
Closed-Loop Controlled Fluid Administration Systems: A Comprehensive Scoping Review

 , , , , ,
, , , , ,
Abstract
:1. Introduction
- In silico simulations—These virtual, computer-based tests measure the controller’s ability to respond accurately and robustly in simulated patients’ scenarios. An example for such a testing platform is reported by Bighamian et al. [18]. This method allows for high-throughput tests of the controller at minimal cost and time, using only a computer on existing datasets but cannot test the hardware components;
- Hardware-in-loop (HIL) testing—A testing method that incorporates hardware components in a physical, manufactured system that simulates a variety of patient scenarios, while measuring the closed-loop controlled system’s performance [19]. These systems can sometimes be merged with an in silico simulation platform [20];
- In vivo studies (animals)—Testing the entire system’s performance in a real, whole-body physiological system, with subject variability, allows for the additional validation for the system’s performance and enabling measurements of the additional relevant data, such as biochemical markers. It is also an important step towards translation to clinical use. An example of such a study was reported by Marques et al. [21]. An inherent limitation for such studies is the biological difference between testing animals and humans, which not only limits the generalizability of the results, but may undermine the performance of a system that was designed based on human data;
- Human volunteer trials—These trials have the advantage of testing the system against a true human response, thus overcoming the limitations typical of animal studies. However, ethical constraints may limit the physiological stress that can be imposed on a human volunteer. An example of such a study was reported by Hundeshagen et al. [22];
- Clinical trials—Testing of a closed-loop controlled system in a clinical setting on real patients can only be completed with a relatively mature system that has been tested by at least some of the methods described above. While it is the ultimate method to prove the system’s real-life benefits, it is more challenging to conduct in emergency scenarios. An example of a clinical trial in a surgical setting was reported by Joosten et al. [23].
2. Materials and Methods
2.1. Registration and Protocol
2.2. Eligibility Criteria
2.3. Search Strategy and Information Sources
2.4. Selection Process
2.5. Deviations from Original Protocol
- As the patent registries often include future possible uses of the described patent, references to “closed-loop systems” are often not indicative of the actual existence of such systems. Therefore, identified patent registries were used as a basis for a search of peer-reviewed publications by the first patent holder’s name in PubMed, but were not considered sufficient to describe a system by themselves;
- In order to confirm that the most updated version of each system is described, an additional PubMed search was conducted, based on the first and last authors’ name of the latest manuscript found on the system. The system’s name, if described, was also included in a search, in addition to communication with the authors themselves;
- Some of the manuscripts, which described experiments with closed-loop controlled systems, were excluded at the final step after communication with the authors clarified that further development of the systems would not be pursued., As such, the aim of this report was to provide a landscape of the foreseeable future of closed-loop fluid management;
- While the original strategy was to review the manuscripts on each system in a new-to-old fashion until all of the required data were obtained, we decided to review all of the relevant manuscripts to deepen our understanding on each system.
2.6. Data Extraction
2.7. Synthesis of Results
3. Results
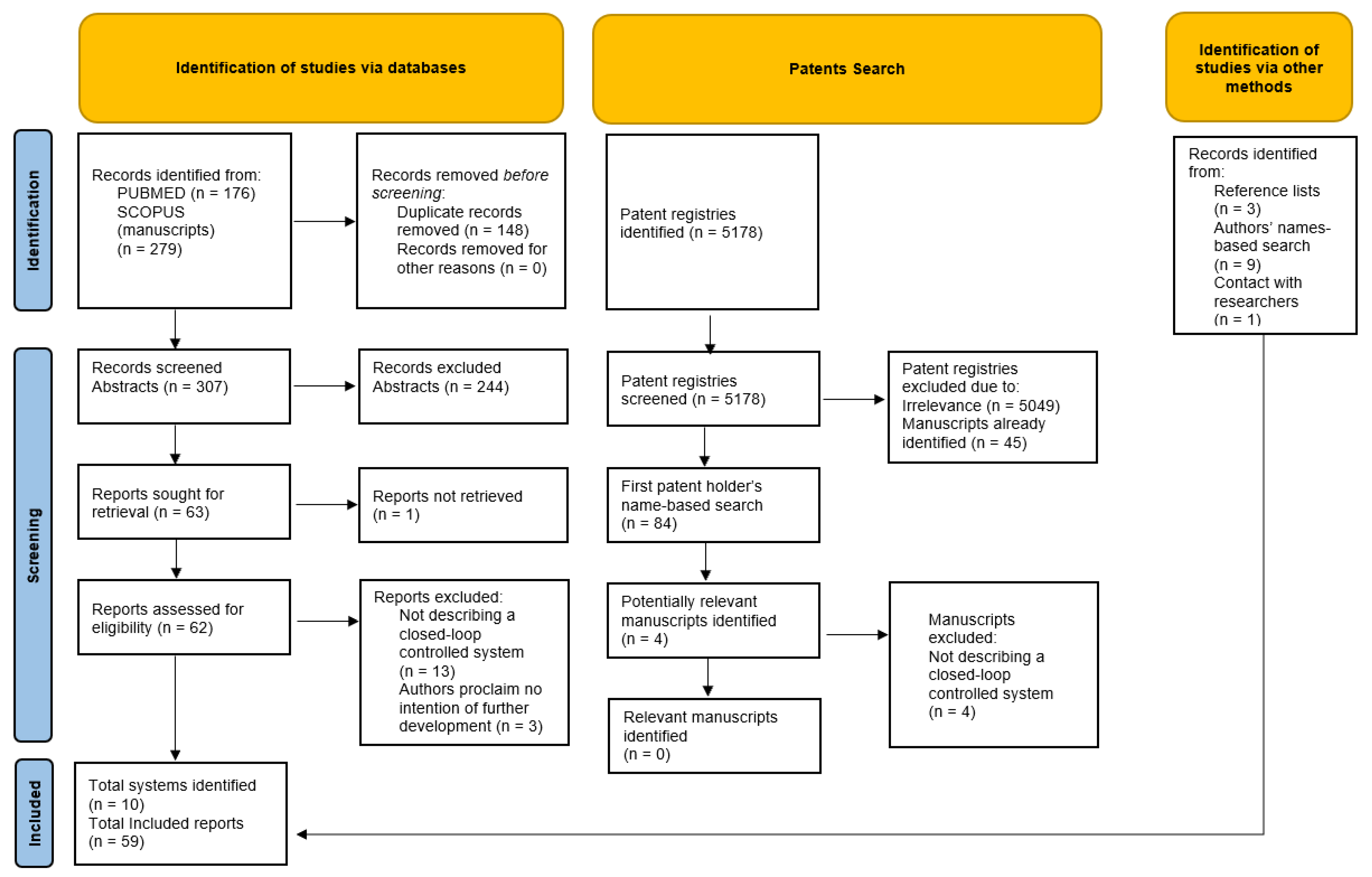
3.1. Source Selection
3.2. Synthesis of Results
3.2.1. Acumen-Assisted Fluid Management (AFM)
3.2.2. Burn Navigator
3.2.3. University of Maryland (UMD) Systems
3.2.4. Tübingen
3.2.5. Renal Guard
3.2.6. Trauma Tab
3.2.7. E-Fusion
3.2.8. Semi-Closed Loop (SCL) Infusion System
3.2.9. Adaptive Resuscitation Controller (ARC)
4. Discussion
- A model-based approach, in which predictions are made based on mathematical models aimed to mimic real physiological processes, most commonly compartmental models, describing the fluid balance between body compartments;
- A population-based approach, in which empirical data collected from clinical patient records or experiments (either human or animal) are used to create prediction formulas.
