
Physiologic Range of Myocardial Mechano-Energetic Efficiency among Healthy Subjects: Impact of Gender and Age

 ,
,  , , , , , , , , , and add
Show full author list
, , , , , , , , , and add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Echocardiography
2.3. Myocardial Mechano-Energetic Efficiency Measurements
2.4. Statistical Methods
3. Results
3.1. MEE and MEEi according to Gender
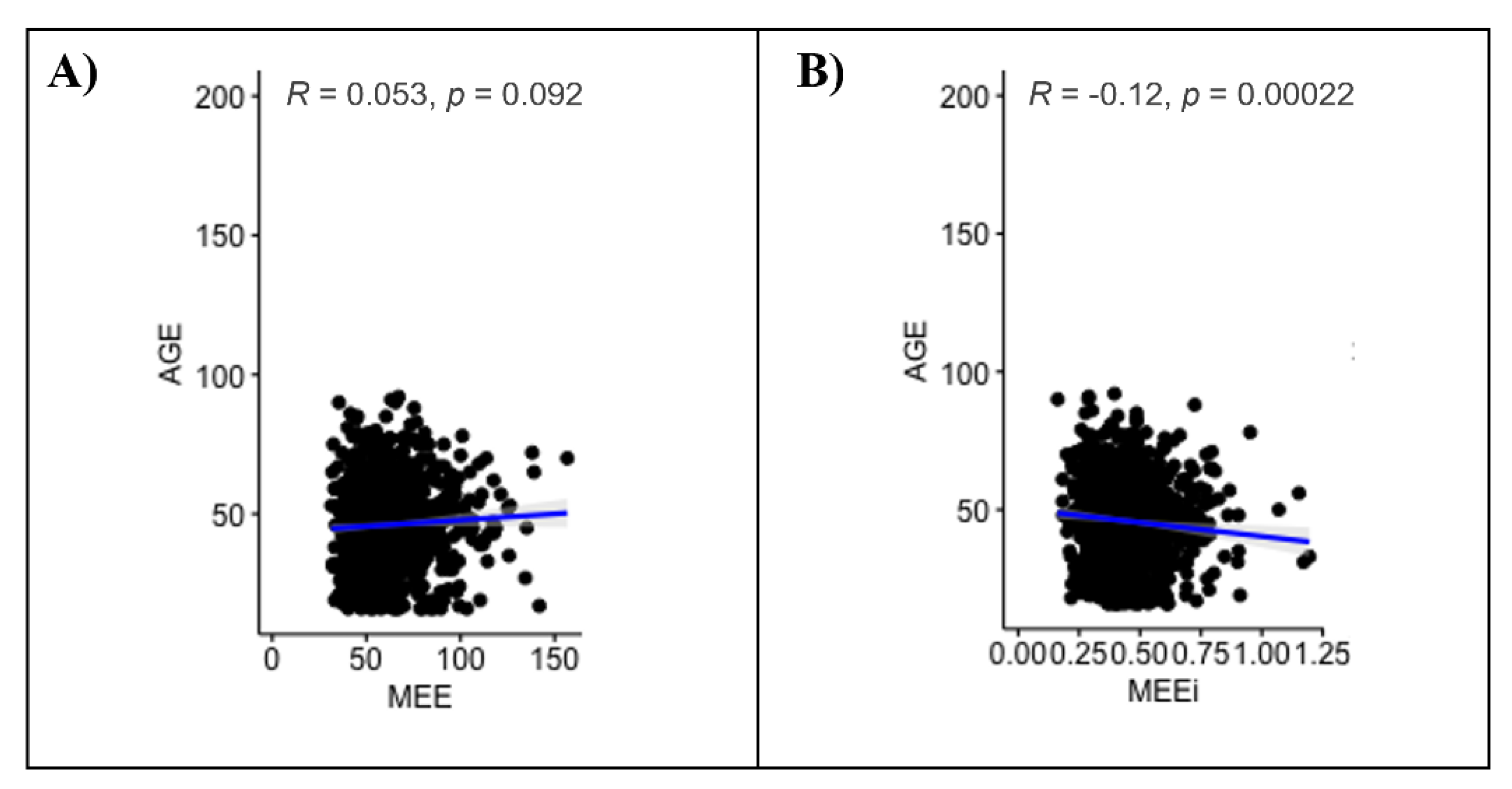
3.2. MEE and MEEi according to Age
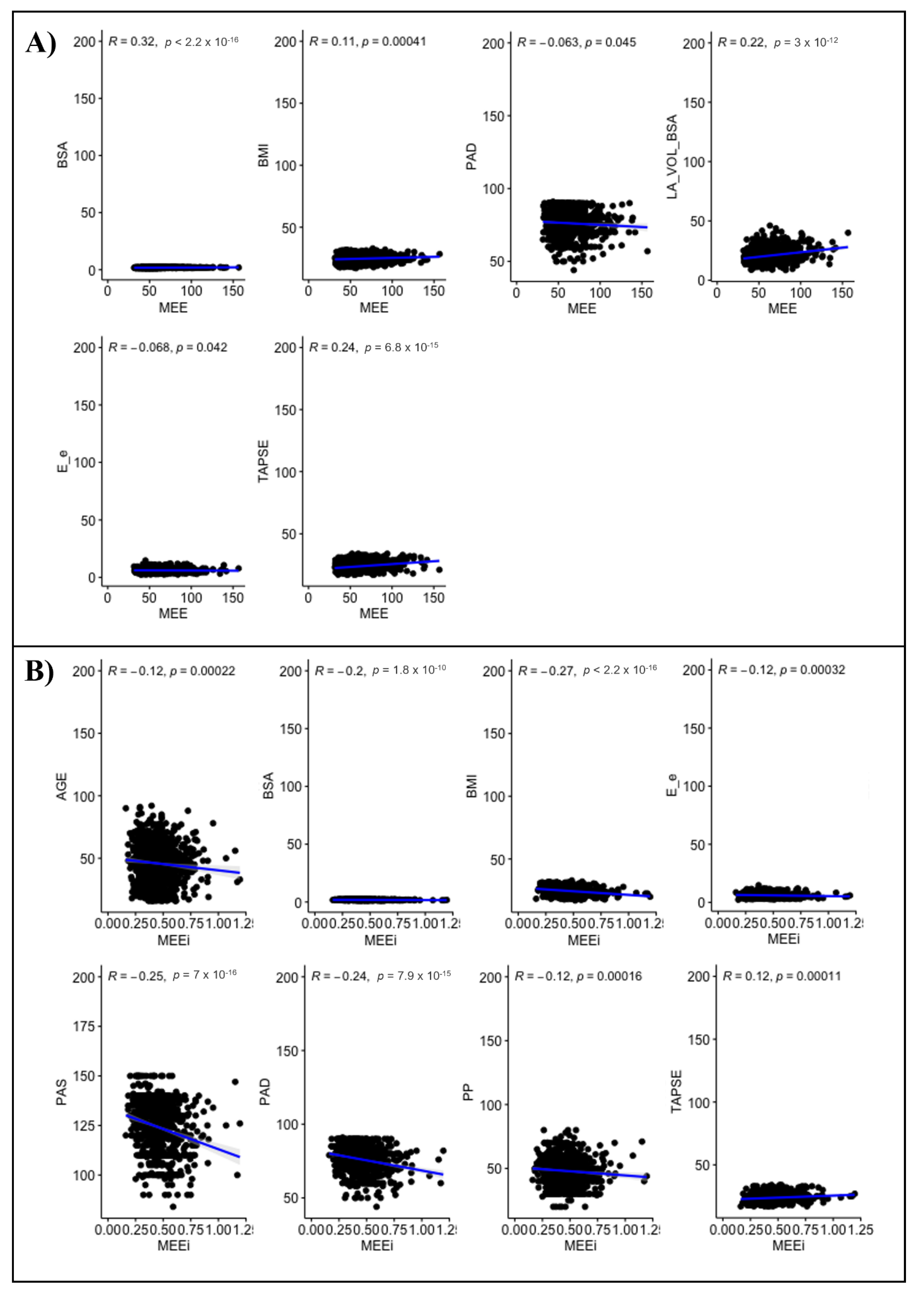
3.3. Clinical and Echocardiographic Correlates of MEE and MEEi
4. Inter- and Intraobserver Variability
5. Discussion
5.1. Previous Studies
5.2. Uniqueness of the Present Study
6. Limitations of the Present Study
7. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Knaapen, P.; Germans, T.; Knuuti, J.; Paulus, W.J.; Dijkmans, P.A.; Allaart, C.P.; Lammertsma, A.A.; Visser, F.C. Myocardial energetics and efficiency: Current status of the noninvasive approach. Circulation 2007, 115, 918–927. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Simone, G.; Chinali, M.; Galderisi, M.; Benincasa, M.; Girfoglio, D.; Botta, I.; D’Addeo, G.; de Divitiis, O. Myocardial mechano-energetic efficiency in hypertensive adults. J. Hypertens. 2009, 27, 650–655. [Google Scholar] [CrossRef] [PubMed]
- de Simone, G.; Izzo, R.; Losi, M.A.; Stabile, E.; Rozza, F.; Canciello, G.; Mancusi, C.; Trimarco, V.; De Luca, N.; Trimarco, B. Depressed myocardial energetic efficiency is associated with increased cardiovascular risk in hypertensive left ventricular hypertrophy. J. Hypertens. 2016, 34, 1846–1853. [Google Scholar] [CrossRef] [PubMed]
- Mancusi, C.; Midtbø, H.; De Luca, N.; Halland, H.; de Simone, G.; Gerdts, E. Association of Myocardial Energetic Efficiency with Circumferential and Longitudinal Left Ventricular Myocardial Function in Subjects with Increased Body Mass Index (the FATCOR Study). J. Clin. Med. 2021, 10, 1581. [Google Scholar] [CrossRef]
- Losi, M.A.; Izzo, R.; Mancusi, C.; Wang, W.; Roman, M.J.; Lee, E.T.; Howard, B.V.; Devereux, R.B.; de Simone, G. Depressed Myocardial Energetic Efficiency Increases Risk of Incident Heart Failure: The Strong Heart Study. J. Clin. Med. 2019, 8, 1044. [Google Scholar] [CrossRef] [Green Version]
