
Prevalence of Physical Health, Mental Health, and Disability Comorbidities among Women Living with HIV in Canada

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Characteristics of Participants
3.2. Lifetime Prevalence of Physical Health Diagnoses Overall and by Gender Identity
3.3. Prevalence of Mental Health Diagnoses Currently Living with Overall and by Gender Identity
3.4. Disabilities Overall and by Gender Identity
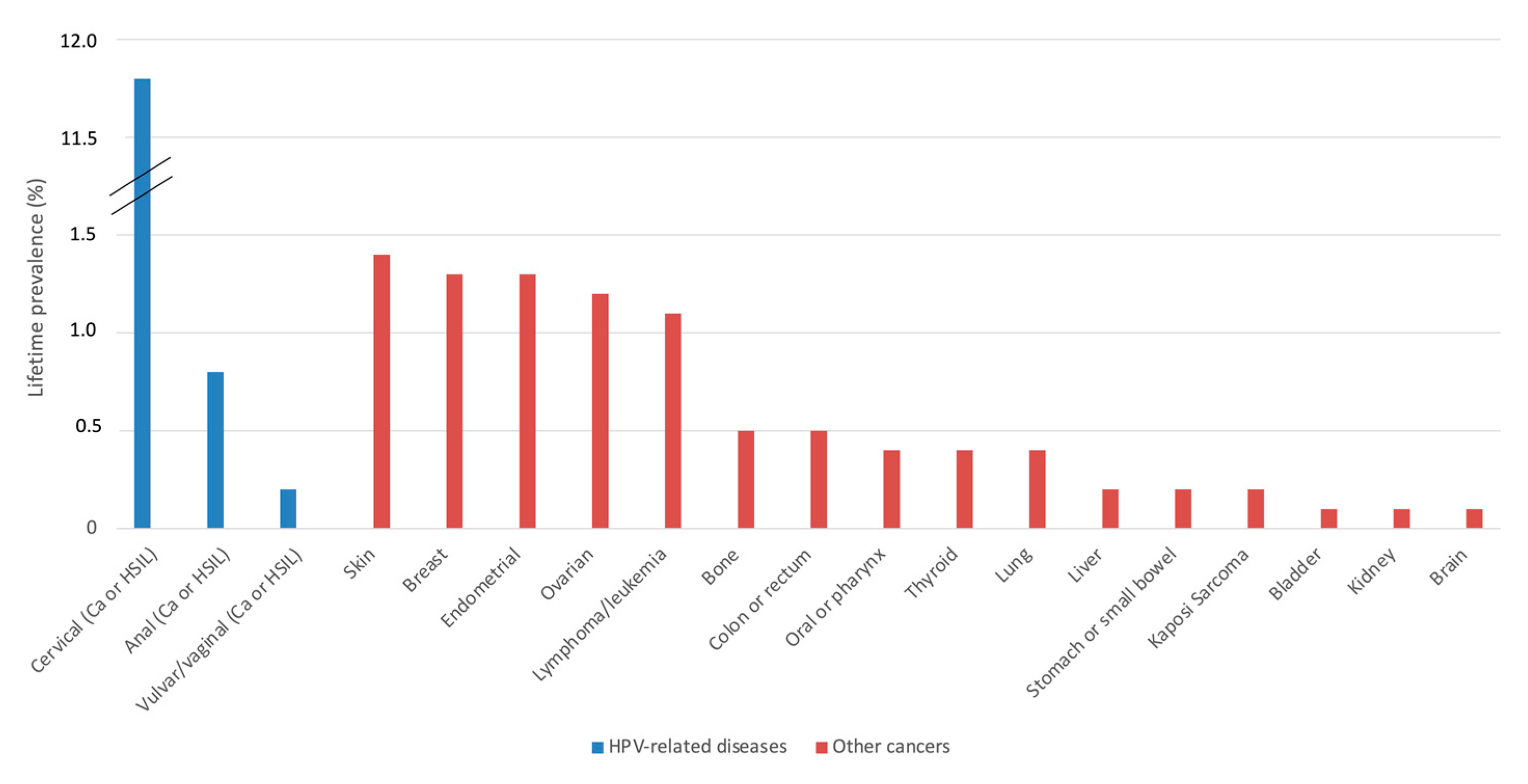
3.5. Cancers or Precancers Overall
3.6. Physical, Mental Health Conditions and Disabilities Stratified by Ethnicity and Age
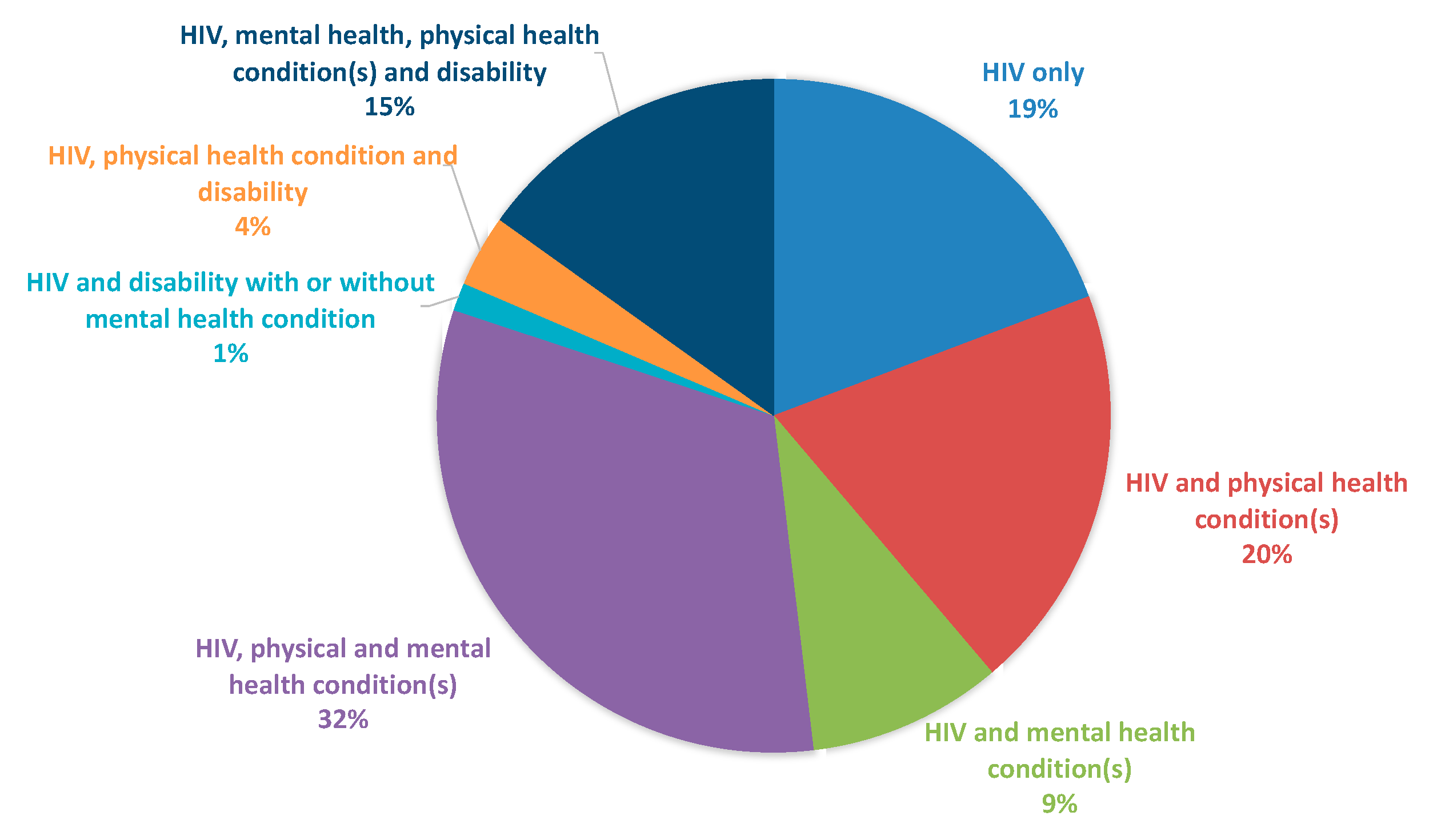
3.7. Overall Burden of Overlapping Health Conditions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wandeler, G.; Johnson, L.F.; Egger, M. Trends in life expectancy of HIV-positive adults on antiretroviral therapy across the globe: Comparisons with general population. Curr. Opin. HIV AIDS 2016, 11, 492–500. [Google Scholar] [CrossRef] [Green Version]
- Deeks, S.G.; Phillips, A.N. HIV infection, antiretroviral treatment, ageing, and non-AIDS related morbidity. BMJ 2009, 338, a3172. [Google Scholar] [CrossRef] [Green Version]
- Goulet, J.L.; Fultz, S.L.; Rimland, D.; Butt, A.; Gibert, C.; Rodriguez-Barradas, M.; Bryant, K.; Justice, A.C. Aging and infectious diseases: Do patterns of comorbidity vary by HIV status, age, and HIV severity? Clin. Infect. Dis. 2007, 45, 1593–1601. [Google Scholar] [CrossRef] [Green Version]
- Warriner, A.H.; Burkholder, G.A.; Overton, E.T. HIV-related metabolic comorbidities in the current ART era. Infect. Dis. Clin. N. Am. 2014, 28, 457–476. [Google Scholar] [CrossRef]
- Kendall, C.E.; Wong, J.; Taljaard, M.; Glazier, R.H.; Hogg, W.; Younger, J.; Manuel, D.G. A cross-sectional, population-based study measuring comorbidity among people living with HIV in Ontario. BMC Public Health 2014, 14, 161. [Google Scholar] [CrossRef] [Green Version]
- Justice, A.C. HIV and aging: Time for a new paradigm. Curr. HIV/AIDS Rep. 2010, 7, 69–76. [Google Scholar] [CrossRef]
- Gabuzda, D.; Jamieson, B.D.; Collman, R.G.; Lederman, M.M.; Burdo, T.H.; Deeks, S.G.; Dittmer, D.P.; Fox, H.S.; Funderburg, N.T.; Pahwa, S.G.; et al. Pathogenesis of Aging and Age-related Comorbidities in People with HIV: Highlights from the HIV ACTION Workshop. Pathog. Immun. 2020, 5, 143–174. [Google Scholar] [CrossRef]
- Sigel, K.; Wisnivesky, J.; Gordon, K.; Dubrow, R.; Justice, A.; Brown, S.T.; Goulet, J.; Butt, A.A.; Crystal, S.; Rimland, D.; et al. HIV as an independent risk factor for incident lung cancer. AIDS 2012, 26, 1017–1025. [Google Scholar] [CrossRef] [Green Version]
