
Pepsin and the Lung—Exploring the Relationship between Micro-Aspiration and Respiratory Manifestations of Gastroesophageal Reflux Disease

 ,
,  ,
,
Abstract
:1. Introduction
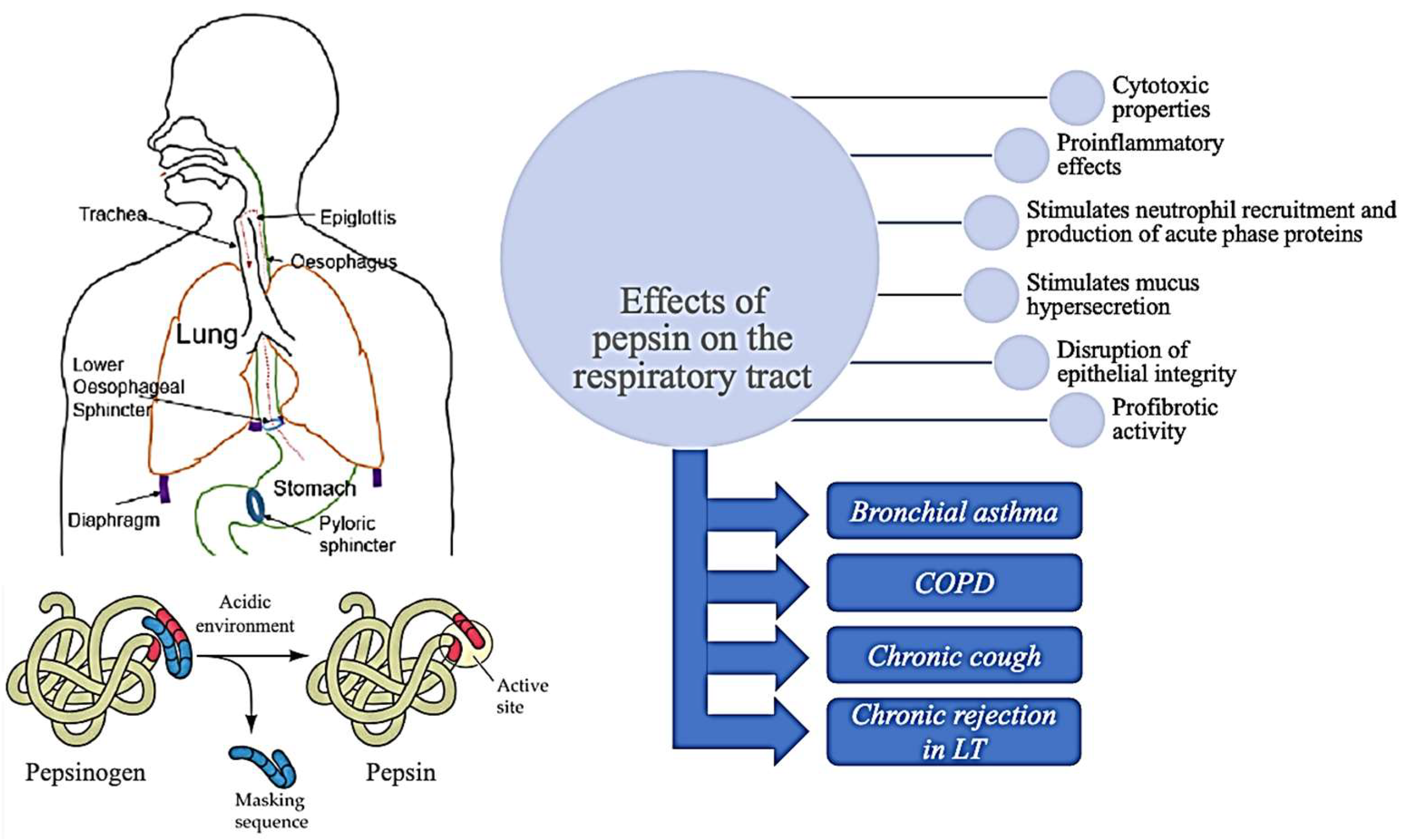
2. Effects of Pepsin on the Airways
3. Pepsin Detection in Bronchial Asthma
4. Pepsin Detection in COPD
5. Pepsin Detection in Chronic Cough
6. Pepsin Detection in Lung Transplant Patients
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dirac, M.A.; Safiri, S.; Tsoi, D.; Adedoyin, R.A.; Afshin, A.; Akhlaghi, N.; Alahdab, F.; Almulhim, A.M.; Amini, S.; Ausloos, F.; et al. The Global, Regional, and National Burden of Gastro-Oesophageal Reflux Disease in 195 Countries and Territories, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol. Hepatol. 2020, 5, 561–581. [Google Scholar] [CrossRef] [Green Version]
- Yamasaki, T.; Hemond, C.; Eisa, M.; Ganocy, S.; Fass, R. The Changing Epidemiology of Gastroesophageal Reflux Disease: Are Patients Getting Younger? J. Neurogastroenterol. Motil. 2018, 24, 559–569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vakil, N.; Van Zanten, S.V.; Kahrilas, P.; Dent, J.; Jones, R.; Bianchi, L.K.; Cesario, K.B. The Montreal Definition and Classification of Gastroesophageal Reflux Disease: A Global Evidence-Based Consensus. Am. J. Gastroenterol. 2006, 101, 1900–1920. [Google Scholar] [CrossRef] [PubMed]
- Broers, C.; Tack, J.; Pauwels, A. Review Article: Gastro-Oesophageal Reflux Disease in Asthma and Chronic Obstructive Pulmonary Disease. Aliment. Pharmacol. Ther. 2018, 47, 176–191. [Google Scholar] [CrossRef] [Green Version]
- Tack, J.; Pandolfino, J.E. Pathophysiology of Gastroesophageal Reflux Disease. Gastroenterology 2018, 154, 277–288. [Google Scholar] [CrossRef]
- Durazzo, M.; Lupi, G.; Cicerchia, F.; Ferro, A.; Barutta, F.; Beccuti, G.; Gruden, G.; Pellicano, R. Extra-Esophageal Presentation of Gastroesophageal Reflux Disease: 2020 Update. J. Clin. Med. 2020, 9, 2559. [Google Scholar] [CrossRef]
- Abdallah, A.F.; El-Desoky, T.; Fathi, K.; Elkashef, W.F.; Zaki, A. Clinical Utility of Bronchoalveolar Lavage Pepsin in Diagnosis of Gastroesophageal Reflux among Wheezy Infants. Can. Respir. J. 2016, 2016, 9480843. [Google Scholar] [CrossRef] [Green Version]
- Rao, Y.F.; Wang, J.; Cheng, D.N.; Xu, Y.; Ren, X.; Yang, W.; Liu, G.; Xu, W.; Yan, X.H.; Song, Y.; et al. The Controversy of Pepsinogen A/Pepsin A in Detecting Extra-Gastroesophageal Reflux. J. Voice, 2021, in press. [CrossRef]
- Bathoorn, E.; Daly, P.; Gaiser, B.; Sternad, K.; Poland, C.; MacNee, W.; Drost, E.M. Cytotoxicity and Induction of Inflammation by Pepsin in Acid in Bronchial Epithelial Cells. Int. J. Inflam. 2011, 2011, 569416. [Google Scholar] [CrossRef] [Green Version]
- Hunt, E.B.; Sullivan, A.; Galvin, J.; MacSharry, J.; Murphy, D.M. Gastric Aspiration and Its Role in Airway Inflammation. Open Respir. Med. J. 2018, 12, 1–10. [Google Scholar] [CrossRef]
