
Effectiveness of a Comprehensive Mental Health Literacy Educational Programme for Junior High School Students: A Randomised Controlled Trial Examining Changes in Their Knowledge, Attitudes, and Behaviour

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
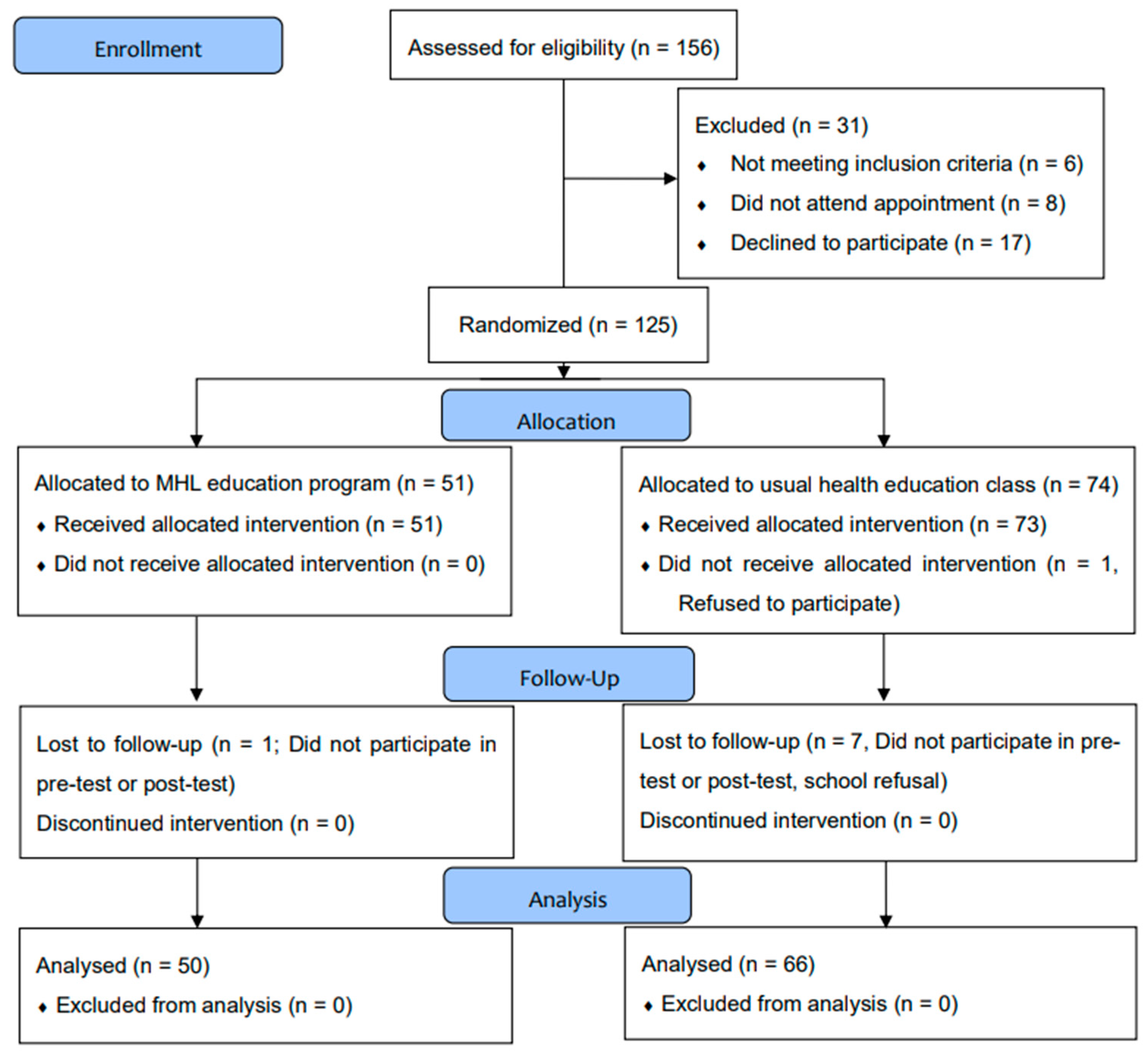
2.2. Study Design
2.3. Interventions
2.4. Measures
2.5. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gore, F.M.; Bloem, P.J.N.; Patton, G.C.; Ferguson, J.; Joseph, V.; Coffey, C.; Sawyer, S.M.; Mathers, C.D. Global burden of disease in young people aged 10-24 years: A systematic analysis. Lancet 2011, 377, 2093–2102. [Google Scholar] [CrossRef]
- Kessler, R.C.; Angermeyer, M.; Anthony, J.C.; De Graaf, R.; Demyttenaere, K.; Gasquet, I.; De Girolamo, G.; Gluzman, S.; Gureje, O.; Haro, J.M.; et al. Lifetime prevalence and age-of-onset distributions of mental disorders in the World Health Organization’s World Mental Health Survey Initiative. World Psychiatry Off. J. World Psychiatr. Assoc. (WPA) 2007, 6, 168–176. [Google Scholar]
- Fusar-Poli, P.; McGorry, P.D.; Kane, J.M. Improving outcomes of first-episode psychosis: An overview. World Psychiatry Off. J. World Psychiatr. Assoc. (WPA) 2017, 16, 251–265. [Google Scholar] [CrossRef] [PubMed]
- Mizuno, M.; Suzuki, M.; Matsumoto, K.; Murakami, M.; Takeshi, K.; Miyakoshi, T.; Ito, F.; Yamazawa, R.; Kobayashi, H.; Nemoto, T.; et al. Clinical practice and research activities for early psychiatric intervention at Japanese leading centres. Early Interv. Psychiatry 2009, 3, 5–9. [Google Scholar] [CrossRef]
- Nemoto, T.; Funatogawa, T.; Takeshi, K.; Tobe, M.; Yamaguchi, T.; Morita, K.; Katagiri, N.; Tsujino, N.; Mizuno, M. Clinical practice at a multi-dimensional treatment centre for individuals with early psychosis in Japan. East Asian Arch. Psychiatry 2012, 22, 110–113. [Google Scholar]
- Fusar-Poli, P.; Bonoldi, I.; Yung, A.R.; Borgwardt, S.; Kempton, M.J.; Valmaggia, L.; Barale, F.; Caverzasi, E.; McGuire, P. Predicting psychosis: Meta-analysis of transition outcomes in individuals at high clinical risk. Arch. Gen. Psychiatry 2012, 69, 220–229. [Google Scholar] [CrossRef] [Green Version]