- Madeddu, G.; Fois, A.G.; Calia, G.M.; Babudieri, S.; Soddu, V.; Becciu, F.; Fiori, M.L.; Spada, V.; Lovigu, C.; Mannazzu, M.; et al. Chronic obstructive pulmonary disease: An emerging comorbidity in HIV-infected patients in the HAART era? Infection 2013, 41, 347–353. [Google Scholar] [CrossRef]
- Leung, J.M.; Liu, J.C.; Mtambo, A.; Ngan, D.; Nashta, N.; Guillemi, S.; Harris, M.; Lima, V.D.; Mattman, A.; Shaipanich, T.; et al. The determinants of poor respiratory health status in adults living with human immunodeficiency virus infection. AIDS Patient Care STDs 2014, 28, 240–247. [Google Scholar] [CrossRef]
- Nasi, M.; De Biasi, S.; Gibellini, L.; Bianchini, E.; Pecorini, S.; Bacca, V.; Guaraldi, G.; Mussini, C.; Pinti, M.; Cossarizza, A. Ageing and inflammation in patients with HIV infection. Clin. Exp. Immunol. 2017, 187, 44–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Brien, N.; Greene, S.; Carter, A.; Lewis, J.; Nicholson, V.; Kwaramba, G.; Ménard, B.; Kaufman, E.; Ennabil, N.; Andersson, N.; et al. Envisioning Women-Centered HIV Care: Perspectives from Women Living with HIV in Canada. Womens Health Issues 2017, 27, 721–730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tapp, C.; Milloy, M.J.; Kerr, T.; Zhang, R.; Guillemi, S.; Hogg, R.S.; Montaner, J.; Wood, E. Female gender predicts lower access and adherence to antiretroviral therapy in a setting of free healthcare. BMC Infect. Dis. 2011, 11, 86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giles, M.L.; Achhra, A.C.; Abraham, A.G.; Haas, A.D.; Gill, M.J.; Lee, M.P.; Luque, M.; McGowan, C.; Cornell, M.; Braitstein, P.; et al. Sex-based differences in antiretroviral therapy initiation, switching and treatment interruptions: Global overview from the International Epidemiologic Databases to Evaluate AIDS (IeDEA). J. Int. AIDS Soc. 2018, 21, e25149. [Google Scholar] [CrossRef]
- Puskas, C.M.; Forrest, J.I.; Parashar, S.; Salters, K.A.; Cescon, A.M.; Kaida, A.; Cescon, A.M.; Kaida, A.; Miller, C.L.; Bangsberg, D.R.; et al. Women and vulnerability to HAART non-adherence: A literature review of treatment adherence by gender from 2000 to 2011. Curr. HIV/AIDS Rep. 2011, 8, 277–287. [Google Scholar] [CrossRef]
- Durvasula, R. HIV/AIDS in older women: Unique challenges, unmet needs. Behav. Med. 2014, 40, 85–98. [Google Scholar] [CrossRef]
- Edwards, A.E.; Collins, C.B., Jr. Exploring the influence of social determinants on HIV risk behaviors and the potential application of structural interventions to prevent HIV in women. J. Health Disparities Res. Pract. 2014, 7, 141–155. [Google Scholar]
- Haddad, N.; Li, J.S.; Totten, S.; McGuire, M. HIV in Canada–Surveillance Report, 2017. Can. Commun. Dis. Rep. 2018, 44, 324–332. [Google Scholar] [CrossRef]