- Hurley, B.P.; Jugo, R.H.; Snow, R.F.; Samuels, T.L.; Yonker, L.M.; Mou, H.; Johnston, N.; Rosen, R. Pepsin Triggers Neutrophil Migration Across Acid Damaged Lung Epithelium. Sci. Rep. 2019, 9, 13778. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.; Chen, H.Y.; Cheng, Y.; Wei, Y.; Zhou, X.M.; Li, T.; Zhu, J.P.; Wang, Q. Gastric Acid and Pepsin Work Together in Simulated Gastric Acid Inhalation Leading to Pulmonary Fibrosis in Rats. Med. Sci. Monit. 2019, 25, 6153–6164. [Google Scholar] [CrossRef] [PubMed]
- Knight, P.R.; Davidson, B.A.; Nader, N.D.; Helinski, J.D.; Marschke, C.J.; Russo, T.A.; Hutson, A.D.; Notter, R.H.; Holm, B.A. Progressive, Severe Lung Injury Secondary to the Interaction of Insults in Gastric Aspiration. Exp. Lung Res. 2004, 30, 535–557. [Google Scholar] [CrossRef] [PubMed]
- Smith, W.B.; Gamble, J.R.; Clark-Lewis, I.; Vadas, M.A. Interleukin-8 Induces Neutrophil Transendothelial Migration. Immunology 1991, 72, 65–72. [Google Scholar] [PubMed]
- Shanley, T.P.; Vasi, N.; Davidson, B.A.; Nader, N.D.; Knight, P.R.; Bless, N.; Ward, P.A.; Johnson, K.J. Role of Macrophage Inflammatory Protein-2 in Aspiration-Induced Lung Injury. Crit. Care Med. 2000, 28, 2437–2444. [Google Scholar] [CrossRef]
- Sacco, O.; Silvestri, M.; Sabatini, F.; Sale, R.; Moscato, G.; Pignatti, P.; Mattioli, G.; Rossi, G.A. IL-8 and Airway Neutrophilia in Children with Gastroesophageal Reflux and Asthma-like Symptoms. Respir. Med. 2006, 100, 307–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samareh Fekri, M.; Poursalehi, H.R.; Najafipour, H.; Dabiri, S.; Shokoohi, M.; Siahposht Khacheki, A.; Shahrokhi, N.; Malekpour Afshar, R.; Lashkarizadeh, M.R. Pulmonary Complications of Gastric Fluid and Bile Salts Aspiration, an Experimental Study in Rat. Iran. J. Basic Med. Sci. 2013, 16, 790–796. [Google Scholar] [CrossRef]
- Mertens, V.; Blondeau, K.; Vanaudenaerde, B.; Vos, R.; Farre, R.; Pauwels, A.; Verleden, G.; Van Raemdonck, D.; Dupont, L.; Sifrim, D. Gastric Juice from Patients “On” Acid Suppressive Therapy Can Still Provoke a Significant Inflammatory Reaction by Human Bronchial Epithelial Cells. Dysphagia 2011, 26, 331. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.S.; Na, H.G.; Bae, C.H.; Song, S.Y.; Kim, Y.D. Pepsin Exposure in a Non-Acidic Environment Upregulates Mucin 5AC (MUC5AC) Expression via Matrix Metalloproteinase 9 (MMP9)/Nuclear Factor ΚB (NF-ΚB) in Human Airway Epithelial Cells. Int. Forum Allergy Rhinol. 2021, 11, 894–901. [Google Scholar] [CrossRef]
- Emilsson, Ö.I.; Benediktsdóttir, B.; Ólafsson, Í.; Cook, E.; Júlíusson, S.; Björnsson, E.S.; Gulaugsdóttir, S.; Gumundsdóttir, A.S.; Mirgorodskaya, E.; Ljungström, E.; et al. Respiratory Symptoms, Sleep-Disordered Breathing and Biomarkers in Nocturnal Gastroesophageal Reflux. Respir. Res. 2016, 17, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Liang, B.; Yi, Q.; Feng, Y. Association of Gastroesophageal Reflux Disease with Asthma Control. Dis. Esophagus 2013, 26, 794–798. [Google Scholar] [CrossRef]
- Kwiecien, J.; MacHura, E.; Halkiewicz, F.; Karpe, J. Clinical Features of Asthma in Children Differ with Regard to the Intensity of Distal Gastroesophageal Acid Reflux. J. Asthma 2011, 48, 366–373. [Google Scholar] [CrossRef] [PubMed]
