
Number of Teeth and Nutritional Status Parameters Are Related to Intima-Media Thickness in Dalmatian Kidney Transplant Recipients

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
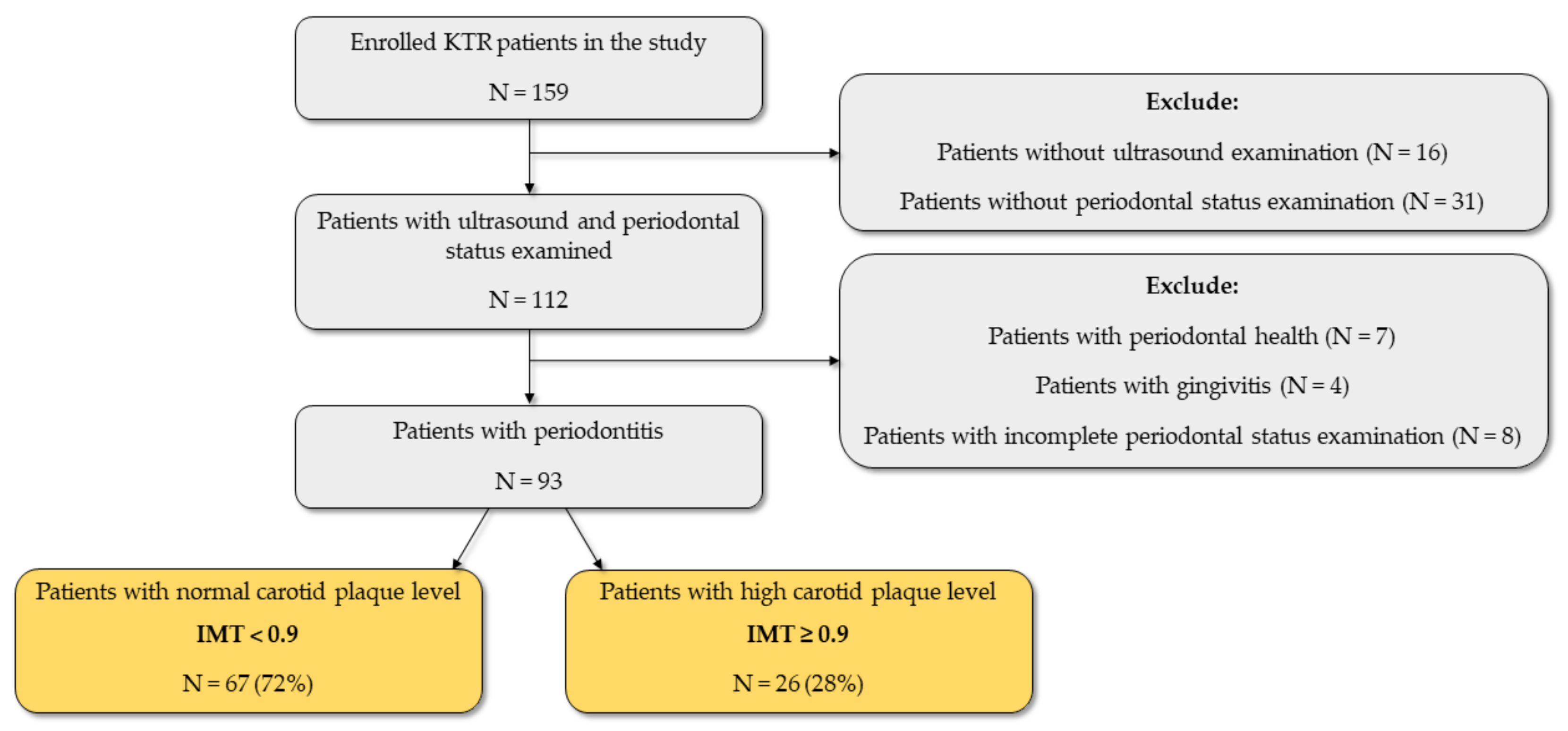
2.1. Study Design and Population
2.2. Medical History, Clinical and Laboratory Parameters
2.2.1. Ultrasound Examination
2.2.2. Body Composition and Anthropometry Measurements
2.2.3. Advanced Glycation End-Product (AGE) Measurement
2.2.4. Central Blood Pressure and Arterial Stiffness Measurement
2.2.5. Periodontal Status Examination
2.3. Statistical Analyses
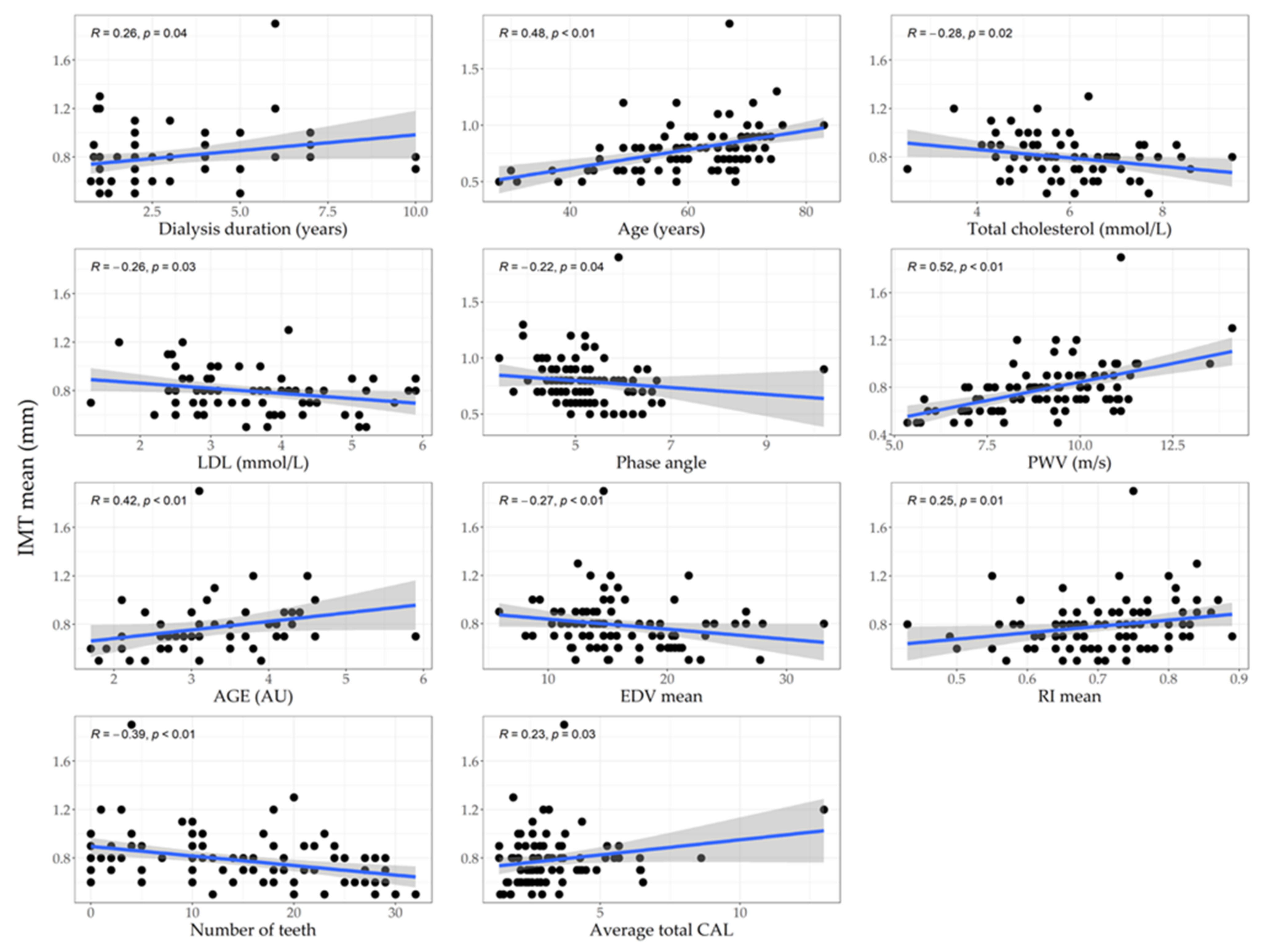
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gansevoort, R.T.; Correa-Rotter, R.; Hemmelgarn, B.R.; Jafar, T.H.; Heerspink, H.J.L.; Mann, J.F.; Matsushita, K.; Wen, C.P. Chronic Kidney Disease and Cardiovascular Risk: Epidemiology, Mechanisms, and Prevention. Lancet 2013, 382, 339–352. [Google Scholar] [CrossRef]
- Voora, S.; Adey, D.B. Management of Kidney Transplant Recipients by General Nephrologists: Core Curriculum 2019. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2019, 73, 866–879. [Google Scholar] [CrossRef] [PubMed]
- Glicklich, D.; Vohra, P. Cardiovascular risk assessment before and after kidney transplantation. Cardiol. Rev. 2014, 22, 153–162. [Google Scholar] [CrossRef] [PubMed]
- Pita-Fernández, S.; Pértega-Díaz, S.; Valdés-Cañedo, F.; Seijo-Bestilleiro, R.; Seoane-Pillado, T.; Fernández-Rivera, C.; Alonso-Hernández, A.; Lorenzo-Aguiar, D.; López-Calvino, B.; López-Muñiz, A. Incidence of cardiovascular events after kidney transplantation and cardiovascular risk scores: Study protocol. BMC Cardiovasc. Disord. 2011, 10, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- London, G.; Covic, A.; Goldsmith, D.; Wiecek, A.; Suleymanlar, G.; Ortiz, A.; Massy, Z.; Lindholm, B.; Martinez-Castelao, A.; Fliser, D.; et al. Arterial Aging and Arterial Disease: Interplay between Central Hemodynamics, Cardiac Work, and Organ Flow—Implications for CKD and Cardiovascular Disease. Kidney Int. Suppl. 2011, 1, 10–12. [Google Scholar] [CrossRef] [Green Version]
- Kolonko, A.; Chudek, J.; Szotowska, M.; Kuczera, P.; Wiecek, A. Cardiovascular Risk Factors and Markers of Atherosclerosis in Stable Kidney Transplant Recipients. Transplant. Proc. 2016, 48, 1543–1550. [Google Scholar] [CrossRef]
- Steenbeke, M.; Speeckaert, R.; Desmedt, S.; Glorieux, G.; Delanghe, J.R.; Speeckaert, M.M. The Role of Advanced Glycation End Products and Its Soluble Receptor in Kidney Diseases. Int. J. Mol. Sci. 2022, 23, 3439. [Google Scholar] [CrossRef]
- Georgianos, P.I.; Pikilidou, M.I.; Liakopoulos, V.; Balaskas, E.V.; Zebekakis, P.E. Arterial Stiffness in End-Stage Renal Disease—Pathogenesis, Clinical Epidemiology, and Therapeutic Potentials. Hypertens. Res. 2018, 41, 309–319. [Google Scholar] [CrossRef]
- Korogiannou, M.; Xagas, E.; Marinaki, S.; Sarafidis, P.; Boletis, J.N. Arterial Stiffness in Patients with Renal Transplantation; Associations with Co-morbid Conditions, Evolution, and Prognostic Importance for Cardiovascular and Renal Outcomes. Front. Cardiovasc. Med. 2019, 24, 67. [Google Scholar] [CrossRef] [Green Version]
