
Individualized Wound Closure—Mechanical Properties of Suture Materials

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Suture Materials
2.2. Group Allocation
2.3. Experimental Array
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bariol, S.V.; Stewart, G.D.; Tolley, D.A. Laparoscopic Suturing: Effect of Instrument Handling on Suture Strength. J. Endourol. 2005, 19, 1127–1133. [Google Scholar] [CrossRef] [PubMed]
- Hong, T.; King, M.W.; Michielsen, S.; Cheung, L.W.; Mary, C.; Guzman, R.; Guidoin, R. Development of in Vitro Performance Tests and Evaluation of Nonabsorbable Monofilament Sutures for Cardiovascular Surgery. ASAIO J. 1998, 44, 776–785. [Google Scholar] [CrossRef] [PubMed]
- Abhari, R.E.; Martins, J.A.; Morris, H.L.; Mouthuy, P.A.; Carr, A. Synthetic Sutures: Clinical Evaluation and Future Developments. J. Biomater. Appl. 2017, 32, 410–421. [Google Scholar] [CrossRef] [PubMed]
- Abellan, D.; Nart, J.; Pascual, A.; Cohen, R.E.; Sanz-Moliner, J.D. Physical and Mechanical Evaluation of Five Suture Materials on Three Knot Configurations: An in Vitro Study. Polymers 2016, 8, 147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polykandriotis, E.; Besrour, F.; Arkudas, A.; Ruppe, F.; Zetzmann, K.; Braeuer, L.; Horch, R.E. Flexor Tendon Repair with a Polytetrafluoroethylene (Ptfe) Suture Material. Arch. Orthop. Trauma Surg. 2019, 139, 429–434. [Google Scholar] [CrossRef]
