
The Diagnosis and Management of Cardiometabolic Risk and Cardiometabolic Syndrome after Spinal Cord Injury

 , , ,
, , ,
Abstract
:1. Introduction
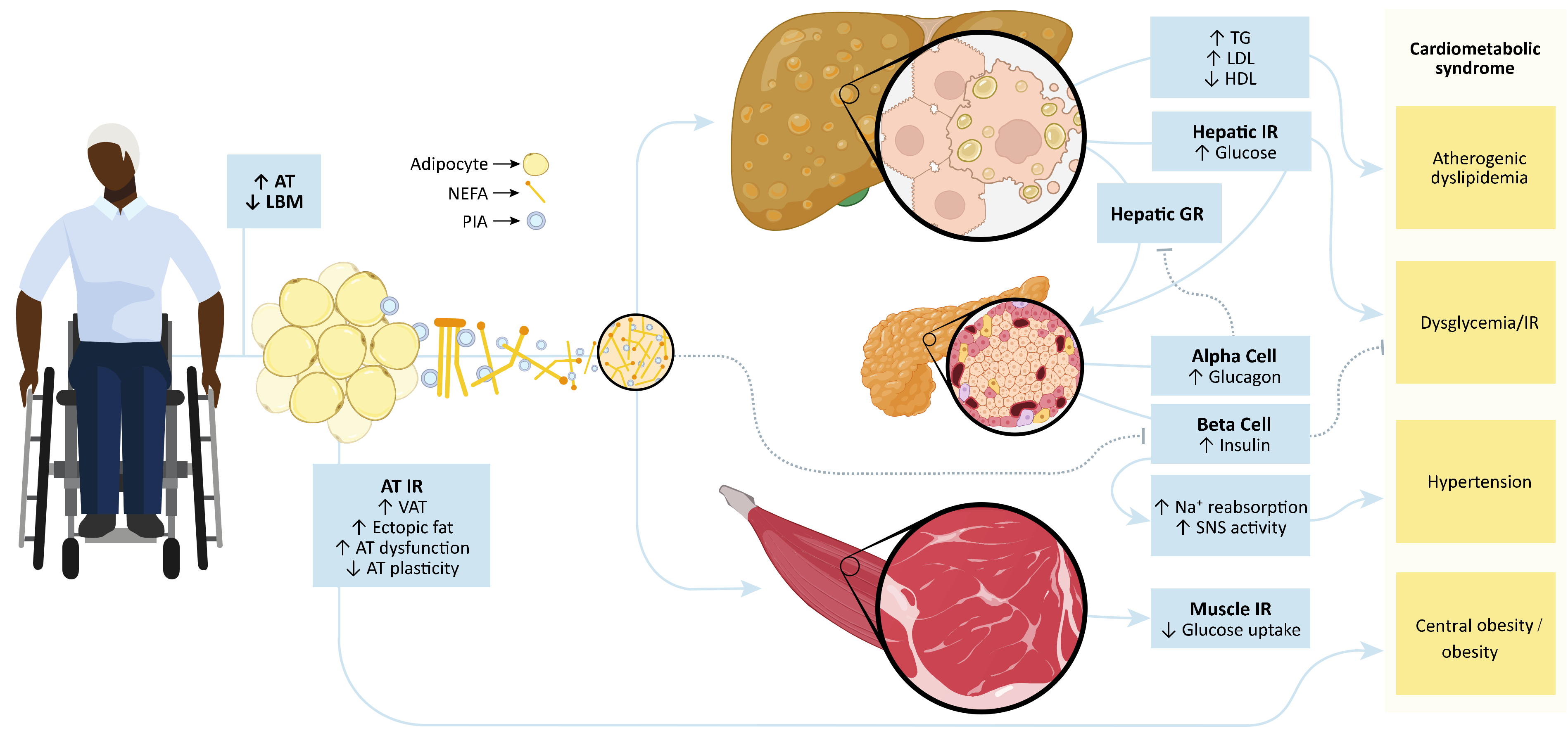
2. Mechanisms Leading to Cardiometabolic Risk
3. Obesity after SCI
4. Dyslipidemia after SCI

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cardiometabolic Risk Factor | ||||||
|---|---|---|---|---|---|---|
| Paper | Country | Sample Size (n) | SCI | Dyslipidemia | Hypertension | Dysglycemia/Insulin Resistance |
| Adriaansen et al., 2017 [103] | Netherlands | 282 | Chronic | 21.50% | ||
| Aidinoff et al., 2017 [102] | Israel | 154 | Chronic | T4-T6: 52% vs. >T4: 23.3% | ||
| Cao et al., 2020 [93] | USA | 501 | Chronic | Hypercholesterolemia: 4-year increase 32–44% | Diabetes: 4-year increase 14–17% | |
| DiPiro et al., 2018 [92] | USA | 787 | Chronic | Hypercholesterolemia: 32.3% | 43.10% | Diabetes: 15.8% |
| Gater et al., 2019 [104] | USA | 473 | Mixed | Hypercholesterolemia: 69.7% Hypertriglyceridemia: 37.1% | 55.10% | Diabetes: 49.7% |
| Gater et al., 2021 [76] | USA | 72 | Chronic | Hypercholesterolemia: 83% Hypertriglyceridemia: 33% | 43% | Hyperglycemia: 32% |
| Jörgensen et al., 2019 [75] | Sweden | 123 | Chronic | Dyslipidemia: 76% Hyperlipidemia: 60% | 33% diagnosed 55% undiagnosed | Diabetes: 16% Impaired Fasting Glucose: 27% Hyperglycemia: 15% |
| Koyuncu et al., 2017 [98] | Turkey | 269 | Mixed | High Total Cholesterol: 21% High LDL-C: 24% Hypertriglyceridemia: 31% Hypoalphalipoproteinemia: 80% | ||
| Peterson et al., 2021 [12] | USA | 9081 | Unknown | Hypercholesterolemia: 5-year incidence, SCI: 25.5% vs. Controls: 16.9%, 1.53 greater hazard for SCI vs. controls | 5-year incidence, SCI: 43.7% vs. Controls: 24.8%, 1.82 greater hazard for SCI vs. controls | |
| Solinsky et al., 2021 [84] | USA | 95 | Acute | Hypoalphalipoproteinemia: 52.4% | Hyperglycemia: 12.5% Insulin Resistance: 33.3% | |
| Tallqvist et al., 2021 [95] | Finland | 884 | Chronic | Hypercholesterolemia: 22% | 40% | |
| Ullah et al., 2018 [105] | Saudi Arabia | 24 | Acute | 75% | Diabetes: 60% | |
| Vriz et al., 2017 [106] | Italy | 57 | Chronic | 11% | ||
5. Hypertension after SCI
6. Dysglycemia and Insulin Resistance after SCI
7. Cardiometabolic Syndrome after SCI
8. Cardiovascular Disease after SCI
9. Diagnosis and Management of Cardiometabolic Risk and Syndrome after SCI
10. Diagnosis of Cardiometabolic Risk and Syndrome after SCI
11. Lifestyle Modifications to Mitigate Cardiometabolic Risk and Syndrome
12. Exercise to Reduce Cardiometabolic Risk and Syndrome after SCI
13. Dietary Patterns to Reduce Cardiometabolic Risk and Syndrome after SCI
14. Summary
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Castro, M.J.; Apple, D.F., Jr.; Hillegass, E.A.; Dudley, G.A. Influence of complete spinal cord injury on skeletal muscle cross-sectional area within the first 6 months of injury. Eur. J. Appl. Physiol. Occup. Physiol. 1999, 80, 373–378. [Google Scholar] [CrossRef] [PubMed]
- Grimby, G.; Broberg, C.; Krotkiewska, I.; Krotkiewski, M. Muscle fiber composition in patients with traumatic cord lesion. Scand. J. Rehabil. Med. 1976, 8, 37–42. [Google Scholar] [PubMed]
- Gorgey, A.; Dudley, G.A. Skeletal muscle atrophy and increased intramuscular fat after incomplete spinal cord injury. Spinal Cord 2006, 45, 304–309. [Google Scholar] [CrossRef] [PubMed]
- Zleik, N.; Weaver, F.; Harmon, R.L.; Le, B.; Radhakrishnan, R.; Jirau-Rosaly, W.D.; Craven, B.C.; Raiford, M.; Hill, J.N.; Etingen, B.; et al. Prevention and management of osteoporosis and osteoporotic fractures in persons with a spinal cord injury or disorder: A systematic scoping review. J. Spinal Cord Med. 2018, 42, 735–759. [Google Scholar] [CrossRef] [PubMed]
- Farkas, G.J.; Gorgey, A.S.; Dolbow, D.R.; Berg, A.S.; Gater, D.R. Sex dimorphism in the distribution of adipose tissue and its influence on proinflammatory adipokines and cardiometabolic profiles in motor complete spinal cord injury. J. Spinal Cord Med. 2018, 42, 430–436. [Google Scholar] [CrossRef]
- Gorgey, A.S.; Ennasr, A.N.; Farkas, G.J.; Gater, D.R. Anthropometric Prediction of Visceral Adiposity in Persons with Spinal Cord Injury. Top. Spinal Cord Inj. Rehabil. 2021, 27, 23–35. [Google Scholar] [CrossRef]
- Groah, S.L.; Nash, M.S.; Ward, E.A.; Libin, A.; Mendez, A.J.; Burns, P.; Elrod, M.; Hamm, L.F. Cardiometabolic Risk in Community-Dwelling Persons with Chronic Spinal Cord Injury. J. Cardiopulm. Rehabil. Prev. 2011, 31, 73–80. [Google Scholar] [CrossRef] [Green Version]
- Booth, F.W.; Roberts, C.K.; Laye, M.J. Lack of Exercise Is a Major Cause of Chronic Diseases. Compr. Physiol. 2012, 2, 1143–1211. [Google Scholar] [CrossRef] [Green Version]
- Lavie, C.J.; Ozemek, C.; Carbone, S.; Katzmarzyk, P.T.; Blair, S.N. Sedentary Behavior, Exercise, and Cardiovascular Health. Circ. Res. 2019, 124, 799–815. [Google Scholar] [CrossRef]
- DeVivo, M.J.; Chen, Y.; Wen, H. Cause of Death Trends among Persons with Spinal Cord Injury in the United States: 1960–2017. Arch. Phys. Med. Rehabil. 2021, 103, 634–641. [Google Scholar] [CrossRef]
- Garshick, E.; Kelley, A.; Cohen, S.A.; Garrison, A.; Tun, C.G.; Gagnon, D.; Brown, R. A prospective assessment of mortality in chronic spinal cord injury. Spinal Cord 2005, 43, 408–416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peterson, M.D.; Berri, M.; Lin, P.; Kamdar, N.; Rodriguez, G.; Mahmoudi, E.; Tate, D. Cardiovascular and metabolic morbidity following spinal cord injury. Spine J. 2021, 21, 1520–1527. [Google Scholar] [CrossRef] [PubMed]
- Després, J.-P.; Lemieux, I. Abdominal obesity and metabolic syndrome. Nature 2006, 444, 881–887. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Risk Factors; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Ash-Bernal, R.; Peterson, L. The Cardiometabolic Syndrome and Cardiovascular Disease. J. CardioMetabolic Syndr. 2006, 1, 25–28. [Google Scholar] [CrossRef]
- Grundy, S.M.; Cleeman, J.I.; Merz, C.N.B.; Brewer, H.B.; Clark, L.T.; Hunninghake, D.B.; Pasternak, R.C.; Smith, S.C.; Stone, N. Implications of Recent Clinical Trials for the National Cholesterol Education Program Adult Treatment Panel III Guidelines. J. Am. Coll. Cardiol. 2004, 44, 720–732. [Google Scholar] [CrossRef] [Green Version]
- National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation 2002, 106, 3143–3421. [Google Scholar] [CrossRef]
- Grundy, S.M.; Brewer, H.B., Jr.; Cleeman, J.I.; Smith, S.C., Jr.; Lenfant, C. Definition of Metabolic Syndrome: Report of the National Heart, Lung, and Blood Institute/American Heart Association conference on scientific issues related to definition. Circulation 2004, 109, 433–438. [Google Scholar] [CrossRef] [Green Version]
- Grundy, S.M.; Cleeman, J.I.; Daniels, S.R.; Donato, K.A.; Eckel, R.H.; Franklin, B.A.; Gordon, D.J.; Krauss, R.M.; Savage, P.J.; Smith, S.C., Jr.; et al. Diagnosis and management of the metabolic syndrome: An American Heart Association/National Heart, Lung, and Blood Institute scientific statement. Circulation 2005, 112, 2735–2752. [Google Scholar] [CrossRef] [Green Version]
- Alberti, K.G.; Zimmet, P.Z. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: Diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet. Med. 1998, 15, 539–553. [Google Scholar] [CrossRef]