- Kabłak-Ziembicka, A.; Przewłocki, T. Clinical Significance of Carotid Intima-Media Complex and Carotid Plaque Assessment by Ultrasound for the Prediction of Adverse Cardiovascular Events in Primary and Secondary Care Patients. J. Clin. Med. 2021, 10, 4628. [Google Scholar] [CrossRef]
- Nezami, N.; Ghabili, K.; Shokouhi-Gogani, B.; Mirchi, M.; Ghojazadeh, M.; Safa, J.; Zomorrodi, A.; Gharadaghi, A.; Mojadidi, M.K.; Tarzamni, M.K.; et al. The Relationship between Carotid and Femoral Artery Intima-Media Thickness and Histopathologic Grade of Atherosclerosis in Patients with Chronic Kidney Disease. Nephron 2018, 139, 159–169. [Google Scholar] [CrossRef]
- Nafar, M.; Khatami, F.; Kardavani, B.; Farjad, R.; Pour-Reza-Gholi, F.; Firoozan, A. Atherosclerosis after Kidney Transplantation: Changes of Intima-Media Thickness of Carotids During Early Posttransplant Period. Urol. J. 2007, 4, 105–110. [Google Scholar]
- Yilmaz, M.I.; Sonmez, A.; Saglam, M.; Cayci, T.; Kilic, S.; Unal, H.U.; Karaman, M.; Cetinkaya, H.; Eyileten, T.; Gok, M.; et al. A Longitudinal Study of Inflammation, CKD-Mineral Bone Disorder, and Carotid Atherosclerosis after Renal Transplantation. Clin. J. Am. Soc. Nephrol. 2015, 10, 471–479. [Google Scholar] [CrossRef] [Green Version]
- Recio-Mayoral, A.; Banerjee, D.; Streather, C.; Kaski, J.C. Endothelial Dysfunction, Inflammation and Atherosclerosis in Chronic Kidney Disease—A Cross-Sectional Study of Predialysis, Dialysis and Kidney-Transplantation Patients. Atherosclerosis 2011, 216, 446–451. [Google Scholar] [CrossRef]
- Wei, T.; Liu, J.; Zhang, D.; Wang, X.; Li, G.; Ma, R.; Chen, G.; Lin, X.; Guo, X. The Relationship between Nutrition and Atherosclerosis. Front. Bioeng. Biotechnol. 2021, 9, 635504. [Google Scholar] [CrossRef]
- Hwang, J.H.; Ryu, J.; An, J.N.; Kim, C.T.; Kim, H.; Yang, J.; Ha, J.; Chae, D.W.; Ahn, C.; Jung, I.M.; et al. Pretransplant Malnutrition, Inflammation, and Atherosclerosis Affect Cardiovascular Outcomes after Kidney Transplantation. BMC Nephrol. 2015, 16, 109. [Google Scholar] [CrossRef] [Green Version]
- Goldfarb Cyrino, L.; Galpern, J.; Moore, L.; Borgi, L.; Riella, L.V. A Narrative Review of Dietary Approaches for Kidney Transplant Patients. Kidney Int. Rep. 2021, 6, 1764–1774. [Google Scholar] [CrossRef]
- Hanna, R.M.; Ghobry, L.; Wassef, O.; Rhee, C.M.; Kalantar-Zadeh, K. A Practical Approach to Nutrition, Protein-Energy Wasting, Sarcopenia, and Cachexia in Patients with Chronic Kidney Disease. Blood Purif. 2020, 49, 202–211. [Google Scholar] [CrossRef]
- Sabbatini, M.; Ferreri, L.; Pisani, A.; Capuano, I.; Morgillo, M.; Memoli, A.; Riccio, E.; Guida, B. Nutritional Management in Renal Transplant Recipients: A Transplant Team Opportunity to Improve Graft Survival. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 319–324. [Google Scholar] [CrossRef]
- Sgambat, K.; Amalya, K.; Moudgil, A. Nutritional Challenges across the Spectrum of Chronic Kidney Disease. Asian J. Pediatr. Nephrol. 2019, 2, 2. [Google Scholar]
- Kassebaum, N.J.; Bernabé, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.L.; Marcenes, W. Global Burden of Severe Periodontitis in 1990–2010. J. Dent. Res. 2014, 93, 1045–1053. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Jepsen, S.; Jin, L.; Otomo-Corgel, J. Impact of the Global Burden of Periodontal Diseases on Health, Nutrition and Wellbeing of Mankind: A Call for Global Action. J. Clin. Periodontol. 2017, 44, 456–462. [Google Scholar] [CrossRef] [Green Version]