- Manzi, M.V.; Mancusi, C.; Lembo, M.; Esposito, G.; Rao, M.; de Simone, G.; Morisco, C.; Trimarco, V.; Izzo, R.; Trimarco, B. Low mechano-energetic efficiency is associated with future left ventricular systolic dysfunction in hypertensives. ESC Heart Fail 2022. advance online publication. [Google Scholar] [CrossRef]
- Vanessa Fiorentino, T.; Miceli, S.; Succurro, E.; Sciacqua, A.; Andreozzi, F.; Sesti, G. Depressed myocardial mechano-energetic efficiency in subjects with dysglycemia. Diabetes Res. Clin. Pract. 2021, 177, 108883. [Google Scholar] [CrossRef] [PubMed]
- Cioffi, G.; Mancusi, C.; de Simone, G.; Ognibeni, F.; Orsolini, G.; Dalbeni, A.; Gatti, D.; Fassio, A.; Adami, G.; Rossini, M.; et al. Predictors and prognostic role of low myocardial mechano-energetic efficiency in chronic inflammatory arthritis. J. Hypertens. 2021, 39, 53–61. [Google Scholar] [CrossRef]
- Ferrara, F.; Rudski, L.G.; Vriz, O.; Gargani, L.; Afilalo, J.; D’Andrea, A.; D’Alto, M.; Marra, A.M.; Acri, E.; Stanziola, A.A.; et al. Physiologic correlates of tricuspid annular plane systolic excursion in 1168 healthy subjects. Int. J. Cardiol. 2016, 223, 736–743. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, F.; Gargani, L.; Ruohonen, S.; Vriz, O.; Scalese, M.; Russo, V.; Marra, A.M.; Stanziola, A.A.; Cittadini, A.; D’Andrea, A.; et al. Reference values and correlates of right atrial volume in healthy adults by two-dimensional echocardiography. Echocardiography 2018, 35, 1097–1107. [Google Scholar] [CrossRef]
- Marra, A.M.; Benjamin, N.; Ferrara, F.; Vriz, O.; D’Alto, M.; D’Andrea, A.; Stanziola, A.A.; Gargani, L.; Cittadini, A.; Grünig, E.; et al. Reference ranges and determinants of right ventricle outflow tract acceleration time in healthy adults by two-dimensional echocardiography. Int. J. Cardiovasc. Imaging 2017, 33, 219–226. [Google Scholar] [CrossRef] [Green Version]
- Rudski, L.G.; Lai, W.W.; Afilalo, J.; Hua, L.; Handschumacher, M.D.; Chandrasekaran, K.; Solomon, S.D.; Louie, E.K.; Schiller, N.B. Guidelines for the echocardiographic assessment of the right heart in adults: A report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J. Am. Soc. Echocardiogr. 2010, 23, 685–788. [Google Scholar] [CrossRef]