- Kiljander, T.O.; Junghard, O.; Beckman, O.; Lind, T. Effect of Esomeprazole 40 Mg Once or Twice Daily on Asthma: A Randomized, Placebo-Controlled Study. Am. J. Respir. Crit. Care Med. 2010, 181, 1042–1048. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Z.; Luo, Y.; Li, J.; Gao, J. Randomised Trials of Proton Pump Inhibitors for Gastro-Oesophageal Reflux Disease in Patients with Asthma: An Updated Systematic Review and Meta-Analysis. BMJ Open 2021, 11, e043860. [Google Scholar] [CrossRef] [PubMed]
- Timms, C.; Thomas, P.S.; Yates, D.H. Detection of Gastro-Oesophageal Reflux Disease ({GORD}) in Patients with Obstructive Lung Disease Using Exhaled Breath Profiling. J. Breath Res. 2012, 6, 16003. [Google Scholar] [CrossRef]
- Marshall, S.; McCann, A.J.; Samuels, T.L.; Blair, A.; Bonne, V.; Johnston, N.; Koufman, J. Detection of Pepsin and IL-8 in Saliva of Adult Asthmatic Patients. J. Asthma Allergy 2019, 12, 155–161. [Google Scholar] [CrossRef] [Green Version]
- Rosen, R.; Johnston, N.; Hart, K.; Khatwa, U.; Nurko, S. The Presence of Pepsin in the Lung and Its Relationship to Pathologic Gastroesophageal Reflux. Neurogastroenterol. Motil. 2012, 24, 129-e85. [Google Scholar] [CrossRef] [Green Version]
- Hunt, E.B.; Ward, C.; Power, S.; Sullivan, A.; Pearson, J.P.; Lapthorne, S.; O’Byrne, P.M.; Eustace, J.; Plant, B.J.; Maher, M.M.; et al. The Potential Role of Aspiration in the Asthmatic Airway. Chest 2017, 151, 1272–1278. [Google Scholar] [CrossRef] [Green Version]
- Soyer, T.; Soyer, Ö.U.; Birben, E.; Kisa, Ü.; Kalayci, Ö.; Çakmak, M. Pepsin Levels and Oxidative Stress Markers in Exhaled Breath Condensate of Patients with Gastroesophageal Reflux Disease. J. Pediatr. Surg. 2013, 48, 2247–2250. [Google Scholar] [CrossRef]
- Takada, K.; Matsumoto, S.; Kojima, E.; Iwata, S.; Okachi, S.; Ninomiya, K.; Morioka, H.; Tanaka, K.; Enomoto, Y. Prospective Evaluation of the Relationship between Acute Exacerbations of COPD and Gastroesophageal Reflux Disease Diagnosed by Questionnaire. Respir. Med. 2011, 105, 1531–1536. [Google Scholar] [CrossRef] [Green Version]
- Hurst, J.R.; Vestbo, J.; Anzueto, A.; Locantore, N.; Müllerova, H.; Tal-Singer, R.; Miller, B.; Lomas, D.A.; Agusti, A.; MacNee, W.; et al. Susceptibility to Exacerbation in Chronic Obstructive Pulmonary Disease. N. Engl. J. Med. 2010, 363, 1128–1138. [Google Scholar] [CrossRef] [Green Version]
- Rascon-Aguilar, I.E.; Pamer, M.; Wludyka, P.; Cury, J.; Coultas, D.; Lambiase, L.R.; Nahman, N.S.; Vega, K.J. Role of Gastroesophageal Reflux Symptoms in Exacerbations of COPD. Chest 2006, 130, 1096–1101. [Google Scholar] [CrossRef] [PubMed]
- Liang, B.; Wang, M.; Yi, Q.; Feng, Y. Association of Gastroesophageal Reflux Disease Risk with Exacerbations of Chronic Obstructive Pulmonary Disease. Dis. Esophagus 2013, 26, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Rogha, M.; Behravesh, B.; Pourmoghaddas, Z. Association of Gastroesophageal Reflux Disease Symptoms with Exacerbations of Chronic Obstructive Pulmonary Disease. J. Gastrointestin Liver Dis. 2010, 19, 253–256. [Google Scholar]
