
Robustness Evaluation of a Deep Learning Model on Sagittal and Axial Breast DCE-MRIs to Predict Pathological Complete Response to Neoadjuvant Chemotherapy

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
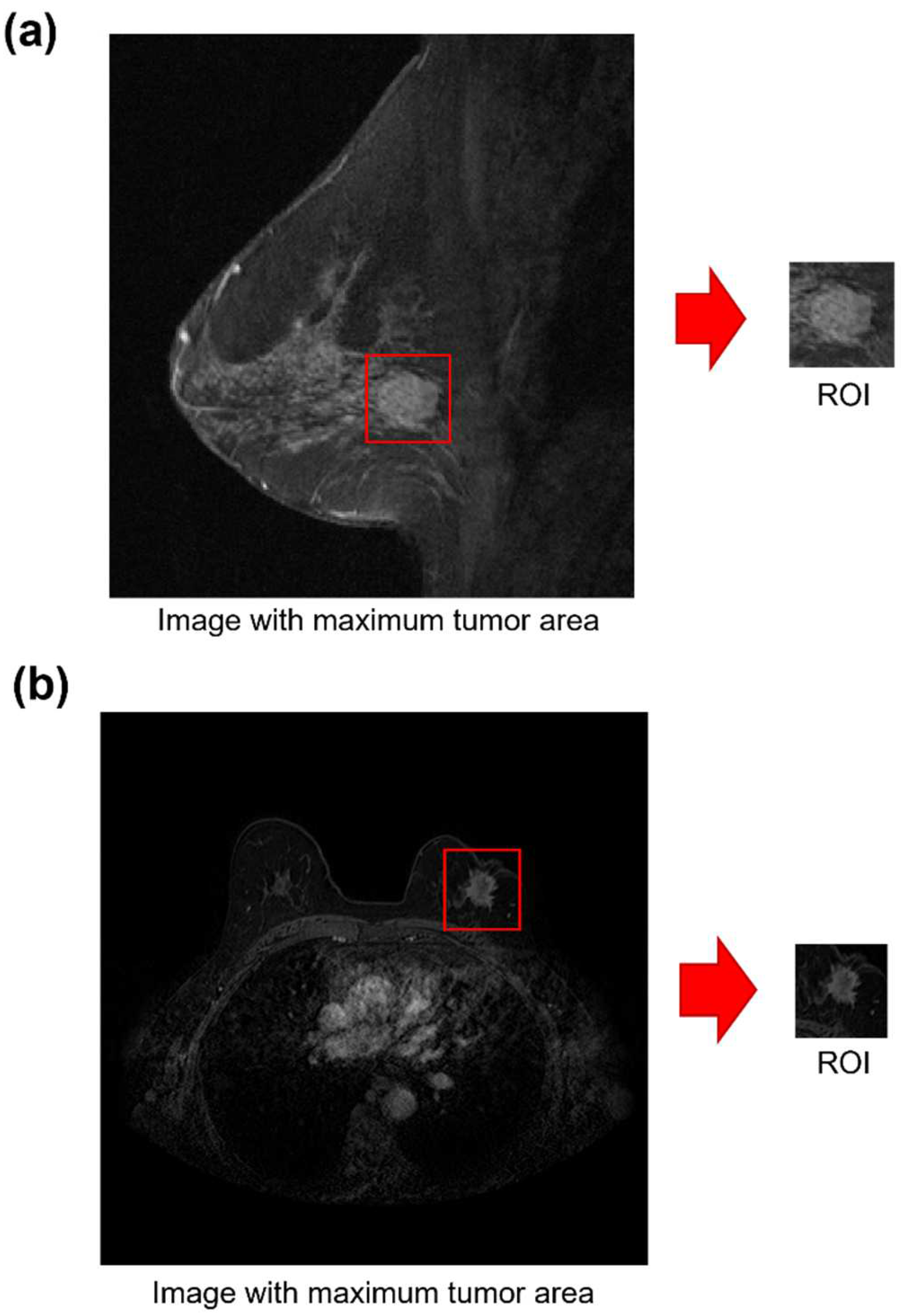
2.2. Data Pre-Processing
2.3. Statistical Analysis
2.4. An AI Framework to Predict pCR “Early On” from Baseline MRI Examinations
3. Results
3.1. Statistical Analysis Results
3.2. Evaluation Perfomance Achieved by the AI Model on Sagittal and Axial Baseline MRIs
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix A.1. Technical Details about the Proposed AI Framework
Appendix A.1.1. Feature Extraction
Appendix A.1.2. Stratified Feature Selection
Appendix A.1.3. Classification
Appendix A.2. Results on Training Sets
References
- Mieog, J.S.D.; Van Der Hage, J.A.; Van De Velde, C.J.H. Neoadjuvant chemotherapy for operable breast cancer. Br. J. Surg. 2007, 94, 1189–1200. [Google Scholar] [CrossRef] [PubMed]
- Cain, H.; Macpherson, I.R.; Beresford, M.; Pinder, S.E.; Pong, J.; Dixon, J.M. Neoadjuvant Therapy in Early Breast Cancer: Treatment Considerations and Common Debates in Practice. Clin. Oncol. 2017, 29, 642–652. [Google Scholar] [CrossRef] [PubMed]
- Minarikova, L.; Bogner, W.; Pinker, K.; Valkovič, L.; Zaric, O.; Bago-Horvath, Z.; Bartsch, R.; Helbich, T.H.; Trattnig, S.; Gruber, S. Investigating the prediction value of multiparametric magnetic resonance imaging at 3 T in response to neoadjuvant chemotherapy in breast cancer. Eur. Radiol. 2017, 27, 1901–1911. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, A.A.T.; Arasu, V.A.; Strand, F.; Li, W.; Onishi, N.; Gibbs, J.; Jones, E.F.; Joe, B.N.; Esserman, L.J.; Newitt, D.C.; et al. Comparison of segmentation methods in assessing background parenchymal enhancement as a biomarker for response to neoadjuvant therapy. Tomography 2020, 6, 101–110. [Google Scholar] [CrossRef]
- Goldhirsch, A.; Winer, E.P.; Coates, A.S.; Gelber, R.D.; Piccart-Gebhart, M.; Thürlimann, B.; Senn, H.-J. Personalizing the treatment of women with early breast cancer: Highlights of the st gallen international expert consensus on the primary therapy of early breast Cancer 2013. Ann. Oncol. 2013, 24, 2206–2223. [Google Scholar] [CrossRef]
- Hylton, N.M.; Blume, J.D.; Bernreuter, W.K.; Pisano, E.D.; Rosen, M.A.; Morris, E.A.; Weatherall, P.T.; Lehman, C.D.; Newstead, G.M.; Polin, S.; et al. Locally advanced breast cancer: MR imaging for prediction of response to neoadjuvant chemotherapy—Results from ACRIN 6657/I-SPY TRIAL. Radiology 2012, 263, 663–672. [Google Scholar] [CrossRef]