- Lang, R.M.; Bierig, M.; Devereux, R.B.; Flachskampf, F.A.; Foster, E.; Pellikka, P.A.; Picard, M.H.; Roman, M.J.; Seward, J.; Shanewise, J.S.; et al. Recommendations for chamber quantification: A report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J. Am. Soc. Echocardiogr. 2005, 18, 1440–1463. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inoue, R.; Ohkubo, T.; Kikuya, M.; Metoki, H.; Asayama, K.; Kanno, A.; Obara, T.; Hirose, T.; Hara, A.; Hoshi, H.; et al. Predictive value for mortality of the double product at rest obtained by home blood pressure measurement: The Ohasama study. Am. J. Hypertens. 2012, 25, 568–575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019. [Google Scholar]
- Juszczyk, A.; Jankowska, K.; Zawiślak, B.; Surdacki, A.; Chyrchel, B. Depressed Cardiac Mechanical Energetic Efficiency: A Contributor to Cardiovascular Risk in Common Metabolic Diseases-From Mechanisms to Clinical Applications. J. Clin. Med. 2020, 9, 2681. [Google Scholar] [CrossRef] [PubMed]
- Bahlmann, E.; Einarsen, E.; Cramariuc, D.; Midtbø, H.; Mancusi, C.; Rossebø, A.; Willems, S.; Gerdts, E. Low myocardial energetic efficiency is associated with increased mortality in aortic stenosis. Open Heart 2021, 8, e001720. [Google Scholar] [CrossRef] [PubMed]
- Asch, F.M.; Miyoshi, T.; Addetia, K.; Citro, R.; Daimon, M.; Desale, S.; Fajardo, P.G.; Kasliwal, R.R.; Kirkpatrick, J.N.; Monaghan, M.J.; et al. Similarities and Differences in Left Ventricular Size and Function among Races and Nationalities: Results of the World Alliance Societies of Echocardiography Normal Values Study. J. Am. Soc. Echocardiogr. 2019, 32, 1396–1406.e2. [Google Scholar] [CrossRef] [Green Version]
- Vriz, O.; Aboyans, V.; D’Andrea, A.; Ferrara, F.; Acri, E.; Limongelli, G.; Della Corte, A.; Driussi, C.; Bettio, M.; Pluchinotta, F.R.; et al. Normal values of aortic root dimensions in healthy adults. Am. J. Cardiol. 2014, 114, 921–927. [Google Scholar] [CrossRef] [PubMed]
- Patel, H.N.; Miyoshi, T.; Addetia, K.; Henry, M.P.; Citro, R.; Daimon, M.; Gutierrez Fajardo, P.; Kasliwal, R.R.; Kirkpatrick, J.N.; Monaghan, M.J.; et al. Normal Values of Cardiac Output and Stroke Volume According to Measurement Technique, Age, Sex, and Ethnicity: Results of the World Alliance of Societies of Echocardiography Study. J. Am. Soc. Echocardiogr. 2021, 34, 1077–1085.e1. [Google Scholar] [CrossRef]
- Ferrara, F.; Capuano, F.; Cocchia, R.; Ranieri, B.; Contaldi, C.; Lacava, G.; Capone, V.; Chianese, S.; Rega, S.; Annunziata, R.; et al. Reference Ranges of Left Ventricular Hemodynamic Forces in Healthy Adults: A Speckle-Tracking Echocardiographic Study. J. Clin. Med. 2021, 10, 5937. [Google Scholar] [CrossRef] [PubMed]