5. Future Directions
- Further maturation of the described systems as well as introduction of new ones;
- Increased adoption of closed-loop controlled fluid administration. The first scenario, where these systems can be safely operated, will probably be the operating room, where constant supervision by an anesthesiologist provides an important safety net;
- Introduction of new modalities of artificial intelligence, such as reinforcement learning [81,82] and other deep-learning modalities. While there’s increasing use of deep-learning for anesthesia and critical care-related applications [83,84], we have not identified detailed reports on deep-learning-based systems matching our inclusion criteria, meaning we have not identified a system that incorporates deep-learning-based capabilities into a CL system (or, for that matter, a DS system with a feedback loop of repeat evaluations);
- Continuing formation of a regulatory pipeline dedicated to autonomous and semi-autonomous controlled systems;
- Increased use of non-invasive sensors in closed-loop fluid administration systems, as their reliability will gradually increase [43,85], as well as artificial intelligence-based advanced sensing modalities (specifically, feature extraction), such as arterial waveform feature analysis [77,78], aimed at providing personalized resuscitation goals;
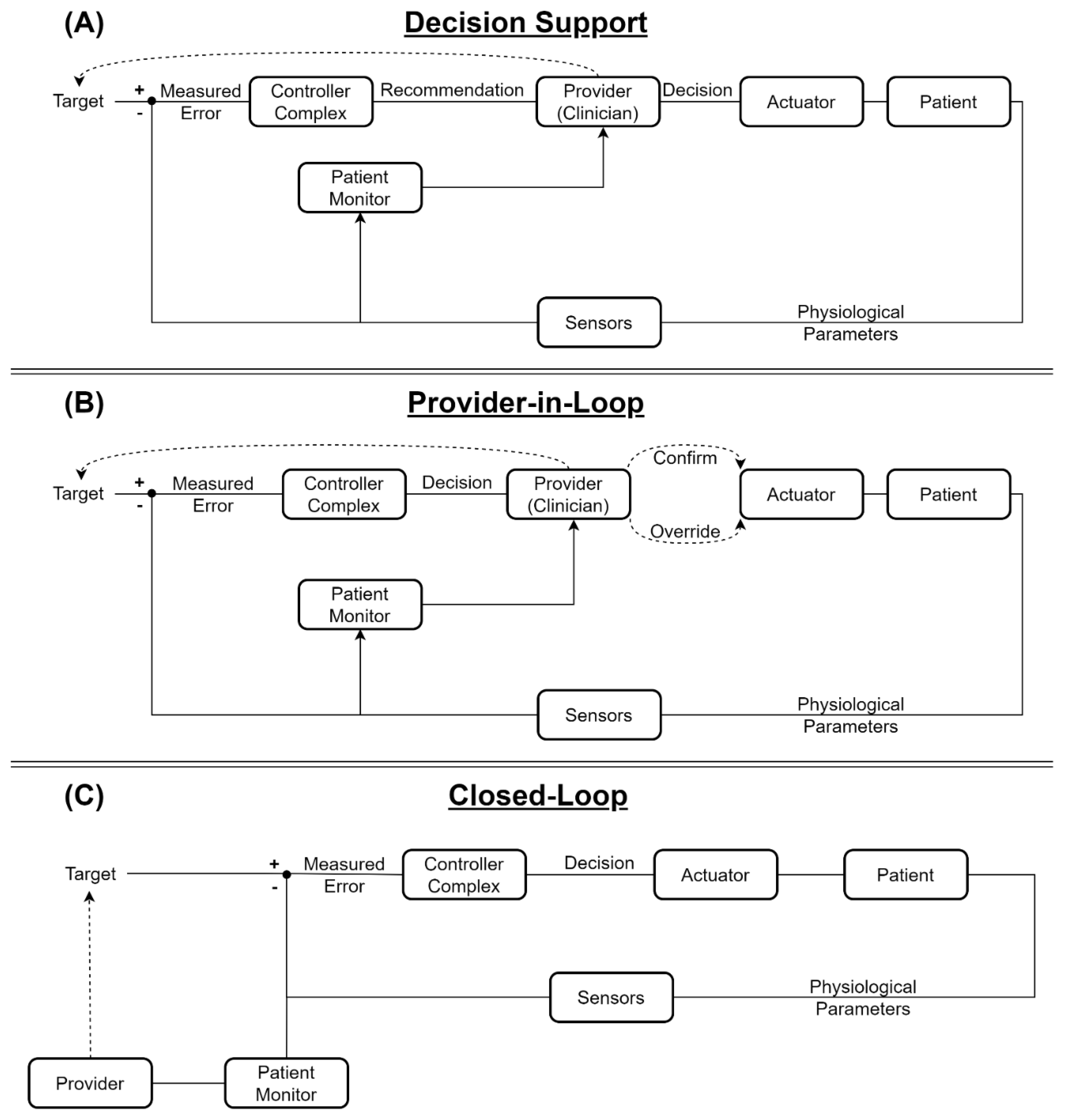
- Gradual increase in the degree of automation—from a regulatory standpoint, decision support systems are generally considered safer and easier to approve. However, they do not offer the same mental offloading and adherence as a closed-loop or even a provider-in-loop system can potentially offer. These advancements require, other than regulatory endorsement, the integration of reliable sensors and actuators (i.e., infusion pumps), so that controllers’ commands will be based on accurate data and executed precisely to ensure patient safety;
- Increase in the level of automation—as more life-support systems are being automated, supervisory controllers will be required to integrate them to accommodate the physiological interaction between the body systems. These controllers will adjust the target goals for the sub-controllers (e.g., more permissive fluid resuscitation to accommodate for the need to increase positive end-expiratory pressure), bringing composite systems to LoAs of three or four.