- Ito, S.; Nemoto, T.; Tsujino, N.; Ohmuro, N.; Matsumoto, K.; Matsuoka, H.; Tanaka, K.; Nishiyama, S.; Suzuki, M.; Kinoshita, H.; et al. Differential impacts of duration of untreated psychosis (DUP) on cognitive function in first-episode schizophrenia according to mode of onset. Eur. Psychiatry 2015, 30, 995–1001. [Google Scholar] [CrossRef]
- Nishi, D.; Ishikawa, H.; Kawakami, N. Prevalence of mental disorders and mental health service use in Japan. Psychiatry Clin. Neurosci. 2019, 73, 458–465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baba, Y.; Nemoto, T.; Tsujino, N.; Yamaguchi, T.; Katagiri, N.; Mizuno, M. Stigma toward psychosis and its formulation process: Prejudice and discrimination against early stages of schizophrenia. Compr. Psychiatry 2017, 73, 181–186. [Google Scholar] [CrossRef]
- Rickwood, D.; Deane, F.P.; Wilson, C.J.; Ciarrochi, J. Young people’s help-seeking for mental health problems. Aust. E-J. Adv. Ment. Health 2005, 4, 218–251. [Google Scholar] [CrossRef] [Green Version]
- Gulliver, A.; Griffiths, K.M.; Christensen, H. Perceived barriers and facilitators to mental health help-seeking in young people: A systematic review. BMC Psychiatry 2010, 10, 113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miyasaka, T. Philosophy of health education. In Health Education and Nutrition Education; Miyasaka, T., Ed.; Koseikan Ltd.: Tokyo, Japan, 1982; pp. 1–9. [Google Scholar]
- Miyasaka, T. Concept of health education. In Health Education.; Miyasaka, T., Kawada, T., Eds.; Medicalfriend Ltd.: Tokyo, Japan, 1984; pp. 2–18. [Google Scholar]
- Schrader, P.G.; Lawless, K.A. The knowledge, attitudes, behaviors approach how to evaluate performance and learning in complex environments. Perform. Improv. 2004, 43, 8–15. [Google Scholar] [CrossRef]
- Yoshida, T. Health Education and Nutrition Education (4) Health education evaluation and health promotion. Jpn. J. Clin. Nutr. 1994, 85, 853–859. [Google Scholar]
- Green, L.W.; Kreuter, M.W. Health Program Planning: An Educational and Ecological Approach, 4th ed.; McGraw-Hill Higher Education: New York, NY, USA, 2005. [Google Scholar]
- Yoshida, T. PRECEDE/PROCEED Model. Health Care 1992, 34, 870–875. [Google Scholar]