- Tsugu, T.; Postolache, A.; Dulgheru, R.; Sugimoto, T.; Tridetti, J.; Nguyen Trung, M.L.; Piette, C.; Moonen, M.; Manganaro, R.; Ilardi, F.; et al. Echocardiographic reference ranges for normal left ventricular layer-specific strain: Results from the EACVI NORRE study. Eur. Heart J. Cardiovasc. Imaging 2020, 21, 896–905. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Overall Population 1168 Patients (Mean ± SD) (Median) | Range | Women 613 (52.5%) (Mean ± SD) | Men 555 (47.5%) (Mean ± SD) | p-Value |
|---|---|---|---|---|---|
| Age (years) | 45.4 ± 15.6 (46) | 16–92 | 46.2 ± 15.4 | 44.6 ± 15.8 | 0.075 |
| Height (cm) | 168.6 ± 9.5 (168) | 144–198 | 162.4 ± 6.7 | 175.5 ± 7.1 | 0.0001 |
| Weight (Kg) | 69.7 ± 12.0 (70) | 41–113 | 62.7 ± 8.8 | 77.3 ± 10.4 | 0.0001 |
| BMI (kg/m2) | 24.4 ± 3.1 (24.2) | 24.2–32.8 | 23.8 ± 3.24 | 25.1 ± 2.8 | 0.0001 |
| BSA (m2) | 1.79 ± 0.19 (1.78) | 1.06–2.76 | 1.67 ± 0.14 | 1.92 ± 0.16 | 0.0001 |
| SBP (mmHg) | 123.9 ± 12.1 (125) | 84–145 | 121.8 ± 12.7 | 126.1 ± 10.9 | 0.0001 |
| DBP (mmHg) | 76.1 ± 8.5 (78.5) | 44–91 | 75.0 ± 8.4 | 77.2 ± 8.3 | 0.0001 |
| MBP (mmHg) | 92.0 ± 8.7 (93.3) | 57.3–110.6 | 90.6 ± 8.9 | 93.5 ± 8.1 | 0.0001 |
| PP (mmHg) | 47.7 ± 9.7 (48) | 20–80 | 46.8 ± 9.6 | 48.8 ± 9.7 | 0.001 |
| HR (b/m) | 71.1 ± 11.6 (70) | 45–105 | 73.3 ± 10.8 | 68.7 ± 11.9 | 0.025 |
| Parameters | Overall Population (Mean ± SD) (Range) | Women (Mean ± SD) | Men (Mean ± SD) | p Value |
|---|---|---|---|---|
| Septal wall thickness in diastole (mm) | 8.6 ± 1.4 (6–11) | 8.3 ± 1.3 | 9.0 ± 1.3 | 0.0001 |
| Inferolateral wall thickness in diastole (mm) | 8.6 ± 1.3 (6–11) | 8.3 ± 1.2 | 9.0 ± 1.3 | 0.0001 |
| LV end-diastolic diameter (mm) | 47.3 ± 5.0 (36–58) | 45.0 ± 4.2 | 49.8 ± 4.5 | 0.0001 |
| LV EDV (mL) | 80.5 ± 25.8 (41–158) | 67.7 ± 18.0 | 94.6 ± 25.8 | 0.0001 |
| LV ESV (mL) | 29.4 ± 11.0 (11–72) | 24.6 ± 7.9 | 34.7 ± 11.6 | 0.0001 |
| LV EF (biplane) (%) | 63.9 ± 5.6 (50–79) | 64.1 ± 5.3 | 63.7 ± 6.0 | 0.226 |
| LV mass index (g/m2) | 77.0 ± 16.5 (38–145) | 72.1 ± 14.9 | 82.7 ± 16.5 | 0.0001 |
| LAVI (mL/m2) | 20.4 ± 5.6 (8.5–46.0) | 20.0 ± 5.2 | 20.8 ± 6.1 | 0.024 |
| Mitral Peak E/e’ ratio | 5.9 ± 1.7 (2.2–11.8) | 6.1 ± 1.8 | 5.7 ± 1.7 | 0.0001 |
| SVI (mL/m2) | 38.7 ± 7.4 (22.0–73.1) | 39.1 ± 6.7 | 38.3 ± 7.9 | 0.121 |
| CI (L/min/m2) | 2.7 ± 0.6 (1.73 −5.7) | 2.8 ± 0.6 | 2.5 ± 0.6 | 0.0001 |