- Polykandriotis, E.; Ruppe, F.; Niederkorn, M.; Polykandriotis, E.; Brauer, L.; Horch, R.E.; Arkudas, A.; Gruener, J.S. Polytetrafluoroethylene (Ptfe) Suture Vs Fiberwire and Polypropylene in Flexor Tendon Repair. Arch. Orthop. Trauma Surg. 2021, 141, 1609–1614. [Google Scholar] [CrossRef]
- Nonabsorbable Surgical Suture. In United States Pharmacopeia and National Formulary, Usp 29-Nf 24th ed.; United States Pharmacopeial Convention: Rockville, MD, USA, 2006; p. 2776.
- Dobrin, P.B. Surgical Manipulation and the Tensile Strength of Polypropylene Sutures. Arch. Surg. 1989, 124, 665–668. [Google Scholar] [CrossRef]
- Naleway, S.E.; Lear, W.; Kruzic, J.J.; Maughan, C.B. Mechanical Properties of Suture Materials in General and Cutaneous Surgery. J. Biomed. Mater. Res. Part B Appl. Biomater. 2015, 103, 735–742. [Google Scholar] [CrossRef]
- von Fraunhofer, J.A.; Storey, R.S.; Stone, I.K.; Masterson, B.J. Tensile Strength of Suture Materials. J. Biomed. Mater. Res. 1985, 19, 595–600. [Google Scholar] [CrossRef]
- Abiri, A.; Paydar, O.; Tao, A.; LaRocca, M.; Liu, K.; Genovese, B.; Candler, R.; Grundfest, W.S.; Dutson, E.P. Tensile Strength and Failure Load of Sutures for Robotic Surgery. Surg. Endosc. 2017, 31, 3258–3270. [Google Scholar] [CrossRef]
- Turker, M.; Yalcinozan, M.; Cirpar, M.; Cetik, O.; Kalaycioglu, B. Clamp Fixation to Prevent Unfolding of a Suture Knot Decreases Tensile Strength of Polypropylene Sutures. Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 2602–2605. [Google Scholar] [CrossRef] [PubMed]
