres, M.J.; Kobayashi, M.; Scholz-Romero, K.; Sobrevia, L.; Dobierzewska, A.; Illanes, S.E.; Mitchell, M.D.; Rice, G.E. A gestational profile of placental exosomes in maternal plasma and their effects on endothelial cell migration. PLoS ONE 2014, 9, e98667. [Google Scholar] [CrossRef]
- Sarker, S.; Scholz-Romero, K.; Perez, A.; Illanes, S.E.; Mitchell, M.D.; Rice, G.E.; Salomon, C. Placenta-derived exosomes continuously increase in maternal circulation over the first trimester of pregnancy. J. Transl. Med. 2014, 12, 204. [Google Scholar] [CrossRef]
- Mitchell, M.D.; Peiris, H.N.; Kobayashi, M.; Koh, Y.Q.; Duncombe, G.; Illanes, S.E.; Rice, G.E.; Salomon, C. Placental exosomes in normal and complicated pregnancy. Am. J. Obstet. Gynecol. 2015, 213, S173–S181. [Google Scholar] [CrossRef]
- Salomon, C.; Scholz-Romero, K.; Sarker, S.; Sweeney, E.; Kobayashi, M.; Correa, P.; Longo, S.; Duncombe, G.; Mitchell, M.D.; Rice, G.E.; et al. Gestational Diabetes Mellitus Is Associated With Changes in the Concentration and Bioactivity of Placenta-Derived Exosomes in Maternal Circulation Across Gestation. Diabetes 2016, 65, 598–609. [Google Scholar] [CrossRef]
- Muoth, C.; Aengenheister, L.; Kucki, M.; Wick, P.; Buerki-Thurnherr, T. Nanoparticle transport across the placental barrier: Pushing the field forward! Nanomedicine 2016, 11, 941–957. [Google Scholar] [CrossRef] [PubMed]
- Leavitt, S. “A private little revolution”: The home pregnancy test in American culture. Bull. Hist. Med. 2006, 80, 317–345. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Wang, S.; Wang, L.; Li, F.; Pingguan-Murphy, B.; Lu, T.J.; Xu, F. Advances in paper-based point-of-care diagnostics. Biosens. Bioelectron. 2014, 54, 585–597. [Google Scholar] [CrossRef] [PubMed]
- Yetisen, A.K.; Akram, M.S.; Lowe, C.R. Paper-based microfluidic point-of-care diagnostic devices. Lab Chip 2013, 13, 2210–2251. [Google Scholar] [CrossRef]
- Cai, L.; Huang, Y.; Sun, P.; Zheng, W.; Zhou, S.; Huang, P.; Liang, Z. Accurate detection of β-hCG in women’s serum and cervical secretions for predicting early pregnancy viability based on time-resolved luminescent lanthanide nanoprobes. Nanoscale 2020, 12, 6729–6735. [Google Scholar] [CrossRef]
- Chiu, N.F.; Kuo, C.T.; Chen, C.Y. High-affinity carboxyl-graphene oxide-based SPR aptasensor for the detection of hCG protein in clinical serum samples. Int. J. Nanomed. 2019, 14, 4833–4847. [Google Scholar] [CrossRef]
- Kuo, H.T.; Yeh, J.Z.; Wu, P.H.; Jiang, C.M.; Wu, M.C. Application of immunomagnetic particles to enzyme-linked immunosorbent assay (ELISA) for improvement of detection sensitivity of HCG. J. Immunoass. Immunochem. 2012, 33, 377–387. [Google Scholar] [CrossRef]
- Kuo, H.T.; Yeh, J.Z.; Jiang, C.M.; Wu, M.C. Magnetic particle-linked anti hCG β antibody for immunoassay of human chorionic gonadotropin (hCG), potential application to early pregnancy diagnosis. J. Immunol. Methods 2012, 381, 32–40. [Google Scholar] [CrossRef]
- Bolnick, J.M.; Kilburn, B.A.; Bajpayee, S.; Reddy, N.; Jeelani, R.; Crone, B.; Simmerman, N.; Singh, M.; Diamond, M.; Armant, D.R. Trophoblast retrieval and isolation from the cervix (TRIC) for noninvasive prenatal screening at 5 to 20 weeks of gestation. Fertil. Steril. 2014, 102, 135–142. [Google Scholar] [CrossRef]