- Loutfy, M.R.; Sherr, L.; Sonnenberg-Schwan, U.; Walmsley, S.L.; Johnson, M.; d’Arminio Monforte, A.; Women for Positive Action. Caring for women living with HIV: Gaps in the evidence. J. Int. AIDS Soc. 2013, 16, 18509. [Google Scholar] [CrossRef]
- Andany, N.; Kennedy, V.L.; Aden, M.; Loutfy, M. Perspectives on menopause and women with HIV. Int. J. Women’s Health 2016, 8, 1–22. [Google Scholar] [CrossRef] [Green Version]
- Raffe, S.; Sabin, C.; Gilleece, Y.; Women against Viruses in Europe EACS. Comorbidities in women living with HIV: A systematic review. HIV Med. 2022, 23, 331–361. [Google Scholar] [CrossRef] [PubMed]
- Loutfy, M.; de Pokomandy, A.; Kennedy, V.L.; Carter, A.; O’Brien, N.; Proulx-Boucher, K.; Ding, E.; Lewis, J.; Nicholson, V.; Beaver, K.; et al. Cohort profile: The Canadian HIV Women’s Sexual and Reproductive Health Cohort Study (CHIWOS). PLoS ONE 2017, 12, e0184708. [Google Scholar] [CrossRef] [Green Version]
- Webster, K.; Carter, A.; Proulx-Boucher, K.; Dubuc, D.; Nicholson, V.; Beaver, K.; Gasingirwa, C.; Ménard, B.; O’Brien, N.; Mitchell, K.; et al. Strategies for Recruiting Women Living with Human Immunodeficiency Virus in Community-Based Research: Lessons from Canada. Prog. Community Health Partnersh. Res. Educ. Action 2018, 12, 21–34. [Google Scholar] [CrossRef] [Green Version]
- Loutfy, M.; Greene, S.; Kennedy, V.L.; Lewis, J.; Thomas-Pavanel, J.; Conway, T.; de Pokomandy, A.; O’Brien, N.; Carter, A.; Tharao, W.; et al. Establishing the Canadian HIV Women’s Sexual and Reproductive Health Cohort Study (CHIWOS): Operationalizing Community-based Research in a Large National Quantitative Study. BMC Med. Res. Methodol. 2016, 16, 101. [Google Scholar] [CrossRef] [Green Version]
- Darragh, T.M.; Colgan, T.J.; Thomas Cox, J.; Heller, D.S.; Henry, M.R.; Luff, R.D.; McCalmont, T.; Nayar, R.; Palefsky, J.M.; Stoler, M.H.; et al. The Lower Anogenital Squamous Terminology Standardization project for HPV-associated lesions: Background and consensus recommendations from the College of American Pathologists and the American Society for Colposcopy and Cervical Pathology. Int. J. Gynecol. Pathol. 2013, 32, 76–115. [Google Scholar] [CrossRef] [Green Version]
- Collins, L.F.; Sheth, A.N.; Mehta, C.C.; Naggie, S.; Golub, E.T.; Anastos, K.; French, A.L.; Kassaye, S.; Taylor, T.; Fischl, M.A.; et al. The Prevalence and Burden of Non-AIDS Comorbidities among Women Living with or at Risk for Human Immunodeficiency Virus Infection in the United States. Clin. Infect. Dis. 2021, 72, 1301–1311. [Google Scholar] [CrossRef]
- Public Health Agency of Canada. Report from the Canadian Chronic Disease Surveillance System: Asthma and Chronic Obstructive Pulmonary Disease (COPD) in Canada, 2018; Government of Canada: Ottawa, ON, Canada, 2018.