- Pomari, C.; Mauroner, L.; Paiano, S.; Assante, L.R.; Bertolaccini, L.; Ruffo, G.; Mainardi, P.; Bocus, P.; Geccherle, A.; Albanese, S.I.; et al. Bronchial Reacutization and Gastroesophageal Reflux: Is There a Potential Clinical Correlation? Ann. Transl. Med. 2016, 4, 304. [Google Scholar] [CrossRef] [Green Version]
- Hashemi-Bajgani, S.M.; Abbasi, F.; Shafahi, A.; Yazdani, R.; Fekri, M.S. Association of Bile Acid and Pepsin Micro-Aspiration with Chronic Obstructive Pulmonary Disease Exacerbation. Tanaffos 2019, 18, 52–57. [Google Scholar]
- Starosta, V.; Kitz, R.; Hartl, D.; Marcos, V.; Reinhardt, D.; Griese, M. Bronchoalveolar Pepsin, Bile Acids, Oxidation, and Inflammation in Children with Gastroesophageal Reflux Disease. Chest 2007, 132, 1557–1564. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.L.; Button, B.M.; Denehy, L.; Roberts, S.J.; Bamford, T.L.; Ellis, S.J.; Mu, F.T.; Heine, R.G.; Stirling, R.G.; Wilson, J.W. Proximal and Distal Gastro-Oesophageal Reflux in Chronic Obstructive Pulmonary Disease and Bronchiectasis. Respirology 2014, 19, 211–217. [Google Scholar] [CrossRef]
- Lee, A.; Button, B.; Denehy, L.; Roberts, S.; Bamford, T.; Mu, F.-T.; Mifsud, N.; Stirling, R.; Wilson, J.W. Exhaled Breath Condensate Pepsin: Potential Noninvasive Test for Gastroesophageal Reflux in COPD and Bronchiectasis. Respir. Care 2015, 60, 244–250. [Google Scholar] [CrossRef] [Green Version]
- Smith, J.A.; Decalmer, S.; Kelsall, A.; McGuinness, K.; Jones, H.; Galloway, S.; Woodcock, A.; Houghton, L.A. Acoustic Cough-Reflux Associations in Chronic Cough: Potential Triggers and Mechanisms. Gastroenterology 2010, 139, 754–762. [Google Scholar] [CrossRef]
- Decalmer, S.; Stovold, R.; Houghton, L.A.; Pearson, J.; Ward, C.; Kelsall, A.; Jones, H.; McGuinness, K.; Woodcock, A.; Smith, J.A. Chronic Cough: Relationship between Microaspiration, Gastroesophageal Reflux, and Cough Frequency. Chest 2012, 142, 958–964. [Google Scholar] [CrossRef]
- Grabowski, M.; Kasran, A.; Seys, S.; Pauwels, A.; Medrala, W.; Dupont, L.; Panaszek, B.; Bullens, D. Pepsin and Bile Acids in Induced Sputum of Chronic Cough Patients. Respir. Med. 2011, 105, 1257–1261. [Google Scholar] [CrossRef] [PubMed]
- Dy, F.; Amirault, J.; Mitchell, P.D.; Rosen, R. Salivary Pepsin Lacks Sensitivity as a Diagnostic Tool to Evaluate Extraesophageal Reflux Disease. J. Pediatr. 2016, 177, 53–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farrell, S.; McMaster, C.; Gibson, D.; Shields, M.D.; McCallion, W.A. Pepsin in Bronchoalveolar Lavage Fluid: A Specific and Sensitive Method of Diagnosing Gastro-Oesophageal Reflux-Related Pulmonary Aspiration. J. Pediatric Surg. 2006, 41, 289–293. [Google Scholar] [CrossRef] [PubMed]
- Strugala, V.; Woodcock, A.D.; Dettmar, P.W.; Faruqi, S.; Morice, A.H. Detection of Pepsin in Sputum: A Rapid and Objective Measure of Airways Reflux. Eur. Respir. J. 2016, 47, 339–341. [Google Scholar] [CrossRef] [Green Version]