| RV basal diameter (mm) | 33.2 ± 3.6 | 32.0 ± 3.3 | 34.7 ± 3.3 | 0.0001 |
| RV mid cavity diameter (mm) | 25.8 ± 3.8 | 24.6 ± 3.2 | 27.3 ±3.9 | 0.0001 |
| RV longitudinal diameter (mm) | 63.8 ± 5.0 | 62.1 ± 4.1 | 65.4 ± 5.3 | 0.0001 |
| RA major dimension (mm) | 41.3 ± 4.6 | 39.9 ± 4.2 | 42.8 ± 4.6 | 0.0001 |
| RA minor dimension (mm) | 33.4 ± 4.4 | 31.9 ± 3.5 | 35.1 ± 4.6 | 0.0001 |
| Tricuspid Peak E velocity (m/s) | 0.51 ± 0.12 | 0.52 ± 0.11 | 0.50 ± 0.13 | 0.041 |
| Tricuspid Peak A velocity (m/s) | 0.37 ± 0.13 | 0.38 ± 0.13 | 0.36± 0.14 | 0.011 |
| Tricuspid Peak E/A ratio | 1.52 ± 0.61 | 1.501 ± 0.613 | 1.55 ± 0.607 | 0.196 |
| TAPSE (mm) | 23.6 ± 3.3 | 23.2 ± 3.0 | 24.1 ± 3.5 | 0.0001 |
| SPAP (mmHg) | 20.9 ± 5.9 | 21.2 ± 5.3 | 20.7 ± 6.5 | 0.143 |
| TAPSE/SPAP | 1.2 ± 0.4 | 1.1 ± 0.3 | 1.3 ± 0.5 | 0.0001 |
| RVOT AT (m/s) | 138.6 ± 17.5 | 139.6 ± 17.7 | 137.5 ± 17.1 | 0.062 |
| PVR (WU) | 1.3 ± 0.3 | 1.3 ± 0.3 | 1.3 ± 0.4 | 0.605 |
| (Mean ± SD) | Lower Limit | Upper Limit | |
|---|---|---|---|
| MEE (mL/s) | |||
| Overall | 61.09 ± 18.19 | 60.05 | 62.13 |
| Male | 67.27 ± 20.18 | 65.59 | 68.95 |
| Female | 54.71 ± 13.13 | 53.67 | 55.75 |
| MEEi (mL/s/g) | |||
| Overall | 0.45 ± 0.14 | 0.44 | 0.46 |
| Male | 0.43 ± 0.13 | 0.42 | 0.44 |
| Female | 0.47 ± 0.14 | 0.45 | 0.48 |
| Variables | Age Subgroups (y) | p-Value | Intragroup p-Value | ||
|---|---|---|---|---|---|
| 16–39 years | 40–59 years | >60 years | |||
| (Mean ± SD) | (Mean ± SD) | (Mean ± SD) | |||
| MEE | |||||
| Overall | 59.54 ± 17.44 | 61.41 ± 18.19 | 63.07 ± 19.33 | 0.086 | C: 0.026; |
| Male | 64.92 ± 18.74 | 68.32 ± 20.27 | 69.69 ± 22.56 | 0.15 | |
| Female | 52.59 ± 12.60 | 54.89 ± 13.01 | 57.35 ± 13.74 | 0.01 | C: 0.0031; |
| MEEi | |||||
| Overall | 0.46 ± 0.13 | 0.45 ± 0.14 | 0.43 ± 0.13 | 0.0045 | A: 0.032; C: 0.001; |
| Male | 0.44 ± 0.13 | 0.42 ± 0.14 | 0.42 ± 0.13 | 0.22 | NS |
| Female | 0.49 ± 0.14 | 0.47 ± 0.14 | 0.43 ± 0.14 | <0.001 | A: 0.037; B: 0.025; C: <0.001; |
| Estimate | Std. Error | p-Value | |
|---|---|---|---|
| (Intercept) | 0.417 | 0.158 | 0.008 |
| Female | −0.146 | 0.024 | <0.001 |
| BSA | 0.219 | 0.070 | 0.001 |
| BMI | −0.003 | 0.003 | 0.331 |
| DBP | −0.003 | 0.001 | <0.001 |
| LAVI | 0.009 | 0.001 | <0.001 |
| E/e’ | 0.015 | 0.005 | 0.003 |
| TAPSE | 0.015 | 0.003 | <0.001 |
| Estimate | Std. Error | p-Value | |
|---|---|---|---|
| (Intercept) | 0.605 | 0.163 | <0.001 |