- Sanz, M.; Marco del Castillo, A.; Jepsen, S.; Gonzalez-Juanatey, J.R.; D’Aiuto, F.; Bouchard, P.; Chapple, I.; Dietrich, T.; Gotsman, I.; Graziani, F.; et al. Periodontitis and Cardiovascular Diseases: Consensus Report. J. Clin. Periodontol. 2020, 47, 268–288. [Google Scholar] [CrossRef]
- Nunes-dos-Santos, D.L.; Gomes, S.V.; Rodrigues, V.P.; Pereira, A.L.A. Periodontal Status and Clinical Outcomes in Kidney Transplant Recipients: A Systematic Review. Oral Dis. 2020, 26, 22–34. [Google Scholar] [CrossRef]
- Chen, J.H.; Lin, X.; Bu, C.; Zhang, X. Role of advanced glycation end products in mobility and considerations in possible dietary and nutritional intervention strategies. Nutr. Metab. 2018, 15, 72. [Google Scholar] [CrossRef]
- Stinghen, A.E.; Massy, Z.A.; Vlassara, H.; Striker, G.E.; Boullier, A. Uremic Toxicity of Advanced Glycation End Products in CKD. J. Am. Soc. Nephrol. JASN 2016, 27, 354–370. [Google Scholar] [CrossRef] [Green Version]
- Colombo, G.; Reggiani, F.; Astori, E.; Altomare, A.; Finazzi, S.; Garavaglia, M.L.; Angelini, C.; Milzani, A.; Badalamenti, S.; Dalle-Donne, I. Advanced oxidation protein products in nondiabetic end stage renal disease patients on maintenance haemodialysis. Free. Radic. Res. 2019, 53, 1114–1124. [Google Scholar] [CrossRef] [PubMed]
- Sotomayor, C.G.; Gomes-Neto, A.W.; van Londen, M.; Gans, R.O.B.; Nolte, I.M.; Berger, S.P.; Navis, G.J.; Rodrigo, R.; Leuvenink, H.G.D.; Schalkwijk, C.G.; et al. Circulating Advanced Glycation Endproducts and Long-Term Risk of Cardiovascular Mortality in Kidney Transplant Recipients. Clin. J. Am. Soc. Nephrol. CJASN 2019, 14, 1512–1520. [Google Scholar] [CrossRef] [PubMed]
- Calviño, J.; Cigarran, S.; Gonzalez-Tabares, L.; Menendez, N.; Latorre, J.; Cillero, S.; Millan, B.; Cobelo, C.; Sanjurjo-Amado, A.; Quispe, J.; et al. Advanced glycation end products (AGEs) estimated by skin autofluorescence are related with cardiovascular risk in renal transplant. PLoS ONE 2018, 13, e0201118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baskal, S.; Post, A.; Kremer, D.; Bollenbach, A.; Bakker, S.J.L.; Tsikas, D. Urinary excretion of amino acids and their advanced glycation end-products (AGEs) in adult kidney transplant recipients with emphasis on lysine: Furosine excretion is associated with cardiovascular and all-cause mortality. Amino Acids 2021, 53, 1679–1693. [Google Scholar] [CrossRef] [PubMed]
- Almengló, C.; Rodriguez-Ruiz, E.; Alvarez, E.; López-Lago, A.; González-Juanatey, J.R.; Garcia-Allut, J.L. Minimal Invasive Fluorescence Methods to Quantify Advanced Glycation End Products (AGEs) in Skin and Plasma of Humans. Methods 2021, 203, 103–107. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and Grading of Periodontitis: Framework and Proposal of a New Classification and Case Definition. J. Periodontol. 2018, 89, S159–S172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kursa, M.B.; Rudnicki, W.R. Feature Selection with the Boruta Package. J. Stat. Softw. 2010, 36, 1–13. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: https://www.r-project.org/.