- Chang, A.B.; Oppenheimer, J.; Weinberger, M.; Grant, C.C.; Rubin, B.; Irwin, R.S.; Altman, K.W.; Azoulay, E.; Barker, A.F.; Birring, S.S.; et al. Etiologies of Chronic Cough in Pediatric Cohorts: CHEST Guideline and Expert Panel Report. Chest 2017, 152, 607–617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, C.N.; Barnawi, Z.; Chorvinsky, E.; Pillai, D.; Gatti, M.; Collins, M.E.; Krakovsky, G.M.; Bauman, N.M.; Sehgal, S.; Pillai, D.K. Positive Bronchoalveolar Lavage Pepsin Assay Associated with Viral and Fungal Respiratory Infections in Children with Chronic Cough. Pediatr. Pulmonol. 2021, 56, 2686–2694. [Google Scholar] [CrossRef]
- Blondeau, K.; Mertens, V.; Vanaudenaerde, B.A.; Verleden, G.M.; Van Raemdonck, D.E.; Sifrim, D.; Dupont, L.J. Gastro-Oesophageal Reflux and Gastric Aspiration in Lung Transplant Patients with or without Chronic Rejection. Eur. Respir. J. 2008, 31, 707–713. [Google Scholar] [CrossRef] [Green Version]
- Fisichella, M.; Davis, C.S.; Lundberg, P.W.; Lowery, E.; Burnham, E.L.; Alex, C.G.; Ramirez, L.; Pelletiere, K.; Love, R.B.; Kuo, P.C.; et al. The Protective Role of Laparoscopic Antireflux Surgery against Aspiration of Pepsin after Lung Transplantation. Surgery 2011, 150, 598–606. [Google Scholar] [CrossRef] [Green Version]
- Fisichella, M.; Davis, C.S.; Lowery, E.; Ramirez, L.; Gamelli, R.L.; Kovacs, E.J. Aspiration, Localized Pulmonary Inflammation, and Predictors of Early-Onset Bronchiolitis Obliterans Syndrome after Lung Transplantation. J. Am. Coll. Surg. 2013, 217, 90–101. [Google Scholar] [CrossRef] [Green Version]
- Griffin, S.M.; Robertson, A.G.N.; Bredenoord, A.J.; Brownlee, I.A.; Stovold, R.; Brodlie, M.; Forrest, I.; Dark, J.H.; Pearson, J.P.; Ward, C. Aspiration and Allograft Injury Secondary to Gastroesophageal Reflux Occur in the Immediate Post-Lung Transplantation Period (Prospective Clinical Trial). Ann. Surg. 2013, 258, 705–712. [Google Scholar] [CrossRef]
- Reder, N.P.; Davis, C.S.; Kovacs, E.J.; Fisichella, P.M. The Diagnostic Value of Gastroesophageal Reflux Disease (GERD) Symptoms and Detection of Pepsin and Bile Acids in Bronchoalveolar Lavage Fluid and Exhaled Breath Condensate for Identifying Lung Transplantation Patients with GERD-Induced Aspiration. Surg. Endosc. 2014, 28, 1794–1800. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Subjects | Age Range | Pepsin Method of Detection and Values | Conclusions | |
|---|---|---|---|---|
| Abdallah et al. (2016) [7] | Wheezy infants and healthy controls | 3–24 months | BAL fluid pepsin was measured using the Human Pepsin enzyme-linked immunosorbent assay Kit of Glory Science Co., Ltd.:
| BAL fluid pepsin was positive both in wheezy infants and in healthy controls. The relationship between GERD standard diagnostic tests and BAL fluid pepsin did not reach statistical significance. BAL fluid pepsin showed a statistically significant positive correlation with the mean acid clearance time and the duration of the longest acid episode in infants older than one year. |
| Emilsson et al. (2016) [20] | Patients with nocturnal GERD (nGERD) and age and gender-matched controls | GERD patients: 55.8 ± 6.7 years No GERD: 56.4 ± 7.0 years | Pepsin measured in EBC by ELISA (Wuhan EIAAB Science Co., Ltd., Wuhan, China).