Supplementary Materials
Author Contributions
Funding
DoD Disclaimer
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fernández de Cañete, J.; Galindo, C.; Moral, I.G. Introduction to Control Systems. In System Engineering and Automation; Springer: Berlin/Heidelberg, Germany, 2011; pp. 137–165. [Google Scholar]
- Åström, K.J. Feedback Systems: An Introduction for Scientists and Engineers, 2nd ed.; Karl, J., Murray, R.M., Eds.; Princeton University Press: Princeton, NJ, USA, 2021. [Google Scholar]
- Cosentino, C.; Bates, D. Feedback Control in Systems Biology; CRC Press: Boca Raton, FL, USA, 2011; p. 296. [Google Scholar]
- Brown, S.A.; Kovatchev, B.P.; Raghinaru, D.; Lum, J.W.; Buckingham, B.A.; Kudva, Y.C.; Laffel, L.M.; Levy, C.J.; Pinsker, J.E.; Wadwa, R.P.; et al. Six-Month Randomized, Multicenter Trial of Closed-Loop Control in Type 1 Diabetes. N. Engl. J. Med. 2019, 381, 1707–1717. [Google Scholar] [CrossRef]
- Arnal, J.M.; Wysocki, M.; Novotni, D.; Demory, D.; Lopez, R.; Donati, S.; Granier, I.; Corno, G.; Jacques, D.G. Safety and Efficacy of a Fully Closed-Loop Control Ventilation (IntelliVent-ASV) in Sedated ICU Patients with Acute Respiratory Failure: A Prospective Randomized Crossover Study. Intensive Care Med. 2012, 38, 781–787. [Google Scholar] [CrossRef]
- Hemmerling, T.M.; Arbeid, E.; Wehbe, M.; Cyr, S.; Taddei, R.; Zaouter, C.; Reilly, C.S. Evaluation of a Novel Closed-Loop Total Intravenous Anaesthesia Drug Delivery System: A Randomized Controlled Trial. Br. J. Anaesth. 2013, 110, 1031–1039. [Google Scholar] [CrossRef] [Green Version]
- Joosten, A.; Coeckelenbergh, S.; Alexander, B.; Cannesson, M.; Rinehart, J. Feasibility of Computer-Assisted Vasopressor Infusion Using Continuous Non-Invasive Blood Pressure Monitoring in High-Risk Patients Undergoing Renal Transplant Surgery. Anaesth. Crit. Care Pain Med. 2020, 39, 623–624. [Google Scholar] [CrossRef]
- Jenkins, D.H.; Rappold, J.F.; Badloe, J.F.; Berséus, O.; Lorne Blackbourne, C.; Brohi, K.H.; Butler, F.K.; Andrew Cap, L.P.; Jay Cohen, M.; Davenport, R.; et al. THOR Position Paper on Remote Damage Control Resuscitation: Definitions, Current Practice and Knowledge Gaps Donald. Shock 2014, 41 (Suppl. S1), 3–12. [Google Scholar] [CrossRef] [Green Version]
- Chung, K.K.; Wolf, S.E.; Cancio, L.C.; Alvarado, R.; Jones, J.A.; McCorcle, J.; King, B.T.; Barillo, D.J.; Renz, E.M.; Blackbourne, L.H. Resuscitation of Severely Burned Military Casualties: Fluid Begets More Fluid. J. Trauma Acute Care Surg. 2009, 67, 231–237. [Google Scholar] [CrossRef] [Green Version]
- Otero, R.M.; Nguyen, B.; Huang, D.T.; Gaieski, D.F.; Goyal, M.; Gunnerson, K.J.; Trzeciak, S.; Sherwin, R.; Holthaus, C.V.; Osborn, T.; et al. Early Goal-Directed Therapy in Severe Sepsis and Septic Shock Revisited: Concepts, Controversies, and Contemporary Findings. Chest 2006, 130, 1579–1595. [Google Scholar] [CrossRef] [Green Version]
- Kendrick, J.; Kaye, A.; Tong, Y.; Belani, K.; Urman, R.; Hoffman, C.; Liu, H. Goal-Directed Fluid Therapy in the Perioperative Setting. J. Anaesthesiol. Clin. Pharmacol. 2019, 35, S29. [Google Scholar] [CrossRef]
- Benes, J.; Giglio, M.; Brienza, N.; Michard, F. The Effects of Goal-Directed Fluid Therapy Based on Dynamic Parameters on Post-Surgical Outcome: A Meta-Analysis of Randomized Controlled Trials. Crit. Care 2014, 18, 584. [Google Scholar] [CrossRef] [Green Version]
- Parvinian, B.; Scully, C.; Wiyor, H.; Kumar, A.; Weininger, S. Regulatory Considerations for Physiological Closed-Loop Controlled Medical Devices Used for Automated Critical Care: Food and Drug Administration Workshop Discussion Topics. Anesth. Analg. 2018, 126, 1916. [Google Scholar] [CrossRef]
- Technical Considerations for Medical Devices with Physiologic Closed-Loop Control Technology. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/technical-considerations-medical-devices-physiologic-closed-loop-control-technology (accessed on 24 May 2022).