- Cai, A.; Pingel, I.; Lorz, D.; Beier, J.P.; Horch, R.E.; Arkudas, A. Force Distribution of a Cylindrical Grip Differs between Dominant and Nondominant Hand in Healthy Subjects. Arch. Orthop. Trauma. Surg. 2018, 138, 1323–1331. [Google Scholar] [CrossRef] [PubMed]
- Abiri, A.; Askari, S.J.; Tao, A.; Juo, Y.Y.; Dai, Y.; Pensa, J.; Candler, R.; Dutson, E.P.; Grundfest, W.S. Suture Breakage Warning System for Robotic Surgery. IEEE Trans. Biomed. Eng. 2019, 66, 1165–1171. [Google Scholar] [CrossRef] [PubMed]
- Dai, Y.; Abiri, A.; Pensa, J.; Liu, S.; Paydar, O.; Sohn, H.; Sun, S.; Pellionisz, P.A.; Pensa, C.; Dutson, E.P.; et al. Biaxial Sensing Suture Breakage Warning System for Robotic Surgery. Biomed. Microdevices 2019, 21, 10. [Google Scholar] [CrossRef]
- Bisson, L.J.; Sobel, A.D.; Godfrey, D. Effects of Using a Surgical Clamp to Hold Tension While Tying Knots with Commonly Used Orthopedic Sutures. Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 1673–1680. [Google Scholar] [CrossRef] [PubMed]
- Diks, J.; Nio, D.; Linsen, M.A.; Rauwerda, J.A.; Wisselink, W. Suture Damage During Robot-Assisted Vascular Surgery: Is It an Issue? Surg. Laparosc. Endosc. Percutaneous Tech. 2007, 17, 524–527. [Google Scholar] [CrossRef]
- Dobrin, P.B. Chronic Loading of Polypropylene Sutures: Implications for Breakage after Carotid Endarterectomy. J. Surg. Res. 1996, 61, 4–10. [Google Scholar] [CrossRef]