- Balkau, B.; Charles, M.A. Comment on the provisional report from the WHO consultation. Diabet. Med. 1999, 16, 442–443. [Google Scholar] [CrossRef]
- Holt, R.I.G. News and Views. Diabet. Obes. Metab. 2005, 7, 618–620. [Google Scholar] [CrossRef] [PubMed]
- Alberti, K.G.M.M.; Zimmet, P.; Shaw, J. Metabolic syndrome—A new world-wide definition. A Consensus Statement from the International Diabetes Federation. Diabet. Med. 2006, 23, 469–480. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association Standards of Medical Care in Diabetes. Diabet. Care 2004, 27, s15–s35. [CrossRef] [Green Version]
- Nesto, R.W. The relation of insulin resistance syndromes to risk of cardiovascular disease. Rev. Cardiovasc. Med. 2003, 4, 11–18. [Google Scholar]
- World Health Organization. A Global Brief on Hypertension: Silent Killer, Global Public Health Crisis: World Health Day 2013; World Health Organization: Geneva, Switzerland, 2013; pp. 1–40. [Google Scholar]
- Farkas, G.J.; Gater, D.R. Energy Expenditure and Nutrition in Neurogenic Obesity following Spinal Cord Injury. J. Phys. Med. Rehabil. 2019, 2, 11–13. [Google Scholar] [CrossRef] [Green Version]
- Farkas, G.J.; Gater, D.R. Neurogenic obesity and systemic inflammation following spinal cord injury: A review. J. Spinal Cord Med. 2017, 41, 378–387. [Google Scholar] [CrossRef] [PubMed]
- Farkas, G.J.; Gorgey, A.S.; Dolbow, D.R.; Berg, A.S.; Gater, D.R. Caloric intake relative to total daily energy expenditure using a spinal cord injury-specific correction factor: An analysis by level of injury. Am. J. Phys. Med. Rehabil. 2019, 98, 947–952. [Google Scholar] [CrossRef] [PubMed]
- Farkas, G.J.; Pitot, M.A.; Berg, A.S.; Gater, D.R. Nutritional status in chronic spinal cord injury: A systematic review and meta-analysis. Spinal Cord 2018, 57, 3–17. [Google Scholar] [CrossRef]
- Farkas, G.J.; Pitot, M.A.; Gater, D.R., Jr. A systematic review of the accuracy of estimated and measured resting metabolic rate in chronic spinal cord injury. Int. J. Sport Nutr. Exerc. Metab. 2019, 29, 548–558. [Google Scholar] [CrossRef]
- Farkas, G.J.; Sneij, A.; Gater, D.R. Dietetics After Spinal Cord Injury: Current Evidence and Future Perspectives. Top. Spinal Cord Inj. Rehabil. 2021, 27, 100–108. [Google Scholar] [CrossRef]
- Farkas, G.J.; Sneij, A.; Gater, D.R. Energy Expenditure Following Spinal Cord Injury: A Delicate Balance. Top. Spinal Cord Inj. Rehabil. 2021, 27, 92–99. [Google Scholar] [CrossRef]
- Farkas, G.J.; Sneij, A.; McMillan, D.W.; Tiozzo, E.; Nash, M.S.; Gater, D.R. Energy expenditure and nutrient intake after spinal cord injury: A comprehensive review and practical recommendations. Br. J. Nutr. 2021, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Gater, D.R.; Farkas, G.J.; Tiozzo, E. Pathophysiology of Neurogenic Obesity After Spinal Cord Injury. Top. Spinal Cord Inj. Rehabil. 2021, 27, 1–10. [Google Scholar] [CrossRef]
- Sakers, A.; De Siqueira, M.K.; Seale, P.; Villanueva, C.J. Adipose-tissue plasticity in health and disease. Cell 2022, 185, 419–446. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.D.; Haymond, M.W.; Rizza, R.A.; Cryer, P.E.; Miles, J.M. Influence of body fat distribution on free fatty acid metabolism in obesity. J. Clin. Investig. 1989, 83, 1168–1173. [Google Scholar] [CrossRef] [PubMed]
- Abate, N.; Chandalia, M.; Snell, P.G.; Grundy, S.M. Adipose Tissue Metabolites and Insulin Resistance in Nondiabetic Asian Indian Men. J. Clin. Endocrinol. Metab. 2004, 89, 2750–2755. [Google Scholar] [CrossRef] [Green Version]
- Perseghin, G.; Ghosh, S.; Gerow, K.; Shulman, G.I. Metabolic Defects in Lean Nondiabetic Offspring of NIDDM Parents: A Cross-Sectional Study. Diabetes 1997, 46, 1001–1009. [Google Scholar] [CrossRef]
- Gancheva, S.; Jelenik, T.; Álvarez-Hernández, E.; Roden, M. Interorgan Metabolic Crosstalk in Human Insulin Resistance. Physiol. Rev. 2018, 98, 1371–1415. [Google Scholar] [CrossRef] [Green Version]
- Van Der Kolk, B.W.; Goossens, G.; Jocken, J.W.; Blaak, E.E. Altered skeletal muscle fatty acid handling is associated with the degree of insulin resistance in overweight and obese humans. Diabetologia 2016, 59, 2686–2696. [Google Scholar] [CrossRef] [Green Version]
- Shin, S.W.; Lee, S.J. Ectopic Fat in Insulin Resistance, Dyslipidemia, and Cardiometabolic Disease. N. Engl. J. Med. 2014, 371, 2236–2238. [Google Scholar] [CrossRef]
- Gordon, P.S.; Farkas, G.J.; Gater, D.R. Neurogenic Obesity-Induced Insulin Resistance and Type 2 Diabetes Mellitus in Chronic Spinal Cord Injury. Top. Spinal Cord Inj. Rehabil. 2021, 27, 36–56. [Google Scholar] [CrossRef] [PubMed]
- Wahl, U.; Hirsch, T. A systematic review of cardiovascular risk factors in patients with traumatic spinal cord injury. Vasa 2021, 51, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Nash, M.S.; Groah, S.L.; Gater, D.R.; Dyson-Hudson, T.A.; Lieberman, J.A.; Myers, J.; Sabharwal, S.; Taylor, A.J. Identification and Management of Cardiometabolic Risk after Spinal Cord Injury. J. Spinal Cord Med. 2019, 42, 643–677. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B.; Meigs, J.B.; Li, T.Y.; Rifai, N.; Manson, J.E. Inflammatory Markers and Risk of Developing Type 2 Diabetes in Women. Diabetes 2004, 53, 693–700. [Google Scholar] [CrossRef] [Green Version]
- Hanley, A.J.; Festa, A.; D’Agostino, R.B.; Wagenknecht, L.E.; Savage, P.J.; Tracy, R.P.; Saad, M.F.; Haffner, S.M. Metabolic and Inflammation Variable Clusters and Prediction of Type 2 Diabetes. Diabetes 2004, 53, 1773–1781. [Google Scholar] [CrossRef] [Green Version]
- Kotsis, V.; Stabouli, S.; Papakatsika, S.; Rizos, Z.; Parati, G. Mechanisms of obesity-induced hypertension. Hypertens. Res. 2010, 33, 386–393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nash, M.S.; Farkas, G.J.; Tiozzo, E.; Gater, D.R. Exercise to mitigate cardiometabolic disorders after spinal cord injury. Curr. Opin. Pharmacol. 2021, 62, 4–11. [Google Scholar] [CrossRef]
- Hoene, M.; Weigert, C. The role of interleukin-6 in insulin resistance, body fat distribution and energy balance. Obes. Rev. 2007, 9, 20–29. [Google Scholar] [CrossRef]
- Larsen, C.M.; Faulenbach, M.; Vaag, A.; Vølund, A.; Ehses, J.A.; Seifert, B.; Mandrup-Poulsen, T.; Donath, M.Y. Interleukin-1–Receptor Antagonist in Type 2 Diabetes Mellitus. N. Engl. J. Med. 2007, 356, 1517–1526. [Google Scholar] [CrossRef] [Green Version]
- Catrysse, L.; van Loo, G. Inflammation and the Metabolic Syndrome: The Tissue-Specific Functions of NF-κB. Trends Cell Biol. 2017, 27, 417–429. [Google Scholar] [CrossRef]
- Dunmore, S.J.; Brown, J.E.P. The role of adipokines in β-cell failure of type 2 diabetes. J. Endocrinol. 2012, 216, T37–T45. [Google Scholar] [CrossRef] [Green Version]
- Oda, E. The Metabolic Syndrome as a Concept of Adipose Tissue Disease. Hypertens. Res. 2008, 31, 1283–1291. [Google Scholar] [CrossRef] [Green Version]
- Heyward, V.H.; Wagner, D.R. Applied Body Composition Assessment; Human Kinetics: Champaign, IL, USA, 2004. [Google Scholar]
- Heyward, V.H. ASEP methods recommendation: Body composition assessment. J. Exerc. Physiol. Online 2001, 4, 1–12. [Google Scholar]
- World Health Organization. Body Mass Index-BMI. Available online: https://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi (accessed on 21 January 2020).