- Tyrrell, D.J.; Goldstein, D.R. Ageing and Atherosclerosis: Vascular Intrinsic and Extrinsic Factors and Potential Role of IL-6. Nat. Rev. Cardiol. 2021, 18, 58–68. [Google Scholar] [CrossRef]
- Ossareh, S.; Alaei, A.; Saedi, D. Dialysis Carotid Intima-Media Thickness in Maintenance Hemodialysis Patients Role of Cardiovascular Risk Factor. Iran. J. Kidney Dis. 2011, 5, 169–174. [Google Scholar] [PubMed]
- Aghaghazvini, L.; Hakemi, M.; Vaghardoost, A.; Shakiba, M.; Saberi-Demneh, A.; Fathi, M. The Effect of Kidney Transplantation on Carotid Artery Intima-Media Thickness in End-Stage Renal Disease Patients. SN Compr. Clin. Med. 2019, 1, 855–860. [Google Scholar] [CrossRef] [Green Version]
- Mineoka, Y.; Ishii, M.; Hashimoto, Y.; Nakamura, N.; Fukui, M. Malnutrition Assessed by Controlling Nutritional Status Is Correlated to Carotid Atherosclerosis in Patients with Type 2 Diabetes. Endocr. J. 2019, 66, 1073–1082. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holmlund, A.; Lind, L. Number of Teeth Is Related to Atherosclerotic Plaque in the Carotid Arteries in an Elderly Population. J. Periodontol. 2012, 83, 287–291. [Google Scholar] [CrossRef] [PubMed]
- Nakashima, A.; Yorioka, N.; Asakimori, Y.; Ito, T.; Masaki, T.; Shigemoto, K.; Harada, S. Different risk factors for the maximum and the mean carotid intima-media thickness in hemodialysis patients. Intern. Med. 2003, 42, 1095–1099. [Google Scholar] [CrossRef] [Green Version]
- Ruospo, M.; Palmer, S.C.; Craig, J.C.; Gentile, G.; Johnson, D.W.; Ford, P.J.; Tonelli, M.; Petruzzi, M.; de Benedittis, M.; Strippoli, G.F.M. Prevalence and Severity of Oral Disease in Adults with Chronic Kidney Disease: A Systematic Review of Observational Studies. Nephrol. Dial. Transplant. 2014, 29, 364–375. [Google Scholar] [CrossRef]
- Butera, A.; Gallo, S.; Pascadopoli, M.; Maiorani, C.; Milone, A.; Alovisi, M.; Scribante, A. Paraprobiotics in Non-Surgical Periodontal Therapy: Clinical and Microbiological Aspects in a 6-Month Follow-Up Domiciliary Protocol for Oral Hygiene. Microorganisms 2022, 10, 337. [Google Scholar] [CrossRef]
- Butera, A.; Gallo, S.; Maiorani, C.; Molino, D.; Chiesa, A.; Preda, C.; Esposito, F.; Scribante, A. Probiotic Alternative to Chlorhexidine in Periodontal Therapy: Evaluation of Clinical and Microbiological Parameters. Microorganisms 2021, 9, 69. [Google Scholar] [CrossRef]
- Hitz Lindenmüller, I.; Lambrecht, J.T. Oral Care. In Topical Applications and the Mucosa; KARGER: Basel, Switzerland, 2011. [Google Scholar]
- Rocha, E. Pulse Wave Velocity: A Marker of Arterial Stiffness and Its Applicability in Clinical Practice. Rev. Port. Cardiol. 2011, 30, 699–702. [Google Scholar] [CrossRef]
- Lawence-Brown, M.; Liffman, K.; Semmens, J.; Sutalo, I. Vascular Arterial Haemodynamics. In Mechanisms of Vascular Disease: A Reference Book for Vascular Specialists; University of Adelaide: Adelaide, SA, Australia, 2011. [Google Scholar]
- Mallamaci, F.; Tripepi, R.; Leonardis, D.; Mafrica, A.; Versace, M.C.; Provenzano, F.; Tripepi, G.; Zoccali, C. Nocturnal Hypertension and Altered Night–Day BP Profile and Atherosclerosis in Renal Transplant Patients. Transplantation 2016, 100, 2211–2218. [Google Scholar] [CrossRef]