- Fritz, R.; Kohan-Ghadr, H.R.; Sacher, A.; Bolnick, A.D.; Kilburn, B.A.; Bolnick, J.M.; Diamond, M.; Drewlo, S.; Armant, D.R. Trophoblast retrieval and isolation from the cervix (TRIC) is unaffected by early gestational age or maternal obesity. Prenat. Diagn. 2015, 35, 1218–1222. [Google Scholar] [CrossRef]
- Rahaie, M.; Ostad-Hasanzadeh, B.; Faridbod, F. A Novel Fluorescence Nanobiosensor based on Modified Graphene Quantum dots-HTAB for Early Detection of Fetal Sexuality with Cell Free Fetal DNA. J. Fluoresc. 2021, 31, 1843–1853. [Google Scholar] [CrossRef] [PubMed]
- Calcagno, M.; D’Agata, R.; Breveglieri, G.; Borgatti, M.; Bellassai, N.; Gambari, R.; Spoto, G. Nanoparticle-Enhanced Surface Plasmon Resonance Imaging Enables the Ultrasensitive Detection of Non-Amplified Cell-Free Fetal DNA for Non-Invasive Prenatal Testing. Anal. Chem. 2022, 94, 1118–1125. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Chen, X.; Wang, Q.; Xiao, M.; Zhong, D.; Sun, W.; Zhang, G.; Zhang, Z. Ultrasensitive Monolayer MoS2 Field-Effect Transistor Based DNA Sensors for Screening of Down Syndrome. Nano Lett. 2019, 19, 1437–1444. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Zhao, S.; Wan, H.; Liu, Y.; Zhang, F.; Guo, X.; Zeng, W.; Zhang, H.; Zeng, L.; Qu, J.; et al. High-resolution DNA size enrichment using a magnetic nano-platform and application in non-invasive prenatal testing. Analyst 2020, 145, 5733–5739. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, S.M.; Wiepz, G.J.; Schotzko, M.; Simmons, H.A.; Mejia, A.; Ludwig, K.D.; Zhu, A.; Brunner, K.; Hernando, D.; Reeder, S.B.; et al. Impact of ferumoxytol magnetic resonance imaging on the rhesus macaque maternal-fetal interface. Biol. Reprod. 2020, 102, 434–444. [Google Scholar] [CrossRef]
- Gatta, G.; Di Grezia, G.; Cuccurullo, V.; Sardu, C.; Iovino, F.; Comune, R.; Ruggiero, A.; Chirico, M.; La Forgia, D.; Fanizzi, A.; et al. MRI in Pregnancy and Precision Medicine: A Review from Literature. J. Pers. Med. 2021, 12, 9. [Google Scholar] [CrossRef]
- Shetty, A.N.; Pautler, R.; Ghaghada, K.; Rendon, D.; Gao, H.; Starosolski, Z.; Bhavane, R.; Patel, C.; Annapragada, A.; Yallampalli, C.; et al. A liposomal Gd contrast agent does not cross the mouse placental barrier. Sci. Rep. 2016, 6, 27863. [Google Scholar] [CrossRef]
- Badachhape, A.A.; Kumar, A.; Ghaghada, K.B.; Stupin, I.V.; Srivastava, M.; Devkota, L.; Starosolski, Z.; Tanifum, E.A.; George, V.; Fox, K.A.; et al. Pre-clinical magnetic resonance imaging of retroplacental clear space throughout gestation. Placenta 2019, 77, 1–7. [Google Scholar] [CrossRef]
- Roberts, V.H.; Frias, A.E. Contrast-enhanced ultrasound for the assessment of placental development and function. Biotechniques 2020, 69, 392–399. [Google Scholar] [CrossRef]
- Wong, C.H.; Chen, C.P.; Chang, C.C.; Chen, C.Y. Bio-functionalized magnetic nanoparticles for the immunoassay of fetal fibronectin: A feasibility study for the prediction of preterm birth. Sci. Rep. 2017, 7, 42461. [Google Scholar] [CrossRef]
- Paul, J.W.; Smith, R. Preventing preterm birth: New approaches to labour therapeutics using Nanoparticles. Best Pract. Res. Clin. Obstet. Gynaecol. 2018, 52, 48–59. [Google Scholar] [CrossRef] [PubMed]