- Centers for Disease Control and Prevention. Defining Adult Overweight and Obesity. Available online: https://www.cdc.gov/obesity/adult/defining.html (accessed on 23 August 2018).
- Klein, S.; Allison, D.; Heymsfield, S.B.; Kelley, D.E.; Leibel, R.L.; Nonas, C.; Kahn, R. Waist Circumference and Cardiometabolic Risk: A Consensus Statement from Shaping America’s Health: Association for Weight Management and Obesity Prevention; NAASO, The Obesity Society; the American Society for Nutrition; and the American Diabetes Association. Obesity 2007, 15, 1061–1067. [Google Scholar] [CrossRef] [PubMed]
- Gater, D.R.; Farkas, G.J. Alterations in Body Composition After SCI and the Mitigating Role of Exercise. Physiol. Exerc. Spinal Cord Inj. 2016, 175–198. [Google Scholar] [CrossRef]
- Silveira, S.; Ledoux, T.A.; Robinson-Whelen, S.; Stough, R.; Nosek, M.A. Methods for classifying obesity in spinal cord injury: A review. Spinal Cord 2017, 55, 812–817. [Google Scholar] [CrossRef]
- Laughton, G.E.; The SHAPE SCI Research Group; Buchholz, A.C.; Ginis, K.A.M.; Goy, R.E. Lowering body mass index cutoffs better identifies obese persons with spinal cord injury. Spinal Cord 2009, 47, 757–762. [Google Scholar] [CrossRef] [Green Version]
- Ayas, N.T.; Epstein, L.J.; Lieberman, S.L.; Tun, C.G.; Larkin, E.K.; Brown, R.; Garshick, E. Predictors Of Loud Snoring In Persons with Spinal Cord Injury. J. Spinal Cord Med. 2001, 24, 30–34. [Google Scholar] [CrossRef]
- Yun, J.-H.; Chun, S.-M.; Kim, J.-C.; Shin, H.-I. Obesity cutoff values in Korean men with motor complete spinal cord injury: Body mass index and waist circumference. Spinal Cord 2018, 57, 110–116. [Google Scholar] [CrossRef]
- Shin, J.W.; Kim, T.; Lee, B.-S.; Kim, O. Factors Affecting Metabolic Syndrome in Individuals with Chronic Spinal Cord Injury. Ann. Rehabil. Med. 2022, 46, 24–32. [Google Scholar] [CrossRef]
- Inayama, T.; Higuchi, Y.; Tsunoda, N.; Uchiyama, H.; Sakuma, H. Associations between abdominal visceral fat and surrogate measures of obesity in Japanese men with spinal cord injury. Spinal Cord 2014, 52, 836–841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gorgey, A.S.; Mather, K.J.; Gater, D.R. Central adiposity associations to carbohydrate and lipid metabolism in individuals with complete motor spinal cord injury. Metabolism 2011, 60, 843–851. [Google Scholar] [CrossRef] [PubMed]
- Gorgey, A.S.; Mather, K.J.; Poarch, H.J.; Gater, D.R. Influence of motor complete spinal cord injury on visceral and subcutaneous adipose tissue measured by multi-axial magnetic resonance imaging. J. Spinal Cord Med. 2011, 34, 99–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ravensbergen, H.J.C.; Lear, S.A.; Claydon, V.E. Waist Circumference Is the Best Index for Obesity-Related Cardiovascular Disease Risk in Individuals with Spinal Cord Injury. J. Neurotrauma 2014, 31, 292–300. [Google Scholar] [CrossRef] [PubMed]
- Sumrell, R.M.; Nightingale, T.; McCauley, L.S.; Gorgey, A.S. Anthropometric cutoffs and associations with visceral adiposity and metabolic biomarkers after spinal cord injury. PLoS ONE 2018, 13, e0203049. [Google Scholar] [CrossRef]
- Gill, S.; Sumrell, R.M.; Sima, A.; Cifu, D.X.; Gorgey, A.S. Waist circumference cutoff identifying risks of obesity, metabolic syndrome, and cardiovascular disease in men with spinal cord injury. PLoS ONE 2020, 15, e0236752. [Google Scholar] [CrossRef]
- Yahiro, A.M.; Wingo, B.C.; Kunwor, S.; Parton, J.; Ellis, A.C. Classification of obesity, cardiometabolic risk, and metabolic syndrome in adults with spinal cord injury. J. Spinal Cord Med. 2019, 43, 485–496. [Google Scholar] [CrossRef]
- Dorton, M.C.; Lucci, V.-E.M.; de Groot, S.; Loughin, T.M.; Cragg, J.J.; Kramer, J.K.; Post, M.W.M.; Claydon, V.E. Evaluation of cardiovascular disease risk in individuals with chronic spinal cord injury. Spinal Cord 2020, 59, 716–729. [Google Scholar] [CrossRef]
- Mercier, H.W.; Solinsky, R.; Taylor, J.A. Relationship of cardiometabolic disease risk factors with age and spinal cord injury duration. J. Spinal Cord Med. 2022, 1–8. [Google Scholar] [CrossRef]
- Jörgensen, S.; Hill, M.; Lexell, J. Cardiovascular Risk Factors among Older Adults with Long-Term Spinal Cord Injury. PM&R 2019, 11, 8–16. [Google Scholar] [CrossRef] [Green Version]
- Gater, D.R., Jr.; Farkas, G.J.; Dolbow, D.R.; Berg, A.S.; Gorgey, A.S. Body composition and metabolic assessment after aotor complete spinal cord injury: Development of a clinically relevant equation to estimate body fat. Top. Spinal Cord Inj. Rehabil. 2021, 27, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Yoon, E.S.; Heffernan, K.S.; Jae, S.Y.; Kim, H.J.; Bunsawat, K.; Fernhall, B. Metabolically healthy obesity and subclinical atherosclerosis in persons with spinal cord injury. J. Rehabil. Med. 2018, 50, 613–618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cirnigliaro, C.M.; La Fountaine, M.F.; Hobson, J.C.; Kirshblum, S.C.; Dengel, D.R.; Spungen, A.M.; Bauman, W.A. Predicting cardiometabolic risk from visceral abdominal adiposity in persons with chronic spinal cord injury. J. Clin. Densitom. Off. J. Int. Soc. Clin. Densitom. 2021, 24, 442–452. [Google Scholar] [CrossRef] [PubMed]
- Farooq, A.; Knez, W.L.; Knez, K.; Al-Noaimi, A.; Grantham, J.; Mohamed-Ali, V. Gender Differences in Fat Distribution and Inflammatory Markers among Arabs. Mediat. Inflamm. 2013, 2013, 497324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farkas, G.J.; Gorgey, A.S.; Dolbow, D.R.; Berg, A.S.; Gater, D.R. The influence of level of spinal cord injury on adipose tissue and its relationship to inflammatory adipokines and cardiometabolic profiles. J. Spinal Cord Med. 2017, 41, 407–415. [Google Scholar] [CrossRef] [PubMed]
- Gorgey, A.S.; Gater, D.R. A Preliminary Report on the Effects of the Level of Spinal Cord Injury on the Association Between Central Adiposity and Metabolic Profile. PM&R 2011, 3, 440–446. [Google Scholar] [CrossRef]
- Gorgey, A.S.; Farkas, G.J.; Dolbow, D.R.; Khalil, R.E.; Gater, D.R. Gender Dimorphism in Central Adiposity May Explain Metabolic Dysfunction After Spinal Cord Injury. PM&R 2017, 10, 338–348. [Google Scholar] [CrossRef]
- Rankin, K.C.; O’Brien, L.C.; Segal, L.; Khan, M.R.; Gorgey, A.S. Liver Adiposity and Metabolic Profile in Individuals with Chronic Spinal Cord Injury. BioMed Res. Int. 2017, 2017, 1364818. [Google Scholar] [CrossRef]
- Solinsky, R.; Betancourt, L.; Schmidt-Read, M.; Kupfer, M.; Owens, M.; Schwab, J.M.; Dusseau, N.B.; Szlachcic, Y.; Sutherland, L.; Taylor, J.A.; et al. Acute Spinal Cord Injury Is Associated with Prevalent Cardiometabolic Risk Factors. Arch. Phys. Med. Rehabil. 2021, 103, 696–701. [Google Scholar] [CrossRef]
- Wen, H.; DeVivo, M.J.; Mehta, T.; Baidwan, N.K.; Chen, Y. The impact of body mass index on one-year mortality after spinal cord injury. J. Spinal Cord Med. 2019, 44, 563–571. [Google Scholar] [CrossRef]
- Sullivan, S.D.; Nash, M.S.; Tefara, E.; Tinsley, E.; Groah, S. Relationship Between Gonadal Function and Cardiometabolic Risk in Young Men with Chronic Spinal Cord Injury. PM&R 2017, 10, 373–381. [Google Scholar] [CrossRef]
- Abilmona, S.M.; Sumrell, R.M.; Gill, R.S.; Adler, R.A.; Gorgey, A.S. Serum testosterone levels may influence body composition and cardiometabolic health in men with spinal cord injury. Spinal Cord 2018, 57, 229–239. [Google Scholar] [CrossRef]
- Raguindin, P.F.; Bertolo, A.; Zeh, R.M.; Fränkl, G.; Itodo, O.A.; Capossela, S.; Bally, L.; Minder, B.; Brach, M.; Eriks-Hoogland, I.; et al. Body Composition According to Spinal Cord Injury Level: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 3911. [Google Scholar] [CrossRef] [PubMed]
- Graupensperger, S.; Sweet, S.N.; Evans, M.B. Multimorbidity of overweight and obesity alongside anxiety and depressive disorders in individuals with spinal cord injury. J. Spinal Cord Med. 2018, 44, 992–1000. [Google Scholar] [CrossRef] [PubMed]
- Wen, H.; Botticello, A.L.; Bae, S.; Heinemann, A.W.; Boninger, M.; Houlihan, B.V.; Chen, Y. Racial and Ethnic Differences in Obesity in People with Spinal Cord Injury: The Effects of Disadvantaged Neighborhood. Arch. Phys. Med. Rehabil. 2019, 100, 1599–1606. [Google Scholar] [CrossRef]
- Wen, H.; Chen, Y.; He, Y.; Bickel, C.S.; Robinson-Whelen, S.; Heinemann, A.W. Racial Differences in Weight Gain: A 5-Year Longitudinal Study of Persons with Spinal Cord Injury. Arch. Phys. Med. Rehabil. 2018, 99, 1957–1964. [Google Scholar] [CrossRef]
- DiPiro, N.D.; Murday, D.; Corley, E.H.; Krause, J.S. Prevalence of chronic health conditions and hospital utilization in adults with spinal cord injury: An analysis of self-report and South Carolina administrative billing data. Spinal Cord 2018, 57, 33–40. [Google Scholar] [CrossRef]
- Cao, Y.; DiPiro, N.; Krause, J.S. Association of Secondary Health Conditions with Future Chronic Health Conditions among Persons with Traumatic Spinal Cord Injury. Top. Spinal Cord Inj. Rehabil. 2020, 26, 283–289. [Google Scholar] [CrossRef]
- South Carolina Department of Health and Environmental Control. High Cholesterol. Available online: https://scdhec.gov/health/diseases-conditions/heart-disease-stroke/high-cholesterol (accessed on 28 April 2022).