| AGE | 0.002 | 0.000 | 0.002 |
| Female | −0.153 | 0.024 | <0.001 |
| BSA | 0.205 | 0.072 | 0.004 |
| BMI | −0.004 | 0.003 | 0.243 |
| SBP | −0.024 | 0.029 | 0.418 |
| DBP | 0.019 | 0.029 | 0.515 |
| PP | 0.023 | 0.029 | 0.426 |
| E/e’ | 0.007 | 0.005 | 0.217 |
| TAPSE | 0.019 | 0.003 | <0.001 |
| Study | N. | Gender (F/M) | BMI (kg/m2) | Age (y) | CVRF | EF (%) | MEE (mL/s) | MEEi (mL/s/g) | Remarks |
|---|---|---|---|---|---|---|---|---|---|
| De Simone G. et al. Journal of Hypertension 2009 [2] | 255 | 151/105 | 27.1 ± 6.6 | 35.3 ± 11.9 | Healthy subjects—no CVRF | 64.6 ± 4.9 | 86.1 ± 25.7 | - | Volunteers involved in a screening program of the department staff or subjects referred to the “Outpatient Nutrition Clinic”. |
| 56 | 26/29 | 27.9 ± 4.8 | 49.3 ± 9.5 | Hypertension | 63.1 ± 6.09 | Low MEE | - | Subjects were divided in groups with normal and low myocardial mechanical efficiency (i.e., below the 90th percentile of the normal distribution; normal distribution: 85.4 ± 22.6) .After adjusting for age and sex, hypertensive patients with low MEE showed greater relative wall thickness and lower EF and midwall shortening than patients with normal MEE. Low MEE was also associated with inappropriately high LV mass. | |
| 250 | 103/148 | 27.9 ± 4.3 | 47.1 ± 10.6 | Hypertension | 66.5 ± 5.4 | Normal MEE | - | ||
| De Simone G. et al. Journal of Hypertension 2016 [3] | 12353 | 5429/7008 | - | 52.4 ± 12.5 | Hypertension (100%), obesity (26%), diabetes (10%) * | 66.3 ± 3.9 | 62.6 ± 14.4 | F:0.35 ± 0.08 M:0.33 ± 0.07 | Patients selected from the Campania Salute Network (CSN) Registry. Low MEE was associated with altered metabolic profile, LVH, concentric left ventricular geometry, and diastolic dysfunction and predicted CV end-points, independently of age, sex, LVH antihypertensive therapy, and CVRF. |
| Mancusi C. et al. Journal of Clinical Medicine 2021 [4] | 111 | F 42% | 33 ± 5 | 48 ± 9 | Hypertension (85%), obesity (75%), diabetes (10%) ** | 61 ± 6 | - | ≤0.41 | Subjects participating in the fat-associated cardiovascular dysfunction (FATCOR) study. Reduced MEEi was associated with lower LV myocardial function both in the circumferential and in the longitudinal direction, independent of cardiometabolic factors. |
| 120 | F 58% | 32 ± 4 | 49 ± 9 | Hypertension (76%), obesity (62%), diabetes (9%) ** | 62 ± 7 | - | 0.42–0.54 | ||