- Patki, M.; Giusto, K.; Gorasiya, S.; Reznik, S.E.; Patel, K. 17-α Hydroxyprogesterone Nanoemulsifying Preconcentrate-Loaded Vaginal Tablet: A Novel Non-Invasive Approach for the Prevention of Preterm Birth. Pharmaceutics 2019, 11, 335. [Google Scholar] [CrossRef] [PubMed]
- Attias Cohen, S.; Kingma, P.S.; Whitsett, J.A.; Goldbart, R.; Traitel, T.; Kost, J. SP-D loaded PLGA nanoparticles as drug delivery system for prevention and treatment of premature infant’s lung diseases. Int. J. Pharm. 2020, 585, 119387. [Google Scholar] [CrossRef] [PubMed]
- Buhimschi, C.S.; Bahtiyar, M.O.; Zhao, G.; Abdelghany, O.; Schneider, L.; Razeq, S.A.; Dulay, A.T.; Lipkind, H.S.; Mieth, S.; Rogers, L.; et al. Antenatal N-acetylcysteine to improve outcomes of premature infants with intra-amniotic infection and inflammation (Triple I): Randomized clinical trial. Pediatr. Res. 2021, 89, 175–184. [Google Scholar] [CrossRef] [PubMed]
- Londero, A.P.; Orsaria, M.; Marzinotto, S.; Grassi, T.; Fruscalzo, A.; Calcagno, A.; Bertozzi, S.; Nardini, N.; Stella, E.; Lellé, R.J.; et al. Placental aging and oxidation damage in a tissue micro-array model: An immunohistochemistry study. Histochem. Cell Biol. 2016, 146, 191–204. [Google Scholar] [CrossRef] [PubMed]
- Chiu, N.F.; Tai, M.J.; Wu, H.P.; Lin, T.L.; Chen, C.Y. Development of a bioaffinity SPR immunosensor based on functionalized graphene oxide for the detection of pregnancy-associated plasma protein A2 in human plasma. Int. J. Nanomed. 2019, 14, 6735–6748. [Google Scholar] [CrossRef]
- Chiu, N.F.; Tai, M.J.; Nurrohman, D.T.; Lin, T.L.; Wang, Y.H.; Chen, C.Y. Immunoassay-Amplified Responses Using a Functionalized MoS2-Based SPR Biosensor to Detect PAPP-A2 in Maternal Serum Samples to Screen for Fetal Down’s Syndrome. Int. J. Nanomed. 2021, 16, 2715–2733. [Google Scholar] [CrossRef]
- Pham, T.T.T.; Tran, D.P.; Nguyen, M.C.; Amen, M.T.; Winter, M.; Whitehead, C.; Toh, J.; Thierry, B. A simplified point-of-care testing approach for preeclampsia blood biomarkers based on nanoscale field effect transistors. Nanoscale. 2021, 13, 12279–12287. [Google Scholar] [CrossRef]
- Suman, P.; Gandhi, S.; Kumar, P.; Garg, K. Prospects of electrochemical immunosensors for early diagnosis of preeclampsia. Am. J. Reprod. Immunol. 2017, 77, e12584. [Google Scholar] [CrossRef]
- Sibley, C.P. Treating the dysfunctional placenta. J. Endocrinol. 2017, 234, R81–R97. [Google Scholar] [CrossRef]
- Alfaifi, A.A.; Heyder, R.S.; Bielski, E.R.; Almuqbil, R.M.; Kavdia, M.; Gerk, P.M.; da Rocha, S.R. Megalin-targeting liposomes for placental drug delivery. J. Control. Release 2020, 324, 366–378. [Google Scholar] [CrossRef] [PubMed]
- de Alwis, N.; Binder, N.K.; Beard, S.; Tu’uhevaha, J.; Tong, S.; Brownfoot, F.; Hannan, N.J. Novel approaches to combat preeclampsia: From new drugs to innovative delivery. Placenta 2020, 102, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Jena, M.K.; Sharma, N.R.; Petitt, M.; Maulik, D.; Nayak, N.R. Pathogenesis of Preeclampsia and Therapeutic Approaches Targeting the Placenta. Biomolecules 2020, 10, 953. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Li, H.; Xue, J.; Chen, P.; Zhou, Q.; Zhang, C. Nanoparticle-Mediated Simultaneous Downregulation of Placental Nrf2 and sFlt1 Improves Maternal and Fetal Outcomes in a Preeclampsia Mouse Model. ACS Biomater. Sci. Eng. 2020, 6, 5866–5873. [Google Scholar] [CrossRef]