- IEC 60601-1-10; Medical Electrical Equipment—Part 1–10: General Requirements for Basic Safety and Essential Performance–Collateral Standard: Requirements for the Development of Physiologic Closed-Loop Controllers. IEC: Geneva, Switzerland, 2013.
- Gholami, B.; Haddad, W.M.; Bailey, J.M.; Muir, W.W. Closed-Loop Control for Fluid Resuscitation: Recent Advances and Future Challenges. Front. Vet. Sci. 2021, 8, 642440. [Google Scholar] [CrossRef]
- Varvel, J.R.; Donoho, D.L.; Shafer, S.L. Measuring the Predictive Performance of Computer-Controlled Infusion Pumps. J. Pharmacokinet. Biopharm. 1992, 20, 63–94. [Google Scholar] [CrossRef]
- Bighamian, R.; Hahn, J.O.; Kramer, G.; Scully, C. Accuracy Assessment Methods for Physiological Model Selection toward Evaluation of Closed-Loop Controlled Medical Devices. PLoS ONE 2021, 16, e0251001. [Google Scholar] [CrossRef]
- Berard, D.; Vega, S.J.; Torres, S.I.H.; Polykratis, I.A.; Salinas, J.; Ross, E.; Avital, G.; Boice, E.N.; Snider, E.J. Development of the PhysioVessel: A Customizable Platform for Simulating Physiological Fluid Resuscitation. Biomed. Phys. Eng. Express 2022, 8, 035017. [Google Scholar] [CrossRef]
- Mirinejad, H.; Parvinian, B.; Ricks, M.; Zhang, Y.; Weininger, S.; Hahn, J.O.; Scully, C.G. Evaluation of Fluid Resuscitation Control Algorithms via a Hardware-in-the-Loop Test Bed. IEEE Trans. Biomed. Eng. 2020, 67, 471–481. [Google Scholar] [CrossRef]
- Marques, N.R.; Ford, B.J.; Khan, M.N.; Kinsky, M.; Deyo, D.J.; Mileski, W.J.; Ying, H.; Kramer, G.C. Automated Closed-Loop Resuscitation of Multiple Hemorrhages: A Comparison between Fuzzy Logic and Decision Table Controllers in a Sheep Model. Disaster Mil. Med. 2017, 3, 1. [Google Scholar] [CrossRef] [Green Version]
- Hundeshagen, G.; Kramer, G.C.; Ribeiro Marques, N.; Salter, M.G.; Koutrouvelis, A.K.; Li, H.; Solanki, D.R.; Indrikovs, A.; Seeton, R.; Henkel, S.N.; et al. Closed-Loop- and Decision-Assist-Guided Fluid Therapy of Human Hemorrhage. Crit. Care Med. 2017, 45, e1068. [Google Scholar] [CrossRef]
- Joosten, A.; Rinehart, J.; van der Linden, P.; Alexander, B.; Penna, C.; de Montblanc, J.; Cannesson, M.; Vincent, J.L.; Vicaut, E.; Duranteau, J. Computer-Assisted Individualized Hemodynamic Management Reduces Intraoperative Hypotension in Intermediate- And High-Risk Surgery: A Randomized Controlled Trial. Anesthesiology 2021, 135, 258–272. [Google Scholar] [CrossRef]
- Alexander, B.; Rinehart, J.; Cannesson, M.; Duranteau, J.; Joosten, A. Closed-Loop Hemodynamic Management. Best Pract. Res. Clin. Anaesthesiol. 2019, 33, 199–209. [Google Scholar] [CrossRef]
- Peters, M.D.J.; Marnie, C.; Tricco, A.C.; Pollock, D.; Munn, Z.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Khalil, H. Updated Methodological Guidance for the Conduct of Scoping Reviews. JBI Evid. Synth. 2020, 18, 2119–2126. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Libert, N.; Chenegros, G.; Harrois, A.; Baudry, N.; Cordurie, G.; Benosman, R.; Vicaut, E.; Duranteau, J. Performance of Closed-Loop Resuscitation of Haemorrhagic Shock with Fluid Alone or in Combination with Norepinephrine: An Experimental Study. Ann. Intensive Care 2018, 8, 89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Libert, N.; Chenegros, G.; Harrois, A.; Baudry, N.; Decante, B.; Cordurie, G.; Benosman, R.; Mercier, O.; Vicaut, E.; Duranteau, J. Performance of Closed-Loop Resuscitation in a Pig Model of Haemorrhagic Shock with Fluid Alone or in Combination with Norepinephrine, a Pilot Study. J. Clin. Monit. Comput. 2021, 35, 835–847. [Google Scholar] [CrossRef] [PubMed]
- Markevicius, V.; Andrijauskas, A.; Navikas, D.; Dubauskiene, N.; Porvaneckas, N.; Stankevicius, E.; Uvarovas, V.; Gelzinis, G.; Cepenas, M.; Andriukaitis, D.; et al. In Silico Testing of the Semi-Closed Loop Infusion System with a New Simulator. Elektron. Elektrotechnika 2014, 20, 19–24. [Google Scholar] [CrossRef] [Green Version]
- Markevicius, V.; Andrijauskas, A.; Navikas, D.; Svensen, C.; Porvaneckas, N.; Andriukaitis, D.; Kvederas, G.; Cincikas, D.; Andrijauskas, P. Statistically Biased Calibration Method for the Real-Time Adjustment of Noninvasive Haemoglobin Measurements in a Semiautomated Infusion System. Elektron. Elektrotechnika 2013, 19, 65–71. [Google Scholar] [CrossRef]
- Green, D.; Jonas, M.; Mills, E. Implementation of Closed-Loop-Assisted Intra-Operative Goal-Directed Fluid Therapy during Surgery. Eur. J. Anaesthesiol. 2019, 36, 303–304. [Google Scholar] [CrossRef]
- Joosten, A.; Coeckelenbergh, S.; Alexander, B.; Delaporte, A.; Cannesson, M.; Duranteau, J.; Saugel, B.; Vincent, J.-L.; van der Linden, P. Hydroxyethyl Starch for Perioperative Goal-Directed Fluid Therapy in 2020: A Narrative Review. BMC Anesthesiol. 2020, 20, 1–9. [Google Scholar] [CrossRef]