- Tallqvist, S.; Kauppila, A.M.; Vainionpää, A.; Koskinen, E.; Bergman, P.; Anttila, H.; Hämäläinen, H.; Täckman, A.; Kallinen, M.; Arokoski, J.; et al. Prevalence of comorbidities and secondary health conditions among the Finnish population with spinal cord injury. Spinal Cord 2021. [Google Scholar] [CrossRef]
- Laatikainen, T.; Tapanainen, H.; Jousilahti, P.; Valsta, L.; Vartiainen, E. Suomalaisten Kolesterolitasot Ja Tyydyttyneen Rasvan Saanti Ylittävät Edelleen Suositukset; Finnish Institute for Health and Welfare: Helsinki, Finland, 2019. [Google Scholar]
- Walldius, G.; Jungner, I.; Kolar, W.; Holme, I.; Steiner, E. High cholesterol and triglyceride values in Swedish males and females: Increased risk of fatal myocardial infarction. First report from the AMORIS (Apolipoprotein related MOrtality RISk) study. Blood Press. Suppl. 1992, 4, 35–42. [Google Scholar]
- Koyuncu, E.; Yüzer, G.F.N.; Yenigün, D.; Özgirgin, N. The analysis of serum lipid levels in patients with spinal cord injury. J. Spinal Cord Med. 2016, 40, 567–572. [Google Scholar] [CrossRef] [PubMed]
- Sabour, H.; Latifi, S.; Soltani, Z.; Shakeri, H.; Javidan, A.N.; Ghodsi, S.-M.; Hadian, M.R.; Razavi, S.-H.E. C-reactive protein as an available biomarker determining mental component of health-related quality of life among individuals with spinal cord injury. J. Spinal Cord Med. 2016, 40, 329–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- La Fountaine, M.F.; Cirnigliaro, C.M.; Kirshblum, S.C.; McKenna, C.; Bauman, W.A. Effect of functional sympathetic nervous system impairment of the liver and abdominal visceral adipose tissue on circulating triglyceride-rich lipoproteins. PLoS ONE 2017, 12, e0173934. [Google Scholar] [CrossRef] [Green Version]
- La Fountaine, M.F.; Cirnigliaro, C.M.; Hobson, J.C.; Dyson-Hudson, T.A.; Mc Kenna, C.; Kirshblum, S.C.; Spungen, A.M.; Bauman, W.A. Establishing a threshold to predict risk of cardiovascular disease from the serum triglyceride and high-density lipoprotein concentrations in persons with spinal cord injury. Spinal Cord 2018, 56, 1051–1058. [Google Scholar] [CrossRef] [Green Version]
- Aidinoff, E.; Bluvshtein, V.; Bierman, U.; Gelernter, I.; Front, L.; Catz, A. Coronary artery disease and hypertension in a non-selected spinal cord injury patient population. Spinal Cord 2016, 55, 321–326. [Google Scholar] [CrossRef]
- Adriaansen, J.J.E.; Douma-Haan, Y.; Van Asbeck, F.W.A.; Van Koppenhagen, C.F.; De Groot, S.; Smit, C.A.; Visser-Meily, J.M.A.; Post, M.W.M. Allrisc Prevalence of hypertension and associated risk factors in people with long-term spinal cord injury living in the Netherlands. Disabil. Rehabil. 2016, 39, 919–927. [Google Scholar] [CrossRef]
- Gater, D.R., Jr.; Farkas, G.J.; Berg, A.S.; Castillo, C. Prevalence of metabolic syndrome in veterans with spinal cord injury. J. Spinal Cord Med. 2019, 42, 86–93. [Google Scholar] [CrossRef]
- Ullah, S.; Qamar, I.; Qureshi, A.Z.; Abu-Shaheen, A.; Niaz, A. Functional outcomes in geriatric patients with spinal cord injuries at a tertiary care rehabilitation hospital in Saudi Arabia. Spinal Cord Ser. Cases 2018, 4, 78. [Google Scholar] [CrossRef] [Green Version]
- Vriz, O.; Bertin, N.; Ius, A.; Bizzarini, E.; Bossone, E.; Antonini-Canterin, F. Carotid artery stiffness and development of hypertension in people with paraplegia and no overt cardiovascular disease: A 7-year follow-up study. J. Cardiovasc. Echogr. 2017, 27, 132–140. [Google Scholar] [CrossRef]
- Moussavi, R.M.; Ribas-Cardus, F.; Rintala, D.H.; Rodriguez, G.P. Dietary and serum lipids in individuals with spinal cord injury living in the community. J. Rehabil. Res. Dev. 2001, 38, 225–234. [Google Scholar]
- Schelleman, H.; Klungel, O.H.; Kromhout, D.; De Boer, A.; Stricker, B.; Verschuren, W.M.M. Prevalence and determinants of undertreatment of hypertension in the Netherlands. J. Hum. Hypertens. 2004, 18, 317–324. [Google Scholar] [CrossRef] [PubMed]
- South Carolina Department of Health and Environmental Control. State of the Heart Heart Disease in South Carolina; South Carolina Department of Health and Environmental Control: Columbia, SC, USA, 2018.
- Al-Nozha, M.M.; Abdullah, M.; Arafah, M.R.; Khalil, M.Z.; Khan, N.B.; Al-Mazrou, Y.Y.; Al-Maatouq, M.A.; Al-Marzouki, K.; Al-Khadra, A.; Nouh, M.S.; et al. Hypertension in Saudi Arabia. Saudi Med J. 2007, 28, 77. [Google Scholar] [PubMed]
- Koponen, P.; Reinikainen, J.; Tolonen, H.; Laatikainen, T.; Jousilahti, P.; Koskinen, S. Prevalence of hypertension and diabetes in Finland by different data sources. Eur. J. Public Health 2019, 29, ckz185-447. [Google Scholar] [CrossRef]
- Swedish Council on Health Technology Assessment. SBU Systematic Review Summaries. In Moderately Elevated Blood Pressure: A Systematic Review; Swedish Council on Health Technology Assessment (SBU): Stockholm, Sweden, 2004. [Google Scholar]
- Groah, S.; Weitzenkamp, D.; Sett, P.; Soni, B.; Savic, G. The relationship between neurological level of injury and symptomatic cardiovascular disease risk in the aging spinal injured. Spinal Cord 2001, 39, 310–317. [Google Scholar] [CrossRef] [PubMed]
- Hubli, M.; Gee, C.M.; Krassioukov, A.V. Refined Assessment of Blood Pressure Instability After Spinal Cord Injury. Am. J. Hypertens. 2014, 28, 173–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- West, C.R.; Popok, D.; Crawford, M.A.; Krassioukov, A.V. Characterizing the Temporal Development of Cardiovascular Dysfunction in Response to Spinal Cord Injury. J. Neurotrauma. 2015, 32, 922–930. [Google Scholar] [CrossRef] [PubMed]
- Allen, K.J.; Leslie, S.W. Autonomic Dysreflexia. In StatPearls; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2022. [Google Scholar]
- Myers, J.; Lee, M.; Kiratli, J. Cardiovascular Disease in Spinal Cord Injury. Am. J. Phys. Med. Rehabil. 2007, 86, 142–152. [Google Scholar] [CrossRef]
- Li, J.; Hunter, G.R.; Chen, Y.; McLain, A.; Smith, D.L.; Yarar-Fisher, C. Differences in Glucose Metabolism among Women with Spinal Cord Injury May Not Be Fully Explained by Variations in Body Composition. Arch. Phys. Med. Rehabil. 2018, 100, 1061–1067.e1. [Google Scholar] [CrossRef]
- State of the Heart Disease in South Carolina. Diabetes Impact in South Carolina; State of the Heart Disease in South Carolina: Columbia, SC, USA, 2020. Available online: https://scdhec.gov/sites/default/files/media/document/DISC%20Diabetes%20Impact%202020.pdf (accessed on 10 September 2021).