- Pepe, G.J.; Albrecht, E.D. Novel Technologies for Target Delivery of Therapeutics to the Placenta during Pregnancy: A Review. Genes 2021, 12, 1255. [Google Scholar] [CrossRef]
- Renshall, L.J.; Beards, F.; Evangelinos, A.; Greenwood, S.L.; Brownbill, P.; Stevens, A.; Sibley, C.P.; Aplin, J.D.; Johnstone, E.D.; Teesalu, T.; et al. Targeted Delivery of Epidermal Growth Factor to the Human Placenta to Treat Fetal Growth Restriction. Pharmaceutics 2021, 13, 1778. [Google Scholar] [CrossRef]
- Yu, Q.; Qiu, Y.; Wang, X.; Tang, J.; Liu, Y.; Mei, L.; Li, M.; Yang, M.; Tang, L.; Gao, H.; et al. Efficient siRNA transfer to knockdown a placenta specific lncRNA using RGD-modified nano-liposome: A new preeclampsia-like mouse model. Int. J. Pharm. 2018, 546, 115–124. [Google Scholar] [CrossRef]
- Barani, M.; Sargazi, S.; Mohammadzadeh, V.; Rahdar, A.; Pandey, S.; Jha, N.K.; Gupta, P.K.; Thakur, V.K. Theranostic Advances of Bionanomaterials against Gestational Diabetes Mellitus: A Preliminary Review. J. Funct. Biomater. 2021, 12, 54. [Google Scholar] [CrossRef]
- Belsare, S.; Coté, G. Development of a colorimetric paper fluidic dipstick assay for measurement of glycated albumin to monitor gestational diabetes at the point-of-care. Talanta 2021, 223, 121728. [Google Scholar] [CrossRef]
- Cheng, X.; Xu, Y.; Jia, Q.; Guo, N.; Wang, Z.; Wang, Y. Novel greener approached synthesis of polyacrylic nanoparticles for therapy and care of gestational diabetes. Drug Deliv. 2020, 27, 1263–1270. [Google Scholar] [CrossRef]
- Du, S.; Lv, Y.; Li, N.; Huang, X.; Liu, X.; Li, H.; Wang, C.; Jia, Y.-F. Biological investigations on therapeutic effect of chitosan encapsulated nano resveratrol against gestational diabetes mellitus rats induced by streptozotocin. Drug Deliv. 2020, 27, 953–963. [Google Scholar] [CrossRef] [PubMed]
- Vafaei-Pour, Z.; Shokrzadeh, M.; Jahani, M.; Shaki, F. Embryo-Protective Effects of Cerium Oxide Nanoparticles against Gestational Diabetes in Mice. Iran. J. Pharm. Res. 2018, 17, 964–975. [Google Scholar] [PubMed]
- Alhazza, I.M.; Ebaid, H.; Omar, M.S.; Hassan, I.; Habila, M.A.; Al-Tamimi, J.; Sheikh, M. Supplementation with selenium nanoparticles alleviates diabetic nephropathy during pregnancy in the diabetic female rats. Environ. Sci. Pollut. Res. Int. 2022, 29, 5517–5525. [Google Scholar] [CrossRef] [PubMed]
- Aslesh, T.; Yokota, T. Restoring SMN Expression: An Overview of the Therapeutic Developments for the Treatment of Spinal Muscular Atrophy. Cells 2022, 11, 417. [Google Scholar] [CrossRef] [PubMed]
- Francia, V.; Schiffelers, R.M.; Cullis, P.R.; Witzigmann, D. The Biomolecular Corona of Lipid Nanoparticles for Gene Therapy. Bioconjug. Chem. 2020, 31, 2046–2059. [Google Scholar] [CrossRef]
- Liang, X.; Liu, L.; Wei, Y.Q.; Gao, G.P.; Wei, X.W. Clinical Evaluations of Toxicity and Efficacy of Nanoparticle-Mediated Gene Therapy. Hum. Gene Ther. 2018, 29, 1227–1234. [Google Scholar] [CrossRef]
- Ochiya, T.; Takahama, Y.; Baba-Toriyama, H.; Tsukamoto, M.; Yasuda, Y.; Kikuchi, H.; Terada, M. Evaluation of cationic liposome suitable for gene transfer into pregnant animals. Biochem. Biophys. Res. Commun. 1999, 258, 358–365. [Google Scholar] [CrossRef]