- Choi, W.J.; Kim, W.K.; Shin, H.J.; Cha, J.H.; Chae, E.Y.; Kim, H.H. Evaluation of the Tumor Response After Neoadjuvant Chemotherapy in Breast Cancer Patients: Correlation Between Dynamic Contrast-enhanced Magnetic Resonance Imaging and Pathologic Tumor Cellularity. Clin. Breast Cancer 2018, 18, e115–e121. [Google Scholar] [CrossRef]
- Li, X.; Abramson, R.G.; Arlinghaus, L.R.; Kang, H.; Chakravarthy, A.B.; Abramson, V.G.; Farley, J.; Mayer, I.A.; Kelley, M.C.; Meszoely, M.C.; et al. Multiparametric magnetic resonance imaging for predicting pathological response after the first cycle of neoadjuvant chemotherapy in breast cancer. Investig. Radiol. 2015, 50, 195–204. [Google Scholar] [CrossRef]
- Smith, I.C.; Heys, S.D.; Hutcheon, A.W.; Miller, I.D.; Payne, S.; Gilbert, F.J.; Ah-See, A.K.; Eremin, O.; Walker, L.G.; Sarkar, T.K.; et al. Neoadjuvant chemotherapy in breast cancer: Significantly enhanced response with docetaxel. J. Clin. Oncol. 2002, 20, 1456–1466. [Google Scholar] [CrossRef]
- Gonzalez-Angulo, A.M.; Morales-Vasquez, F.; Hortobagyi, G.N. Overview of resistance to systemic therapy in patients with breast cancer. In Breast Cancer Chemosensitivity; Advances in Experimental Medicine and Biology; Springer: Berlin/Heidelberg, Germany, 2007; Volume 608, pp. 1–22. [Google Scholar] [CrossRef]
- Wei, D.; Jahani, N.; Cohen, E.; Weinstein, S.; Hsieh, M.-K.; Pantalone, L.; Kontos, D. Fully automatic quantification of fibroglandular tissue and background parenchymal enhancement with accurate implementation for axial and sagittal breast MRI protocols. Med. Phys. 2021, 48, 238–252. [Google Scholar] [CrossRef]
- Fausto, A.; Fanizzi, A.; Volterrani, L.; Mazzei, F.G.; Calabrese, C.; Casella, D.; Marcasciano, M.; Massafra, R.; La Forgia, D.; Mazzei, M.A. Feasibility, image quality and clinical evaluation of contrast-enhanced breast mri performed in a supine position compared to the standard prone position. Cancers 2020, 12, 2364. [Google Scholar] [CrossRef] [PubMed]
- Margolies, L.R.; Salvatore, M.; Tam, K.; Yip, R.; Bertolini, A.; Henschke, C.I.; Yankelevitz, D.F. Breast mass assessment on chest CT: Axial, sagittal, coronal or maximal intensity projection? Clin. Imaging 2020, 63, 60–64. [Google Scholar] [CrossRef] [PubMed]
- Mann, R.M.; Cho, N.; Moy, L. Breast MRI: State of the art. Radiology 2019, 292, 520–536. [Google Scholar] [CrossRef] [PubMed]
- Fowler, A.M.; Mankoff, D.A.; Joe, B.N. Imaging neoadjuvant therapy Response in Breast Cancer. Online SA-CME STATE OF THE ART: Imaging Neoadjuvant Therapy Response in Breast Cancer Fowler et al. Radiology 2017, 285, 358–375. [Google Scholar] [CrossRef]
