In Vivo Effects of Balanced Crystalloid or Gelatine Infusions on Functional Parameters of Coagulation and Fibrinolysis: A Prospective Randomized Crossover Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
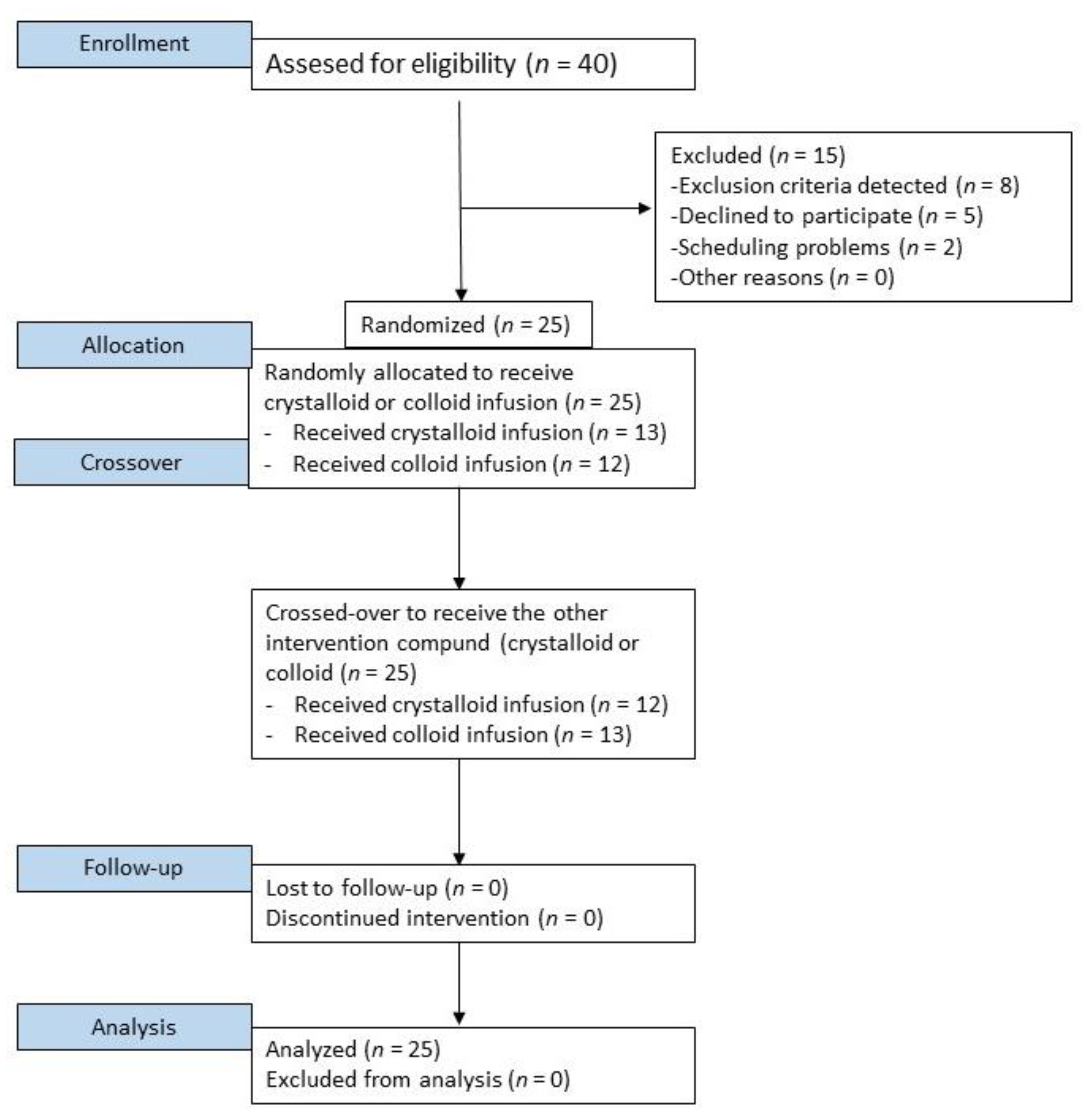
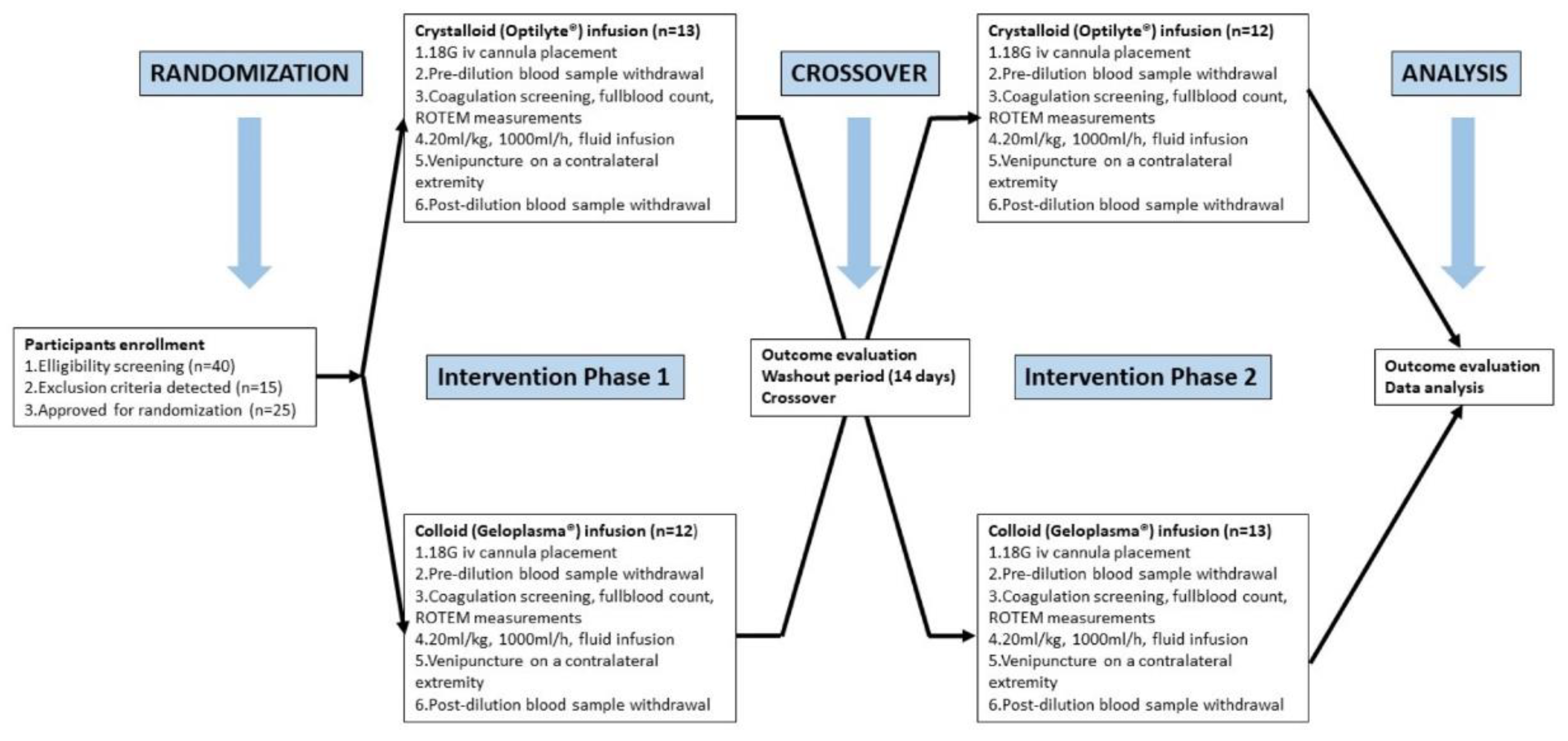
2.2. Study Design and Interventions
2.3. Randomization
2.4. Laboratory Investigations
2.5. Statistical Analysis
3. Results
Effects of Fluids Infusion on Coagulation
4. Discussion
Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kozek-Langenecker, S.A. Fluids and coagulation. Curr. Opin. Crit. Care 2015, 21, 285–291. [Google Scholar] [CrossRef] [PubMed]
- Perez Nieto, O.R.; Wong, A.; Lopez Fermin, J.; Lopez, E.I.Z.; Aguilar, J.A.M.; Tomas, E.D.; Moya, J.D.C.; Gutierrez, G.C.; Ramos, M.G.O.; Montes, X.G.; et al. Aiming for zero fluid accumulation: First, do no harm. Anaesthesiol. Intensive Ther. 2021, 53, 162–178. [Google Scholar] [CrossRef] [PubMed]
- Rehm, M.; Hulde, N.; Kammerer, T.; Meidert, A.S.; Hofmann-Kiefer, K. State of the art in fluid and volume therapy: A user-friendly staged concept. Anaesthesist 2019, 68, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Szczepańska, A.; Pluta, M.; Krzych, Ł. Clinical practice in intraoperative haemodynamic monitoring in Poland: A point prevalence study in 31 Polish hospitals. Anaesthesiol. Intensive Ther. 2020, 52, 97–104. [Google Scholar] [CrossRef]
- Allen, S.J. Fluid therapy and outcome: Balance is best. J. Extra Corpor. Technol. 2014, 46, 28–32. [Google Scholar]
- Harrois, A.; Hamada, S.R.; Duranteau, J. Fluid resuscitation and vasopressors in severe trauma patients. Curr. Opin. Crit. Care 2014, 20, 632–637. [Google Scholar] [CrossRef]
- Trzebicki, J.; Kuźmińska, G.; Nicińska, B.; Flakiewicz, E.; Kulik, A.; Łazowski, T. Application of thromboelastometry in monitoring of dynamics of formation, quality and lysis of the whole blood clot—New possibilities for rapid and reliable diagnosis. Anestezjol. I Ratow. 2013, 7, 53–62. [Google Scholar]
- Reis, S.P.; DeSimone, N.; Barnes, L.; Nordeck, S.M.; Grewal, S.; Cripps, M.; Kalva, S.P. The Utility of Viscoelastic Testing in Patients Undergoing IR Procedures. J. Vasc. Interv. Radiol. 2017, 28, 78–87. [Google Scholar] [CrossRef]