- Grobbee, D.E.; Bots, M.L. Carotid Artery Intima-Media Thickness as an Indicator of Generalized Atherosclerosis. J. Intern. Med. 1994, 236, 567–573. [Google Scholar] [CrossRef]
- Devine, P.A.; Courtney, A.E.; Maxwell, A.P. Cardiovascular risk in renal transplant recipients. J. Nephrol. 2019, 32, 389–399. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, A.; Saez, A.; Kos, M.; Witzke, O.; Kribben, A.; Nürnberger, J. Pulse Wave Velocity Predicts Mortality in Renal Transplant Patients. Eur. J. Med. Res. 2010, 15, 452. [Google Scholar] [CrossRef] [Green Version]
- Birdwell, K.A.; Jaffe, G.; Bian, A.; Wu, P.; Ikizler, T.A. Assessment of Arterial Stiffness Using Pulse Wave Velocity in Tacrolimus Users the First Year Post Kidney Transplantation: A Prospective Cohort Study. BMC Nephrol. 2015, 16, 93. [Google Scholar] [CrossRef] [Green Version]
- Prasad, K. AGE–RAGE Stress: A Changing Landscape in Pathology and Treatment of Alzheimer’s Disease. Mol. Cell. Biochem. 2019, 459, 95–112. [Google Scholar] [CrossRef]
- Oleniuc, M.; Schiller, A.; Secara, I.; Onofriescu, M.; Hogas, S.; Apetrii, M.; Siriopol, D.; Covic, A. Evaluation of Advanced Glycation End Products Accumulation, Using Skin Autofluorescence, in CKD and Dialysis Patients. Int. Urol. Nephrol. 2012, 44, 1441–1449. [Google Scholar] [CrossRef]
- Yamagishi, S.-I.; Matsui, T.; Ueda, S.-I.; Nakamura, K.; Imaizumi, T. Advanced Glycation End Products (AGEs) and Cardiovascular Disease (CVD) in Diabetes. Cardiovasc. Hematol. Agents Med. Chem. 2007, 5, 236–240. [Google Scholar] [CrossRef] [PubMed]
- Prasad, A.; Bekker, P.; Tsimikas, S. Advanced Glycation End Products and Diabetic Cardiovascular Disease. Cardiol. Rev. 2012, 20, 177–183. [Google Scholar] [CrossRef]
- Atzeni, I.M.; van de Zande, S.C.; Westra, J.; Zwerver, J.; Smit, A.J.; Mulder, D.J. The AGE Reader: A Non-Invasive Method to Assess Long-Term Tissue Damage. Methods 2021, 203, 533–541. [Google Scholar] [CrossRef] [PubMed]
- Goldin, A.; Beckman, J.A.; Schmidt, A.M.; Creager, M.A. Advanced Glycation End Products. Circulation 2006, 114, 597–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, V.P.; Bali, A.; Singh, N.; Jaggi, A.S. Advanced glycation end products and diabetic complications. Korean J. Physiol. Pharmacol. 2014, 18, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Kang, S.H.; Do, J.Y.; Kim, J.C. Impedance-Derived Phase Angle Is Associated with Muscle Mass, Strength, Quality of Life, and Clinical Outcomes in Maintenance Hemodialysis Patients. PLoS ONE 2022, 17, e0261070. [Google Scholar] [CrossRef]
- Kaya, E.; Bakir, A.; Koseoglu, Y.K.; Velidedeoglu, M.; Trabulus, S.; Seyahi, N. Association of Nutritional Assessment by Phase Angle with Mortality in Kidney Transplant Patients in an 8-Year Follow-Up. Prog. Transplant. 2019, 29, 321–326. [Google Scholar] [CrossRef]
- Yajima, T.; Yajima, K.; Takahashi, H.; Yasuda, K. The Impact of Abdominal Fat Levels on All-Cause Mortality Risk in Patients Undergoing Hemodialysis. Nutrients 2018, 10, 480. [Google Scholar] [CrossRef] [Green Version]
- Kalantar-Zadeh, K.; Block, G.; Humphreys, M.H.; Kopple, J.D. Reverse Epidemiology of Cardiovascular Risk Factors in Maintenance Dialysis Patients. Kidney Int. 2003, 63, 793–808. [Google Scholar] [CrossRef] [Green Version]