- Scheel, J.R.; Kim, E.; Partridge, S.C.; Lehman, C.D.; Rosen, M.A.; Bernreuter, W.; Pisano, E.D.; Marques, H.; Morris, E.A.; Weatherall, P.T.; et al. MRI, clinical examination, and mammography for preoperative assessment of residual disease and pathologic complete response after neoadjuvant chemotherapy for breast cancer: ACRIN 6657 trial. Am. J. Roentgenol. 2018, 210, 1376–1385. [Google Scholar] [CrossRef]
- Park, J.S.; Moon, W.K.; Lyou, C.Y.; Cho, N.; Kang, K.W.; Chung, J.-K. The assessment of breast cancer response to neoadjuvant chemotherapy: Comparison of magnetic resonance imaging and 18F-fluorodeoxyglucose positron emission tomography. Acta Radiol. 2011, 52, 21–28. [Google Scholar] [CrossRef]
- La Forgia, D.; Vestito, A.; Lasciarrea, M.; Comes, M.C.; Diotaiuti, S.; Giotta, F.; Latorre, A.; Lorusso, V.; Massafra, R.; Palmiotti, G.; et al. Response Predictivity to Neoadjuvant Therapies in Breast Cancer: A Qualitative Analysis of Background Parenchymal Enhancement in DCE-MRI. J. Pers. Med. 2021, 11, 256. [Google Scholar] [CrossRef]
- Eun, N.L.; Kang, D.; Son, E.J.; Park, J.S.; Youk, J.H.; Kim, J.A.; Gweon, H.M. Texture analysis with 3.0-T MRI for association of response to neoadjuvant chemotherapy in breast cancer. Radiology 2020, 294, 31–41. [Google Scholar] [CrossRef]
- Braman, N.M.; Etesami, M.; Prasanna, P.; Dubchuk, C.; Gilmore, H.; Tiwari, P.; Plecha, D.; Madabhushi, A. Intratumoral and peritumoral radiomics for the pretreatment prediction of pathological complete response to neoadjuvant chemotherapy based on breast DCE-MRI. Breast Cancer Res. 2017, 19, 57. [Google Scholar] [CrossRef]
- Tahmassebi, A.; Wengert, G.J.; Helbich, T.H.; Bago-Horvath, Z.; Alaei, S.; Bartsch, R.; Dubsky, P.; Baltzer, P.; Clauser, P.; Kapetas, P.; et al. Impact of machine learning with multiparametric magnetic resonance imaging of the breast for early prediction of response to neoadjuvant chemotherapy and survival outcomes in breast cancer patients. Investig. Radiol. 2019, 54, 110–117. [Google Scholar] [CrossRef]
- Drisis, S.; Metens, T.; Ignatiadis, M.; Stathopoulos, K.; Chao, S.L.; Lemort, M. Quantitative DCE-MRI for prediction of pathological complete response following neoadjuvant treatment for locally advanced breast cancer: The impact of breast cancer subtypes on the diagnostic accuracy. Eur. Radiol. 2016, 26, 1474–1484. [Google Scholar] [CrossRef]
- Mencattini, A.; Di Giuseppe, D.; Comes, M.C.; Casti, P.; Corsi, F.; Bertani, F.R.; Ghibelli, L.; Businaro, L.; Di Natale, C.; Parrini, M.C.; et al. Discovering the hidden messages within cell trajectories using a deep learning approach for in vitro evaluation of cancer drug treatments. Sci. Rep. 2020, 10, 7653. [Google Scholar] [CrossRef] [PubMed]