- Valero, L.; Alhareth, K.; Espinoza Romero, J.; Viricel, W.; Leblond, J.; Chissey, A.; Dhotel, H.; Roques, C.; Campiol Arruda, D.; Escriou, V.; et al. Liposomes as Gene Delivery Vectors for Human Placental Cells. Molecules 2018, 23, 1085. [Google Scholar] [CrossRef]
- Schwab, M.E.; MacKenzie, T.C. Prenatal Gene Therapy. Clin. Obstet. Gynecol. 2021, 64, 876–885. [Google Scholar] [CrossRef]
- Hacein-Bey-Abina, S.; Von Kalle, C.; Schmidt, M.; Le Deist, F.; Wulffraat, N.; McIntyre, E.; Radford, I.; Villeval, J.-L.; Fraser, C.C.; Cavazzana-Calvo, M.; et al. A serious adverse event after successful gene therapy for X-linked severe combined immunodeficiency. N. Engl. J. Med. 2003, 348, 255–256. [Google Scholar] [CrossRef]
- Grant, J.; Hoorens, S.; Sivadasan, S.; Loo, M.V.H.; DaVanzo, J.; Hale, L.; Butz, W. Trends in European fertility: Should Europe try to increase its fertility rate...or just manage the consequences? Int. J. Androl. 2006, 29, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Remião, M.H.; Segatto, N.V.; Pohlmann, A.; Guterres, S.S.; Seixas, F.K.; Collares, T. The Potential of Nanotechnology in Medically Assisted Reproduction. Front. Pharmacol. 2017, 8, 994. [Google Scholar] [CrossRef] [PubMed]
- Abreu, C.M.; Thomas, V.; Knaggs, P.; Bunkheila, A.; Cruz, A.; Teixeira, S.R.; Alpuim, P.; Francis, L.W.; Gebril, A.; Ibrahim, A.; et al. Non-invasive molecular assessment of human embryo development and implantation potential. Biosens. Bioelectron. 2020, 157, 112144. [Google Scholar] [CrossRef] [PubMed]
- Calsteren, K.V.; Heyns, L.; Smet, F.D.; Eycken, L.V.; Gziri, M.M.; Gemert, W.V.; Halaska, M.; Vergote, I.; Ottevanger, N.; Amant, F. Cancer during pregnancy: An analysis of 215 patients emphasizing the obstetrical and the neonatal outcomes. J. Clin. Oncol. 2010, 28, 683–689. [Google Scholar] [CrossRef] [PubMed]
- Ramaswamy, R.; Joshi, N.; Khan, M.A.; Siddhara, S. Nanosomal docetaxel lipid suspension based chemotherapy in a pregnant MBC patient—A case report. Onco Targets Ther. 2019, 12, 5679–5685. [Google Scholar] [CrossRef]
- Marmé, F.; Schneeweiss, A. Personalized therapy in breast cancer. Onkologie 2012, 35 (Suppl 1), 28–33. [Google Scholar] [CrossRef]
- Ali, S.; Albekairi, N.A.; Al-Enazy, S.; Shah, M.; Patrikeeva, S.; Nanovskaya, T.N.; Ahmed, M.S.; Rytting, E. Formulation effects on paclitaxel transfer and uptake in the human placenta. Nanomedicine 2021, 33, 102354. [Google Scholar] [CrossRef]
- Scialli, A.R.; Waterhouse, T.B.; Desesso, J.M.; Rahman, A.; Goeringer, G.C. Protective effect of liposome encapsulation on paclitaxel developmental toxicity in the rat. Teratology 1997, 56, 305–310. [Google Scholar] [CrossRef]
- Green, A.E.; Rose, P.G. Pegylated liposomal doxorubicin in ovarian cancer. Int. J. Nanomed. 2006, 1, 229–239. [Google Scholar]
- Khodaverdi, S.; Jafari, A.; Movahedzadeh, F.; Madani, F.; Yousefi Avarvand, A.; Falahatkar, S. Evaluating Inhibitory Effects of Paclitaxel and Vitamin D3 Loaded Poly Lactic Glycolic Acid Co-Delivery Nanoparticles on the Breast Cancer Cell Line. Adv. Pharm. Bull. 2020, 10, 30–38. [Google Scholar] [CrossRef]
- Refuerzo, J.S.; Alexander, J.F.; Leonard, F.; Leon, M.; Longo, M.; Godin, B. Liposomes: A nanoscale drug carrying system to prevent indomethacin passage to the fetus in a pregnant mouse model. Am. J. Obstet. Gynecol. 2015, 212, 508. [Google Scholar] [CrossRef] [PubMed]