- Dobrin, P.B.; Mrkvicka, R. Chronic Loading and Extension Increases the Acute Breaking Strength of Polypropylene Sutures. Ann. Vasc. Surg. 1998, 12, 424–429. [Google Scholar] [CrossRef]
- Lekic, N.; Dodds, S.D. Suture Materials, Needles, and Methods of Skin Closure: What Every Hand Surgeon Should Know. J. Hand Surg. Am. 2022, 47, 160–171.e1. [Google Scholar] [CrossRef]
- Lear, W. Instruments and Materials. In Surgery of the Skin, 3rd ed.; Robinson, J.K., Hanke, C.W., Siegel, D., Fratila, A., Bhatia, A., Rohrer, T., Eds.; Saunders: Philadelphia, PA, USA, 2014; pp. 64–72. ISBN 9780323260282. [Google Scholar]
- Kim, K.Y.; Anoushiravani, A.A.; Long, W.J.; Vigdorchik, J.M.; Fernandez-Madrid, I.; Schwarzkopf, R.A. Meta-Analysis and Systematic Review Evaluating Skin Closure after Total Knee Arthroplasty-What Is the Best Method? J. Arthroplast. 2017, 32, 2920–2927. [Google Scholar] [CrossRef]
- Knackstedt, R.W.; Dixon, J.A.; O’Neill, P.J.; Herrera, F.A. Rash with Dermabond Prineo Skin Closure System Use in Bilateral Reduction Mammoplasty: A Case Series. Case Rep. Med. 2015, 2015, 642595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ko, J.H.; Yang, I.H.; Ko, M.S.; Kamolhuja, E.; Park, K.K. Do Zip-Type Skin-Closing Devices Show Better Wound Status Compared to Conventional Staple Devices in Total Knee Arthroplasty? Int. Wound J. 2017, 14, 250–254. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, Y.; Miyamoto, T.; Naito, Y.; Yoshitake, S.; Sasahara, A.; Miyaji, K. Randomized Study of a New Noninvasive Skin Closure Device for Use after Congenital Heart Operations. Ann. Thorac. Surg. 2016, 102, 1368–1374. [Google Scholar] [CrossRef] [PubMed]
- Zou, F.; Wang, Y.; Zheng, Y.; Xie, Y.; Zhang, H.; Chen, J.; Hussain, M.I.; Meng, H.; Peng, J. A Novel Bioactive Polyurethane with Controlled Degradation and L-Arg Release Used as Strong Adhesive Tissue Patch for Hemostasis and Promoting Wound Healing. Bioact. Mater. 2022, 17, 471–487. [Google Scholar] [CrossRef]
- Tian, P.; Li, Y.M.; Li, Z.J.; Xu, G.J.; Ma, X.L. Comparison between Zip-Type Skin Closure Device and Staple for Total Knee Arthroplasty: A Meta-Analysis. BioMed Res. Int. 2021, 2021, 6670064. [Google Scholar] [CrossRef]
- Han, C.M.; Cheng, B.; Wu, P. Writing group of growth factor guideline on behalf of Chinese Burn, Association. Clinical Guideline on Topical Growth Factors for Skin Wounds. Burn. Trauma 2020, 8, tkaa035. [Google Scholar] [CrossRef]
- Calhoun, C.C.; Cardenes, O.; Ducksworth, J.; Le, A.D. Off-Label Use of Becaplermin Gel (Recombinant Platelet-Derived Growth Factor-Bb) for Treatment of Mucosal Defects after Corticocancellous Bone Graft: Report of 2 Cases with Review of the Literature. J. Oral Maxillofac. Surg. 2009, 67, 2516–2520. [Google Scholar] [CrossRef]