- Huynh, B.Q.; Antropova, N.; Giger, M.L. Comparison of breast DCE-MRI contrast time points for predicting response to neoadjuvant chemotherapy using deep convolutional neural network features with transfer learning. In Medical Imaging 2017: Computer-Aided Diagnosis, Proceedings of the SPIE Medical Imaging, Orlando, FL, USA, 11–16 February 2017; SPIE: Bellingham, WA, USA, 2017; Volume 10134, p. 101340U. [Google Scholar] [CrossRef]
- Ha, R.; Chin, C.; Karcich, J.; Liu, M.Z.; Chang, P.; Mutasa, S.; Van Sant, E.P.; Wynn, R.T.; Connolly, E.; Jambawalikar, S. Prior to Initiation of Chemotherapy, Can We Predict Breast Tumor Response? Deep Learning Convolutional Neural Networks Approach Using a Breast MRI Tumor Dataset. J. Digit. Imaging 2019, 32, 693–701. [Google Scholar] [CrossRef]
- Ravichandran, K.; Braman, N.; Janowczyk, A.; Madabhushi, A. A deep learning classifier for prediction of pathological complete response to neoadjuvant chemotherapy from baseline breast DCE-MRI. In Medical Imaging 2018: Computer-Aided Diagnosis, Proceedings of the SPIE Medical Imaging, Houston, TX, USA, 10–15 February 2018; SPIE: Bellingham, WA, USA, 2018; Volume 10575. [Google Scholar] [CrossRef]
- El Adoui, M.; Drisis, S.; Benjelloun, M. Multi-input deep learning architecture for predicting breast tumor response to chemotherapy using quantitative MR images. Int. J. Comput. Assist. Radiol. Surg. 2020, 15, 1491–1500. [Google Scholar] [CrossRef]
- Comes, M.C.; Fanizzi, A.; Bove, S.; Didonna, V.; Diotiaiuti, S.; La Forgia, D.; Latorre, A.; Martinelli, E.; Mencattini, A.; Nardone, A.; et al. Early prediction of neoadjuvant chemotherapy response by exploiting a transfer learning approach on breast DCE-MRIs. Sci. Rep. 2021, 11, 14123. [Google Scholar] [CrossRef]
- Newitt, D.; Hylton, N. Multi-center breast DCE-MRI data and segmentations from patients in the I-SPY 1/ACRIN 6657 trials. Cancer Imaging Arch. 2016, 10, 7. [Google Scholar] [CrossRef]
- Hylton, N.M.; Gatsonis, C.A.; Rosen, M.A.; Lehman, C.D.; Newitt, D.C.; Partridge, S.C.; Bernreuter, W.K.; Pisano, E.D.; Morris, E.A.; Weatherall, P.T.; et al. Neoadjuvant chemotherapy for breast cancer: Functional tumor volume by MR imaging predicts recurrencefree survival-results from the ACRIN 6657/CALGB 150007 I-SPY 1 TRIAL. Radiology 2016, 279, 44–55. [Google Scholar] [CrossRef] [PubMed]
- Clark, K.; Vendt, B.; Smith, K.; Freymann, J.; Kirby, J.; Koppel, P.; Moore, S.; Phillips, S.; Maffitt, D.; Pringle, D.; et al. The cancer imaging archive (TCIA): Maintaining and operating a public information repository. J. Digit. Imaging 2013, 26, 1045–1057. [Google Scholar] [CrossRef] [PubMed]
- Mann, H.B.; Whitney, D.R. On a Test of Whether one of Two Random Variables is Stochastically Larger Larger than the other. Ann. Math. Stat. 1947, 18, 50–60. [Google Scholar] [CrossRef]