- Statistics Canada. Prevalence of Osteoarthritis, by Age Group and Site of Joint Pain, Household Population Aged 20 or Older Diagnosed with Arthritis, Canada Excluding Territories, 2009; Statistics Canada: Ottawa, ON, Canada, 2015.
- Statistics Canada. Blood Pressure of Adults, 2016–2019. Ottawa. 23 March 2021. Available online: https://www150.statcan.gc.ca/n1/en/pub/82-625-x/2021001/article/00001-eng.pdf?st=9vVmVLBT (accessed on 15 January 2022).
- Statistics Canada. Cholesterol Levels of Adults, 2016–2019. Ottawa. 28 June 2021. Available online: https://www150.statcan.gc.ca/n1/en/pub/82-625-x/2021001/article/00003-eng.pdf?st=4JWxL_A7 (accessed on 15 January 2022).
- Public Health Agency of Canada. Fast Facts from the 2009 Canadian Community Health Survey—Osteoporosis Rapid Response; Government of Canada: Ottawa, ON, Canada, 2010.
- Statistics Canada. Health Fact Sheets: Diabetes, 2017; Statistics Canada: Ottawa, ON, Canada, 2018.
- de Pokomandy, A.; Burchell, A.N.; Salters, K.; Ding, E.; O’Brien, N.; Bakombo, D.M.; Proulx-Boucher, K.; Boucoiran, I.; Pick, N.; Ogilvie, G.; et al. Cervical cancer screening among women living with HIV: A cross-sectional study using the baseline questionnaire data from the Canadian HIV Women’s Sexual and Reproductive Health Cohort Study (CHIWOS). Can. Med. Assoc. Open Access J. 2019, 7, E217–E226. [Google Scholar] [CrossRef] [Green Version]
- Knoll, A.; MacLennan, R. Prevalence and correlates of depression in Canada: Findings from the Canadian Community Health Survey. Can. Psychol. Psychol. Can. 2017, 58, 116–123. [Google Scholar] [CrossRef]
- Pelletier, L.; O’Donnell, S.; McRae, L.; Grenier, J. The burden of generalized anxiety disorder in Canada. Health Promot. Chronic Dis. Prev. Can. Res. Policy Pract. 2017, 37, 54–62. [Google Scholar] [CrossRef] [Green Version]
- Van Ameringen, M.; Mancini, C.; Patterson, B.; Boyle, M.H. Post-traumatic stress disorder in Canada. CNS Neurosci. Ther. 2008, 14, 171–181. [Google Scholar] [CrossRef]
- Wagner, A.C.; Jaworsky, D.; Logie, C.H.; Conway, T.; Pick, N.; Wozniak, D.; Rana, J.; Tharao, W.; Kaida, A.; de Pokomandy, A.; et al. High rates of posttraumatic stress symptoms in women living with HIV in Canada. PLoS ONE 2018, 13, e0200526. [Google Scholar] [CrossRef]
- Lacombe-Duncan, A.; Warren, L.; Kay, E.S.; Persad, Y.; Soor, J.; Kia, H.; Underhill, A.; Logie, C.H.; Kazemi, M.; Kaida, A.; et al. Mental health among transgender women living with HIV in Canada: Findings from a national community-based research study. AIDS Care 2021, 33, 192–200. [Google Scholar] [CrossRef]
- Brennan, J.; Kuhns, L.M.; Johnson, A.K.; Belzer, M.; Wilson, E.C.; Garofalo, R.; Adolescent Medicine Trials Network for HIV/AIDS Interventions. Syndemic theory and HIV-related risk among young transgender women: The role of multiple, co-occurring health problems and social marginalization. Am. J. Public Health 2012, 102, 1751–1757. [Google Scholar] [CrossRef]
- Balderson, B.H.; Grothaus, L.; Harrison, R.G.; McCoy, K.; Mahoney, C.; Catz, S. Chronic illness burden and quality of life in an aging HIV population. AIDS Care 2013, 25, 451–458. [Google Scholar] [CrossRef]
- Edelman, E.J.; Gordon, K.S.; Glover, J.; McNicholl, I.R.; Fiellin, D.A.; Justice, A.C. The next therapeutic challenge in HIV: Polypharmacy. Drugs Aging 2013, 30, 613–628. [Google Scholar] [CrossRef] [Green Version]
- Wing, E.J. HIV and aging. Int. J. Infect. Dis. 2016, 53, 61–68. [Google Scholar] [CrossRef] [Green Version]
- Muessig, K.E.; Panter, A.T.; Mouw, M.S.; Amola, K.; Stein, K.E.; Murphy, J.S.; Maiese, E.M.; Wohl, D.A. Medication-Taking Practices of Patients on Antiretroviral HIV Therapy: Control, Power, and Intentionality. AIDS Patient Care STDs 2015, 29, 606–616. [Google Scholar] [CrossRef] [Green Version]