- Papanas, N.; Maltezos, E. Benefit-Risk Assessment of Becaplermin in the Treatment of Diabetic Foot Ulcers. Drug Saf. 2010, 33, 455–461. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Product | Manufacturer | Material | Type | Absorbable | Coating |
|---|---|---|---|---|---|
| Vicryl® Plus | Ethicon | Polyglactine 910 | Braided | + | + |
| Vicryl® | Ethicon | Polyglactine 910 | Braided | + | − |
| Monocryl® Plus | Ethicon | Polyglecaprone 25 | Braided | + | + |
| PDS® Plus | Ethicon | Polydioxanone | Monofil. | + | + |
| PDS® II | Ethicon | Polydioxanone | Monofil. | + | − |
| Prolene® | Ethicon | Polypropylene | Monofil. | − | − |
| Surgipro® | Covidien | Polypropylene-Polyethylene | Monofil. | − | − |
| Seratan® | Serag-Wiessner | Polyamide | Monofil. | − | + |
| Resolon® | Resorba | Polyamide | Monofil. | − | − |
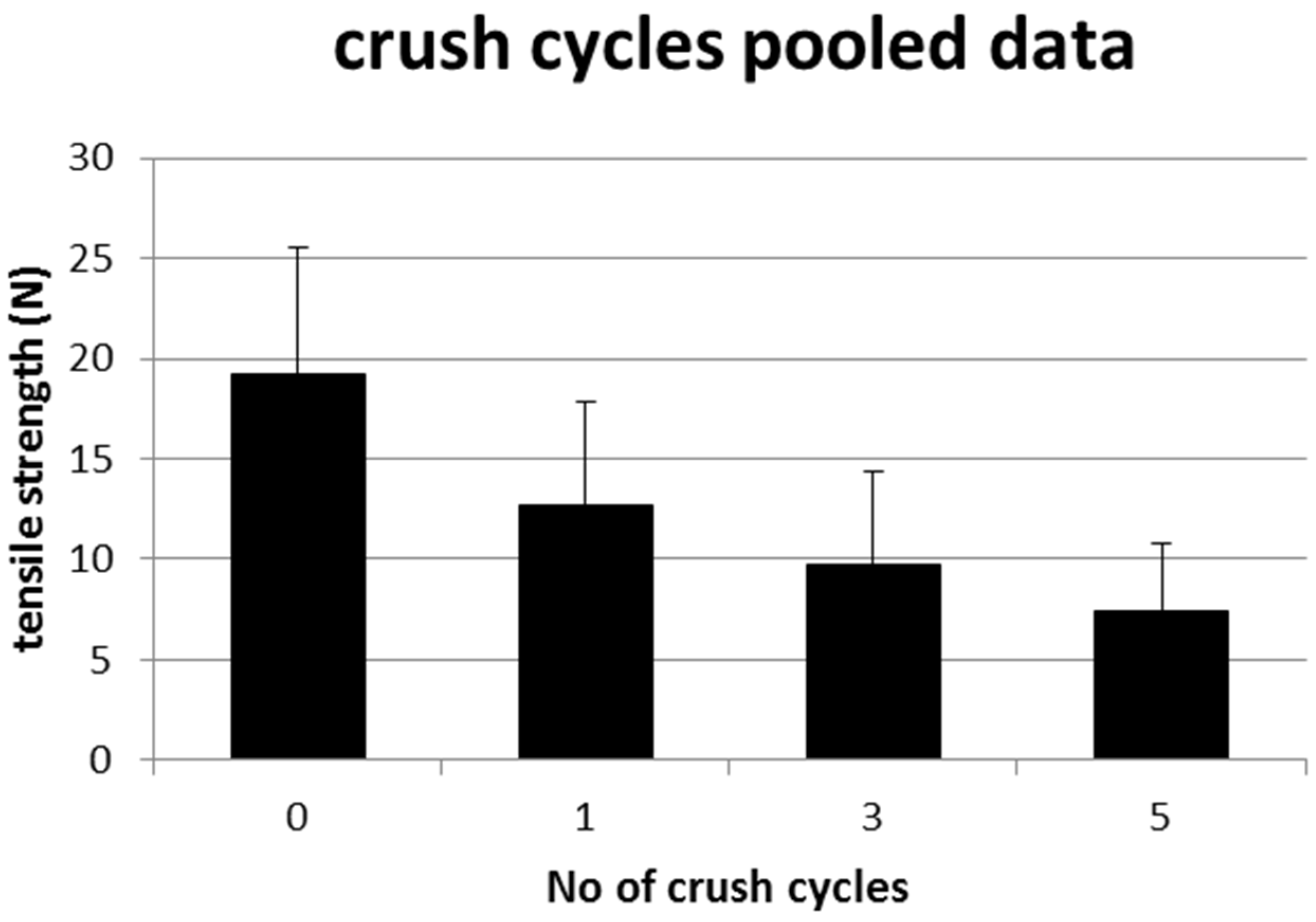
| Crushing Load (Cycles) | Mean Tensile Strength (N) | Tensile Strength Remaining (%) |
|---|---|---|
| 0 | 19.21 (±6.371, 11.66–30.72) | 100.0 |
| 1 | 12.70 (±5.13, 7.62–21.33) | 66.1 |
| 3 | 9.75 (±4.63, 4.48–18.24) | 50.0 |
| 5 | 7.36 (±3.45, 3.49–15.18) | 38.3 |
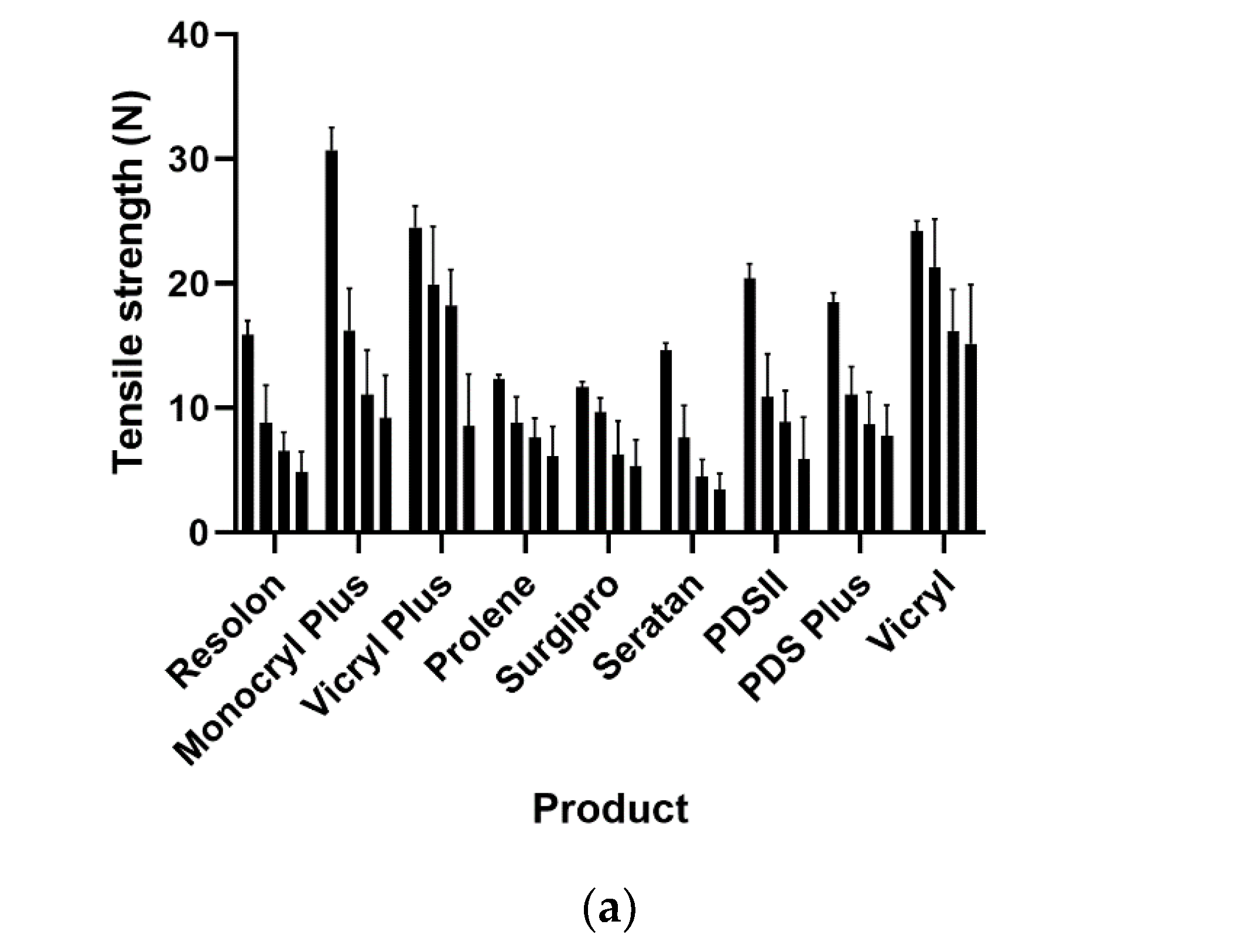
| Product | 0 Crushing Load | 1× Crushing Load | 3× Crushing Load | 5× Crushing Load | ||||
|---|---|---|---|---|---|---|---|---|
| Mean | (SD) | Mean | (SD) | Mean | (SD) | Mean | (SD) | |
| Resolon | 15.87 | (1.13) | 8.78 | (3.03) | 6.50 | (1.55) | 4.86 | (1.63) |
| Monocryl Plus | 30.72 | (1.82) | 16.24 | (3.37) | 11.06 | (3.60) | 9.19 | (3.43) |