- Lyerly, S.B. The average spearman rank correlation coefficient. Psychometrika 1952, 17, 421–428. [Google Scholar] [CrossRef]
- Russakovsky, O.; Deng, J.; Su, H.; Satheesh, S.; Ma, S.; Huang, Z.; Karpathy, A.; Khosla, A.; Bernstein, M.; Berg, A.C.; et al. ImageNet Large Scale Visual Recognition Challenge. Int. J. Comput. Vis. 2015, 115, 211–252. [Google Scholar] [CrossRef]
- Amoroso, N.; Errico, R.; Bruno, S.; Chincarini, A.; Garuccio, E.; Sensi, F.; Tangaro, S.; Tateo, A.; Bellotti, R. Hippocampal unified multi-atlas network (HUMAN): Protocol and scale validation of a novel segmentation tool. Phys. Med. Biol. 2015, 60, 8851–8867. [Google Scholar] [CrossRef] [PubMed]
- Esserman, L.J.; Berry, D.A.; DeMichele, A.; Carey, L.; Davis, S.E.; Buxton, M.; Hudis, C.; Gray, J.W.; Perou, C.; Yau, C.; et al. Pathologic complete response predicts recurrence-free survival more effectively by cancer subset: Results from the I-SPY 1 TRIAL—CALGB 150007/150012, ACRIN 6657. J. Clin. Oncol. 2012, 30, 3242–3249. [Google Scholar] [CrossRef] [PubMed]
- Schirosi, L.; Strippoli, S.; Gaudio, F.; Graziano, G.; Popescu, O.; Guida, M.; Simone, G.; Mangia, A. Is immunohistochemistry of BRAF V600E useful as a screening tool and during progression disease of melanoma patients? BMC Cancer 2016, 16, 905. [Google Scholar] [CrossRef]
- Esteva, A.; Robicquet, A.; Ramsundar, B.; Kuleshov, V.; DePristo, M.; Chou, K.; Cui, C.; Corrado, G.; Thrun, S.; Dean, J.; et al. A guide to deep learning in healthcare. Nat. Med. 2019, 25, 24–29. [Google Scholar] [CrossRef]
- Comes, M.C.; Filippi, J.; Mencattini, A.; Casti, P.; Cerrato, G.; Sauvat, A.; Vacchelli, E.; De Ninno, A.; Di Giuseppe, D.; D’Orazio, M.; et al. Multi-scale generative adversarial network for improved evaluation of cell–cell interactions observed in organ-on-chip experiments. Neural Comput. Appl. 2021, 33, 3671–3689. [Google Scholar] [CrossRef]
- Liu, M.Z.; Mutasa, S.; Chang, P.; Siddiqueb, M.; Jambawalikara, S.; Ha, R. A novel CNN algorithm for pathological complete response prediction using an I-SPY TRIAL breast MRI database. Magn. Reson. Imaging 2020, 73, 148–151. [Google Scholar] [CrossRef]
- Comes, M.C.; La Forgia, D.; Didonna, V.; Fanizzi, A.; Giotta, F.; Latorre, A.; Martinelli, E.; Mencattini, A.; Paradiso, A.V.; Tamborra, P.; et al. Early Prediction of Breast Cancer Recurrence for Patients Treated with Neoadjuvant Chemotherapy: A Transfer Learning Approach on DCE-MRIs. Cancers 2021, 13, 2298. [Google Scholar] [CrossRef]
- Wein, L.; Luen, S.J.; Savas, P.; Salgado, R.; Loi, S. Checkpoint blockade in the treatment of breast cancer: Current status and future directions. Br. J. Cancer 2018, 119, 4–11. [Google Scholar] [CrossRef]