- Saugel, B.; Critchley, L.A.H.; Kaufmann, T.; Flick, M.; Kouz, K.; Vistisen, S.T.; Scheeren, T.W.L. Journal of Clinical Monitoring and Computing End of Year Summary 2019: Hemodynamic Monitoring and Management. J. Clin. Monit. Comput. 2020, 34, 207–219. [Google Scholar] [CrossRef] [Green Version]
- Joosten, A.; Jame, V.; Alexander, B.; Chazot, T.; Liu, N.; Cannesson, M.; Rinehart, J.; Barvais, L. Feasibility of Fully Automated Hypnosis, Analgesia, and Fluid Management Using 2 Independent Closed-Loop Systems during Major Vascular Surgery: A Pilot Study. Anesth. Analg. 2019, 128, E88–E92. [Google Scholar] [CrossRef]
- van Beest, P.A. Implementation of Goal-Directed Therapy Needs a Boost, and It Is Called Assisted Fluid Management. J. Clin. Monit. Comput. 2019, 33, 13–14. [Google Scholar] [CrossRef]
- Joosten, A.; Hafiane, R.; Pustetto, M.; van Obbergh, L.; Quackels, T.; Buggenhout, A.; Vincent, J.-L.; Ickx, B.; Rinehart, J. Practical Impact of a Decision Support for Goal-Directed Fluid Therapy on Protocol Adherence: A Clinical Implementation Study in Patients Undergoing Major Abdominal Surgery. J. Clin. Monit. Comput. 2019, 33, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Coeckelenbergh, S.; van der Linden, P.; Rinehart, J.; Joosten, A. Reply to: Implementation of Closed-Loop-Assisted Intra-Operative Goal-Directed Fluid Therapy during Surgery. Eur. J. Anaesthesiol. 2019, 36, 304–305. [Google Scholar] [CrossRef]
- Lilot, M.; Bellon, A.; Gueugnon, M.; Laplace, M.-C.; Baffeleuf, B.; Hacquard, P.; Barthomeuf, F.; Parent, C.; Tran, T.; Soubirou, J.-L.; et al. Comparison of Cardiac Output Optimization with an Automated Closed-Loop Goal-Directed Fluid Therapy versus Non Standardized Manual Fluid Administration during Elective Abdominal Surgery: First Prospective Randomized Controlled Trial. J. Clin. Monit. Comput. 2018, 32, 993–1003. [Google Scholar] [CrossRef]
- Joosten, A.; Delaporte, A.; Ickx, B.; Touihri, K.; Stany, I.; Barvais, L.; van Obbergh, L.; Loi, P.; Rinehart, J.; Cannesson, M.; et al. Crystalloid versus Colloid for Intraoperative Goal-Directed Fluid Therapy Using a Closed-Loop System: A Randomized, Double-Blinded, Controlled Trial in Major Abdominal Surgery. Anesthesiology 2018, 128, 55–66. [Google Scholar] [CrossRef] [PubMed]
- Joosten, A.; Coeckelenbergh, S.; Delaporte, A.; Ickx, B.; Closset, J.; Roumeguere, T.; Barvais, L.; van Obbergh, L.; Cannesson, M.; Rinehart, J.; et al. Implementation of Closed-Loop-Assisted Intra-Operative Goal-Directed Fluid Therapy during Major Abdominal Surgery: A Case-Control Study with Propensity Matching. Eur J Anaesthesiol. 2018, 35, 650–658. [Google Scholar] [CrossRef] [PubMed]
- Joosten, A.; Delaporte, A.; Cannesson, M.; Rinehart, J.; Dewilde, J.P.; van Obbergh, L.; Barvais, L. Fully Automated Anesthesia and Fluid Management Using Multiple Physiologic Closed-Loop Systems in a Patient Undergoing High-Risk Surgery. A&A Pract. 2016, 7, 260–265. [Google Scholar] [CrossRef]
- Rinehart, J.; Lilot, M.; Lee, C.; Joosten, A.; Huynh, T.; Canales, C.; Imagawa, D.; Demirjian, A.; Cannesson, M. Closed-Loop Assisted versus Manual Goal-Directed Fluid Therapy during High-Risk Abdominal Surgery: A Case-Control Study with Propensity Matching. Crit. Care 2015, 19, 94. [Google Scholar] [CrossRef] [Green Version]
- Joosten, A.; Huynh, T.; Suehiro, K.; Canales, C.; Cannesson, M.; Rinehart, J. Goal-Directed Fluid Therapy with Closed-Loop Assistance during Moderate Risk Surgery Using Noninvasive Cardiac Output Monitoring: A Pilot Study. Br. J. Anaesth. 2015, 114, 886–892. [Google Scholar] [CrossRef] [Green Version]
- Joosten, A.; Alexander, B.; Delaporte, A.; Lilot, M.; Rinehart, J.; Cannesson, M. Perioperative Goal Directed Therapy Using Automated Closed-Loop Fluid Management: The Future? Anaesthesiol. Intensive Ther. 2015, 47, 517–523. [Google Scholar] [CrossRef]
- Rinehart, J.; le Manach, Y.; Douiri, H.; Lee, C.; Lilot, M.; Le, K.; Canales, C.; Cannesson, M. First Closed-Loop Goal Directed Fluid Therapy during Surgery: A Pilot Study. Ann. Fr. D’anesth. Reanim. 2014, 33, e35–e41. [Google Scholar] [CrossRef]
- Rinehart, J.; Lee, C.; Canales, C.; Kong, A.; Kain, Z.; Cannesson, M. Closed-Loop Fluid Administration Compared to Anesthesiologist Management for Hemodynamic Optimization and Resuscitation during Surgery: An in Vivo Study. Anesth. Analg. 2013, 117, 1119–1129. [Google Scholar] [CrossRef]
- Rinehart, J.; Lee, C.; Cannesson, M.; Dumont, G. Closed-Loop Fluid Resuscitation: Robustness against Weight and Cardiac Contractility Variations. Anesth. Analg. 2013, 117, 1110–1118. [Google Scholar] [CrossRef] [PubMed]