| Bronchial asthma and bronchitis symptoms, as well as respiratory exacerbations, were associated with nGERD. Pepsin levels were significantly higher in nGERD patients compared to controls (p = 0.03). |
| Timms et al. (2012) [25] | Bronchial asthma and COPD patients and healthy controls | Between 38.00 ± 6.34 years in asthma patients and 70.63 ± 3.391 years in COPD patients | Pepsin measured in EBC by using an in-house quantitative ELISA based on a monospecific antibody to porcine pepsin.
| Participants with obstructive lung disease and GERD had significantly higher levels of pepsin compared to those without GERD (p < 0.002) and healthy controls (p = < 0.013). COPD group with GERD had a significantly higher median pepsin concentration than the COPD control group (p = 0.0175). Patients with asthma and GERD had a higher mean pepsin concentration compared to the asthma control group but without reaching statistical significance. |
| Marshall et al. (2019) [26] | Bronchial asthma patients | 58.7 ± 11.3 years | Pepsin was measured in three saliva samples (a throat-clearing saliva sample provided during a routine clinic visit, half of which was mixed with citric acid, and another sample upon waking, prior to brushing their teeth, drinking or eating in the morning the day after their clinic visit) by non-competitive indirect sandwich ELISA:
| No significant associations were found between pepsin and clinical measures of asthma severity. |
| Rosen et al. (2012) [27] | Bronchial asthma and chronic cough paediatric patients | 67 ± 43 months | Pepsin was analysed in BAL fluid by ELISA using rabbit anti-pepsin antibody diluted and mouse anti-b-actin antibody (CP01, EMD Chemicals, Gibbstown, NJ, USA):
| A significantly higher mean lipid-laden macrophage index was found in patients that were pepsin positive compared to pepsin-negative patients (81 ± 54 vs. 47 ± 26, p = 0.001). |
| Hunt et al. (2017) [28] | Bronchial asthma patients | BAL fluid pepsin was analysed by using a locally developed indirect ELISA—the primary antibody was specific to porcine pepsin (Biodesign International Cat no W59117G), and the secondary antibody was horse radish peroxidase-conjugated rabbit, anti-goat (Sigma):
| No significant associations between pepsin level and measures of disease severity asthma control, FEV1, ACQ or exacerbation frequency. | |
| Soyer et al. (2013) [29] | Paediatric patients with a presumptive diagnosis of GERD with recurrent respiratory and/or gastrointestinal problems | 2–14 years | Pepsin concentrations in EBC specimens were analysed by using homemade indirect ELISA. Concentrations were below the level of detection. | A more sensitive ELISA with a lower threshold of detection may be useful in order to investigate pepsin levels in paediatric populations. |
| Subjects | Age Range | Pepsin Method of Detection and Values | Conclusions | ||
|---|---|---|---|---|---|
| Pomari et al. (2016) [35] | Patients with a history of a chronic cough, plug or dyspnea and abnormal lung examination enrolled for the worsening of respiratory symptoms in spite of regular treatment | 20–84 years | Semiquantitative assessment of BAL fluid pepsin using Pep-test (PeptestTM, RD Biomed Ltd., Cottingham, UK).
| A strong positive statistical correlation was found between pepsin detection in bronchial secretions and radiological signs of GERD and GERD diagnosis. | |
| Hashemi-Bajgani et al. (2019) [36] | COPD patients with and without exacerbations | COPD group with exacerbation history: 60.88 ± 8.10 years COPD group without exacerbation history: 60.15 ± 9.53 years | BAL fluid pepsin was measured using the standard pepsin kit (ELISA Kit for pepsin) from the USCNK Company.