- Bartsch, R.; Bergen, E.; Galid, A. Current concepts and future directions in neoadjuvant chemotherapy of breast cancer. Memo-Mag. Eur. Med. Oncol. 2018, 11, 199–203. [Google Scholar] [CrossRef]
- Granzier, R.W.Y.; van Nijnatten, T.J.A.; Woodruff, H.C.; Smidt, M.L.; Lobbes, M.B.I. Exploring breast cancer response prediction to neoadjuvant systemic therapy using MRI-based radiomics: A systematic review. Eur. J. Radiol. 2019, 121, 108736. [Google Scholar] [CrossRef] [PubMed]
- Peng, S.; Chen, L.; Tao, J.; Liu, J.; Zhu, W.; Liu, H.; Yang, F. Radiomics Analysis of Multi-Phase DCE-MRI in Predicting Tumor Response to Neoadjuvant Therapy in Breast Cancer. Diagnostics 2021, 11, 2086. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Li, P.; Chen, Z.; Zhang, J. A survey on deep learning for multimodal data fusion. Neural Comput. 2020, 32, 829–864. [Google Scholar] [CrossRef] [PubMed]
- Bellotti, R.; Bagnasco, S.; Bottigli, U.; Castellano, M.; Cataldo, R.; Catanzariti, E.; Cerello, P.; Cheran, S.C.; De Carlo, F.; Delogu, P.; et al. The MAGIC-5 project: Medical applications on a grid infrastructure connection. IEEE Nucl. Sci. Symp. Conf. Rec. 2004, 3, 1902–1906. [Google Scholar] [CrossRef]
- Bellotti, R.; De Carlo, F.; Massafra, R.; de Tommaso, M.; Sciruicchio, V. Topographic classification of EEG patterns in Huntington’s disease. Neurol. Clin. Neurophysiol. NCN 2004, 2004, 37. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Public DB | Private DB | ||||
|---|---|---|---|---|---|
| pCR | Non-pCR | pCR | Non-pCR | ||
| Overall | 42 (28%) | 109 (72%) | Overall | 22 (30%) | 52 (70%) |
| Age (years) | Age (years) | ||||
| Mean std | 46.81 8.59 | 49.06 9.15 | Mean std | 51.55 12.72 | 52.02 12.39 |
| T (mm) | T (mm) | ||||
| Mean std | 75.86 36.39 | 65.24 27.66 | Mean std | 35.78 20.95 | 36.05 18.13 |
| Grading | Grading | ||||
| G1 | 0 (0%) | 8 (7.4%) | G1 | 1 (4.5%) | 1 (1.9%) |
| G2 | 12 (28.6%) | 60 (55.0%) | G2 | 1 (4.5%) | 16 (30.8%) |
| G3 | 27 (64.3%) | 41 (37.6%) | G3 | 20 (91.0%) | 30 (57.7%) |
| NA | 3 (7.1%) | 0 (0%) | NA | 0 (0%) | 5 (9.6%) |
| ER | ER | ||||
| Negative | 29 (69.0%) | 38 (34.9%) | Negative | 12 (54.5%) | 13 (25.0%) |
| Positive | 13 (31.0%) | 71 (65.1%) | Positive | 10 (45.5%) | 38 (73.1%) |
| NA | 0 (0%) | 0 (0%) | NA | 0 (0%) | 1 (1.9%) |
| PgR | PgR | ||||
| Negative | 34 (81.0%) | 49 (45.0%) | Negative | 17 (77.3%) | 21 (40.4%) |
| Positive | 8 (19.0%) | 60 (55.0%) | Positive | 5 (22.7%) | 30 (57.7%) |
| NA | 0 (0%) | 0 (0%) | NA | 0 (0%) | 1 (1.9%) |
| Ki67 | Ki67 | ||||
| Negative | 2 (4.8%) | 4 (3.7%) | Negative | 0 (0%) | 0 (0%) |
| Low | 2 (4.8%) | 28 (25.7%) | Low | 0 (0%) | 2 (3.8%) |
| Intermediate | 7 (16.7%) | 32 (29.4%) | Intermediate | 4 (18.2%) | 15 (28.8%) |