- Miller, T.E.; Gan, T.J. Closed-Loop Systems in Anesthesia: Reality or Fantasy? Anesth. Analg. 2013, 117, 1039–1041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rinehart, J.; Liu, N.; Alexander, B.; Cannesson, M. Closed-Loop Systems in Anesthesia: Is There a Potential for Closed-Loop Fluid Management and Hemodynamic Optimization? Anesth. Analg. 2012, 114, 130–143. [Google Scholar] [CrossRef] [PubMed]
- Rinehart, J.; Chung, E.; Canales, C.; Cannesson, M. Intraoperative Stroke Volume Optimization Using Stroke Volume, Arterial Pressure, and Heart Rate: Closed-Loop (Learning Intravenous Resuscitator) versus Anesthesiologists. J. Cardiothorac. Vasc. Anesth. 2012, 26, 933–939. [Google Scholar] [CrossRef] [PubMed]
- Maheshwari, K.; Malhotra, G.; Bao, X.; Lahsaei, P.; Hand, W.R.; Fleming, N.W.; Ramsingh, D.; Treggiari, M.M.; Sessler, D.I.; Miller, T.E.; et al. Assisted Fluid Management Software Guidance for Intraoperative Fluid Administration. Anesthesiology 2021, 135, 273–283. [Google Scholar] [CrossRef] [PubMed]
- Rinehart, J.; Alexander, B.; Manach, Y.L.; Hofer, C.; Tavernier, B.; Kain, Z.N.; Cannesson, M. Evaluation of a Novel Closed-Loop Fluid-Administration System Based on Dynamic Predictors of Fluid Responsiveness: An in Silico Simulation Study. Crit. Care 2011, 15, R278. [Google Scholar] [CrossRef] [Green Version]
- Cancio, L.C.; Salinas, J.; Kramer, G.C. Protocolized Resuscitation of Burn Patients. Crit. Care Clin. 2016, 32, 599–610. [Google Scholar] [CrossRef]
- Hu, X.-Y.; Luo, P.-F.; Xia, Z.-F. Computerized Decision Support System in Fluid Resuscitation Study Design Questions. Crit. Care 2013, 41, e31–e32. [Google Scholar] [CrossRef]
- Ip, J.; James, E.; Singh, S. Computer-Assisted Decision Making in Burns Fluid Resuscitation. Crit. Care Med. 2012, 40, 1395–1396. [Google Scholar] [CrossRef]
- Liu, N.T.; Fenrich, C.A.; Serio-Melvin, M.L.; Peterson, W.C.; Cancio, L.C.; Salinas, J. The Impact of Patient Weight on Burn Resuscitation. J. Trauma Acute Care Surg. 2017, 83, S112–S119. [Google Scholar] [CrossRef] [PubMed]
- Liu, N.T.; Salinas, J.; Fenrich, C.A.; Serio-Melvin, M.L.; Kramer, G.C.; Driscoll, I.R.; Schreiber, M.A.; Cancio, L.C.; Chung, K.K. Predicting the Proportion of Full-Thickness Involvement for Any given Burn Size Based on Burn Resuscitation Volumes. J. Trauma Acute Care Surg. 2016, 81, S144–S149. [Google Scholar] [CrossRef] [PubMed]
- Mann, E.A.; Allen, D.A.; Serio-Melvin, M.L.; Wolf, S.E.; Salinas, J. Clinician Satisfaction with Computer Decision Support in the Intensive Care Unit. Dimens. Crit. Care Nurs. 2012, 31, 31–36. [Google Scholar] [CrossRef] [Green Version]
- Rizzo, J.A.; Liu, N.T.; Coates, E.C.; Serio-Melvin, M.L.; Foster, K.N.; Shabbir, M.; Pham, T.N.; Salinas, J. Initial Results of the American Burn Association Observational Multicenter Evaluation on the Effectiveness of the Burn Navigator. J. Burn. Care Res. 2022, 43, 728–734. [Google Scholar] [CrossRef] [PubMed]
- Salinas, J.; Cancio, L.C.; Renz, E.M.; Chung, K.K.; Mann-Salinas, E.A.; Serio-Melvin, M.; Wolf, S.E. The Authors Reply. Crit. Care Med. 2013, 41, e32. [Google Scholar] [CrossRef]
- Salinas, J.; Cancio, L.C.; Renz, E.M.; Chung, K.K.; Mann-Salinas, E.A.; Wade, C.E.; Serio-Melvin, M.; Wolf, S.E. The Authors Reply. Crit. Care Med. 2012, 40, 1396–1397. [Google Scholar] [CrossRef]
- Salinas, J.; Chung, K.K.; Mann, E.A.; Cancio, L.C.; Kramer, G.C.; Serio-Melvin, M.L.; Renz, E.M.; Wade, C.E.; Wolf, S.E. Computerized Decision Support System Improves Fluid Resuscitation Following Severe Burns: An Original Study. Crit. Care Med. 2011, 39, 2031–2038. [Google Scholar] [CrossRef] [Green Version]
- Bighamian, R.; Kim, C.-S.; Reisner, A.T.; Hahn, J.-O. Closed-Loop Fluid Resuscitation Control Via Blood Volume Estimation. J. Dyn. Syst. Meas. Control. Trans. ASME 2016, 138, 111005. [Google Scholar] [CrossRef]
- Jin, X.; Bighamian, R.; Hahn, J.O. Development and in Silico Evaluation of a Model-Based Closed-Loop Fluid Resuscitation Control Algorithm. IEEE Trans. Biomed. Eng. 2019, 66, 1905–1914. [Google Scholar] [CrossRef]
- Alsalti, M.; Tivay, A.; Jin, X.; Kramer, G.C.; Hahn, J.O. Design and in Silico Evaluation of a Closed-Loop Hemorrhage Resuscitation Algorithm with Blood Pressure as Controlled Variable. J. Dyn. Syst. Meas. Control. Trans. ASME 2022, 144, 021001. [Google Scholar] [CrossRef]