| No association was found between disease severity and the number of exacerbations with micro-aspiration of pepsin. | |
| Starosta et al. (2007) [37] | Paediatric patients with chronic bronchitis, allergic asthma, recurrent pneumonia, bronchiectasis, tracheomalacia, primary ciliary dyskinesia and bronchiolitis obliterans | 4.7 (3.3–7.5) years | Levels of pepsin in BAL fluid were determined by using a modification of the proteolytic enzyme assay method. | The average concentration of pepsin was higher in the group with extensive proximal acidic gastroesophageal reflux index than in children with reflux index < 2% (p < 0.037). Pepsin in BAL fluid of this paediatric group with chronic respiratory symptoms correlated positively with the number of proximal reflux events; however, it does not differentiate patients with reflux from those without. | |
| Lee et al. (2014) [38] | Patients with COPD or bronchiectasis and healthy controls | COPD group: 67.7 ± 7.7 years Bronchiectasis group: 53.7 ± 14.0 years Controls: 36.6 ± 15.1 years | Pepsin levels in sputum samples were analysed using a locally developed ELISA based on a monospecific antibody to porcine pepsin. Samples were collected at four intervals over 24 h: upon waking, mid-morning, mid-afternoon and prior to sleeping (prior to or 1 h after meals).
| Pepsin in sputum was not related to a diagnosis of GERD. Neither a diagnosis of GERD nor the presence of pepsin in sputum was associated with reduced lung function in COPD or bronchiectasis. | |
| Lee et al. (2015) [39] | Patients with COPD or bronchiectasis and healthy controls | COPD group: 58–74 years Bronchiectasis group: 52–69 years Controls: 26–72 years | EBC pepsin concentrations were measured using a locally developed ELISA based on a monospecific antibody to porcine pepsin.
| A diagnosis of GERD was not associated with a higher concentration of EBC pepsin in bronchiectasis or COPD. | |
| Subjects | Age Range | Pepsin Method of Detection and Values | Conclusions | |
|---|---|---|---|---|
| Decalmer et al. (2012) [41] | Chronic cough patients and healthy controls | Chronic cough group: 55.8 ± 11.0 years Healthy controls: 30–50.8 years | Pepsin was measured in BAL fluid and induced sputum using a plate ELISA based on a monospecific antibody to porcine pepsin.
| Log cough frequency was inversely related to sputum pepsin concentration: subjects with higher cough frequency had lower sputum pepsin concentrations. Therefore, coughing appears to be protective, reducing pepsin concentration in the larger airways of patients with chronic cough. |
| Grabowski et al. (2011) [42] | Chronic cough patients and healthy controls | Chronic cough group: 21–75 years Healthy controls: 24–66 years | Pepsin levels in induced sputum were measured by ELISA kit (USCN Life Science Inc. Wuhan, China).
| In pepsin-positive samples, no significant difference in pepsin concentration could be found between chronic cough patients and the healthy control group. |
| Dy et al. (2016) [43] | Paediatric patients undergoing testing for the evaluation of GERD | 1–19 years | Random saliva samples were collected for pepsin testing. For subjects who were unable to produce a salivary sample, an oropharyngeal saliva aspirate was obtained. All samples were obtained after fasting for at least 2 h. Saliva specimens were analyzed using the PepTest (RD BioMed, Hull UK).
| No significant difference between the pepsin-positive and pepsin-negative groups in terms of distribution of acid, nonacid, total reflux episodes, full column reflux or any other reflux variable. There was no significant correlation between the number of reflux episodes and pepsin concentrations. |
| Farrell et al. (2006) [44] | Children undergoing general anaesthesia as part of their investigations for symptoms of GERD. Positive control group: intubated children with proven macroscopic aspiration. Negative control group—children with no history of GERD or respiratory disease undergoing general anaesthesia for elective surgery. | < 14 years | A BAL fluid pepsin assay was developed based on a sandwich ELISA principle using 2 primary antiporcine pepsin antibodies.