| Vicryl Plus | 24.52 | (1.69) | 19.91 | (4.66) | 18.24 | (2.88) | 8.55 | (4.15) |
| Prolene | 12.30 | (0.35) | 8.80 | (2.09) | 7.60 | (1.59) | 6.10 | (2.43) |
| Surgipro | 11.66 | (0.44) | 9.65 | (1.14) | 6.28 | (2.67) | 5.33 | (2.12) |
| Seratan | 14.62 | (0.59) | 7.62 | (2.56) | 4.48 | (1.35) | 3.49 | (1.23) |
| PDSII | 20.43 | (1.16) | 10.85 | (3.49) | 8.86 | (2.51) | 5.87 | (3.37) |
| PDS Plus | 18.53 | (0.72) | 11.08 | (2.25) | 8.64 | (2.61) | 7.74 | (2.49) |
| Vicryl | 24.22 | (0.78) | 21.33 | (3.85) | 16.17 | (3.33) | 15.18 | (4.75) |
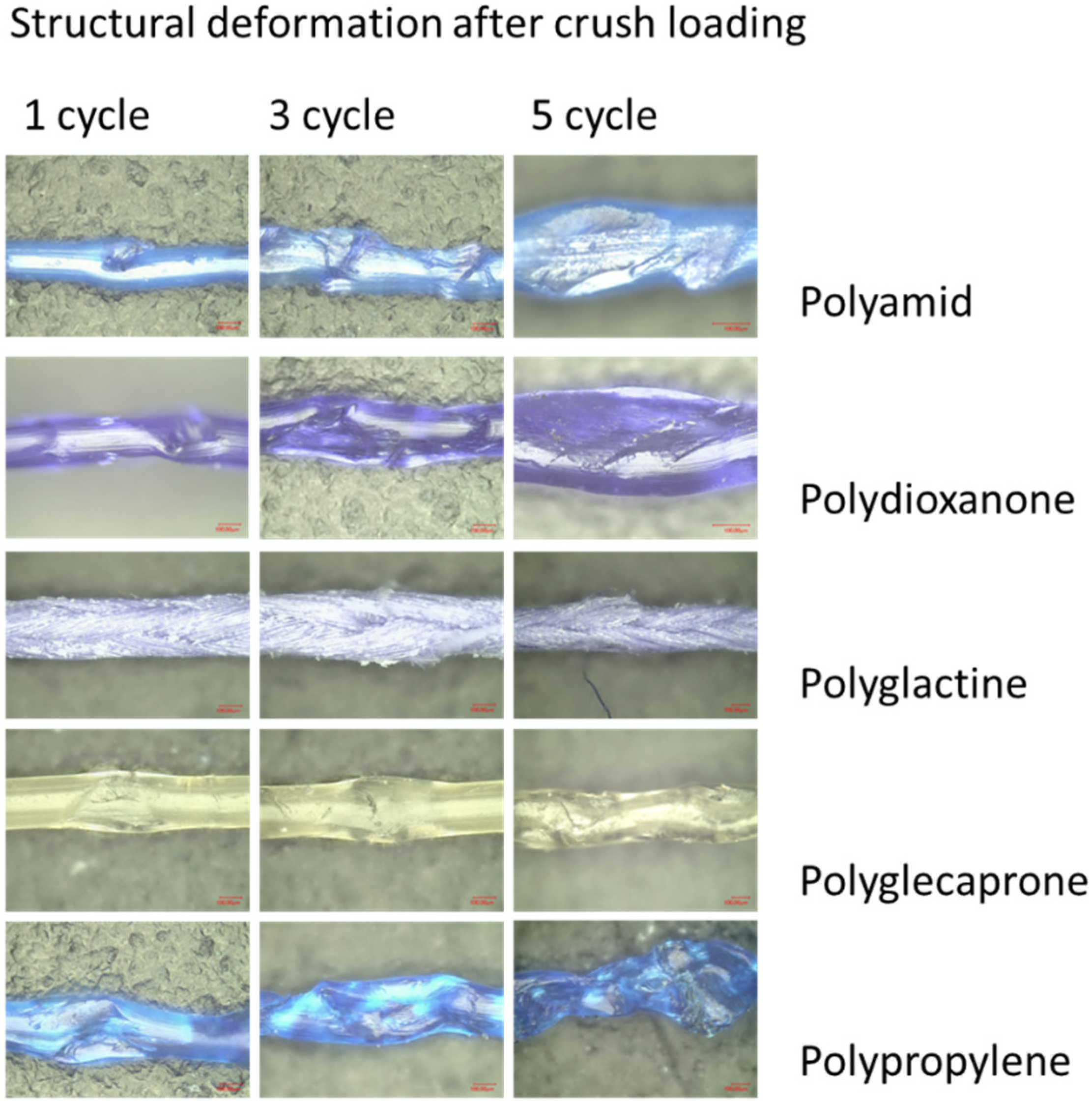
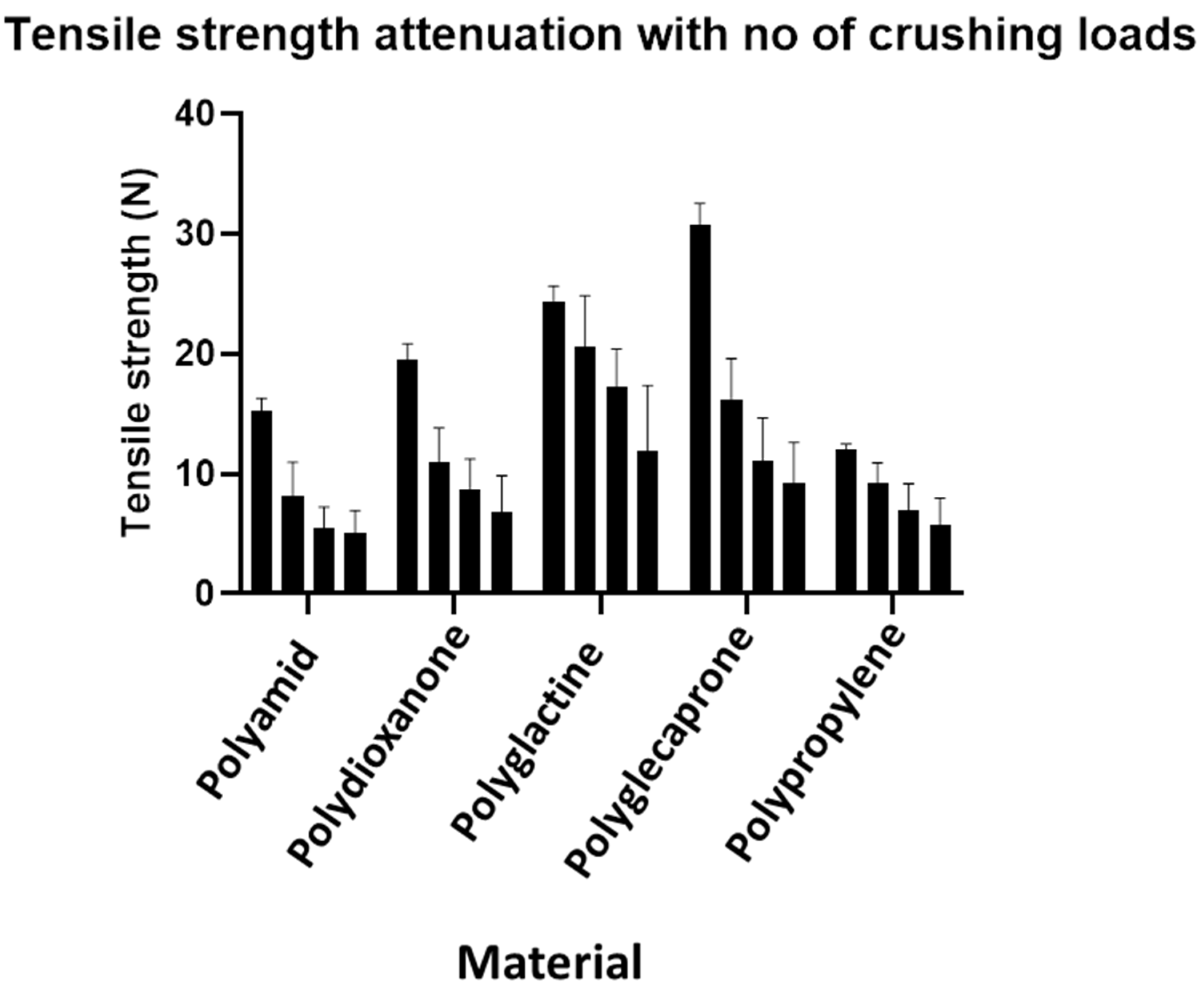
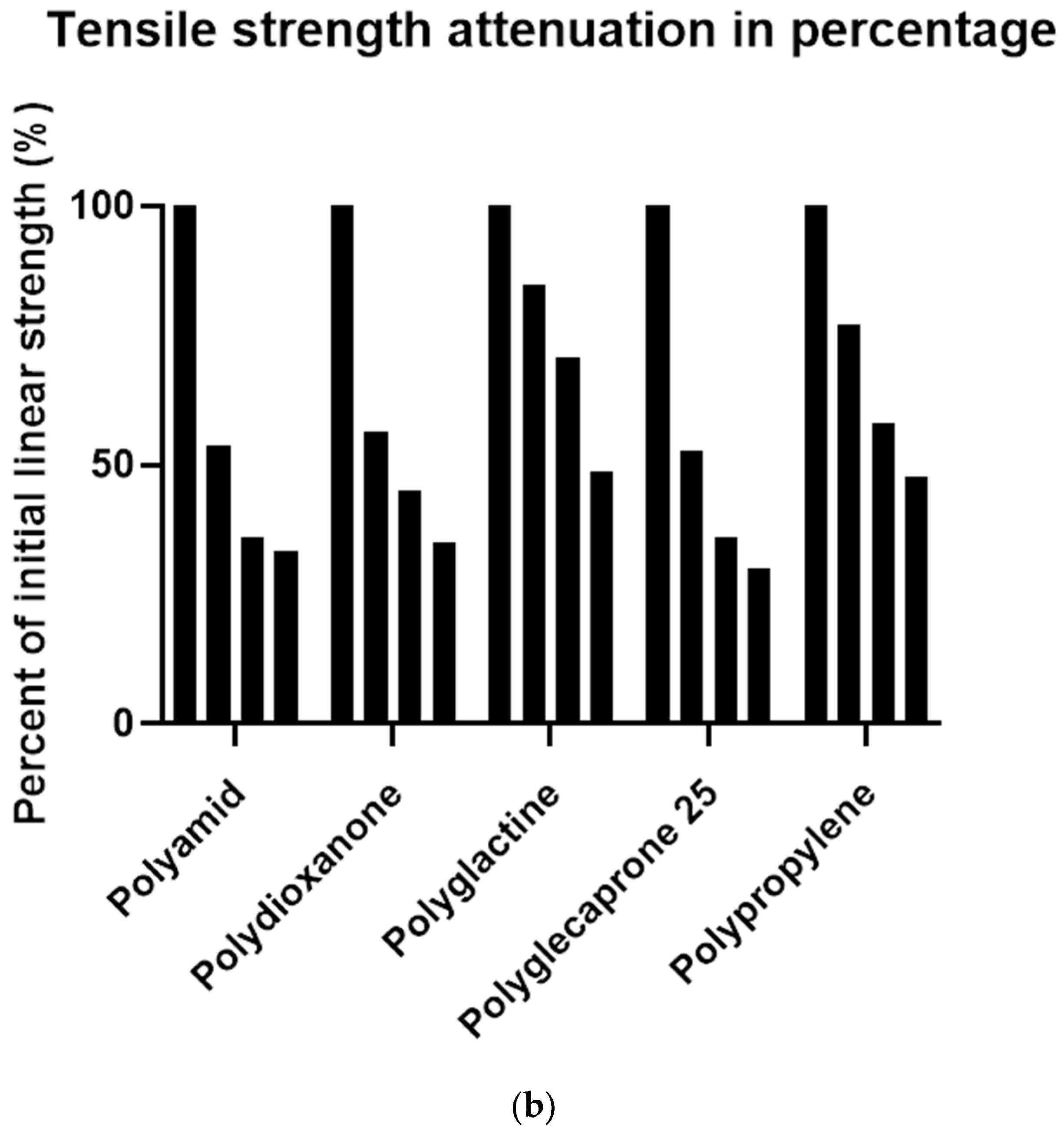
| Material | 0 Crushing Load | 1× Crushing Load | 3× Crushing Load | 5× Crushing Load | ||||
|---|---|---|---|---|---|---|---|---|
| Mean (SD) | Remaining Linear Strength | Mean (SD) | Remaining Linear Strength | Mean (SD) | Remaining Linear Strength | Mean (SD) | Remaining Linear Strength | |
| Polyamid | 15.25 (1.09) | 100% | 8.20 (2.80) | 53.79% | 5.49 (1.75) | 36.01% | 5.10 (1.85) | 33.42% |
| Polydioxanone | 19.48 (1.35) | 100% | 10.97 (2.86) | 56.29% | 8.75 (2.49) | 44.92% | 6.81 (3.04) | 34.93% |
| Polyglactine | 24.37 (1.29) | 100% | 20.62 (4.22) | 84.61% | 17.21 (3.21) | 70.60% | 11.87 (5.51) | 48.69% |
| Polyglecaprone | 30.72 (1.82) | 100% | 16.24 (3.37) | 52.86% | 11.06 (3.60) | 36.00% | 9.19 (3.43) | 29.92% |
| Polypropylene | 11.98 (0.51) | 100% | 9.23 (1.70) | 77.00% | 6.94 (2.24) | 57.93% | 5.72 (2.25) | 47.70% |