- Andersson, T.; Ahlbom, A.; Carlsson, S. Diabetes Prevalence in Sweden at Present and Projections for Year. PLoS ONE 2015, 10, e0143084. [Google Scholar] [CrossRef] [Green Version]
- Naeem, Z. Burden of Diabetes Mellitus in Saudi Arabia. Int. J. Health Sci. 2015, 9, V–VI. [Google Scholar] [CrossRef]
- Chen, Y.; Wen, H.; Baidwan, N.K.; DeVivo, M.J. Demographic and Health Profiles of People Living with Traumatic Spinal Cord Injury in the United States During 2015–2019: Findings from the Spinal Cord Injury Model Systems Database. Arch. Phys. Med. Rehabil. 2022, 103, 622–633. [Google Scholar] [CrossRef] [PubMed]
- Mordarska, K.; Godziejewska-Zawada, M. Diabetes in the elderly. Menopausal Rev. 2017, 16, 38–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirkman, M.S.; Briscoe, V.J.; Clark, N.; Florez, H.; Haas, L.B.; Halter, J.B.; Huang, E.S.; Korytkowski, M.T.; Munshi, M.N.; Odegard, P.S.; et al. Diabetes in Older Adults. Diabet. Care 2012, 35, 2650–2664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farkas, G.J.; Gordon, P.S.; Trewick, N.; Gorgey, A.S.; Dolbow, D.R.; Tiozzo, E.; Berg, A.S.; Gater, D.R. Comparison of Various Indices in Identifying Insulin Resistance and Diabetes in Chronic Spinal Cord Injury. J. Clin. Med. 2021, 10, 5591. [Google Scholar] [CrossRef]
- Heymsfield, S.B.; Lichtman, S.; Baumgartner, R.N.; Wang, J.; Kamen, Y.; Aliprantis, A.; Pierson, R.N. Body composition of humans: Comparison of two improved four-compartment models that differ in expense, technical complexity, and radiation exposure. Am. J. Clin. Nutr. 1990, 52, 52–58. [Google Scholar] [CrossRef]
- Saklayen, M.G. The Global Epidemic of the Metabolic Syndrome. Curr. Hypertens. Rep. 2018, 20, 12. [Google Scholar] [CrossRef] [Green Version]
- Hirode, G.; Wong, R.J. Trends in the Prevalence of Metabolic Syndrome in the United States, 2011–2016. JAMA 2020, 323, 2526–2528. [Google Scholar] [CrossRef]
- Kuk, J.L.; Ardern, C.I.; Church, T.S.; Sharma, A.M.; Padwal, R.; Sui, X.; Blair, S.N. Edmonton Obesity Staging System: Association with weight history and mortality risk. Appl. Physiol. Nutr. Metab. 2011, 36, 570–576. [Google Scholar] [CrossRef]
- Sharma, A.M.; Kushner, R.F. A proposed clinical staging system for obesity. Int. J. Obes. 2009, 33, 289–295. [Google Scholar] [CrossRef] [Green Version]
- Guo, F.; Garvey, W.T. Development of a Weighted Cardiometabolic Disease Staging (CMDS) System for the Prediction of Future Diabetes. J. Clin. Endocrinol. Metab. 2015, 100, 3871–3877. [Google Scholar] [CrossRef] [Green Version]
- Guo, F.; Moellering, D.R.; Garvey, W.T. The progression of cardiometabolic disease: Validation of a new cardiometabolic disease staging system applicable to obesity. Obesity 2013, 22, 110–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Agostino, R.B., Sr.; Vasan, R.S.; Pencina, M.J.; Wolf, P.A.; Cobain, M.; Massaro, J.M.; Kannel, W.B. General Cardiovascular Risk Profile for Use in Primary Care: The Framingham Heart Study. Circulation 2008, 117, 743–753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gander, J.; Sui, X.; Hazlett, L.J.; Cai, B.; Hébert, J.R.; Blair, S.N. Factors Related to Coronary Heart Disease Risk among Men: Validation of the Framingham Risk Score. Prev. Chronic Dis. 2014, 11, E140. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. Heart Disease Facts. Available online: https://www.cdc.gov/heartdisease/facts.htm#:~:text=Heart%20disease%20is%20the%20leading,1%20in%20every%204%20deaths (accessed on 10 September 2021).
- Weaver, F.M.; Smith, B.; LaVela, S.L.; Evans, C.T.; Ullrich, P.; Miskevics, S.; Goldstein, B.; Strayer, J.; Burns, S.P. Smoking behavior and delivery of evidence-based care for veterans with spinal cord injuries and disorders. J. Spinal Cord Med. 2011, 34, 35–45. [Google Scholar] [CrossRef] [Green Version]
- Saunders, L.L.; Krause, J.S.; Carpenter, M.J.; Saladin, M. Risk Behaviors Related to Cigarette Smoking among Persons with Spinal Cord Injury. Nicotine Tob. Res. 2013, 16, 224–230. [Google Scholar] [CrossRef]
- Saunders, L.L.; Krause, J.S.; Saladin, M.; Carpenter, M.J. Prevalence of cigarette smoking and attempts to quit in a population-based cohort with spinal cord injury. Spinal Cord 2015, 53, 641–645. [Google Scholar] [CrossRef] [PubMed]
- Ginis, K.A.M.; Latimer, A.; Arbour-Nicitopoulos, K.P.; Buchholz, A.C.; Bray, S.; Craven, B.; Hayes, K.C.; Hicks, A.L.; McColl, M.A.; Potter, P.J.; et al. Leisure Time Physical Activity in a Population-Based Sample of People with Spinal Cord Injury Part I: Demographic and Injury-Related Correlates. Arch. Phys. Med. Rehabil. 2010, 91, 722–728. [Google Scholar] [CrossRef]
- Verschuren, O.; Dekker, B.; van Koppenhagen, C.; Post, M. Sedentary Behavior in People with Spinal Cord Injury. Arch. Phys. Med. Rehabil. 2016, 97, 173. [Google Scholar] [CrossRef] [PubMed]
- Rauch, A.; for the SwiSCI Study Group; Hinrichs, T.; Oberhauser, C.; Cieza, A. Do people with spinal cord injury meet the WHO recommendations on physical activity? Int. J. Public Health 2015, 61, 17–27. [Google Scholar] [CrossRef]
- Berg-Emons, R.J.V.D.; Bussmann, J.B.; Haisma, J.A.; Sluis, T.A.; van der Woude, L.; Bergen, M.P.; Stam, H.J. A Prospective Study on Physical Activity Levels After Spinal Cord Injury During Inpatient Rehabilitation and the Year After Discharge. Arch. Phys. Med. Rehabil. 2008, 89, 2094–2101. [Google Scholar] [CrossRef]
- Frisbie, J.H.; Tun, C.G. Drinking and spinal cord injury. J. Am. Paraplegia Soc. 1984, 7, 71–73. [Google Scholar]
- Tate, D.G.; Forchheimer, M.; Krause, J.S.; Meade, M.A.; Bombardier, C.H. Patterns of alcohol and substance use and abuse in persons with spinal cord injury: Risk factors and correlates. Arch. Phys. Med. Rehabil. 2004, 85, 1837–1847. [Google Scholar] [CrossRef] [PubMed]
- Saunders, L.L.; Krause, J.S. Psychological factors affecting alcohol use after spinal cord injury. Spinal Cord 2010, 49, 637–642. [Google Scholar] [CrossRef] [PubMed]
- Krause, J.S.; Kemp, B.; Coker, J. Depression after spinal cord injury: Relation to gender, ethnicity, aging, and socioeconomic indicators. Arch. Phys. Med. Rehabil. 2000, 81, 1099–1109. [Google Scholar] [CrossRef]
- Jorge, A.; White, M.; Agarwal, N. Outcomes in socioeconomically disadvantaged patients with spinal cord injury: A systematic review. J. Neurosurg. Spine 2018, 29, 680–686. [Google Scholar] [CrossRef] [Green Version]
- Strauss, D.; DeVivo, M.; Shavelle, R.; Brooks, J.; Paculdo, D. Economic Factors and Longevity in Spinal Cord Injury: A Reappraisal. Arch. Phys. Med. Rehabil. 2008, 89, 572–574. [Google Scholar] [CrossRef] [PubMed]
- Krause, J.S.; DeVivo, M.J.; Jackson, A.B. Health status, community integration, and economic risk factors for mortality after spinal cord injury. Arch. Phys. Med. Rehabil. 2004, 85, 1764–1773. [Google Scholar] [CrossRef]
- Driussi, C.; Ius, A.; Bizzarini, E.; Antonini-Canterin, F.; D’Andrea, A.; Bossone, E.; Vriz, O. Structural and functional left ventricular impairment in subjects with chronic spinal cord injury and no overt cardiovascular disease. J. Spinal Cord Med. 2014, 37, 85–92. [Google Scholar] [CrossRef] [Green Version]
- Eysmann, S.B.; Douglas, P.S.; Katz, S.E.; Sarkarati, M.; Wei, J.Y. Left ventricular mass and diastolic filling patterns in quadriplegia and implications for effects of normal aging on the heart. Am. J. Cardiol. 1995, 75, 201–203. [Google Scholar] [CrossRef]
- Williams, A.M.; Gee, C.M.; Voss, C.; West, C.R. Cardiac consequences of spinal cord injury: Systematic review and meta-analysis. Heart 2018, 105, 217–225. [Google Scholar] [CrossRef]
- Barton, T.J.; Low, D.A.; Bakker, E.A.; Janssen, T.; de Groot, S.; van der Woude, L.; Thijssen, D.H. Traditional Cardiovascular Risk Factors Strongly Underestimate the 5-Year Occurrence of Cardiovascular Morbidity and Mortality in Spinal Cord Injured Individuals. Arch. Phys. Med. Rehabil. 2020, 102, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.-C.; Chen, Y.-C.; Liu, L.; Chen, T.-J.; Huang, W.-C.; Cheng, H.; Tung-Ping, S. Increased risk of stroke after spinal cord injury: A nationwide 4-year follow-up cohort study. Neurology 2012, 78, 1051–1057. [Google Scholar] [CrossRef] [PubMed]
- Miyatani, M.; Alavinia, M.; Szeto, M.; Moore, C.; Craven, B. Association between abnormal arterial stiffness and cardiovascular risk factors in people with chronic spinal cord injury. Eur. J. Prev. Cardiol. 2017, 24, 552–558. [Google Scholar] [CrossRef] [PubMed]
- Currie, K.D.; Hubli, M.; Macdonald, M.J.; Krassioukov, A.V. Associations between arterial stiffness and blood pressure fluctuations after spinal cord injury. Spinal Cord 2019, 57, 1057–1063. [Google Scholar] [CrossRef]
- Wahman, K.; Nash, M.; Lewis, J.; Seiger, Å.; Levi, R. Cardiovascular disease risk and the need for prevention after paraplegia determined by conventional multifactorial risk models: The Stockholm spinal cord injury study. J. Rehabil. Med. 2011, 43, 237–242. [Google Scholar] [CrossRef] [Green Version]
- Wahman, K.; Nash, M.; Lewis, J.; Seiger, Å.; Levi, R. Increased cardiovascular disease risk in Swedish persons with paraplegia: The Stockholm spinal cord injury study. J. Rehabil. Med. 2010, 42, 489–492. [Google Scholar] [CrossRef] [Green Version]
- Wilt, T.J.; Carlson, K.F.; Goldish, G.D.; MacDonald, R.; Niewoehner, C.; Rutks, I.; Shamliyan, T.; Tacklind, J.; Taylor, B.C.; Kane, R.L. Carbohydrate and lipid disorders and relevant considerations in persons with spinal cord injury. Évid. Rep. Assess. 2008, 1–95. Available online: https://pubmed.ncbi.nlm.nih.gov/18457480/ (accessed on 10 September 2021).
