
The Sexual Dimorphism in Cerebrospinal Fluid Protein Content Does Not Affect Intrathecal IgG Synthesis in Multiple Sclerosis

 ,
,  ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients
2.3. Clinical Evaluations
2.4. Cerebrospinal Fluid Analysis
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Cerebrospinal Fluid (CSF) Characteristics
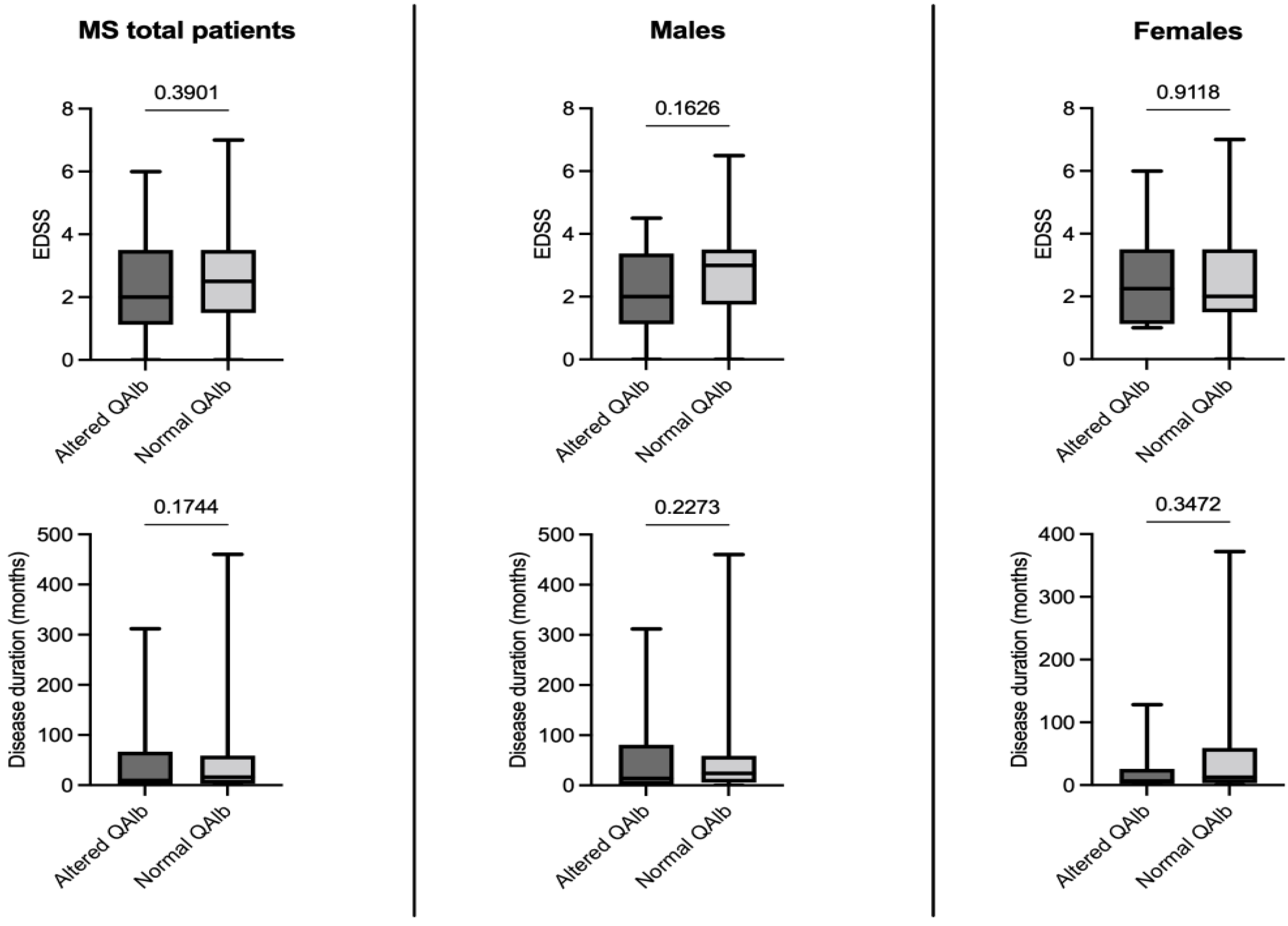
3.3. Effect of the Blood-Cerebrospinal Fluid-Barrier (BCSFB) Permeability on Disease Severity and Duration
3.4. Effect of Age on Disease Severity and Duration
3.5. Effect of Age on Quantitative Cerebrospinal Fluid Indexes
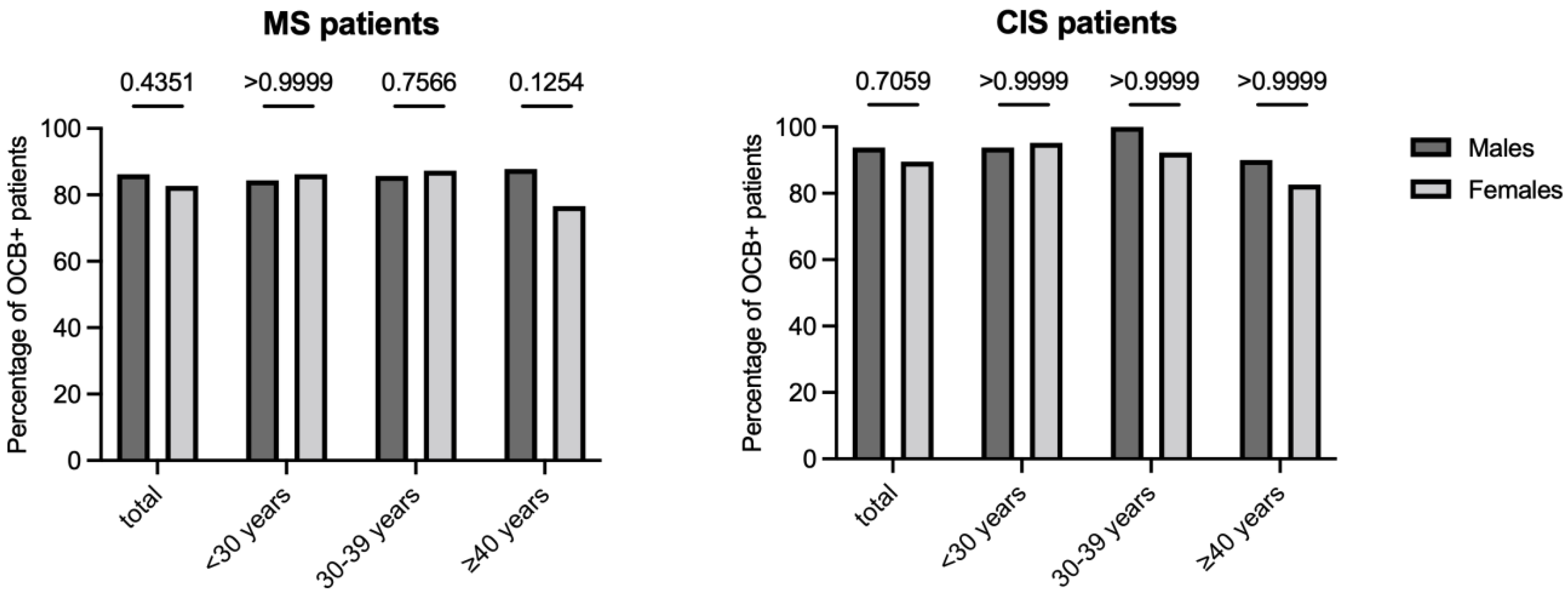
3.6. Impact of Sex and Age on IgG Oligoclonal Bands Determination
3.7. Impact of Sex on the Agreement between Quantitative and Qualitative Methods for the Determination of an Intrathecal IgG Synthesis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Thompson, A.J.; Baranzini, S.E.; Geurts, J.; Hemmer, B.; Ciccarelli, O. Multiple sclerosis. Lancet 2018, 391, 1622–1636. [Google Scholar] [CrossRef]
- McGinley, M.P.; Goldschmidt, C.H.; Rae-Grant, A.D. Diagnosis and Treatment of Multiple Sclerosis: A Review. JAMA 2021, 325, 765–779. [Google Scholar] [CrossRef] [PubMed]
- Voskuhl, R.R. The effect of sex on multiple sclerosis risk and disease progression. Mult. Scler. 2020, 26, 554–560. [Google Scholar] [CrossRef] [PubMed]
- Sadovnick, A.D. European Charcot Foundation Lecture: The natural history of multiple sclerosis and gender. J. Neurol. Sci. 2009, 286, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Confavreux, C.; Vukusic, S.; Moreau, T.; Adeleine, P. Relapses and progression of disability in multiple sclerosis. N. Engl. J. Med. 2000, 343, 1430–1438. [Google Scholar] [CrossRef]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S.; et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018, 17, 162–173. [Google Scholar] [CrossRef]
- Gilli, F.; DiSano, K.D.; Pachner, A.R. SeXX Matters in Multiple Sclerosis. Front. Neurol. 2020, 11, 616. [Google Scholar] [CrossRef]
- Miller, D.H.; Chard, D.T.; Ciccarelli, O. Clinically isolated syndromes. Lancet Neurol. 2012, 11, 157–169. [Google Scholar] [CrossRef]
- Holmøy, T. The discovery of oligoclonal bands: A 50-year anniversary. Eur. Neurol. 2009, 62, 311–315. [Google Scholar] [CrossRef]