| Pepsin concentrations in the BAL fluid of children with proximal oesophageal GERD were significantly higher in subjects with chronic cough compared to negative controls. No such difference was observed between participants with proximal GERD without cough and negative controls. |
| Strugala et al. (2015) [45] | Chronic cough patients and a previously investigated healthy volunteer population | Chronic cough group: 58.4 ± 13.8 years | Patients were instructed to provide three expectorated saliva/sputum samples during daily activities and immediately after three spontaneous coughing episodes. Pepsin levels were assessed using Peptest (RD Biomed Ltd., Cottingham, UK). | Chronic cough patients had a significantly higher prevalence of pepsin detection (p < 0.0001) and increased pepsin concentration compared to the control group. |
| Martin et al. (2021) [47] | Children undergoing flexible bronchoscopy and bronchoalveolar lavage | 4.9 (2.2–9.1) years | BAL fluid pepsin was assessed by enzyme-linked immunosorbent gastric pepsin A assay. | No demographic characteristic of our patient population was significantly associated with pepsin positivity. Pepsin-positive groups did not have more severe respiratory symptoms. No significant difference in pulmonary function testing was observed between the two groups. No correlation was found between pepsin detection and pH-impedance or esophago-gastro-duodenoscopy findings. A significant association was observed between pepsin positivity and viral PCR, hinting at the possibility of cough-induced reflux. |
| Subjects | Age Range | Pepsin Method of Detection and Values | Conclusions | |
|---|---|---|---|---|
| Blondeau et al. (2008) [48] | Lung transplant recipients BAL fluid samples were collected from non-transplant subjects requiring a bronchoscopy as controls | 52 (19–69) years | Pepsin was measured using an ELISA using a primary polyclonal antibody to porcine pepsin and goat immunoglobulin G as a secondary antibody.
| Gastric aspiration occurred frequently after lung transplantation, as shown by the presence of pepsin in BAL fluid specimens retrieved from all transplanted patients. Patients with bronchiolitis obliterans syndrome did not have increased GERD and did not have a particularly higher concentration of pepsin in BAL fluid. An increased prevalence of reflux could not be found in these patients compared to stable transplant recipients. No significant correlation was found between reflux and FEV1. |
| Fisichella et al. (2011) [49] | Lung transplant recipients (divided into GERD positive and negative) and healthy controls | BAL fluid pepsin levels were measured by a locally developed ELISA in the laboratories at the Burn and Shock Trauma Institute at Loyola University Medical Center using a monospecific antibody to porcine pepsin (Calbio-chem/EMD4Biosciences, Gibbstown, NJ, USA).
| Subjects with any detectable pepsin concentrations had a quicker progression to bronchiolitis obliterans syndrome than patients with undetectable pepsin (p = 0.058) Greater levels of pepsin were associated with worse episodes of rejection. | |
| Fisichella et al. (2013) [50] | Lung transplant recipients (divided into bronchiolitis obliterans syndrome positive and negative) | 59 years (IQR 50–62 years) | BAL fluid pepsin levels were measured by a locally developed ELISA in the laboratories at the Burn and Shock Trauma Institute at Loyola University Medical Center using a monospecific antibody to porcine pepsin (Calbio-chem/EMD4Biosciences, Gibbstown, NJ, USA).
| Detectable pepsin concentrations in BAL fluid samples from lung transplant recipients were associated with significantly increased neutrophilia and reduced concentrations of IL-12, which was associated with more severe acute cellular rejection. |
| Griffin et al. (2013) [51] | Lung transplant recipients within the first month post-transplantation A reference stable control range was established in 7 optimally stable patients independent of the study cohort. | 22–59 years | An in-house, indirect pepsin ELISA with a specific antipepsin antibody and an antisheep/goat secondary antibody was used to evaluate BAL fluid pepsin levels.
| Aspiration and allograft injury may occur in the early posttransplant period. |
| Reder et al. (2014) [52] | Lung transplant recipients | 54.4 ± 12.9 years | Pepsin concentrations were measured by ELISA using a monoclonal antibody to porcine pepsin as described by the manufacturer (Biodesign International, Saco, ME, USA). EBC and BAL fluid specimens were retrieved during routine follow-up visits.
| Typical symptoms of GERD did not predict the presence or absence of pepsin in BAL. Symptoms such as aspiration and bronchitis had greater predictive value. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iov, D.-E.; Bărboi, O.-B.; Floria, M.; Neamțu, A.; Iliescu, R.; Drug, V.-L. Pepsin and the Lung—Exploring the Relationship between Micro-Aspiration and Respiratory Manifestations of Gastroesophageal Reflux Disease. J. Pers. Med. 2022, 12, 1296. https://doi.org/10.3390/jpm12081296
Iov D-E, Bărboi O-B, Floria M, Neamțu A, Iliescu R, Drug V-L. Pepsin and the Lung—Exploring the Relationship between Micro-Aspiration and Respiratory Manifestations of Gastroesophageal Reflux Disease. Journal of Personalized Medicine. 2022; 12(8):1296. https://doi.org/10.3390/jpm12081296
Chicago/Turabian StyleIov, Diana-Elena, Oana-Bogdana Bărboi, Mariana Floria, Andrei Neamțu, Radu Iliescu, and Vasile-Liviu Drug. 2022. "Pepsin and the Lung—Exploring the Relationship between Micro-Aspiration and Respiratory Manifestations of Gastroesophageal Reflux Disease" Journal of Personalized Medicine 12, no. 8: 1296. https://doi.org/10.3390/jpm12081296