- Klingert, W.; Peter, J.; Thiel, C.; Thiel, K.; Rosenstiel, W.; Klingert, K.; Grasshoff, C.; Königsrainer, A.; Schenk, M. Fully Automated Life Support: An Implementation and Feasibility Pilot Study in Healthy Pigs. Intensive Care Med. 2018, 6, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arbel, Y.; Ben-Assa, E.; Halkin, A.; Keren, G.; Schwartz, A.L.; Havakuk, O.; Leshem-Rubinow, E.; Konigstein, M.; Steinvil, A.; Abramowitz, Y.; et al. Forced Diuresis with Matched Hydration in Reducing Acute Kidney Injury during Transcatheter Aortic Valve Implantation (Reduce-AKI): Study Protocol for a Randomized Sham-Controlled Trial. Trials 2014, 15, 262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arbel, Y.; Ben-Assa, E.; Puzhevsky, D.; Litmanowicz, B.; Galli, N.; Chorin, E.; Halkin, A.; Sadeh, B.; Konigstein, M.; Bassat, O.K.-B.; et al. Forced Diuresis with Matched Hydration during Transcatheter Aortic Valve Implantation for Reducing Acute Kidney Injury: A Randomized, Sham-Controlled Study (REDUCE-AKI). Eur. Heart J. 2019, 40, 3169–3178. [Google Scholar] [CrossRef] [PubMed]
- Dorval, J.-F.; Dixon, S.R.; Zelman, R.B.; Davidson, C.J.; Rudko, R.; Resnic, F.S. Feasibility Study of the RenalGuardTM Balanced Hydration System: A Novel Strategy for the Prevention of Contrast-Induced Nephropathy in High Risk Patients. Int. J. Cardiol. 2013, 166, 482–486. [Google Scholar] [CrossRef] [PubMed]
- Ben-Haim, Y.; Chorin, E.; Hochstadt, A.; Ingbir, M.; Arbel, Y.; Khoury, S.; Halkin, A.; Finkelstein, A.; Banai, S.; Konigstein, M. Forced Diuresis with Matched Isotonic Intravenous Hydration Prevents Renal Contrast Media Accumulation. J. Clin. Med. 2022, 11, 885. [Google Scholar] [CrossRef]
- Luckraz, H.; Giri, R.; Wrigley, B.; Nagarajan, K.; Senanayake, E.; Sharman, E.; Beare, L.; Nevill, A. Reduction in Acute Kidney Injury Post Cardiac Surgery Using Balanced Forced Diuresis: A Randomized, Controlled Trial. Eur. J. Cardio-Thorac. Surg. 2021, 59, 562–569. [Google Scholar] [CrossRef]
- Luckraz, H.; Giri, R.; Wrigley, B.; Nagarajan, K.; Senanayake, E.; Sharman, E.; Beare, L.; Nevill, A. Balanced Forced-Diuresis as a Renal Protective Approach in Cardiac Surgery: Secondary Outcomes of Electrolyte Changes. J. Card. Surg. 2021, 36, 4125–4131. [Google Scholar] [CrossRef]
- Luckraz, H.; Giri, R.; Wrigley, B.; Nagarajan, K.; Senanayake, E.; Sharman, E.; Beare, L.; Nevill, A. Balanced Forced-Diuresis Compared to Control as a Reno-Protective Approach in Cardiac Surgery: Secondary Outcome of a Randomized Controlled Trial, Assessment of Neutrophil Gelatinase-Associated Lipocalin Levels. J. Cardiothorac. Surg. 2021, 16, 240. [Google Scholar] [CrossRef]
- Wang, Y.; Guo, Y. RenalGuard System and Conventional Hydration for Preventing Contrast-Associated Acute Kidney Injury in Patients Undergoing Cardiac Interventional Procedures: A Systematic Review and Meta-Analysis. Int. J. Cardiol. 2021, 333, 83–89. [Google Scholar] [CrossRef]
- Gholami, B.; Haddad, W.M.; Bailey, J.M.; Geist, B.; Ueyama, Y.; Muir, W.W. A Pilot Study Evaluating Adaptive Closed-Loop Fluid Resuscitation during States of Absolute and Relative Hypovolemia in Dogs. J. Vet. Emerg. Crit. Care 2018, 28, 436–446. [Google Scholar] [CrossRef]
- Snider, E.J.; Vega, S.J.; Ross, E.; Boice, E.N.; Berard, D.; Hernandez-Torres, S.I.; Salinas, J. Supervisory Algorithm for Autonomous Hemodynamic Management Systems. Sensors 2022, 22, 529. [Google Scholar] [CrossRef] [PubMed]
- Convertino, V.A.; Koons, N.J.; Suresh, M.R. Physiology of Human Hemorrhage and Compensation. Compr. Physiol. 2021, 11, 1531–1574. [Google Scholar] [CrossRef] [PubMed]
- Convertino, V.A.; Schauer, S.G.; Weitzel, E.K.; Cardin, S.; Stackle, M.E.; Talley, M.J.; Sawka, M.N.; Inan, O.T. Wearable Sensors Incorporating Compensatory Reserve Measurement for Advancing Physiological Monitoring in Critically Injured Trauma Patients. Sensors 2020, 20, 6413. [Google Scholar] [CrossRef] [PubMed]
- Kramer, G.C.; Dor, G.A.D.; Meador, C.; Tivay, A.; Hahn, J.-O.; Salinas, J.; Bighamian, R. A Physiological Model for Burn Injury and Resuscitation. In Proceedings of the 11th International Conference on Computer Modeling and Simulation, North Rockhampton, Australia, 16–19 January 2019; Association for Computing Machinery: New York, NY, USA, 2019; pp. 66–69. [Google Scholar]
- Tivay, A.; Kramer, G.C.; Hahn, J.O. Virtual Patient Generation Using Physiological Models through a Compressed Latent Parameterization. In Proceedings of the American Control Conference, Denver, CO, USA, 1–3 July 2020. [Google Scholar]
- Roggeveen, L.; El Hassouni, A.; Ahrendt, J.; Guo, T.; Fleuren, L.; Thoral, P.; Girbes, A.R.; Hoogendoorn, M.; Elbers, P.W. Transatlantic Transferability of a New Reinforcement Learning Model for Optimizing Haemodynamic Treatment for Critically Ill Patients with Sepsis. Artif. Intell. Med. 2021, 112, 102003. [Google Scholar] [CrossRef] [PubMed]
- Saria, S. Individualized Sepsis Treatment Using Reinforcement Learning. Nat. Med. 2018, 24, 1641–1642. [Google Scholar] [CrossRef] [PubMed]