| 125 | F 68% | 32 ± 4 | 46 ± 9 | Hypertension (71%), obesity (67%), diabetes (4%) ** | 64 ± 6 | - | 0.54–0.67 | ||
| 124 | F 75% | 31 ± 4 | 47 ± 9 | Hypertension (65%), obesity (48%), diabetes (7.5%) ** | 63 ± 6 | - | ≥0.67 | ||
| Losi MA. et al. Journal of Clinical Medicine 2019 [5] | 478 | F 55% | 60 ± 8 | Hypertension (34%), obesity (58%), diabetes (57%), hyperlipemia (62%), former smoker (38%), current smoker (35%) * | - | - | ≤0.34 | Data from the “Strong Heart Study” (SHS), a population-based cohort with CVRF but free of CV disease. A low LV MEEi was a predictor of incident, non-AMI related HF in subjects with initially normal EF. | |
| 479 | F 65% | 59 ± 8 | Hypertension (29%), obesity (57%), diabetes (41%), hyperlipemia (59%), former smoker (36%), current smoker (34%) * | - | - | 0.35–0.39 | |||
| 477 | F 69% | 60 ± 8 | Hypertension (25%), obesity (51%), diabetes (37%), hyperlipemia (55%), former smoker (34%), current smoker (35%) * | - | - | 0.40–0.44 | |||
| 478 | F 68% | 59 ± 8 | Hypertension (22%), obesity (40%), diabetes (25%), hyperlipemia (57%), former smoker (33%), current smoker (39%) * | - | - | ≥0.45 | |||
| Manzi MV. et al. ESC Heart Fail. 2022 [6] | 5536 | F 42.1% | 53.40 ± 11.41 | Hypertension (100%), obesity (24.3%), diabetes (9.8%), smoker (19.1%) * | 65.8 ± 3.86 | - | 0.34 ± 0.07 | Patients selected from the Campania Salute Network (CSN) Registry. Lower values of MEEi at baseline significantly contributed to identify patients more prone to develop LV systolic dysfunction. | |
| 137 | F 38% | 59.46 ± 11.58 | Hypertension (100%), obesity (27%), diabetes (18.2%), smoker (19%) * | 65.2 ± 11.5 | - | 0.32 ± 0.08 | |||
| Bahlmann E. et al. Open Heart 2021 [18] | 569 | F 35% | 27.9 ± 4.7 | 68 ± 10 | Hypertension (88%), obesity (28%) *** | 65 ± 7 | - | <0.34–0.26 ± 0.06 | Post hoc analysis performed within the prospective Simvastatin and Ezetimibe in Aortic Stenosis (SEAS) study. In patients with initially asymptomatic aortic stenosis, a low MEEi was associated with clustering of cardiometabolic risk factors, lower LV myocardial function and subsequent increased mortality during a 4.3 year follow-up, independent of known prognosticators. |
| 1134 | F 41% | 26.3 ± 4.1 | 67 ± 10 | Hypertension (81%), obesity (16%) *** | 67 ± 6 | - | ≥0.34–0.54 ± 0.16 | ||