- Do, A.N.; Rosenberg, E.S.; Sullivan, P.S.; Beer, L.; Strine, T.W.; Schulden, J.D.; Fagan, J.L.; Freedman, M.S.; Skarbinski, J. Excess burden of depression among HIV-infected persons receiving medical care in the united states: Data from the medical monitoring project and the behavioral risk factor surveillance system. PLoS ONE 2014, 9, e92842. [Google Scholar] [CrossRef] [Green Version]
- Justice, A.C. Prioritizing primary care in HIV: Comorbidity, toxicity, and demography. Top. HIV Med. A Publ. Int. AIDS Soc. USA 2006, 14, 159–163. [Google Scholar]
- Franceschi, S.; Jaffe, H. Cervical cancer screening of women living with HIV infection: A must in the era of antiretroviral therapy. Clin. Infect. Dis. 2007, 45, 510–513. [Google Scholar] [CrossRef] [Green Version]
- Soto, T.A.; Bell, J.; Pillen, M.B.; Hiv/aids Treatment Adherence, Health Outcomes, Cost Study Group. Literature on integrated HIV care: A review. AIDS Care 2004, 16 (Suppl. S1), S43–S55. [Google Scholar] [CrossRef]
- Hoang, T.; Goetz, M.B.; Yano, E.M.; Rossman, B.; Anaya, H.D.; Knapp, H.; Korthuis, P.T.; Henry, R.; Bowman, C.; Gifford, A.; et al. The impact of integrated HIV care on patient health outcomes. Med. Care 2009, 47, 560–567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Brien, N.; Hong, Q.N.; Law, S.; Massoud, S.; Carter, A.; Kaida, A.; Loutfy, M.; Cox, J.; Andersson, N.; de Pokomandy, A. Health System Features That Enhance Access to Comprehensive Primary Care for Women Living with HIV in High-Income Settings: A Systematic Mixed Studies Review. AIDS Patient Care STDs 2018, 32, 129–148. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.; Samarina, A.; Xi, H.; Valdez Ramalho Madruga, J.; Hocqueloux, L.; Loutfy, M.; Fournelle, M.-J.; Norton, M.; van Wyk, J.; Zachry, W.; et al. Barriers to access to care reported by women living with HIV across 27 countries. AIDS Care 2015, 27, 1220–1230. [Google Scholar] [CrossRef] [PubMed]
- Sordo del Castillo, L.; Ruiz-Perez, I.; Olry de Labry Lima, A. Biological, psychosocial, therapeutic and quality of life inequalities between HIV-positive men and women-a review from a gender perspective. AIDS Rev. 2010, 12, 113–120. [Google Scholar]
- Shokoohi, M.; Bauer, G.R.; Kaida, A.; Logie, C.H.; Lacombe-Duncan, A.; Milloy, M.J.; Lloyd-Smith, E.; Carter, A.; Loutfy, M.; CHIWOS Research Team. Patterns of social determinants of health associated with drug use among women living with HIV in Canada: A latent class analysis. Addiction 2019, 114, 1214–1224. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | 18-Months Survey Completed n (%) [95% CI] | Lost to Follow-Up n (%) [95% CI] |
|---|---|---|
| TOTAL | 1039 (85.4) | 178 (14.6) |
| Province | ||
| British Columbia | 299 (28.8) [26.0–31.6] | 57 (32.0) [25.2–39.4] |
| Ontario | 420 (40.4) [37.4–43.5] | 88 (49.4) [41.9–57.0] |
| Québec | 320 (30.8) [28.0–33.7] | 33 (18.5) [13.1–25.0] |
| Age | ||
| 16–29 | 71 (6.8) [5.4–8.5] | 20 (11.2) [7.0–16.8] |
| 30–39 | 272 (26.2) [23.5–29.0] | 53 (39.8) [23.2–37.1] |
| 40–49 | 355 (34.2) [31.3–37.1] | 66 (37.1) [30.0–44.6] |
| 50+ | 341 (32.8) [30.0–35.8] | 39 (21.9) [16.1–28.7] |
| Ethnicity | ||
| Indigenous | 173 (16.7) [14.4–19.1] | 51 (28.7) [22.1–35.9] |
| ACB | 375 (36.1) [33.2–39.1] | 39 (21.9) [16.1–28.7] |
| White | 414 (39.8) [36.9–42.9] | 70 (39.3) [32.1–46.9] |
| Other | 77 (7.4) [5.9–9.2] | 18 (10.1) [6.1–15.5] |
| Country of birth | ||
| Canadian-born | 589 (56.8) [53.6–59.7] | 124 (69.7) [62.3–76.3] |
| Foreign-born | 448 (43.1) [40.1–46.2] | 54 (30.3) [23.7–37.7] |
| DK/PNTA | 2 (0.2) [0–0.7] | 0 (0) [0–2.1] |
| Gender identity | ||
| Cisgender woman | 1001 (96.3) [95.0–97.4] | 171 (96.1) [92.1–98.4] |