- Liddelow, S.A. Fluids and barriers of the CNS: A historical viewpoint. Fluids Barriers CNS 2011, 8, 2. [Google Scholar] [CrossRef] [Green Version]
- Tumani, H.; Huss, A.; Bachhuber, F. The cerebrospinal fluid and barriers—Anatomic and physiologic considerations. Handb. Clin. Neurol. 2017, 146, 21–32. [Google Scholar] [CrossRef] [PubMed]
- Andersson, M.; Alvarez-Cermeno, J.; Bernardi, G.; Cogato, I.; Fredman, P.; Frederiksen, J.; Fredrikson, S.; Gallo, P.; Grimaldi, L.M.; Gronning, M.; et al. Cerebrospinal fluid in the diagnosis of multiple sclerosis: A consensus report. J. Neurol. Neurosurg. Psychiatry 1994, 57, 897–902. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deisenhammer, F.; Zetterberg, H.; Fitzner, B.; Zettl, U.K. The Cerebrospinal Fluid in Multiple Sclerosis. Front. Immunol. 2019, 10, 726. [Google Scholar] [CrossRef] [PubMed]
- McCudden, C.R.; Brooks, J.; Figurado, P.; Bourque, P.R. Cerebrospinal Fluid Total Protein Reference Intervals Derived from 20 Years of Patient Data. Clin. Chem. 2017, 63, 1856–1865. [Google Scholar] [CrossRef]
- Castellazzi, M.; Pizzicotti, S.; Lombardo, I.; Alfiero, S.; Morotti, A.; Pellegatti, P.; Negri, G.; Natali, L.; Ferri, C.; Fainardi, E.; et al. Sexual dimorphism in the cerebrospinal fluid total protein content. Clin. Chem. Lab. Med. 2020, 58, 1885–1890. [Google Scholar] [CrossRef]
- Castellazzi, M.; Morotti, A.; Tamborino, C.; Alessi, F.; Pilotto, S.; Baldi, E.; Caniatti, L.M.; Trentini, A.; Casetta, I.; Granieri, E.; et al. Increased age and male sex are independently associated with higher frequency of blood-cerebrospinal fluid barrier dysfunction using the albumin quotient. Fluids Barriers CNS 2020, 17, 14. [Google Scholar] [CrossRef]
- Castellazzi, M.; Ferri, C.; Alfiero, S.; Lombardo, I.; Laudisi, M.; Tecilla, G.; Boni, M.; Pizzicotti, S.; Fainardi, E.; Bellini, T.; et al. Sex-Related Differences in Cerebrospinal Fluid Plasma-Derived Proteins of Neurological Patients. Diagnostics 2021, 11, 884. [Google Scholar] [CrossRef]
- Meixensberger, S.; Bechter, K.; Dersch, R.; Feige, B.; Maier, S.; Schiele, M.A.; Runge, K.; Denzel, D.; Nickel, K.; Spieler, D.; et al. Sex difference in cerebrospinal fluid/blood albumin quotients in patients with schizophreniform and affective psychosis. Fluids Barriers CNS 2020, 17, 67. [Google Scholar] [CrossRef]