- Kutcher, S.; Wei, Y.; Coniglio, C. Mental Health Literacy: Past, Present, and Future. Can. J. Psychiatry 2016, 61, 154–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mcluckie, A.; Kutcher, S.; Wei, Y.; Weaver, C. Sustained improvements in students’ mental health literacy with use of a mental health curriculum in Canadian schools. BMC Psychiatry 2014, 14, 379. [Google Scholar] [CrossRef] [Green Version]
- Milin, R.; Kutcher, S.; Lewis, S.P.; Walker, S.; Wei, Y.; Ferrill, N.; Armstrong, M.A. Impact of a Mental Health Curriculum on Knowledge and Stigma Among High School Students: A Randomized Controlled Trial. J. Am. Acad. Child Adolesc. Psychiatry 2016, 55, 383–391.e1. [Google Scholar] [CrossRef]
- Swartz, K.; Musci, R.J.; Beaudry, M.B.; Heley, K.; Miller, L.; Alfes, C.; Townsend, L.; Thornicroft, G.; Wilcox, H.C. School-Based Curriculum to Improve Depression Literacy Among US Secondary School Students: A Randomized Effectiveness Trial. Am. J. Public Health 2017, 107, 1970–1976. [Google Scholar] [CrossRef]
- Patafio, B.; Miller, P.; Baldwin, R.; Taylor, N.; Hyder, S. A systematic mapping review of interventions to improve adolescent mental health literacy, attitudes and behaviours. Early Interv. Psychiatry 2021, 15, 1470–1501. [Google Scholar] [CrossRef]
- Beaudry, M.B.; Swartz, K.; Miller, L.; Schweizer, B.; Glazer, K.; Wilcox, H. Effectiveness of the Adolescent Depression Awareness Program (ADAP) on Depression Literacy and Mental Health Treatment. J. Sch. Health 2019, 89, 165–172. [Google Scholar] [CrossRef]
- Solmi, M.; Radua, J.; Olivola, M.; Croce, E.; Soardo, L.; Salazar de Pablo, G.; Il Shin, J.; Kirkbride, J.B.; Jones, P.; Kim, J.H.; et al. Age at onset of mental disorders worldwide: Large-scale meta-analysis of 192 epidemiological studies. Mol. Psychiatry 2021, 27, 281–295. [Google Scholar] [CrossRef]
- Ojio, Y.; Ohnuma, K.; Miki, T.; Sasaki, T. Development of a mental health literacy program for secondary school students in Japan. In School Mental Health: Global Challenges and Opportunities; Weist, M.D., Kutcher, S., Wei, Y., Eds.; Cambridge University Press: Cambridge, UK, 2015; pp. 139–150. [Google Scholar] [CrossRef]
- Sanita. Available online: https://sanita-mentale.jp/ (accessed on 17 June 2022).