| High | 20 (47.6%) | 34 (31.1%) | High | 18 (81.8%) | 34 (65.5%) |
| NA | 11 (26.1%) | 11 (10.1%) | NA | 0 (0%) | 1 (1.9%) |
| HER2 | HER2 | ||||
| Negative | 24 (57.1%) | 86 (78.9%) | Negative | 10 (45.5%) | 35 (67.3%) |
| Positive | 17 (40.5%) | 22 (20.1%) | Positive | 12 (54.5%) | 16 (30.8%) |
| NA | 1 (2.4%) | 1 (1.0%) | NA | 0 (0%) | 1 (1.9%) |
| Variable | Type | DB | p-Value |
|---|---|---|---|
| Age | Continuous | public | 0.1673 |
| private | 0.8805 | ||
| T | Continuous | public | 0.2508 |
| private | 0.8097 | ||
| ER | Categorical (binary) | public | 1.2 × 10−4 |
| private | 0.0164 | ||
| PgR | Categorical (binary) | public | 4.9 × 10−5 |
| private | 0.0046 | ||
| HER2 | Categorical (binary) | public | 0.0087 |
| private | 0.0617 | ||
| Grading | Categorical | public | 1.4 × 10−4 |
| private | 0.0286 | ||
| Ki67 | Categorical | public | 0.0116 |
| private | 0.3494 | ||
| private (over patients AC + tax) | 0.0995 |
| Set | Model | N. Features | AUC | Acc. | Sens. | Spec. |
|---|---|---|---|---|---|---|
| Public DB Independent test: 45 patients (13 pCR) | Clinical | 5 | 58.2% | 64.4% | 53.6% | 68.8% |
| F-merged | 29 | 75.0% | 73.3% | 69.2% | 75.0% | |
| F-merged + clinical | 34 | 80.3% | 84.4% | 69.2% | 90.6% | |
| Private DB Independent test: 22 patients (7 pCR) | Clinical | 5 | 56.0% | 59.1% | 42.9% | 66.7% |
| F-merged | 28 | 72.4% | 77.3% | 57.1% | 86.7% | |
| F-merged + clinical | 33 | 78.0% | 77.3% | 71.4% | 80.0% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Massafra, R.; Comes, M.C.; Bove, S.; Didonna, V.; Gatta, G.; Giotta, F.; Fanizzi, A.; La Forgia, D.; Latorre, A.; Pastena, M.I.; et al. Robustness Evaluation of a Deep Learning Model on Sagittal and Axial Breast DCE-MRIs to Predict Pathological Complete Response to Neoadjuvant Chemotherapy. J. Pers. Med. 2022, 12, 953. https://doi.org/10.3390/jpm12060953
Massafra R, Comes MC, Bove S, Didonna V, Gatta G, Giotta F, Fanizzi A, La Forgia D, Latorre A, Pastena MI, et al. Robustness Evaluation of a Deep Learning Model on Sagittal and Axial Breast DCE-MRIs to Predict Pathological Complete Response to Neoadjuvant Chemotherapy. Journal of Personalized Medicine. 2022; 12(6):953. https://doi.org/10.3390/jpm12060953
Chicago/Turabian StyleMassafra, Raffaella, Maria Colomba Comes, Samantha Bove, Vittorio Didonna, Gianluca Gatta, Francesco Giotta, Annarita Fanizzi, Daniele La Forgia, Agnese Latorre, Maria Irene Pastena, and et al. 2022. "Robustness Evaluation of a Deep Learning Model on Sagittal and Axial Breast DCE-MRIs to Predict Pathological Complete Response to Neoadjuvant Chemotherapy" Journal of Personalized Medicine 12, no. 6: 953. https://doi.org/10.3390/jpm12060953