| Transgender woman | 32 (3.1) [2.1–4.3] | 5 (2.8) [0.9–6.4] |
| Other | 6 (0.6) [0.2–1.3] | 2 (1.1) [0.1–4.0] |
| Education | ||
| Less than high school | 181 (17.4) [15.2–19.9] | 37 (20.8) [15.1–27.5] |
| High school or more | 854 (82.2) [79.7–84.5] | 140 (78.7) [71.9–84.4] |
| DK/PNTA | 4 (0.4) [0.1–1.0] | 1 (0.6) [0–3.1] |
| Employment | ||
| Yes | 233 (22.4) [19.9–25.1] | 27 (15.2) [10.2–21.3] |
| No | 800 (77.0) [74.3–79.5] | 150 (84.2) [78.1–89.3] |
| DK/PNTA | 6 (0.6) [0.2–1.3] | 1 (0.6) [0–3.1] |
| Household income (CAD) | ||
| <20,000 | 641 (61.7) [58.7–66.7] | 121 (68.0) [60.6–74.8] |
| ≥20,000 | 366 (35.2) [32.3–38.2] | 47 (26.4) [20.1–33.5] |
| DK/PNTA | 32 (3.1) [2.1–4.3] | 10 (5.6) [2.7–10.1] |
| Injection drug use | ||
| Never | 687 (66.1) [63.2–69.0] | 95 (53.4) [45.8–60.9] |
| Ever | 348 (33.5) [30.6–36.5] | 76 (42.7) [35.3–50.3] |
| DK/PNTA | 4 (0.4) [0.1–1.0] | 7 (3.9) [1.6–7.9] |
| Cigarette smoking status | ||
| Never | 428 (41.2) [38.2–44.3] | 50 (28.1) [21.6–35.3] |
| Former | 138 (13.3) [11.3–15.5] | 21 (11.8) [7.5–17.5] |
| Regular/occasional smoker | 469 (45.1) [42.1–48.2] | 103 (57.9) [50.3–65.2] |
| DK/PNTA | 4 (0.4) [0.1–1.0] | 4 (2.3) [0.6–5.7] |
| Most recent HIV viral load | ||
| Undetectable (<50 copies/mL) | 861 (82.9) [80.4–85.1] | 135 (75.8) [68.9–81.9] |
| Detectable (≥50 copies/mL) 2 | 134 (12.9) [10.9–15.1] | 31 (17.4) [12.2–23.8] |
| DK/PNTA | 44 (4.2) [3.1–5.6] | 10 (5.6) [2.7–10.1] |
| Diagnosed Health Condition 1 | Overall | Gender Identity | |
|---|---|---|---|
| Transgender Women | Cisgender Women | ||
| n = 1039 n (%) [95% CI] | n = 32 n (%) [95% CI] | n = 1007 n (%) [95% CI] | |
| Physical health diagnosis (lifetime prevalence) | |||
| Obesity (BMI > 30) | 277 (26.7) [24.0–29.5] | 7 (21.9) [9.3–40.0] | 270 (26.8) [24.1–29.7] |
| Asthma/COPD | 242 (23.3) [20.8–26.0] | 7 (21.9) [9.3–40.0] | 235 (23.3) [20.8–26.1] |
| Arthritis, osteoarthritis | 217 (20.9) [18.5–23.5] | 4 (12.5) [3.5–29.0] | 213 (21.2) [18.7–23.8] |
| Cancer or pre-cancer | 207 (19.9) [17.5–22.5] | 3 (9.4) [2.0–25.0] | 204 (20.3) [17.8–22.9] |
| Chronic pains for other causes than arthritis/ osteoarthritis requiring medication | 198 (19.1) [16.7–21.6] | 4 (12.5) [3.5–29.0] | 194 (19.3) [16.9–21.8] |
| Hypertension | 179 (17.2) [15.0–19.7] | 2 (6.3) [0.8–20.8] | 177 (17.6) [15.3–20.1] |
| High cholesterol | 139 (13.4) [11.4–15.6] | 3 (9.4) [2.0–25.0] | 136 (13.5) [11.5–15.8] |
| Osteoporosis/osteopenia/decreased bone density | 120 (11.6) [9.7–13.7] | 4 (12.5) [3.5–29.0] | 116 (11.5) [9.6–13.7] |
| Thyroid problem | 107 (10.3) [8.5–12.3] | 2 (6.3) [0.8–20.8] | 105 (10.4) [8.6–12.5] |
| Fractures | 98 (9.4) [7.7–11.4] | 4 (12.5) [3.5–29.0] | 94 (9.3) [7.6–11.3] |
| Diabetes | 90 (8.7) [7.0–10.5] | 2 (6.3) [0.8–20.8] | 88 (8.7) [7.1–10.7] |
| HIV/AIDS wasting syndrome | 71 (6.8) [5.4–8.5] | 2 (6.3) [0.8–20.8] | 69 (6.9) [5.4–8.6] |
| Cardiac arrythmia | 64 (6.2) [4.8–7.8] | 5 (15.6) [5.3–32.8] | 59 (5.9) [4.5–7.5] |
| Strokes | 39 (3.8) [2.7–5.1] | 3 (9.4) [2.0–25.0] | 36 (3.6) [2.5–4.9] |
| Cognitive impairment | 39 (3.8) [2.7–5.1] | 2 (6.3) [0.8–20.8] | 37 (3.7) [2.6–4.9] |
| Mental health diagnoses currently living with | |||
| Depression | 336 (32.3) [29.5–35.3] | 8 (25.0) [11.5–43.4] | 328 (32.6) [29.7–35.6] |
| Anxiety | 306 (29.5) [26.7–32.3] | 7 (21.9) [9.3–40.0] | 299 (29.7) [26.9–32.6] |
| Sleep disorder | 229 (22.0) [19.6–24.7] | 2 (6.3) [0.8–20.8] | 227 (22.5) [20.0–25.3] |
| Drug addiction | 227 (21.9) [19.4–24.5] | 10 (31.3) [16.1–50.0] | 217 (21.5) [19.0–24.2] |
| Post-traumatic stress disorder | 144 (13.9) [11.8–16.1] | 2 (6.3) [0.8–20.8] | 142 (14.1) [12.0–16.4] |
| Alcohol addiction | 94 (9.1) [7.4–11.0] | 2 (6.3) [0.8–20.8] | 92 (9.1) [7.4–11.1] |