- Wingert, T.; Lee, C.; Cannesson, M. Machine Learning, Deep Learning, and Closed Loop Devices—Anesthesia Delivery. Anesthesiol. Clin. 2021, 39, 565–581. [Google Scholar] [CrossRef]
- Singh, M.; Nath, G. Artificial Intelligence and Anesthesia: A Narrative Review. Saudi J. Anaesth. 2022, 16, 86. [Google Scholar] [CrossRef]
- Zia, J.; Kimball, J.; Rolfes, C.; Hahn, J.O.; Inan, O.T. Enabling the Assessment of Trauma-Induced Hemorrhage via Smart Wearable Systems. Sci. Adv. 2020, 6, eabb1708. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| System | AFM | Burn Navigator | UMD 2016 | CAC | Tubingen | RenalGuard | TraumaTab | E-Fusion | SCL Infusion System | ARC |
|---|---|---|---|---|---|---|---|---|---|---|
| Year last reported | 2021 | 2021 | 2016 | 2022 | 2018 | 2022 | 2021 | 2021 | 2014 | 2022 |
| Degree of automation | DS ** | DS | CL | CL | CL | CL | CL | CL | PIL | CL |
| Rationale | Population based | Population based | Model Based | Model Based | Pmcf Method | No prediction | Fuzzy Logic and “phase recognition” | Model Based | Rule based | Population based |
| Adaptivity | Yes | Yes | Yes | Yes | Partial *** | No | Yes | Yes | No | Yes |
| Inputs * | HR, MAP, SV, SVV | UO | Arterial waveform and ECG | MAP, SpHb | SBP (VNA) | UO | SBP | SVV | MAP, SpHb | MAP |
| Output | Suggestion for fluid administration | Recommended fluid rate | Infusion volume | Infusion volume | 2 mL/kg bolus | Infusion rate | Infusion rate | Infusion rate | Recommendations on fluid rate, vasopressor titration and PRBC administration | Infusion rate |
| Optimization goal | % Increase in SV following fluid bolus | 30 < UO < 50 | % Increase in EDV following fluid bolus | MAP | VNA ≤ 10 | Infusion rate = UO | SBP | SVV ≤ 13 | MAP, SpHb | Target MAP Value |
| Intended use case | GDFT for peri-operative care | Acute burn resuscitation | Hemorrhagic shock resuscitation | Hemorrhagic shock resuscitation | ICU Patient Maintenance | Forced Diuresis | Hemorrhagic shock resuscitation | Peri-operative and trauma care | Peri-operative care | Hemorrhagic shock resuscitation |
| Fluids used or simulated | Crystalloids/colloids/blood | Ringer’s Lactate | Crystalloids | Crystalloids | Crystalloids | Normal Saline | Normal Saline + Norepinephrine | Ringer’s Lactate | Crystalloids, PRBC, Adrenaline | Crystalloids/whole blood |
| Most advanced research stage | Clinical trials | Clinical trials | In silico testing | In silico testing | Large Animal Pilot Study | Clinical Trials | Large Animal pilot study | Large Animal Pilot Study | In silico testing | Hardware-in-loop |
| Regulatory Status | FDA and CE approved | FDA Approved | N/A | N/A | Unknown | CE approved, pending FDA approval | Unknown | Unknown | Unknown | N/A |
| Performance metrics provided | Agreement of user with recommendations, effectiveness of recommended boluses comparing to user-initiated | Clinical outcomes, Users’ satisfaction | Algorithm’s prediction accuracy | Varvel’s criteria | % of time spent under VNA delta threshold | Difference between measured UO and infused volume, clinical outcomes | Varvel’s criteria, clinical markers | Time to target, fluid balance | Not specified | Time to target, Fluid balance |
| Funding sources disclosed in studies | Edwards Lifesciences, NIH, ESIC, Brugmann Foundation | US DoD, NIH | US-ONR | Fulbright program, US-NSF, US-ONR | Institutional funding from B. Braun | NIHR, RenalGuard solutions, PLC Medical | French Ministry of Defense | Autonomous Health Inc. | European Union | US DoD |
| Sources | [23,24,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52] | [53,54,55,56,57,58,59,60,61,62] | [63] | [64,65] | [66] | [67,68,69,70,71,72,73,74] | [27,28] | [16,75] | [29,30] | [76] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Avital, G.; Snider, E.J.; Berard, D.; Vega, S.J.; Hernandez Torres, S.I.; Convertino, V.A.; Salinas, J.; Boice, E.N. Closed-Loop Controlled Fluid Administration Systems: A Comprehensive Scoping Review. J. Pers. Med. 2022, 12, 1168. https://doi.org/10.3390/jpm12071168
Avital G, Snider EJ, Berard D, Vega SJ, Hernandez Torres SI, Convertino VA, Salinas J, Boice EN. Closed-Loop Controlled Fluid Administration Systems: A Comprehensive Scoping Review. Journal of Personalized Medicine. 2022; 12(7):1168. https://doi.org/10.3390/jpm12071168
Chicago/Turabian StyleAvital, Guy, Eric J. Snider, David Berard, Saul J. Vega, Sofia I. Hernandez Torres, Victor A. Convertino, Jose Salinas, and Emily N. Boice. 2022. "Closed-Loop Controlled Fluid Administration Systems: A Comprehensive Scoping Review" Journal of Personalized Medicine 12, no. 7: 1168. https://doi.org/10.3390/jpm12071168