- Ojio, Y.; Mori, R.; Matsumoto, K.; Nemoto, T.; Sumiyoshi, T.; Fujita, H.; Morimoto, T.; Nishizono-Maher, A.; Fuji, C.; Mizuno, M. Innovative approach to adolescent mental health in Japan: School-based education about mental health literacy. Early Interv. Psychiatry 2021, 15, 174–182. [Google Scholar] [CrossRef] [PubMed]
- MEXT: Ministry of Education, Culture, Sports, Science, and Technology. Gakushûshidouyouryou Koutougakko Gakushûshidouyouryou Kaisetsu Hokentaiikuhen Taiikuhen. 2018. Available online: http://www.mext.go.jp/component/a_menu/education/micro_detail/__icsFiles/afieldfile/2019/03/28/1407073_07_1_1.pdf (accessed on 9 May 2022). (In Japanese).
- Tanaka, G. Development of the Mental Illness and Disorder Understanding Scale. Int. J. Jpn. Sociol. 2003, 12, 95–107. [Google Scholar] [CrossRef]
- Evans-Lacko, S.; Rose, D.; Little, K.; Flach, C.; Rhydderch, D.; Henderson, C.; Thornicroft, G. Development and psychometric properties of the reported and intended behaviour scale (RIBS): A stigma-related behaviour measure. Epidemiol. Psychiatr. Sci. 2011, 20, 263–271. [Google Scholar] [CrossRef]
- Yamaguchi, S.; Koike, S.; Watanabe, K.-I.; Ando, S. Development of a Japanese version of the reported and intended behaviour scale: Reliability and validity. Psychiatry Clin. Neurosci. 2014, 68, 448–455. [Google Scholar] [CrossRef]
- Corrigan, P.W.; Shapiro, J.R. Measuring the impact of programs that challenge the public stigma of mental illness. Clin. Psychol. Rev. 2010, 30, 907–922. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Australian Government Department of Health, MindMatters. Available online: https://www1.health.gov.au/internet/publications/publishing.nsf/Content/suicide-prevention-activities-evaluation~positioning-the-nspp~mindmatters (accessed on 23 July 2022).
- TeenMentalHealth.org. School Mental Health The Curriculum Guide. Available online: https://mhlcurriculum.org/about-the-guide/download-the-guide/ (accessed on 23 July 2022).
- Neil, A.L.; Christensen, H. Efficacy and effectiveness of school-based prevention and early intervention programs for anxiety. Clin. Psychol. Rev. 2009, 29, 208–215. [Google Scholar] [CrossRef]
- Sekizaki, R.; Nemoto, T.; Tsujino, N.; Takano, C.; Yoshida, C.; Yamaguchi, T.; Katagiri, N.; Ono, Y.; Mizuno, M. School mental healthcare services using internet-based cognitive behaviour therapy for young male athletes in Japan. Early Interv. Psychiatry 2019, 13, 79–85. [Google Scholar] [CrossRef] [Green Version]
- Veltro, F.; Latte, G.; Ialenti, V.; Bonanni, E.; Di Padua, P.; Gigantesco, A. Effectiveness of psycho-educational intervention to promote mental health focused on emotional intelligence in middle-school. Ann. Dell’Istituto Super. Di Sanita 2020, 56, 66–71. [Google Scholar] [CrossRef]
- Japan Society of School Health. Survey report on the usage status of the infirmary in 2016. Available online: https://www.gakkohoken.jp/book/ebook/ebook_H290080/index_h5.html#1 (accessed on 27 June 2022).