- Parrado-Fernandez, C.; Blennow, K.; Hansson, M.; Leoni, V.; Cedazo-Minguez, A.; Bjorkhem, I. Evidence for sex difference in the CSF/plasma albumin ratio in ~20,000 patients and 335 healthy volunteers. J. Cell. Mol. Med. 2018, 22, 5151–5154. [Google Scholar] [CrossRef] [Green Version]
- Gastaldi, M.; Zardini, E.; Franciotta, D. An update on the use of cerebrospinal fluid analysis as a diagnostic tool in multiple sclerosis. Expert. Rev. Mol. Diagn. 2017, 17, 31–46. [Google Scholar] [CrossRef]
- Tumani, H.; Petereit, H.F.; Gerritzen, A.; Gross, C.C.; Huss, A.; Isenmann, S.; Jesse, S.; Khalil, M.; Lewczuk, P.; Lewerenz, J.; et al. S1 guidelines “lumbar puncture and cerebrospinal fluid analysis” (abridged and translated version). Neurol. Res. Pract. 2020, 2, 8. [Google Scholar] [CrossRef] [PubMed]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tibbling, G.; Link, H.; Ohman, S. Principles of albumin and IgG analyses in neurological disorders. I. Establishment of reference values. Scand. J. Clin. Lab. Investig. 1977, 37, 385–390. [Google Scholar] [CrossRef]
- Reiber, H. External quality assessment in clinical neurochemistry: Survey of analysis for cerebrospinal fluid (CSF) proteins based on CSF/serum quotients. Clin. Chem. 1995, 41, 256–263. [Google Scholar] [CrossRef] [PubMed]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [Green Version]
- Thompson, E.J.; Keir, G. Laboratory investigation of cerebrospinal fluid proteins. Ann. Clin. Biochem. 1990, 27, 425–435. [Google Scholar] [CrossRef] [Green Version]
- Uher, T.; Horakova, D.; Tyblova, M.; Zeman, D.; Krasulova, E.; Mrazova, K.; Seidl, Z.; Vaneckova, M.; Krasensky, J.; Weinstock-Guttman, B.; et al. Increased albumin quotient (QAlb) in patients after first clinical event suggestive of multiple sclerosis is associated with development of brain atrophy and greater disability 48 months later. Mult. Scler. 2016, 22, 770–781. [Google Scholar] [CrossRef]
- Yin, H.; Wan, Q.; Tian, Y.; Zhao, B.; Deng, Y. Female Hormone 17beta-Estradiol Downregulated MMP-2 Expression and Upregulated A1PI Expression in Human Corneal Stromal Cells. Cell. Biochem. Biophys. 2018, 76, 265–271. [Google Scholar] [CrossRef]