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update From the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef]
- Afshin, A.; Sur, P.J.; Fay, K.A.; Cornaby, L.; Ferrara, G.; Salama, J.S.; Mullany, E.C.; Abate, K.H.; Abbafati, C.; Abebe, Z.; et al. Health effects of dietary risks in 195 countries, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef] [Green Version]
- Froehlich-Grobe, K.; Nary, D.E.; VanSciver, A.; Washburn, R.A.; Aaronson, L. Truth Be Told: Evidence of Wheelchair Users’ Accuracy in Reporting Their Height and Weight. Arch. Phys. Med. Rehabil. 2012, 93, 2055–2061. [Google Scholar] [CrossRef] [Green Version]
- Froehlich-Grobe, K.; Nary, D.E.; Van Sciver, A.; Lee, J.; Little, T.D. Measuring Height without a Stadiometer. Am. J. Phys. Med. Rehabilitation 2011, 90, 658–666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bray, G.A. HEALTH HAZARDS OF OBESITY. Endocrinol. Metab. Clin. N. Am. 1996, 25, 907–919. [Google Scholar] [CrossRef]
- Cole, T. Weight-stature indices to measure underweight, overweight, and obesity. In Anthropometric Assessment of Nutritional Status; Himes, J., Ed.; Wiley Liss: New York, NY, USA, 1991; pp. 83–111. [Google Scholar]
- Gallagher, D.; Heymsfield, S.B.; Heo, M.; Jebb, S.A.; Murgatroyd, P.R.; Sakamoto, Y. Healthy percentage body fat ranges: An approach for developing guidelines based on body mass index. Am. J. Clin. Nutr. 2000, 72, 694–701. [Google Scholar] [CrossRef] [PubMed]
- Farkas, G.J.; Swartz, A.M.; Gorgey, A.S.; Berg, A.S.; Gater, D.R. Acute exercise improves glucose effectiveness but not insulin sensitivity in paraplegia. Disabil. Rehabil. 2021, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Farkas, G.J.; Gorgey, A.S.; Dolbow, D.R.; Berg, A.S.; Gater, D.R. Energy Expenditure, Cardiorespiratory Fitness, and Body Composition Following Arm Cycling or Functional Electrical Stimulation Exercises in Spinal Cord Injury: A 16-Week Randomized Controlled Trial. Top. Spinal Cord Inj. Rehabil. 2021, 27, 121–134. [Google Scholar] [CrossRef]
- Ma, Y.; de Groot, S.; Weijs, P.J.M.; Achterberg, W.; Adriaansen, J.; Janssen, T.W.J. Accuracy of bioelectrical impedance analysis and skinfold thickness in the assessment of body composition in people with chronic spinal cord injury. Spinal Cord 2021, 60, 228–236. [Google Scholar] [CrossRef]
- Bigford, G.E.; Mendez, A.J.; Betancourt, L.; Burns-Drecq, P.; Backus, D.; Nash, M.S. A lifestyle intervention program for successfully addressing major cardiometabolic risks in persons with SCI: A three-subject case series. Spinal Cord Ser. Cases 2017, 3, 17007. [Google Scholar] [CrossRef] [Green Version]
- Dolbow, D.R.; Credeur, D.P.; Lemacks, J.L.; Stokic, D.S.; Pattanaik, S.; Corbin, G.N.; Courtner, A.S. Electrically induced cycling and nutritional counseling for counteracting obesity after spinal cord injury: A pilot study. J. Spinal Cord Med. 2020, 44, 533–545. [Google Scholar] [CrossRef]
- Jacobs, P.L.; Mahoney, E.T.; Nash, M.S.; Green, B.A. Circuit resistance training in persons with complete paraplegia. J. Rehabilitation Res. Dev. 2002, 39, 21–28. [Google Scholar]
- Nash, M.S.; Jacobs, P.L.; Mendez, A.J.; Goldberg, R.B. Circuit resistance training improves the atherogenic lipid profiles of persons with chronic paraplegia. J. Spinal Cord Med. 2001, 24, 2–9. [Google Scholar] [CrossRef]
- Nash, M.S.; van de Ven, I.; van Elk, N.; Johnson, B.M. Effects of Circuit Resistance Training on Fitness Attributes and Upper-Extremity Pain in Middle-Aged Men with Paraplegia. Arch. Phys. Med. Rehabil. 2007, 88, 70–75. [Google Scholar] [CrossRef] [PubMed]
- Nash, M.S.; Kressler, J. Model Programs to Address Obesity and Cardiometabolic Disease: Interventions for Suboptimal Nutrition and Sedentary Lifestyles. Arch. Phys. Med. Rehabil. 2016, 97, S238–S246. [Google Scholar] [CrossRef] [PubMed]
- Farrow, M.; Nightingale, T.; Maher, J.; McKay, C.D.; Thompson, D.; Bilzon, J.L. Effect of Exercise on Cardiometabolic Risk Factors in Adults with Chronic Spinal Cord Injury: A Systematic Review. Arch. Phys. Med. Rehabil. 2020, 101, 2177–2205. [Google Scholar] [CrossRef]
- Bakkum, A.; Paulson, T.; Bishop, N.; Goosey-Tolfrey, V.; Stolwijk-Swã¼Ste, J.; Kuppevelt, D.; Groot, S.; Janssen, T. Effects of hybrid cycle and handcycle exercise on cardiovascular disease risk factors in people with spinal cord injury: A randomized controlled trial. J. Rehabil. Med. 2015, 47, 523–530. [Google Scholar] [CrossRef] [Green Version]
- de Zepetnek, J.O.T.; Pelletier, C.A.; Hicks, A.L.; MacDonald, M.J. Following the Physical Activity Guidelines for Adults with Spinal Cord Injury for 16 Weeks Does Not Improve Vascular Health: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2015, 96, 1566–1575. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.-I.; Taylor, J.A.; Tan, C.O.; Park, H.; Kim, J.Y.; Park, S.-Y.; Chung, K.-M.; Lee, Y.-H.; Lee, B.-S.; Jeon, J.Y. A pilot randomized controlled trial of 6-week combined exercise program on fasting insulin and fitness levels in individuals with spinal cord injury. Eur. Spine J. 2019, 28, 1082–1091. [Google Scholar] [CrossRef] [PubMed]
- Nightingale, T.E.; Walhin, J.-P.; Thompson, D.; Bilzon, J.L.J. Impact of Exercise on Cardiometabolic Component Risks in Spinal Cord–injured Humans. Med. Sci. Sports Exerc. 2017, 49, 2469–2477. [Google Scholar] [CrossRef] [Green Version]
- Bresnahan, J.J.; Farkas, G.J.; Clasey, J.L.; Yates, J.W.; Gater, D.R. Arm crank ergometry improves cardiovascular disease risk factors and community mobility independent of body composition in high motor complete spinal cord injury. J. Spinal Cord Med. 2017, 42, 272–280. [Google Scholar] [CrossRef]
- Kim, D.-I.; Lee, H.; Lee, B.-S.; Kim, J.; Jeon, J.Y. Effects of a 6-Week Indoor Hand-Bike Exercise Program on Health and Fitness Levels in People with Spinal Cord Injury: A Randomized Controlled Trial Study. Arch. Phys. Med. Rehabil. 2015, 96, 2033–2040.e1. [Google Scholar] [CrossRef]
- Li, J.; Polston, K.F.L.; Eraslan, M.; Bickel, C.S.; Windham, S.T.; McLain, A.B.; Oster, R.A.; Bamman, M.M.; Yarar-Fisher, C. A high-protein diet or combination exercise training to improve metabolic health in individuals with long-standing spinal cord injury: A pilot randomized study. Physiol. Rep. 2018, 6, e13813. [Google Scholar] [CrossRef]
- Graham, K.; Yarar-Fisher, C.; Li, J.; McCully, K.M.; Rimmer, J.H.; Powell, D.; Bickel, C.S.; Fisher, G. Effects of High-Intensity Interval Training Versus Moderate-Intensity Training on Cardiometabolic Health Markers in Individuals with Spinal Cord Injury: A Pilot Study. Top. Spinal Cord Inj. Rehabil. 2019, 25, 248–259. [Google Scholar] [CrossRef] [PubMed]
- Mogharnasi, M.; TaheriChadorneshin, H.; Papoli-Baravati, S.A.; Teymuri, A. Effects of upper-body resistance exercise training on serum nesfatin-1 level, insulin resistance, and body composition in obese paraplegic men. Disabil. Health J. 2019, 12, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Horiuchi, M.; Okita, K. Arm-Cranking Exercise Training Reduces Plasminogen Activator Inhibitor 1 in People with Spinal Cord Injury. Arch. Phys. Med. Rehabil. 2017, 98, 2174–2180. [Google Scholar] [CrossRef] [PubMed]
- Cugusi, L.; Solla, P.; Serpe, R.; Pilia, K.; Pintus, V.; Madeddu, C.; Bassareo, P.; Mercuro, G. Effects of an adapted physical training on functional status, body composition and quality of life in persons with spinal cord injury paraplegia: A pilot study. Med. Sport 2015, 68, 473–485. [Google Scholar]
- Bochkezanian, V.; Newton, R.U.; Trajano, G.S.; Blazevich, A.J. Effects of Neuromuscular Electrical Stimulation in People with Spinal Cord Injury. Med. Sci. Sports Exerc. 2018, 50, 1733–1739. [Google Scholar] [CrossRef]
- Ginis, K.A.M.; Van Der Scheer, J.W.; Latimer, A.; Barrow, A.; Bourne, C.; Carruthers, P.; Bernardi, M.; Ditor, D.S.; Gaudet, S.; De Groot, S.; et al. Evidence-based scientific exercise guidelines for adults with spinal cord injury: An update and a new guideline. Spinal Cord 2017, 56, 308–321. [Google Scholar] [CrossRef] [Green Version]