- United Nations Children’s Fund (UNICEF). World at large. In Worlds of Influence: Understanding What Shapes Child Well-Being in Rich Countries; United Nations Children’s Fund (UNICEF): New York, NY, USA, 2020; pp. 34–55. [Google Scholar]
- Takubo, Y.; Nemoto, T.; Iwai, M.; Kashima, M.; Yamaguchi, E.; Maruyama, A.; Miura, S.; Saito, H.; Tsujino, N.; Mizuno, M. Demographic and clinical characteristics of foreign nationals accessing psychiatric services in Japan: A multicentre study in a metropolitan area. BMC Psychiatry 2020, 20, 569. [Google Scholar] [CrossRef]
- Hetrick, S.E.; Bailey, A.P.; Smith, K.E.; Malla, A.; Mathias, S.; Singh, S.P.; O’Reilly, A.; Verma, S.K.; Benoit, L.; Fleming, T.M.; et al. Integrated (one-stop shop) youth health care: Best available evidence and future directions. Med. J. Aust. 2017, 207, S5–S18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uchino, T.; Kotsuji, Y.; Kitano, T.; Shiozawa, T.; Iida, S.; Aoki, A.; Iwai, M.; Shirahata, M.; Seki, A.; Mizuno, M.; et al. An integrated youth mental health service in a densely populated metropolitan area in Japan: Clinical case management bridges the gap between mental health and illness services. Early Interv. Psychiatry 2022, 16, 568–575. [Google Scholar] [CrossRef] [PubMed]
- Demetrios, K.; Roger, L. Confounding by Indication in Clinical Research. JAMA. 2016, 316, 1818–1819. [Google Scholar] [CrossRef]
- Issa, D.; Radley, S.; Jessica, P.; Mei, C.; Vasileia, V.; Haseeb, J.; Jeremy, R.; Thomas, T.; Georgios, K. Do observational studies using propensity score methods agree with randomized trials? A systematic comparison of studies on acute coronary syndromes. Eur. Heart J. 2012, 33, 1893–1901. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Class | Aims and Learning Activities |
|---|---|
| 1 (50 min) | Aims:
|
| 2 (50 min) | Aims:
|
| 3 (50 min) | Aims:
|
| Sanita [26]. | |
| MHL Group n = 50 | Control Group n = 66 | Statistical Values (a) | ||
|---|---|---|---|---|
| Sex, female, n (%) | 25 (50.0) | 36 (54.5) | χ2 = 0.24 | p = 0.63 |
| MIDUS, mean (SD) | 19.40 (6.65) | 21.00 (6.62) | t = −1.29 | p = 0.20 |
| RIBS-J future, mean (SD) | 15.02 (3.24) | 14.17 (3.09) | t = 1.44 | p = 0.15 |
| Behavioural experiences of | ||||
| “Talking to family”, n (%) | 11 (22.0) | 6 (9.1) | χ2 = 3.79 | p = 0.05 |
| “Visiting a website”, n (%) | 6 (12.0) | 8 (12.1) | χ2 = 0.00 | p = 0.98 |
| “Talking to a friend”, n (%) | 6 (12.0) | 5 (7.6) | χ2 = 0.65 | p = 0.42 |
| “Consulting someone”, n (%) | 3 (6.0) | 4 (6.1) | χ2 = 0.00 | p = 0.99 |
| MHL Group Mean ± SD (Effect Size) (a) | Control Group Mean ± SD (Effect Size) (a) | Main Effect of Time | Main Effect of Group (b) | Time × Group Interaction (b) | |
|---|---|---|---|---|---|
| B [95% CI] p Value | B [95% CI] p Value | B [95% CI] p Value | |||
| MIDUS | |||||
| Baseline | 19.40 ± 6.65 | 21.00 ± 6.62 | 0 (ref) | 1.60 [−9.65,12.85] p = 0.780 | 0 (ref) |
| Post-test | 11.00 ± 5.88 (1.34) | 19.95 ± 7.34 (0.15) | −8.40 [−10.07, −6.73] p < 0.001 | 7.36 [5.14,9.57] p < 0.001 | |
| 3-month follow-up | 13.26 ± 5.80 (0.98) | 19.05 ± 7.60 (0.27) | −6.14 [−7.81, −4.47] p < 0.001 | 4.19 [1.97, 6.41] p < 0.001 | |