- Sezer, S.; Karakan, Ş.; Şaşak, G.; Tutal, E.; Özdemir Acar, F.N. Body Fat Percentage as a Risk Factor for Atherosclerosis but Not for Inflammation for Hemodialysis Patients: Differences between Genders. J. Ren. Nutr. 2012, 22, 490–498. [Google Scholar] [CrossRef]
- Yin, S.; Wu, L.; Huang, Z.; Fan, Y.; Lin, T.; Song, T. Nonlinear Relationship between Body Mass Index and Clinical Outcomes after Kidney Transplantation: A Dose-Response Meta-Analysis of 50 Observational Studies. Surgery 2021, 171, 1396–1405. [Google Scholar] [CrossRef]
- Battaglia, Y.; Cojocaru, E.; Fiorini, F.; Granata, A.; Esposito, P.; Russo, L.; Bortoluzzi, A.; Storari, A.; Russo, D. Vitamin D in Kidney Transplant Recipients. Clin. Nephrol. 2020, 93, 57–64. [Google Scholar] [CrossRef]
- Hartog, J.W.L.; de Vries, A.P.J.; Lutgers, H.L.; Meerwaldt, R.; Huisman, R.M.; van Son, W.J.; de Jong, P.E.; Smit, A.J. Accumulation of Advanced Glycation End Products, Measured as Skin Autofluorescence, in Renal Disease. Ann. N. Y. Acad. Sci. 2005, 1043, 299–307. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| All (N = 93) | IMT < 0.9 mm (N = 67) | IMT ≥ 0.9 mm (N = 26) | p | |
|---|---|---|---|---|
| Time since transplantation (years), median (IQR) | 4.5 (6.62) | 4 (6.25) | 6 (6.5) | 0.206 |
| Dialysis type, N (%) | ||||
| PD | 35 (38.04) | 26 (39.39) | 9 (34.62) | 0.686 |
| HD | 51 (55.43) | 35 (53.03) | 16 (61.54) | |
| PD + HD | 6 (6.52) | 5 (7.58) | 1 (3.85) | |
| Dialysis duration (years), median (IQR) | 2 (3) | 2 (2) | 3.5 (2.25) | 0.130 |
| Age (years), median (IQR) | 62 (14) | 59 (15) | 69.5 (7.75) | <0.001 |
| Sex, N (%) | ||||
| Women | 43 (46.24) | 34 (50.75) | 9 (34.62) | 0.243 |
| Men | 50 (53.76) | 33 (49.25) | 17 (65.38) | |
| Presence of arterial hypertension, N (%) | ||||
| No | 12 (12.9) | 10 (14.93) | 2 (7.69) | 0.556 |
| Yes | 81 (87.1) | 57 (85.07) | 24 (92.31) | |
| Presence of diabetes mellitus, N (%) | ||||
| No | 73 (78.49) | 54 (80.6) | 19 (73.08) | 0.609 |
| Yes | 20 (21.51) | 13 (19.4) | 7 (26.92) | |
| Smoking status, N (%) | ||||
| Nonsmoker | 41 (48.81) | 29 (47.54) | 12 (52.17) | 0.690 |
| Former smoker | 27 (32.14) | 19 (31.15) | 8 (34.78) | |
| Smoker | 16 (19.05) | 13 (21.31) | 3 (13.04) | |
| Presence of chronic kidney disease, N (%) | ||||
| eGFR > 60 mL/min/1.73 m2 | 27 (30.34) | 18 (28.12) | 9 (36) | 0.638 |
| eGFR < 60 mL/min/1.73 m2 | 62 (69.66) | 46 (71.88) | 16 (64) | |
| Laboratory parameters | ||||
| Alb (g/L), median (IQR) | 42 (4.75) | 42 (5) | 42 (4.25) | 0.878 |
| Ca (mmol/L), median (IQR) | 2.43 (0.17) | 2.44 (0.18) | 2.42 (0.12) | 0.711 |
| CRP (mg/L), median (IQR) | 2.5 (3.78) | 2.6 (3.75) | 1.8 (2.7) | 0.406 |
| E, median (IQR) | 4.71 (0.65) | 4.69 (0.65) | 4.78 (0.66) | 0.546 |
| GUP (mmol/L), median (IQR) | 5.3 (0.88) | 5.34 (0.82) | 5.19 (1.04) | 0.483 |
| Hb (g/L), median (IQR) | 135.24 (15.97) | 133.67 (16.57) | 139.24 (13.82) | 0.140 |
| K (mmol/L), mean (SD) | 4.11 (0.49) | 4.13 (0.5) | 4.03 (0.44) | 0.375 |
| Total cholesterol (mmol/L), mean (SD) | 5.96 (1.27) | 6.2 (1.23) | 5.42 (1.2) | 0.016 |
| Creatinine (mmol/L), median (IQR) | 126 (59) | 127.5 (54.5) | 117 (50) | 0.246 |
| LDL (mmol/L), median (IQR) | 3.6 (1.03) | 3.75 (1.01) | 3.25 (1.04) | 0.056 |
| MCV (fL), mean (SD) | 87.89 (5.6) | 87.67 (5.88) | 88.44 (4.93) | 0.566 |