| Bipolar disorder | 66 (6.4) [4.9–8.0] | 0 (0) [0–10.9] | 66 (6.6) [5.1–8.3] |
| Obsessive-compulsive disorder | 34 (3.3) [2.3–4.5] | 2 (6.3) [0.8–20.8] | 32 (3.2) [2.2–4.5] |
| Disabilities currently living with | |||
| Partial deafness | 91 (8.8) [7.1–10.6] | 4 (12.5) [3.5–29.0] | 87 (8.6) [7.0–10.5] |
| Difficulty walking—require cane | 81 (7.8) [6.2–9.6] | 0 (0) [0–10.9] | 81 (8.0) [6.4–9.9] |
| Ethnicity | Indigenous | ACB | White/Other | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Age | 16–39 n (%) [95% CI] | 40–49 n (%) [95% CI] | 50+ n (%) [95% CI] | 16–39 n (%) [95% CI] | 40–49 n (%) [95% CI] | 50+ n (%) [95% CI] | 16–39 n (%) [95% CI] | 40–49 n (%) [95% CI] | 50+ n (%) [95% CI] |
| Total (row%) | 52 (30.1) | 62 (35.8) | 59 (34.1) | 127 (33.9) | 131 (34.9) | 117 (31.2) | 99 (20.2) | 159 (32.3) | 233 (47.5) |
| Physical health diagnosis (lifetime prevalence) 1 | |||||||||
| Obesity (BMI > 30) 2,3 | 17 (32.7) [20.3–47.1] | 19 (30.7) [19.6–43.7] | 12 (20.3) [11.0–32.8] | 28 (22.1) [15.2–30.3] | 40 (30.5) [22.8–39.2] | 50 (42.7) [33.6–52.2] | 32 (32.3) [23.3–42.5] | 42 (26.4) [19.7–34.0] | 37 (15.9) [11.4–21.2] |
| Asthma/COPD 2,3 | 10 (19.2) [9.6–23.5] | 23 (37.1) [25.2–50.3] | 19 (32.2) [20.6–45.6] | 8 (6.3) [2.8–12.0] | 9 (6.9) [3.2–12.6] | 9 (7.7) [3.6–14.1] | 28 (28.3) [19.7–38.2] | 55 (34.6) [27.2–42.5] | 81 (34.8) [28.7–41.3] |
| Arthritis, osteoarthritis 2,3 | 6 (11.5) [4.4–23.4] | 27 (43.6) [31.0–56.7] | 28 (47.5) [34.3–60.9] | <5% | 9 (6.9) [3.2–12.6] | 20 (17.1) [10.8–25.2] | 8 (8.1) [3.6–15.3] | 33 (20.8) [14.7–27.9] | 84 (36.1) [29.9–42.6] |
| Cancer or pre-cancer 2 | 9 (17.3) [8.2–30.3] | 14 (22.6) [12.9–35.0] | 12 (20.3) [11.0–32.8] | 11 (8.7) [4.4–15.0] | 13 (9.9) [5.4–16.4] | 18 (15.4) [9.4–23.2] | 25 (25.3) [17.1–35.0] | 41 (25.8) [19.2–33.3] | 64 (27.5) [21.8–33.7] |
| Chronic pains for other causes than arthristis/osteoarthritis requiring medication 2,3 | 7 (13.5) [5.6–25.8] | 24 (38.7) [26.6–51.9] | 19 (32.2) [20.6–45.6] | <5% | 9 (6.9) [3.2–12.6] | 13 (11.1) [6.1–18.3] | 10 (10.1) [5.0–17.8] | 44 (27.7) [20.9–35.3] | 67 (28.8) [23.0–35.0] |
| Hypertension 3 | 5 (9.6) [3.2–21.0] | 9 (14.5) [6.9–25.8] | 15 (25.4) [15.0–38.4] | 9 (7.1) [3.3–13.0] | 24 (18.3) [12.1–26.0] | 41 (35.0) [26.5–44.4] | <5% | 19 (12.0) [7.4–18.0] | 53 (22.8) [17.5–28.7] |
| High cholesterol 2,3 | 3 (5.8) [1.2–15.9] | 4 (6.5) [1.8–15.7] | 9 (15.3) [7.2–27.0] | <5% | 13 (9.9) [5.4–16.4] | 15 (12.8) [7.4–20.3] | 10 (10.1) [5.0–17.8] | 21 (13.2) [8.4–19.5] | 60 (25.8) [20.3–31.9] |
| Osteoporosis/osteopenia/decreased bone density 2,3 | 4 (7.7) [2.1–18.5] | 8 (12.9) [5.7–23.9] | 17 (28.8) [17.8–42.1] | <5% | <5% | 13 (11.1) [6.1–18.3] | 5 (5.1) [1.7–35.0] | 12 (7.6) [4.0–12.8] | 55 (23.6) [18.3–29.6] |
| Thyroid problem | 5 (9.6) [3.2–21.0] | 8 (12.9) [5.7–23.9] | 6 (10.2) [3.8–20.8] | <5% | <5% | 10 (8.6) [4.2–15.2] | 7 (7.1) [2.9–14.0] | 25 (15.7) [10.4–22.3] | 38 (16.3) [11.8–21.7] |
| Fractures | 7 (13.5) [5.6–25.8] | 8 (12.9) [5.7–23.9] | 13 (22.0) [12.3–34.7] | <5% | <5% | 6 (5.1) [1.9–10.8] | 8 (8.1) [3.6–15.3] | 17 (10.7) [6.4–16.7] | 35 (15.0) [10.7–20.3] |
| Diabetes | <5% | <5% | 7 (11.9) [4.9–22.9] | <5% | 12 (9.2) [4.8–15.5] | 20 (17.1) [10.8–25.2] | 5 (5.1) [1.7–35.0] | 15 (9.4) [5.4–15.1] | 25 (10.7) [7.1–15.4] |
| HIV/AIDS wasting syndrome | <5% | <5% | <5% | <5% | 11 (8.4) [4.3–14.5] | 9 (7.7) [3.6–14.1] | 6 (6.1) [2.3–12.7] | 10 (6.3) [3.1–11.3] | 26 (11.2) [7.4–15.9] |
| Cardiac arrythmia | <5% | 7 (11.3) [4.7-21.9] | 6 (10.2) [3.8–20.8] | <5% | <5% | 6 (5.1) [1.9–10.8] | 5 (5.1) [1.7–35.0] | 11 (6.9) [3.5–12.0] | 20 (8.6) [5.3–12.9] |
| Strokes | <5% | 4 (6.5) [1.8–15.7] | 6 (10.2) [3.8–20.8] | 0 | <5% | 6 (5.1) [1.9–10.8] | <5% | <5% | 13 (5.6) [3.0–9.4] |