- Haisma, J.A.; Van Der Woude, L.H.V.; Stam, H.J.; Bergen, M.P.; Sluis, T.A.R.; Bussmann, J.B.J. Physical capacity in wheelchair-dependent persons with a spinal cord injury: A critical review of the literature. Spinal Cord 2006, 44, 642–652. [Google Scholar] [CrossRef]
- Berg-Emons, R.J.V.D.; Bussmann, J.B.; Stam, H.J. Accelerometry-Based Activity Spectrum in Persons with Chronic Physical Conditions. Arch. Phys. Med. Rehabil. 2010, 91, 1856–1861. [Google Scholar] [CrossRef]
- Scelza, W.M.; Kalpakjian, C.Z.; Zemper, E.D.; Tate, D.G. Perceived Barriers to Exercise in People with Spinal Cord Injury. Am. J. Phys. Med. Rehabil. 2005, 84, 576–583. [Google Scholar] [CrossRef]
- Kroll, T.; Kratz, A.; Kehn, M.; Jensen, M.P.; Groah, S.; Ljungberg, I.H.; Molton, I.R.; Bombardier, C. Perceived Exercise Self-efficacy as a Predictor of Exercise Behavior in Individuals Aging with Spinal Cord Injury. Am. J. Phys. Med. Rehabil. 2012, 91, 640–651. [Google Scholar] [CrossRef]
- Cowan, R.; Nash, M.S.; Anderson-Erisman, K. Perceived Exercise Barriers and Odds of Exercise Participation among Persons with SCI Living in High-Income Households. Top. Spinal Cord Inj. Rehabil. 2012, 18, 126–127. [Google Scholar] [CrossRef]
- Cowan, R.; Nash, M.S.; Anderson, K.D. Exercise participation barrier prevalence and association with exercise participation status in individuals with spinal cord injury. Spinal Cord 2012, 51, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Noreau, L.; Shephard, R.J.; Simard, C.; Paré, G.; Pomerleau, P. Relationship of impairment and functional ability to habitual activity and fitness following spinal cord injury. Int. J. Rehabil. Res. 1993, 16, 265–276. [Google Scholar] [CrossRef] [PubMed]
- Boninger, M.L.; Dicianno, B.E.; Cooper, R.A.; Towers, J.D.; Koontz, A.M.; Souza, A.L. Shoulder magnetic resonance imaging abnormalities, wheelchair propulsion, and gender. Arch. Phys. Med. Rehabil. 2003, 84, 1615–1620. [Google Scholar] [CrossRef]
- Alvarado, J.R.V.; Felix, E.R.; Gater, D.R. Upper Extremity Overuse Injuries and Obesity after Spinal Cord Injury. Top. Spinal Cord Inj. Rehabil. 2021, 27, 68–74. [Google Scholar] [CrossRef]
- Ballinger, D.A.; Rintala, D.H.; Hart, K.A. The relation of shoulder pain and range-of-motion problems to functional limitations, disability, and perceived health of men with spinal cord injury: A multifaceted longitudinal study. Arch. Phys. Med. Rehabil. 2000, 81, 1575–1581. [Google Scholar] [CrossRef]
- Van Hall, G.; Jensen-Urstad, M.; Rosdahl, H.; Holmberg, H.-C.; Saltin, B.; Calbet, J.A. Leg and arm lactate and substrate kinetics during exercise. Am. J. Physiol. Metab. 2003, 284, E193–E205. [Google Scholar] [CrossRef]
- McMillan, D.W.; Maher, J.L.; Jacobs, K.A.; Nash, M.S.; Gater, D.R. Exercise Interventions Targeting Obesity in Persons with Spinal Cord Injury. Top. Spinal Cord Inj. Rehabil. 2021, 27, 109–120. [Google Scholar] [CrossRef]
- Gorgey, A.S.; Dolbow, D.R.; Dolbow, J.D.; Khalil, R.K.; Gater, D.R. The effects of electrical stimulation on body composition and metabolic profile after spinal cord injury—Part II. J. Spinal Cord Med. 2014, 38, 23–37. [Google Scholar] [CrossRef] [Green Version]
- Ragnarsson, K.T. Functional electrical stimulation after spinal cord injury: Current use, therapeutic effects and future directions. Spinal Cord 2007, 46, 255–274. [Google Scholar] [CrossRef] [Green Version]
- Ragnarsson, K.T. Physiologic effects of functional electrical stimulation-induced exercises in spinal cord-injured individuals. Clin. Orthop. Relat. Res. 1988, 53–63. Available online: https://europepmc.org/article/med/3261220 (accessed on 10 September 2021).
- Rodgers, M.M.; Glaser, R.M.; Figoni, S.E.; Hooker, S.; Ezenwa, B.N.; Collins, S.R.; Mathews, T.; Suryaprasad, A.G.; Gupta, S.C. Musculoskeletal responses of spinal cord injured individuals to functional neuromuscular stimulation-induced knee extension exercise training. J. Rehabil. Res. Dev. 1991, 28, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Hooker, S.P.; Wells, C.L. Effects of low-and moderate-intensity training in spinal cord-injured persons. Med. Sci. Sports Exerc. 1989, 21, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Gorgey, A.S.; Harnish, C.R.; Daniels, J.A.; Dolbow, D.R.; Keeley, A.; Moore, J.; Gater, D.R. A report of anticipated benefits of functional electrical stimulation after spinal cord injury. J. Spinal Cord Med. 2012, 35, 107–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hjeltnes, N.; Galuska, D.; Björnholm, M.; Aksnes, A.-K.; Lannem, A.; Zierath, J.; Wallberg-Henriksson, H. Exercise-induced overexpression of key regulatory proteins involved in glucose uptake and metabolism in tetraplegic persons: Molecular mechanism for improved glucose homeostasis. FASEB J. 1998, 12, 1701–1712. [Google Scholar] [CrossRef] [PubMed]
- Figoni, S.F.; Rodgers, M.M.; Glaser, R.M.; Hooker, S.P.; Feghri, P.D.; Ezenwa, B.N.; Mathews, T.; Suryaprasad, A.G.; Gupta, S.C. Physiologic Responses of Paraplegics and Quadriplegics to Passive and Active Leg Cycle Ergometry. J. Am. Paraplegia Soc. 1990, 13, 33–39. [Google Scholar] [CrossRef]
- Arnold, P.B.; McVey, P.P.; Farrell, W.J.; Deurloo, T.M.; Grasso, A.R. Functional electric stimulation: Its efficacy and safety in improving pulmonary function and musculoskeletal fitness. Arch. Phys. Med. Rehabil. 1992, 73, 665–668. [Google Scholar]
- Barstow, T.J.; Scremin, A.M.E.; Mutton, D.L.; Kunkel, C.F.; Cagle, T.G.; Whipp, B.J. Changes in gas exchange kinetics with training in patients with spinal cord injury. Med. Sci. Sports Exerc. 1996, 28, 1221–1228. [Google Scholar] [CrossRef]
- Nash, M.S.; Bilsker, M.S.; Kearney, H.M.; Ramirez, J.N.; Applegate, B.; Green, B.A. Effects of electrically-stimulated exercise and passive motion on echocardiographically-derived wall motion and cardiodynamic functic in tetraplegic persons. Spinal Cord 1995, 33, 80–89. [Google Scholar] [CrossRef] [Green Version]
- Griffin, L.; Decker, M.; Hwang, J.; Wang, B.; Kitchen, K.; Ding, Z.; Ivy, J. Functional electrical stimulation cycling improves body composition, metabolic and neural factors in persons with spinal cord injury. J. Electromyogr. Kinesiol. 2009, 19, 614–622. [Google Scholar] [CrossRef]
- Rosety-Rodriguez, M.; Camacho, A.; Rosety, I.; Fornieles, G.; Rosety, M.A.; Diaz, A.J.; Bernardi, M.; Rosety, M.; Ordonez, F.J. Low-Grade Systemic Inflammation and Leptin Levels Were Improved by Arm Cranking Exercise in Adults with Chronic Spinal Cord Injury. Arch. Phys. Med. Rehabil. 2013, 95, 297–302. [Google Scholar] [CrossRef]
- Bigford, G.; Nash, M.S. Nutritional Health Considerations for Persons with Spinal Cord Injury. Top. Spinal Cord Inj. Rehabil. 2017, 23, 188–206. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Henson, S.L.; Jackson, A.B.; Richards, J.S. Obesity intervention in persons with spinal cord injury. Spinal Cord 2005, 44, 82–91. [Google Scholar] [CrossRef] [PubMed]
- Allison, D.J.; Beaudry, K.M.; Thomas, A.M.; Josse, A.; Ditor, D.S. Changes in nutrient intake and inflammation following an anti-inflammatory diet in spinal cord injury. J. Spinal Cord Med. 2018, 42, 768–777. [Google Scholar] [CrossRef] [PubMed]
- Nash, M.S.; Groah, S.L.; Gater, D.R.; Dyson-Hudson, T.; Lieberman, J.A.; Myers, J.; Sabharwal, S.; Taylor, A.J. Consortium for Spinal Cord Medicine Identification and Management of Cardiometabolic Risk after Spinal Cord Injury: Clinical Practice Guideline for Health Care Providers. Top. Spinal Cord Inj. Rehabil. 2018, 24, 379–423. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services and U.S. Department of Agriculture. 2020–2025 Dietary Guidelines for Americans, 9th ed.; U.S. Department of Health and Human Services and U.S. Department of Agriculture: Washington, DC, USA, 2020.