- Na, W.; Lee, J.Y.; Kim, W.S.; Yune, T.Y.; Ju, B.G. 17beta-Estradiol Ameliorates Tight Junction Disruption via Repression of MMP Transcription. Mol. Endocrinol. 2015, 29, 1347–1361. [Google Scholar] [CrossRef] [Green Version]
- Castellazzi, M.; Ligi, D.; Contaldi, E.; Quartana, D.; Fonderico, M.; Borgatti, L.; Bellini, T.; Trentini, A.; Granieri, E.; Fainardi, E.; et al. Multiplex Matrix Metalloproteinases Analysis in the Cerebrospinal Fluid Reveals Potential Specific Patterns in Multiple Sclerosis Patients. Front. Neurol. 2018, 9, 1080. [Google Scholar] [CrossRef]
- Weisner, B.; Bernhardt, W. Protein fractions of lumbar, cisternal, and ventricular cerebrospinal fluid. Separate areas of reference. J. Neurol. Sci. 1978, 37, 205–214. [Google Scholar] [CrossRef]
- Aasebø, E.; Opsahl, J.A.; Bjørlykke, Y.; Myhr, K.M.; Kroksveen, A.C.; Berven, F.S. Effects of blood contamination and the rostro-caudal gradient on the human cerebrospinal fluid proteome. PLoS ONE 2014, 9, e90429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pannewitz-Makaj, K.; Wurster, U.; Jendretzky, K.F.; Gingele, S.; Sühs, K.W.; Stangel, M.; Skripuletz, T.; Schwenkenbecher, P. Evidence of Oligoclonal Bands Does Not Exclude Non-Inflammatory Neurological Diseases. Diagnostics 2020, 11, 37. [Google Scholar] [CrossRef] [PubMed]
- Manouchehrinia, A.; Westerlind, H.; Kingwell, E.; Zhu, F.; Carruthers, R.; Ramanujam, R.; Ban, M.; Glaser, A.; Sawcer, S.; Tremlett, H.; et al. Age Related Multiple Sclerosis Severity Score: Disability ranked by age. Mult. Scler. 2017, 23, 1938–1946. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andreadou, E.; Chatzipanagiotou, S.; Constantinides, V.C.; Rombos, A.; Stamboulis, E.; Nicolaou, C. Prevalence of cerebrospinal fluid oligoclonal IgG bands in Greek patients with clinically isolated syndrome and multiple sclerosis. Clin. Neurol. Neurosurg. 2013, 115, 2094–2098. [Google Scholar] [CrossRef] [PubMed]
- Mero, I.L.; Gustavsen, M.W.; Sæther, H.S.; Flåm, S.T.; Berg-Hansen, P.; Søndergaard, H.B.; Jensen, P.E.; Berge, T.; Bjølgerud, A.; Muggerud, A.; et al. Oligoclonal band status in Scandinavian multiple sclerosis patients is associated with specific genetic risk alleles. PLoS ONE 2013, 8, e58352. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Males | Females | p | |
|---|---|---|---|
| Cohort 1, MS: Ferrara (Italy): n | 77 | 189 | |