| Mental health diagnoses currently living with 1 | |||||||||
| Depression 2 | 23 (44.2) [30.5–58.7] | 32 (51.6) [38.6–64.5] | 27 (45.8) [32.7–59.2] | 18 (14.2) [8.6–21.5] | 20 (15.3) [9.6–22.6] | 27 (23.1) [15.8–31.8] | 31 (31.3) [22.4–41.4] | 70 (44.0) [36.2–52.1] | 88 (37.8) [31.5–44.3] |
| Anxiety 2 | 19 (36.5) [23.6–51.0] | 33 (52.2) [40.1–66.0] | 24 (40.7) [18.1–54.3] | 12 (9.5) [5.0–15.9] | 11 (8.4) [4.3–14.5] | 16 (13.7) [8.0–21.3] | 40 (40.4) [30.7–50.7] | 71 (44.7) [36.8–52.7] | 80 (34.3) [28.3–40.8] |
| Sleep disorder 2 | 10 (19.2) [9.6–23.5] | 18 (29.0) [18.2–41.9] | 15 (25.4) [15.0–38.4] | 11 (8.7) [4.4–15.0] | 12 (9.2) [4.8–15.5] | 18 (15.4) [9.4–23.2] | 23 (23.2) [15.3–32.8] | 47 (29.6) [22.6–37.3] | 75 (32.2) [26.2–38.6] |
| Drug addiction 2,3 | 35 (67.3) [52.9–79.7] | 39 (62.9) [49.7–74.8] | 27 (45.8) [32.7–59.2] | <5% | <5% | <5% | 35 (35.4) [26.0–45.6] | 45 (28.3) [21.5–36.0] | 41 (17.6) [12.9–23.1] |
| Post-traumatic stress disorder 2 | 15 (28.9) [17.1–43.1] | 22 (35.5) [23.7–48.7] | 28 (30.5) [34.3–60.9] | <5% | <5% | 6 (5.1) [1.9–10.8] | 14 (14.1) [8.0–22.6] | 35 (12.5) [15.8–29.3] | 29 (12.5) [8.5–17.4] |
| Alcohol addiction 2 | 11 (21.2) [11.1–34.7] | 23 (37.1) [25.2–50.3] | 17 (28.8) [17.8–42.1] | <5% | <5% | <5% | 13 (13.1) [7.2–21.4] | 13 (8.2) [4.4–13.6] | 13 (5.6) [3.0–9.4] |
| Bipolar disorder | 7 (13.5) [5.6–25.8] | 9 (14.5) [6.9–25.8] | 6 (10.2) [3.8–20.8] | <5% | 0 | <5% | 11 (11.1) [5.7–19.0] | 16 (10.1) [5.9–15.8] | 13 (5.6) [3.0–9.4] |
| Anorexia nervosa or bulimia nervosa | 4 (7.7) [2.1–18.5] | <5% | <5% | 0 | 0 | 0 | <5% | <5% | <5% |
| Personality disorder | 4 (7.7) [2.1–18.5] | 8 (12.9) [5.7–23.9] | <5% | <5% | <5% | 0 | 8 (8.1) [3.6–15.3] | 11 (6.9) [3.5–12.0] | <5% |
| Obsessive-compulsive disorder | 5 (9.6) [3.2–21.0] | <5% | 5 (8.5) [2.8–18.7] | <5% | 0 | 0 | <5% | 9 (5.7) [2.6–10.5] | <5% |
| Disabilities currently living with 1 | |||||||||
| Partial deafness | 4 (7.7) [2.1–18.5] | 10 (16.1) [8.0–27.7] | 16 (27.1) [16.4–40.3] | <5% | <5% | <5% | <5% | 13 (8.2) [4.4–13.6] | 39 (16.7) [12.2–22.2] |
| Partial blindness | 6 (11.5) [4.4–23.4] | 5 (9.7) [2.7–17.8] | 6 (10.2) [3.8–20.8] | <5% | <5% | <5% | <5% | 11 (6.9) [3.5–12.0] | <5% |
| Difficulty walking—require cane | 3 (5.8) [1.2–15.9] | 6 (9.7) [3.6–19.9] | 9 (15.3) [7.2–27.0] | <5% | <5% | 8 (6.8) [3.0–13.0] | <5% | 11 (6.9) [3.5–12.0] | 37 (15.9) [11.4–21.2] |
| Difficulty walking—require wheelchair | 0 | <5% | 4 (6.8) [1.9–16.5] | 0 | 0 | <5% | 0 | <5% | <5% |
| Difficulty moving one or both arms | <5% | <5% | 5 (8.5) [2.8–18.7] | <5% | <5% | <5% | <5% | <5% | <5% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heer, E.; Kaida, A.; O’Brien, N.; Kleiner, B.; Pierre, A.; Rouleau, D.; Burchell, A.N.; Skerritt, L.; Proulx-Boucher, K.; Nicholson, V.; et al. Prevalence of Physical Health, Mental Health, and Disability Comorbidities among Women Living with HIV in Canada. J. Pers. Med. 2022, 12, 1294. https://doi.org/10.3390/jpm12081294
Heer E, Kaida A, O’Brien N, Kleiner B, Pierre A, Rouleau D, Burchell AN, Skerritt L, Proulx-Boucher K, Nicholson V, et al. Prevalence of Physical Health, Mental Health, and Disability Comorbidities among Women Living with HIV in Canada. Journal of Personalized Medicine. 2022; 12(8):1294. https://doi.org/10.3390/jpm12081294
Chicago/Turabian StyleHeer, Emily, Angela Kaida, Nadia O’Brien, Bluma Kleiner, Alie Pierre, Danielle Rouleau, Ann N. Burchell, Lashanda Skerritt, Karène Proulx-Boucher, Valerie Nicholson, and et al. 2022. "Prevalence of Physical Health, Mental Health, and Disability Comorbidities among Women Living with HIV in Canada" Journal of Personalized Medicine 12, no. 8: 1294. https://doi.org/10.3390/jpm12081294