- Nightingale, T.E.; Gorgey, A.S. Predicting Basal Metabolic Rate in Men with Motor Complete Spinal Cord Injury. Med. Sci. Sports Exerc. 2018, 50, 1305–1312. [Google Scholar] [CrossRef]
- Chun, S.M.; Kim, H.-R.; Shin, H.I. Estimating the Basal metabolic rate from fat free mass in individuals with motor complete spinal cord injury. Spinal Cord 2017, 55, 844–847. [Google Scholar] [CrossRef] [Green Version]
- Buchholz, A.C.; McGillivray, C.; Pencharz, P.B. Differences in resting metabolic rate between paraplegic and able-bodied subjects are explained by differences in body composition. Am. J. Clin. Nutr. 2003, 77, 371–378. [Google Scholar] [CrossRef] [Green Version]
- Kelly, H. The classical definition of a pandemic is not elusive. Bull. World Health Organ. 2011, 89, 540–541. [Google Scholar] [CrossRef]




| International Diabetes Federation [22,23] | National Cholesterol Education Project Adult Treatment Panel III [17] | National Heart, Lung, and Blood Institute/American Heart Association [18,19] | World Health Organization [20] | European Group for the Study of Insulin Resistance [21] | ||
|---|---|---|---|---|---|---|
| Required Criteria/Emphasis | Obesity Plus, any 2 of the following risk factors | None. Any 3 of the following risk factors | None. Any 3 of the following risk factors | Impaired fasting glucose, impaired glucose tolerance (prediabetes) or type 2 diabetes mellitus, and/or insulin resistance * Plus, any 2 of the following risk factors | Insulin resistance or fasting hyperinsulinemia (>75% percentile) Plus, any 2 of the following risk factors | |
| Component Risk Factors | ||||||
| Central Obesity | Waist circumference ≥ 102 cm in US men or ≥88 cm in US women †,†† | Waist circumference ≥ 102 cm in men ‡ or ≥88 cm in women | Waist circumference ≥ 102 cm in men or ≥88 cm in women | Waist-to-hip ratio > 0.90 in men; Waist-to-hip ratio > 0.85 in women; and/or body mass index > 30 kg/m2 | Waist circumference ≥ 94 cm in men or ≥80 cm in women | |
| Dyslipidemia | Elevated triglycerides | Triglycerides ≥ 150 mg/dL, or on treatment for dyslipidemia | Triglycerides ≥ 150 mg/dL | Triglycerides ≥ 150 mg/dL, or on treatment for evaluated triglycerides | Triglycerides ≥ 150 mg/dL | Triglycerides > 150 mg/dL, HDL-C < 39 mg/dL in men and women, or on treatment for dyslipidemia |
| Reduced HDL-C | HDL-C < 40 mg/dL in men or <50 mg/dL in women, or on treatment for dyslipidemia | HDL-C < 40 mg/dL in men or <50 mg/dL in women | HDL-C < 40 mg/dL in men or <50 mg/dL in women, or on treatment for reduced HDL-C | HDL-C < 35 mg/dL in men or <39 mg/dL in women | ||
| Hypertension | Systolic blood pressure ≥ 130 or diastolic blood pressure ≥ 85 mmHg, or on treatment previously diagnosed hypertension | Systolic blood pressure ≥ 130, or diastolic blood pressure ≥ 85 mmHg | Systolic blood pressure ≥ 130, diastolic blood pressure ≥ 85 mmHg, or on treatment for or previously diagnosed with hypertension | Blood pressure ≥ 160/90 mmHg § Blood pressure ≥ 140/90 mmHg § | ≥140/90 mmHg, or on treatment for hypertension | |
| Dysglycemia | Fasting plasma glucose ≥ 100 mg/dL, or previously diagnosed type 2 diabetes mellitus | Fasting plasma glucose ≥ 100 mg/dL **/≥ 110 mg/dL ** | Fasting plasma glucose ≥ 100 mg/dL, or on treatment elevated glucose | Impaired fasting glucose, impaired glucose tolerance (prediabetes), or type 2 diabetes mellitus | Fasting glucose ≥ 110 mg/dL (but not diabetes, <126 mg/dL) | |
| Insulin Resistance | None. | None. | None. | Insulin resistance * | Insulin resistance or fasting hyperinsulinemia (>75% percentile) | |
| Other | None. | None. | None. | Microalbuminuria: urinary albumin excretion rate ≥ 20 µg/min, or albumin:creatinine ratio ≥ 20 mg/g | None. | |
| Body Mass Index (kg/m2) | Waist Circumference (cm) | |||
|---|---|---|---|---|
| Classification | Threshold/Range | Classification | Gender | Threshold |
| Underweight | <18.5 | Obese | Men | >102 |
| Normal | 18.5–24.9 | |||
| Pre-Obesity/Overweight * | 25.0–29.9 | |||
| Obese | ≥30 | Women | >88 | |
| Obese I | 30.0–34.9 | |||
| Obese II | 35.0–39.9 | |||
| Obese III | ≥40 | |||
| Author (Year) | BMI Cutoff (kg/m2) | WC Cutoff (cm) | Nationality | Sample Size (n) | Age (y) | Sex (% Male) | ISNCSCI * | Injury Duration (y) | Method of Calculation |
|---|---|---|---|---|---|---|---|---|---|
| Ayas et al. [63] (2001) | >25.3 | N/A | American | 197 | 51 ± 15 | NP | T, P/C, I | 18 ± 13 | Sample median |
| Inayama et al. [66] (2014) | >22.5 | >81.3 | Japanese | 74 | 46 ± 14 | 100 | T, P/C, I | 15 ± 10 | Non-LR |
| Laughton et al. [62] (2009) | >22.1 | N/A | Canadian | 77 | 44 ± 12 | 82 | T, P/C, I | 15 ± 11 | Piecewise LR, ROC |
| Shin et al. [65] (2022) | >22.8 | N/A | Korean | 157 | 49 ± 12 | 70 | T, P/C, I | 12 ± 8 | ROC |
| Sumrell et al. [70] (2018) | N/A | >86.5 | American | 22 | 36 ± 10 | 100 | T, P/C, I | 8 ± 8 | LR |
| Ravensbergen et al. [69] (2014) | N/A | >94.0 | Canadian | 27 | 40 ± 11 | 70 | T, P/C, I | 14 ± 10 | ROC |
| Yun et al. [64] (2019) | >20.2 | >81.3 | Korean | 52 | 42 ± 11 | 100 | T, P/C, I | 13 ± 8 | ROC, Youden index |
| Pooled Data | |||||||||
| BMI (kg/m2) | >23.3 | N/A | Multiple | 557 | 50 ± 13 | 84 | T, P/C, I | 15 ± 11 | Pooling data * |
| WC (cm) | N/A | >83.9 | Multiple | 175 | 43 ± 12 | 95 | T, P/C, I | 13 ± 9 | Pooling data * |
| Any 3 of the Following Component Risk Factors to Diagnosis Cardiometabolic Syndrome after SCI | |
|---|---|
| Obesity * | Total percent body fat (%BF) as determined by 3- (i.e., dual X-ray absorptiometry) or 4-compartment models [56,126]. Classify adult SCI men with >22%BF and adult SCI women with >35%BF as obese |
| - Or - | |
| Body mass index (BMI) > 22 kg/m2 [62] is the SCI-specific cutoff point for obesity | |
| Elevated triglycerides | Triglycerides ≥ 150 mg/dL |
| Reduced HDL-C | HDL-C < 40 mg/dL in men or <50 mg/dL in women |
| Hypertension | Systolic blood pressure ≥ 130 mmHg, diastolic blood pressure 85, or use of medication for hypertension |
| Dysglycemia | Fasting glucose ≥ 100 mg/dL or use of medication for hyperglycemia |
| Criterion | Normal | Pre-Diabetes | Diabetes |
|---|---|---|---|
| Fasting Plasma Glucose (mg/dL) | <100 | 100–125 | ≥126 |
| Oral Glucose Tolerance Test (mg/dL) * | <140 | 140–199 | ≥200 |
| Hemoglobin A1C (%) | <5.7 | 5.7–6.4 | ≥6.5 |
| Normal | Insulin Resistance | ||
| Insulin Resistance ** | >0.339 | ≤0.339 | |
| Body Mass Index (kg/m2) | Proposed %BF Cutoffs/Ranges to Report Obesity * | |||
|---|---|---|---|---|
| Category [57,58] | Threshold/Range | Category | Men | Women |
| Underweight | <18.5 | Irregular | <13.6 | <21.6 |
| Normal | 18.5–24.9 | Healthy | 13.6–18.26 | 21.6–29.1 |
| Pre-Obesity/Overweight ** | 25.0–29.9 | Pre-Obesity | 18.3–22 | 29.2–34.9 |
| Obese ^ | ≥30 | Obese [55,56] | >22 | >35 |
| Obese I | 30.0–34.9 | Obese I | 22–25.6 | 35–40.7 |
| Obese II | 35.0–39.9 | Obese II | 25.7–29.3 | 40.8–46.6 |
| Obese III | ≥40 | Obese III | >29.3 | >46.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Farkas, G.J.; Burton, A.M.; McMillan, D.W.; Sneij, A.; Gater, D.R., Jr. The Diagnosis and Management of Cardiometabolic Risk and Cardiometabolic Syndrome after Spinal Cord Injury. J. Pers. Med. 2022, 12, 1088. https://doi.org/10.3390/jpm12071088
Farkas GJ, Burton AM, McMillan DW, Sneij A, Gater DR Jr. The Diagnosis and Management of Cardiometabolic Risk and Cardiometabolic Syndrome after Spinal Cord Injury. Journal of Personalized Medicine. 2022; 12(7):1088. https://doi.org/10.3390/jpm12071088
Chicago/Turabian StyleFarkas, Gary J., Adam M. Burton, David W. McMillan, Alicia Sneij, and David R. Gater, Jr. 2022. "The Diagnosis and Management of Cardiometabolic Risk and Cardiometabolic Syndrome after Spinal Cord Injury" Journal of Personalized Medicine 12, no. 7: 1088. https://doi.org/10.3390/jpm12071088