- Yao, Y.; Zhou, Y.; Liu, L.; Xu, Y.; Chen, Q.; Wang, Y.; Wu, S.; Deng, Y.; Zhang, J.; Shao, A. Nanoparticle-Based Drug Delivery in Cancer Therapy and Its Role in Overcoming Drug Resistance. Front. Mol. Biosci. 2020, 7, 193. [Google Scholar] [CrossRef] [PubMed]
- Costa, R.L.B.; Czerniecki, B.J. Clinical development of immunotherapies for HER2+ breast cancer: A review of HER2-directed monoclonal antibodies and beyond. NPJ Breast Cancer 2020, 6, 10. [Google Scholar] [CrossRef] [PubMed]
- Tamang, S.T.; Dorji, T.; Yoezer, S.; Phuntsho, T.; Dorji, P. Knowledge and understanding of obstetric danger signs among pregnant women attending the antenatal clinic at the National Referral Hospital in Thimphu, Bhutan: A cross-sectional study. BMC Pregnancy Childbirth 2021, 21, 104. [Google Scholar] [CrossRef] [PubMed]
- Stapleton, P.A. Gestational nanomaterial exposures: Microvascular implications during pregnancy, fetal development and adulthood. J. Physiol. 2016, 594, 2161–2173. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Models | Advantages | Disadvantages |
|---|---|---|
| In vivo | ||
| Mouse models |
|
|
| Rat models | ||
| Ex vivo | ||
| Villous explants |
|
|
| Perfused placenta | ||
| In vitro | ||
| Primary cell culture |
|
|
| Cell lines |
|
|
| Placenta-on-a-chip model |
|
|
| Co-colture |
|
|
| Organoids |
|
|
| Types of Nanoparticles | Examples |
|---|---|
| Inorganic | Silver nanoparticles; gold nanoparticles; superparamagnetic iron oxide nanoparticles; cobalt and chromium nanoparticles; cadmium telluride nanoparticles; copper oxide nanoparticles; titanium dioxide nanoparticles; silicon dioxide; silica nanoparticles; zinc oxide nanoparticles; zirconium dioxide nanoparticles. |
| Organic | Dexamethasone-loaded polymeric nanoparticles; polyamidoamine dendrimers; polystyrene nanoparticles; carboxylate modified polystyrene nanoparticles; polyethylene glycol coated liposomes; polylactic-co-glycolic acid nanoparticles; fullerenes; liposomes nanoparticles; engineered exosomes. |
| Hybrid | Antibody conjugated with magnetic nanoparticles;liposomal gadolinium; superparamagnetic iron oxide nanoparticle; zinc oxide resveratrol encapsulated in Chitosan. |
| Topic | Open Question |
|---|---|
| Diagnostic |
|
| Placental models |
|
| Pathology models |
|
| Treatment |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bertozzi, S.; Corradetti, B.; Seriau, L.; Diaz Ñañez, J.A.; Cedolini, C.; Fruscalzo, A.; Cesselli, D.; Cagnacci, A.; Londero, A.P. Nanotechnologies in Obstetrics and Cancer during Pregnancy: A Narrative Review. J. Pers. Med. 2022, 12, 1324. https://doi.org/10.3390/jpm12081324
Bertozzi S, Corradetti B, Seriau L, Diaz Ñañez JA, Cedolini C, Fruscalzo A, Cesselli D, Cagnacci A, Londero AP. Nanotechnologies in Obstetrics and Cancer during Pregnancy: A Narrative Review. Journal of Personalized Medicine. 2022; 12(8):1324. https://doi.org/10.3390/jpm12081324
Chicago/Turabian StyleBertozzi, Serena, Bruna Corradetti, Luca Seriau, José Andrés Diaz Ñañez, Carla Cedolini, Arrigo Fruscalzo, Daniela Cesselli, Angelo Cagnacci, and Ambrogio P. Londero. 2022. "Nanotechnologies in Obstetrics and Cancer during Pregnancy: A Narrative Review" Journal of Personalized Medicine 12, no. 8: 1324. https://doi.org/10.3390/jpm12081324