| Age, years: median (IQR) | 37 (29.0–45.0) a | 36 (29.4–44.5) b | 0.9270 |
| Clinical activity: n (%) | 55 (71.4) | 143 (75.7) | |
| Disease duration, months: median (IQR) | 27 (3.5–79.5) c | 12.5 (3.0–59.75) d | 0.1419 |
| EDSS: median (IQR) | 3.0 (1.5–3.5) e | 2.5 (1.5–3.5) f | 0.5651 |
| Cohort 2, MS: San Giovanni Rotondo (Italy): n | 32 | 42 | |
| Age, years: median (IQR) | 39 (26–46) a | 38.5 (28–47) b | 0.6080 |
| Clinical activity: n (%) | 27 (84.4) | 35 (83.3) | >0.9999 |
| Disease duration, months: median (IQR) | 12 (1–46) c | 10 (1–46) d | 0.9719 |
| EDSS: median (IQR) | 2.0 (1.0–3.0) e | 2.0 (1.5–3.0) f | 0.8315 |
| Cohort 3, CIS: Ulm (Germany): n | 32 | 57 | |
| Age, years: median (IQR) | 30 (24–42) | 36 (26–46) | 0.1660 |
| Disease duration, months: median (IQR) | 0 (0–0) | 0 (0–6) | >0.9999 |
| Males | Females | p | |
|---|---|---|---|
| MS patients (Cohorts 1 and 2): n | 109 | 231 | |
| QAlb (×1000) value: median (IQR) | 5.6 (4.37–8.39) a | 4.34 (3.38–5.49) b | <0.0001 |
| QAlb (×1000) max value: | 16.3 | 16.5 | |
| Altered QAlb value: n (%) | 36 (33.0) | 24 (10.4) | <0.0001 |
| Elevated IgG index: n (%) | 58 (53.2) | 140 (60.6) | 0.2387 |
| IgG intrathecal fraction > 0: n (%) | 53 (48.6) | 133 (57.6) | 0.1304 |
| CSF-restricted IgG OCB: n (%) | 94 (86.2) c | 191 (82.7) d | 0.4351 |
| CIS patients (Cohort 3): n | 32 | 57 | |
| QAlb (×1000) value: median (IQR) | 5.5 (4.7–6.8) a | 5.2 (4.05–6.7) b | 0.1810 |
| QAlb (×1000) max value: | 12.7 | 11.1 | |
| Altered QAlb value: n (%) | 9 (28.1) | 9 (15.8) | 0.1800 |
| Elevated IgG index: n (%) | 13 (40.6) | 26 (45.6) | 0.6642 |
| IgG intrathecal fraction > 0: n (%) | 11 (34.4) | 25 (43.9) | 0.5002 |
| CSF-restricted IgG OCB: n (%) | 30 (93.8) c | 51 (89.5) d | 0.7059 |
| Age vs. Disease Duration | Age vs. EDSS | EDSS vs. Disease Duration | |
|---|---|---|---|
| MS patients (n = 340) | |||
| Spearman r | 0.3502 | 0.2986 | 0.2837 |
| 95% CI | 0.2502–0.4429 | 0.1955–0.3952 | 0.1797–0.3815 |
| p value | <0.0001 | <0.0001 | <0.0001 |
| MS males (n = 109) | |||
| Spearman r | 0.4219 | 0.1997 | 0.05800 |
| 95% CI | 0.2487–0.5690 | 0.006416–0.3786 | −0.1371–0.2487 |
| p-value | <0.0001 | 0.0374 | 0.5491 |
| MS females (n = 231) | |||
| Spearman r | 0.3137 | 0.3395 | 0.3798 |
| 95% CI | 0.1884–0.4289 | 0.2164–0.4520 | 0.2598–0.4882 |