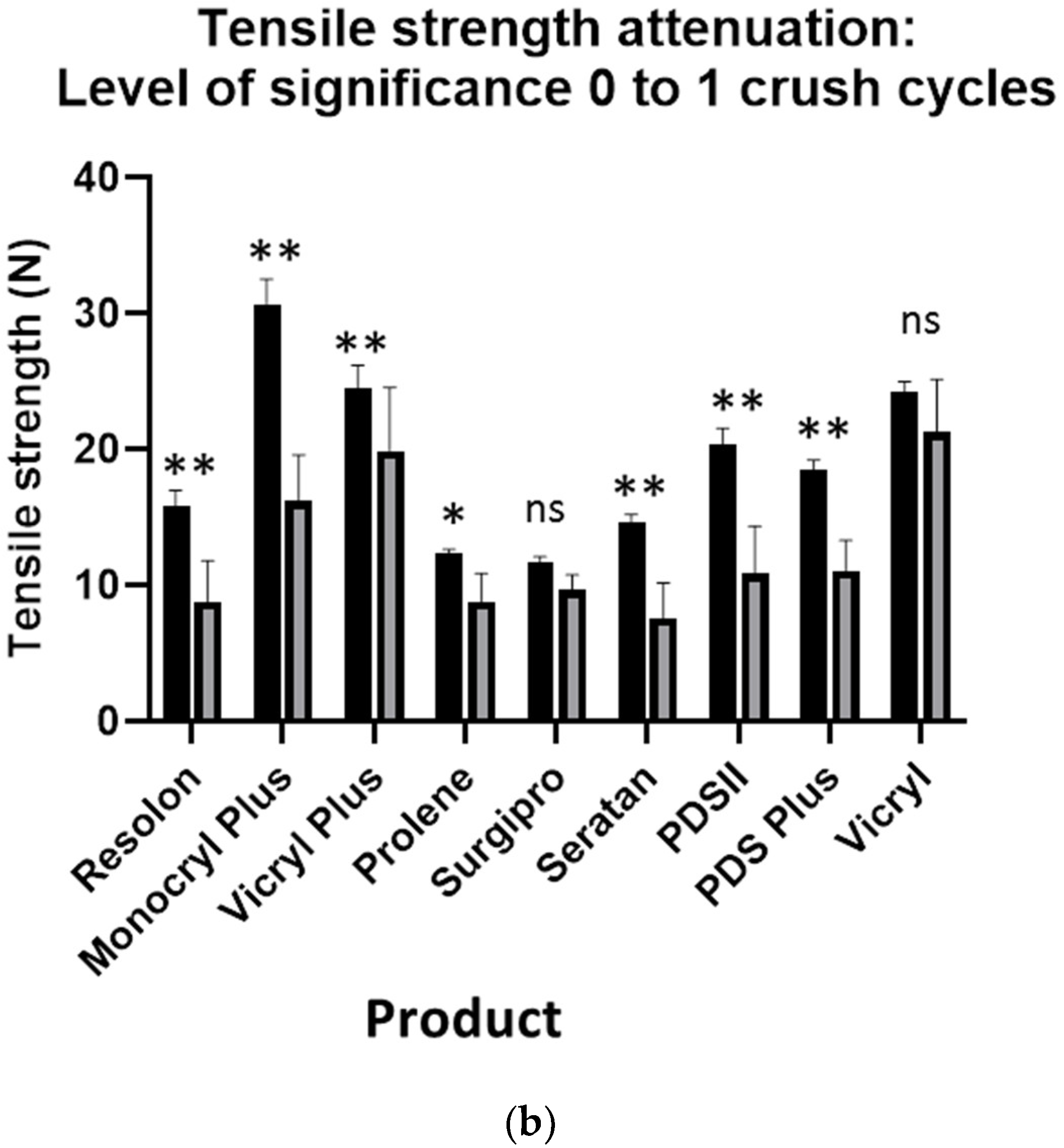
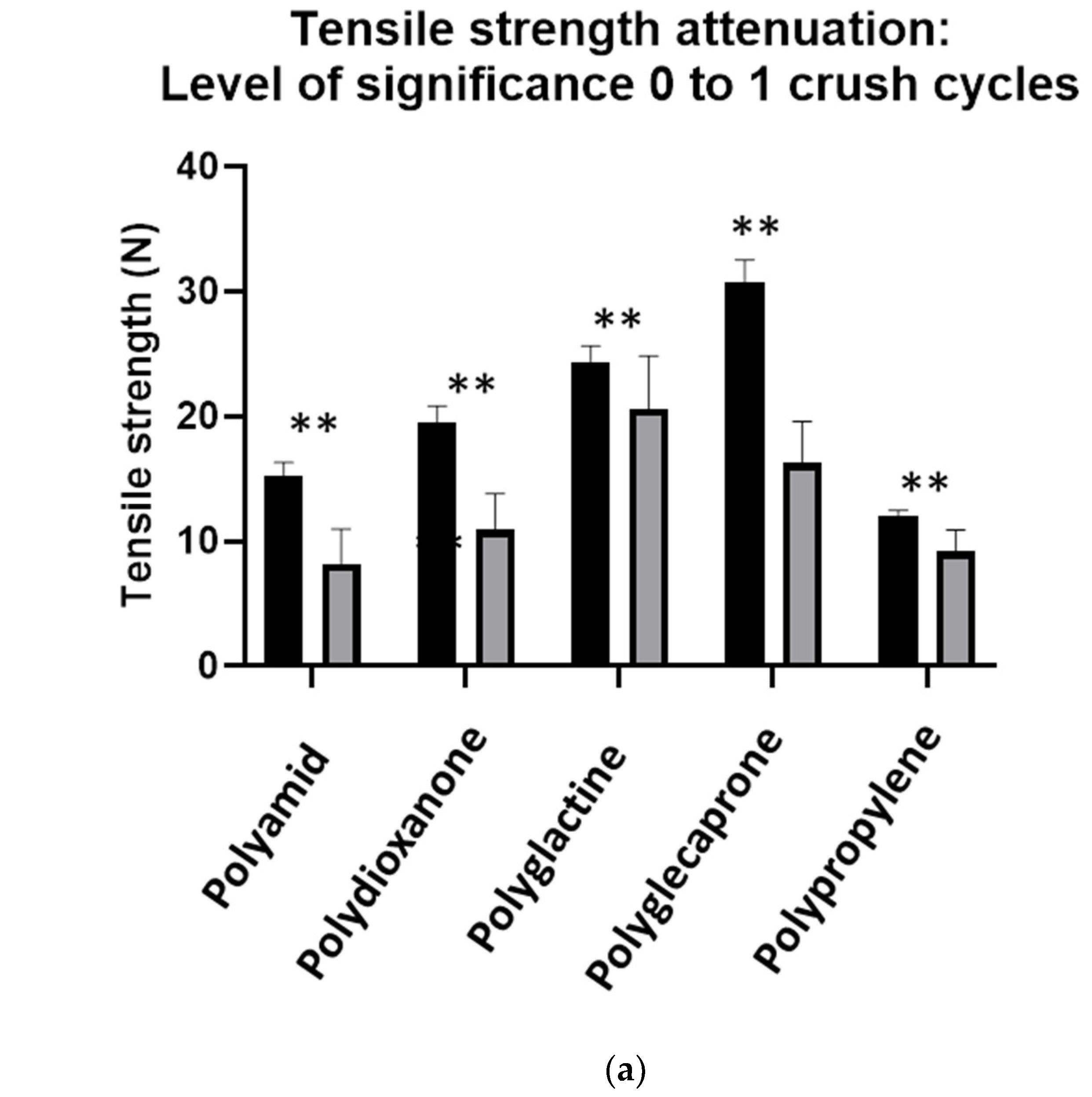
| Material | 0× vs. 1× Crushing Load | 1× vs. 3× Crushing Load | 3× vs. 5× Crushing Load |
|---|---|---|---|
| Level of Significance | Level of Significance | Level of Significance | |
| Polyamid | p < 0.0001 (**) | p = 0.0110 (*) | p > 0.9999 (ns) |
| Polydioxanone | p < 0.0001 (**) | p = 0.0639 (ns) | p = 0.1486 (ns) |
| Polyglactine | p = 0.0001 (**) | p = 0.0005 (**) | p < 0.0001 (**) |
| Polyglecaprone | p < 0,0001 (**) | p = 0.0002 (**) | p = 0.7571 (ns) |
| Polypropylene | p = 0.0092 (**) | p = 0.0507 (ns) | p = 0.9387 (ns) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Polykandriotis, E.; Daenicke, J.; Bolat, A.; Grüner, J.; Schubert, D.W.; Horch, R.E. Individualized Wound Closure—Mechanical Properties of Suture Materials. J. Pers. Med. 2022, 12, 1041. https://doi.org/10.3390/jpm12071041
Polykandriotis E, Daenicke J, Bolat A, Grüner J, Schubert DW, Horch RE. Individualized Wound Closure—Mechanical Properties of Suture Materials. Journal of Personalized Medicine. 2022; 12(7):1041. https://doi.org/10.3390/jpm12071041
Chicago/Turabian StylePolykandriotis, Elias, Jonas Daenicke, Anil Bolat, Jasmin Grüner, Dirk W. Schubert, and Raymund E. Horch. 2022. "Individualized Wound Closure—Mechanical Properties of Suture Materials" Journal of Personalized Medicine 12, no. 7: 1041. https://doi.org/10.3390/jpm12071041