| Fiorentino TV et al. Diabetes Research and Clinical Practice 2021 [7] | 617 NGT 1 h-low (1) | 389/228 | 29.4 ± 6.6 | 44 ± 13 | ≥1 cardio-metabolic risk factors **** | - | - | 0.41 ± 0.11 | The study cohort consisted of 1467 non-diabetic adult subjects participating in the CATAMERI study. Subjects with NGT 1 h-high, isolated IFG, and IGT had a raised myocardial oxygen consumption and a reduced MEE. |
| 210 NGT 1 h-high (2) | 100/110 | 30.1 ± 5.9 | 49 ± 12 | ≥1 cardio-metabolic risk factors **** | - | - | 0.38 ± 0.11 | ||
| 237 Isolated IFG (3) | 94/143 | 30.3 ± 5.3 | 54 ± 11 | ≥1 cardio-metabolic risk factors **** | - | - | 0.37 ± 0.10 | ||
| 403 IGT (4) | 217/186 | 31.4 ± 5.9 | 54 ± 12 | ≥1 cardio-metabolic risk factors **** | - | - | 0.35 ± 0.09 | ||
| Cioffi G. et al. Journal of Hypertension 2021 [8] | 432 | F 64% | 26.0 ± 4.5 | 57 ± 12 | Hypertension (46%), obesity (16%), diabetes (9%), hyperlipemia (56%), active smoker (34%) | 66 ±7 | - | 0.35 ± 0.11 | The study population consisted of 432 outpatients with established chronic inflammatory arthritis without overt cardiac disease, compared to 216 patients without chronic inflammatory arthritis. In patients with chronic inflammatory arthritis, a low-MEE was a powerful prognosticator of adverse CV events. |
| 216 | F 58% | 25.4 ± 4.3 | 59 ± 14 | Hypertension (46%), obesity (16%), diabetes (9%), hyperlipemia (56%), active smoker (34%) | 64 ± 9 | - | 0.45 ± 0.10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferrara, F.; Capone, V.; Cademartiri, F.; Vriz, O.; Cocchia, R.; Ranieri, B.; Franzese, M.; Castaldo, R.; D’Andrea, A.; Citro, R.; et al. Physiologic Range of Myocardial Mechano-Energetic Efficiency among Healthy Subjects: Impact of Gender and Age. J. Pers. Med. 2022, 12, 996. https://doi.org/10.3390/jpm12060996
Ferrara F, Capone V, Cademartiri F, Vriz O, Cocchia R, Ranieri B, Franzese M, Castaldo R, D’Andrea A, Citro R, et al. Physiologic Range of Myocardial Mechano-Energetic Efficiency among Healthy Subjects: Impact of Gender and Age. Journal of Personalized Medicine. 2022; 12(6):996. https://doi.org/10.3390/jpm12060996
Chicago/Turabian StyleFerrara, Francesco, Valentina Capone, Filippo Cademartiri, Olga Vriz, Rosangela Cocchia, Brigida Ranieri, Monica Franzese, Rossana Castaldo, Antonello D’Andrea, Rodolfo Citro, and et al. 2022. "Physiologic Range of Myocardial Mechano-Energetic Efficiency among Healthy Subjects: Impact of Gender and Age" Journal of Personalized Medicine 12, no. 6: 996. https://doi.org/10.3390/jpm12060996