| p-value | <0.0001 | <0.0001 | <0.0001 |
| Age vs. QAlb (×1000) | Age vs. IgG Index | Age vs. IgG IF (%) | |
|---|---|---|---|
| MS patients (n = 340) | |||
| Spearman r | 0.1807 | −0.01312 | −0.01483 |
| 95% CI | 0.07270–0.2846 | −0.1224–0.09650 | −0.1241–0.09481 |
| p-value | 0.0008 | 0.8095 | 0.7853 |
| MS males (n = 109) | |||
| Spearman r | 0.2711 a | 0.02820 | −0.001166 |
| 95% CI | 0.08190–0.4415 | −0.1662–0.2205 | −0.1946–0.1924 |
| p-value | 0.0043 | 0.7710 | 0.9904 |
| MS females (n = 231) | |||
| Spearman r | 0.1540 a | −0.03586 | −0.003181 |
| 95% CI | 0.02161–0.2811 | −0.1679–0.09745 | −0.1360–0.1297 |
| p-value | 0.0192 | 0.5877 | 0.9616 |
| CIS patients (n = 89) | |||
| Spearman r | 0.2368 | 0.1775 | 0.05126 |
| 95% CI | 0.02380–0.4293 | −0.03816–0.3774 | −0.1648–0.2626 |
| p-value | 0.0255 | 0.0961 | 0.6333 |
| CIS males (n = 32) | |||
| Spearman r | 0.4561 | 0.3567 | 0.1519 |
| 95% CI | 0.1171–0.6999 | −0.001664–0.6338 | −0.2180–0.4837 |
| p-value | 0.0087 | 0.0451 | 0.4065 |
| CIS females (n = 57) | |||
| Spearman r | 0.1834 | 0.1027 | −0.01537 |
| 95% CI | −0.08886–0.4302 | −0.1698–0.3607 | −0.2821–0.2536 |
| p-value | 0.1720 | 0.4470 | 0.9096 |
| IgG Index | Reiber’s Formula | |
|---|---|---|
| Values (95% CI) | Values (95% CI) | |
| MS patients (n = 340) | ||
| Kappa | 0.371 (0.284–0.458) | 0.331 (0.249–0.414) |
| Sensitivity | 0.6807 (0.6245–0.7321) | 0.6386 (0.5813–0.6922) |
| Specificity | 0.9273 (0.8274–0.9714) | 0.9273 (0.8274–0.9714) |
| Positive Predictive Value | 0.9798 (0.9492–0.9921) | 0.9785 (0.9460–0.9916) |
| Negative Predictive Value | 0.3592 (0.2849–0.4408) | 0.3312 (0.2617–0.4088) |
| MS males (n = 109) | ||
| Kappa | 0.307 (0.174–0.441) | 0.234 (0.110–0.359) |
| Sensitivity | 0.617 (0.5160–0.7089) | 0.5532 (0.4526–0.6496) |
| Specificity | 1.000 (0.7961–1.000) | 0.9333 (0.7018–0.9966) |
| Positive Predictive Value | 1.000 (0.9379–1.000) | 0.9811 (0.9006–0.9990) |
| Negative Predictive Value | 0.2941 (0.1871–0.4300) | 0.2500 (0.1552–0.3769) |
| MS females (n = 231) | ||
| Kappa | 0.407 (0.296–0.518) | 0.385 (0.279–0.518) |
| Sensitivity | 0.712 (0.6441–0.7716) | 0.6806 (0.6115–0.7426) |
| Specificity | 0.900 (0.7695–0.9604) | 0.925 (0.8014–0.9742) |
| Positive Predictive Value | 0.9714 (0.9288–0.9888) | 0.9774 (0.9358–0.9939) |