| RIBS-J future | |||||
| Baseline | 15.02 ± 3.24 | 14.17 ± 3.09 | 0 (ref) | −0.85 [−5.97,4.26] p = 0.743 | 0 (ref) |
| Post-test | 17.22 ± 2.67 (0.74) | 14.52 ± 3.35 (0.11) | 2.20 [1.45, 2.96] p < 0.001 | −1.85 [−2.85, −0.85] p < 0.001 | |
| 3-month follow-up | 16.86 ± 2.66 (0.62) | 15.29 ± 3.21 (0.36) | 1.84 [1.85, 2.60] p < 0.001 | −0.72 [−1.72, 0.28] p = 0.158 |
| MHL Group Number (Proportion) | Control Group Number (Proportion) | Main Effect of Time | Main Effect of Group (a) | Time × Group Interaction (a) | |
|---|---|---|---|---|---|
| Odds Ratio [95% CI] p Value | Odds Ratio [95% CI] p Value | Odds Ratio [95% CI] p Value | |||
| “Talking to family” | |||||
| Baseline | 11 (22.0) | 6 (9.1) | 0 (ref) | 2.82 [0.05, 156.41] p = 0.612 | 0 (ref) |
| Post-test | 21 (42.0) | 11 (16.7) | 0.39 [0.19, 0.78] p = 0.008 | 1.28 [0.43, 3.86] p = 0.656 | |
| 3-month follow-up | 13 (26.0) | 12 (18.2) | 0.80 [0.39, 1.67] p = 0.555 | 0.56 [0.18, 1.71] p = 0.309 | |
| “Visiting a website” | |||||
| Baseline | 6 (12.0) | 8 (12.1) | 0 (ref) | 0.99 [0.02, 42.37] p = 0.995 | 0 (ref) |
| Post-test | 17 (34.0) | 13 (19.7) | 0.27 [0.13, 0.53] p < 0.001 | 2.12 [0.84, 5.39] p = 0.112 | |
| 3-month follow-up | 6 (12.0) | 10 (15.2) | 1.00 [0.46, 2.17] p = 0.100 | 0.77 [0.28, 2.11] p = 0.613 | |
| “Talking to a friend” | |||||
| Baseline | 6 (12.0) | 5 (7.6) | 0 (ref) | 1.66 [0.44, 63.26] p = 0.783 | 0 (ref) |
| Post-test | 18 (36.0) | 8 (12.1) | 0.24 [0.11, 0.52] p< 0.001 | 2.45 [0.79, 7.63] p = 0.121 | |
| 3-month follow-up | 10 (20.0) | 8 (12.1) | 0.55 [0.25, 1.20] p = 0.132 | 1.09 [0.34, 3.46] p = 0.884 | |
| “Consulting someone” | |||||
| Baseline | 3 (6.0) | 4 (6.1) | 0 (ref) | 0.99 [0.06, 15.78] p = 0.994 | 0 (ref) |
| Post-test | 4 (8.0) | 7 (10.6) | 0.73 [0.26, 2.10] p = 0.563 | 0.74 [0.19, 2.92] p = 0.667 | |
| 3-month follow-up | 2 (4.0) | 4 (6.1) | 1.53 [0.44, 5.35] p = 0.502 | 0.65 [0.14, 3.17] p = 0.595 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mori, R.; Uchino, T.; Mizuno, M.; Yamaguchi, T.; Katagiri, N.; Nemoto, T. Effectiveness of a Comprehensive Mental Health Literacy Educational Programme for Junior High School Students: A Randomised Controlled Trial Examining Changes in Their Knowledge, Attitudes, and Behaviour. J. Pers. Med. 2022, 12, 1281. https://doi.org/10.3390/jpm12081281
Mori R, Uchino T, Mizuno M, Yamaguchi T, Katagiri N, Nemoto T. Effectiveness of a Comprehensive Mental Health Literacy Educational Programme for Junior High School Students: A Randomised Controlled Trial Examining Changes in Their Knowledge, Attitudes, and Behaviour. Journal of Personalized Medicine. 2022; 12(8):1281. https://doi.org/10.3390/jpm12081281
Chicago/Turabian StyleMori, Ryoichi, Takashi Uchino, Masafumi Mizuno, Taiju Yamaguchi, Naoyuki Katagiri, and Takahiro Nemoto. 2022. "Effectiveness of a Comprehensive Mental Health Literacy Educational Programme for Junior High School Students: A Randomised Controlled Trial Examining Changes in Their Knowledge, Attitudes, and Behaviour" Journal of Personalized Medicine 12, no. 8: 1281. https://doi.org/10.3390/jpm12081281