| Na (mmol/L), median (IQR) | 141 (3) | 141 (3) | 141 (3.25) | 0.984 |
| P (mmol/L), median (IQR) | 1 (0.22) | 1.01 (0.23) | 0.99 (0.15) | 0.263 |
| Tgl (mmol/L), median (IQR) | 1.8 (1.25) | 1.9 (1.1) | 1.65 (0.79) | 0.152 |
| Uric acid (mmol/L), median (IQR) | 394 (76.25) | 400 (81) | 387 (60) | 0.485 |
| Urea (mmol/L), median (IQR) | 9 (6) | 9.15 (5.47) | 8.9 (4.9) | 0.338 |
| eGFR (mL/min/1.73 m2), median (IQR) | 47.1 (27.4) | 46.35 (30.17) | 50.9 (26.9) | 0.235 |
| Anthropometric parameters | ||||
| BMI (kg/m2), mean (SD) | 26.84 (4.02) | 27.07 (4.36) | 26.29 (3.07) | 0.412 |
| Middle upper arm circumference (cm), median (IQR) | 30 (7) | 30 (5) | 27 (8.5) | 0.568 |
| Waist circumference (cm), mean (SD) | 101 (12.24) | 100.95 (12.89) | 101.17 (10.22) | 0.948 |
| WHtR, mean (SD) | 0.58 (0.07) | 0.58 (0.07) | 0.59 (0.06) | 0.927 |
| Body composition parameters | ||||
| Fat mass (kg), median (IQR) | 20.24 (8.49) | 21.43 (8.97) | 17.43 (6.6) | 0.044 |
| Fat mass (%), mean (SD) | 24.57 (8.58) | 25.7 (8.88) | 21.94 (7.31) | 0.061 |
| Fat-free mass (kg), median (IQR) | 60.2 (18.25) | 57.2 (16.5) | 64.6 (17.93) | 0.547 |
| Visceral fat, mean (SD) | 9.72 (3.82) | 9.4 (4.08) | 10.46 (3.09) | 0.239 |
| Muscle mass (kg), median (IQR) | 57.2 (17.4) | 54.3 (15.7) | 61.35 (17.05) | 0.547 |
| Skeletal muscle mass (kg), median (IQR) | 32 (11.4) | 31.1 (11.9) | 35.1 (11.12) | 0.650 |
| Skeletal muscle mass (%), median (IQR) | 40.78 (6.3) | 40.27 (6.67) | 41.98 (5.25) | 0.246 |
| Phase angle, median (IQR) | 5.1 (0.9) | 5.1 (0.8) | 4.95 (0.85) | 0.134 |
| Bone mass (kg), mean (SD) | 3.03 (0.54) | 3.01 (0.53) | 3.08 (0.55) | 0.572 |
| Trunk visceral fat (kg), mean (SD) | 10.63 (5.01) | 11.25 (5.28) | 9.2 (4.04) | 0.081 |
| Blood pressure parameters | ||||
| pSBP (mHg), mean (SD) | 134.14 (19.52) | 132.25 (18.87) | 139.17 (20.71) | 0.140 |
| pDBP (mHg), mean (SD) | 86.31 (12.85) | 85.8 (12.06) | 87.67 (14.97) | 0.546 |
| pMAP (mHg), mean (SD) | 109.27 (14.23) | 108.16 (13.67) | 112.5 (15.62) | 0.231 |
| pPP (mHg), mean (SD) | 50.88 (14) | 49.2 (12.27) | 55.79 (17.57) | 0.063 |
| cSBP (mHg), mean (SD) | 127.95 (17.6) | 126.07 (16.45) | 133.4 (20.03) | 0.100 |
| cDBP (mHg), mean (SD) | 86.98 (12.58) | 86.66 (12) | 87.93 (14.38) | 0.692 |
| cMAP (mHg), mean (SD) | 100.64 (13.15) | 99.8 (12.57) | 103.08 (14.76) | 0.327 |
| cPP (mHg), mean (SD) | 37.51 (11.73) | 36.21 (10.53) | 41.26 (14.29) | 0.089 |
| HR, mean (SD) | 71.47 (11.19) | 71.48 (11.11) | 71.44 (11.65) | 0.988 |
| PR, median (IQR) | 1.83 (0.35) | 1.83 (0.33) | 1.83 (0.46) | 0.852 |
| AIx, median (IQR) | 19.75 (19) | 19.5 (19) | 23 (17) | 0.865 |
| PWV (m/s), mean (SD) | 9.05 (1.75) | 8.55 (1.6) | 10.38 (1.43) | <0.001 |
| AGE (AU), mean (SD) | 3.26 (0.88) | 3.16 (0.89) | 3.58 (0.81) | 0.130 |
| Ultrasound parameters | ||||
| IMT mean, mean (SD) | 0.8 (0.2) | 0.7 (0.2) | 1 (0.18) | <0.001 |
| PSV mean, mean (SD) | 57.11 (13.33) | 56.88 (12.27) | 57.72 (15.99) | 0.786 |
| EDV mean, median (IQR) | 15 (6.55) | 15.85 (6.25) | 13.68 (2.9) | 0.007 |
| RI mean, mean (SD) | 0.71 (0.09) | 0.69 (0.09) | 0.75 (0.08) | 0.008 |
| Periodontal status parameters | ||||
| Number of teeth, median (IQR) | 14 (16) | 16 (13.5) | 10 (13.75) | 0.024 |
| Dental plaque (%), median (IQR) | 87.5 (40) | 87 (40) | 90 (40) | 0.611 |