| Negative Predictive Value | 0.3956 (0.3013–0.4983) | 0.3776 (0.2879–0.4764) |
| CIS patients (n = 89) | ||
| Kappa | 0.143 (0.046–0.240) | 0.126 (0.039–0.213) |
| Sensitivity | 0.4815 (0.3760–0.5886) | 0.4444 (0.3412–0.5527) |
| Specificity | 1.000 (0.6756–1.000) | 1.000 (0.6756–1.000) |
| Positive Predictive Value | 1.000 (0.9103–1.000) | 1.000 (0.9036–1.000) |
| Negative Predictive Value | 0.16 (0.08337–0.2851) | 0.1509 (0.07852–0.2705) |
| CIS males (n = 32) | ||
| Kappa | 0.087 (−0.034–0.209) | 0.067 (−0.029–0.164) |
| Sensitivity | 0.4333 (0.2738–0.6080) | 0.3667 (0.2187–0.5449) |
| Specificity | 1.000 (0.1777–1.000) | 1.000 (0.1777–1.000) |
| Positive Predictive Value | 1.000 (0.7719–1.000) | 1.000 (0.7412–1.000) |
| Negative Predictive Value | 0.1053 (0.01870–0.3139) | 0.09524 (0.01692–0.2891) |
| CIS females (n = 57) | ||
| Kappa | 0.180 (0.042–0.317) | 0.168 (0.037–0.299) |
| Sensitivity | 0.5098 (0.3768–0.6414) | 0.4902 (0.3586–0.6232) |
| Specificity | 1.000 (0.6097–1.000) | 1.000 (0.6097–1.000) |
| Positive Predictive Value | 1.000 (0.8713–1.000) | 1.000 (0.8668–1.000) |
| Negative Predictive Value | 0.1935 (0.09187–0.3628) | 0.1875 (0.08890–0.3531) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castellazzi, M.; Ferri, C.; Tecilla, G.; Huss, A.; Crociani, P.; Desina, G.; Barbella, G.; Piola, A.; Permunian, S.; Senel, M.; et al. The Sexual Dimorphism in Cerebrospinal Fluid Protein Content Does Not Affect Intrathecal IgG Synthesis in Multiple Sclerosis. J. Pers. Med. 2022, 12, 977. https://doi.org/10.3390/jpm12060977
Castellazzi M, Ferri C, Tecilla G, Huss A, Crociani P, Desina G, Barbella G, Piola A, Permunian S, Senel M, et al. The Sexual Dimorphism in Cerebrospinal Fluid Protein Content Does Not Affect Intrathecal IgG Synthesis in Multiple Sclerosis. Journal of Personalized Medicine. 2022; 12(6):977. https://doi.org/10.3390/jpm12060977
Chicago/Turabian StyleCastellazzi, Massimiliano, Caterina Ferri, Ginevra Tecilla, André Huss, Paola Crociani, Gaetano Desina, Gianvito Barbella, Alice Piola, Samantha Permunian, Makbule Senel, and et al. 2022. "The Sexual Dimorphism in Cerebrospinal Fluid Protein Content Does Not Affect Intrathecal IgG Synthesis in Multiple Sclerosis" Journal of Personalized Medicine 12, no. 6: 977. https://doi.org/10.3390/jpm12060977