| Bleeding (%), median (IQR) | 10 (26.75) | 13 (24) | 5 (34) | 0.457 |
| Average pocket depth, median (IQR) | 1.98 (0.84) | 2.08 (0.86) | 1.91 (0.79) | 0.340 |
| Average total CAL, median (IQR) | 2.86 (1.34) | 2.75 (1.41) | 2.97 (1.21) | 0.602 |
| Reason for tooth loss, N (%) | ||||
| Periodontitis | 39 (41.94) | 24 (35.82) | 15 (57.69) | 0.092 |
| Other | 54 (58.06) | 43 (64.18) | 11 (42.31) | |
| Periodontitis stage, N (%) | ||||
| I + II (mild) | 48 (51.61) | 39 (58.21) | 9 (34.62) | 0.070 |
| III + IV (severe) | 45 (48.39) | 28 (41.79) | 17 (65.38) | |
| Predictor | OR | 95% CI | p |
|---|---|---|---|
| Full model (Nagelkerke’s R2:0.566, AIC: 91.83) | |||
| Dialysis duration (years) | 1.29 | 0.9–1.85 | 0.172 |
| Age (years) | 1.1 | 0.93–1.3 | 0.278 |
| Sex (men) | 3.6 | 0.62–20.87 | 0.153 |
| Total cholesterol (mmol/L) | 0.57 | 0.07–4.43 | 0.591 |
| LDL (mmol/L) | 1.33 | 0.12–14.85 | 0.815 |
| Fat mass (kg) | 0.93 | 0.84–1.02 | 0.142 |
| Phase angle | 2.9 | 0.75–11.2 | 0.123 |
| PWV (m/s) | 2.49 | 1.05–5.92 | 0.038 |
| AGE (AU) | 0.51 | 0.18–1.48 | 0.218 |
| EDV mean | 0.87 | 0.68–1.11 | 0.266 |
| RI mean | 0 | 0–33.84 | 0.139 |
| Number of teeth | 0.87 | 0.77–0.99 | 0.035 |
| Average total CAL | 0.54 | 0.3–0.97 | 0.038 |
| Reduced model (after feature selection with Boruta; Nagelkerke’s R2: 0.513, AIC: 89.26) | |||
| Sex (men) | 3.45 | 0.8–14.91 | 0.098 |
| Age (years) | 1.02 | 0.89–1.18 | 0.765 |
| Total cholesterol (mmol/L) | 0.67 | 0.38–1.2 | 0.183 |
| Fat mass (kg) | 0.95 | 0.88–1.03 | 0.194 |
| PWV (m/s) | 2.4 | 1.02–5.64 | 0.045 |
| EDV mean | 0.89 | 0.72–1.11 | 0.313 |
| RI mean | 0 | 0–204.34 | 0.257 |
| N teeth | 0.88 | 0.79–0.98 | 0.024 |
| Average total CAL | 0.7 | 0.45–1.06 | 0.095 |
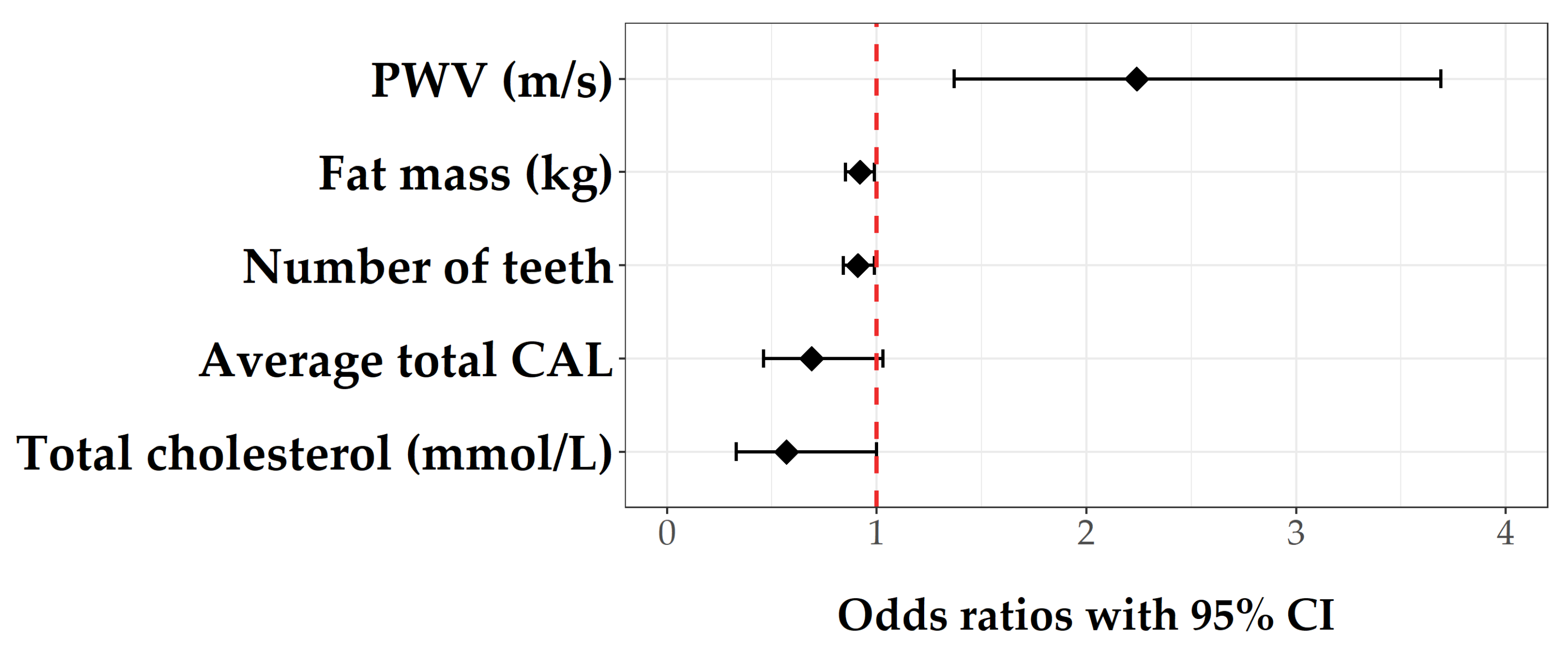
| Final model (after stepwise selection; Nagelkerke’s R2: 0.487, AIC: 83.88) | |||
| Total cholesterol (mmol/L) | 0.57 | 0.33–1 | 0.051 |
| Fat mass (kg) | 0.92 | 0.85–0.99 | 0.033 |
| PWV (m/s) * | 2.24 | 1.37–3.69 | 0.001 |
| Number of teeth | 0.91 | 0.84–0.99 | 0.032 |
| Average total CAL | 0.69 | 0.46–1.03 | 0.072 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dodig Novaković, M.; Lovrić Kojundžić, S.; Radić, M.; Vučković, M.; Gelemanović, A.; Roguljić, M.; Kovačević, K.; Orešković, J.; Radić, J. Number of Teeth and Nutritional Status Parameters Are Related to Intima-Media Thickness in Dalmatian Kidney Transplant Recipients. J. Pers. Med. 2022, 12, 984. https://doi.org/10.3390/jpm12060984
Dodig Novaković M, Lovrić Kojundžić S, Radić M, Vučković M, Gelemanović A, Roguljić M, Kovačević K, Orešković J, Radić J. Number of Teeth and Nutritional Status Parameters Are Related to Intima-Media Thickness in Dalmatian Kidney Transplant Recipients. Journal of Personalized Medicine. 2022; 12(6):984. https://doi.org/10.3390/jpm12060984
Chicago/Turabian StyleDodig Novaković, Maja, Sanja Lovrić Kojundžić, Mislav Radić, Marijana Vučković, Andrea Gelemanović, Marija Roguljić, Katja Kovačević, Josip Orešković, and Josipa Radić. 2022. "Number of Teeth and Nutritional Status Parameters Are Related to Intima-Media Thickness in Dalmatian Kidney Transplant Recipients" Journal of Personalized Medicine 12, no. 6: 984. https://doi.org/10.3390/jpm12060984