- Myburgh, J.A.; Finfer, S.; Bellomo, R.; Billot, L.; Cass, A.; Gattas, D.; Glass, P.; Lipman, J.; Liu, B.; McArthur, C.; et al. Hydroxyethyl starch or saline for fluid resuscitation in intensive care. N. Engl. J. Med. 2016, 367, 1901–1911. [Google Scholar] [CrossRef] [Green Version]
- Jahangir, A.; Sahra, S.; Niazi, M.R.K.; Siddiqui, F.S.; Anwar, M.Y.; Jahangir, A.; El-Charabaty, E.J. Comparison of normal saline solution with low-chloride solutions in renal transplants: A meta-analysis. Kidney Res. Clin. Pract. 2021, 40, 484–495. [Google Scholar] [CrossRef]
- Antonelli, M.; Sandroni, C. Hydroxyethyl starch for intravenous volume replacement: More harm than benefit. JAMA 2013, 309, 723–724. [Google Scholar] [CrossRef] [PubMed]
- Zarychanski, R.; Abou-Setta, A.M.; Turgeon, A.F.; Houston, B.; McIntyre, L.; Marshall, J.C.; Fergusson, D. Association of hydroxyethyl starch administration with mortality and acute kidney injury in critically ill patients requiring volume resuscitation: A systematic review and meta-analysis. JAMA 2013, 309, 678–688. [Google Scholar] [CrossRef] [PubMed]
- de Lange, N.; Schol, P.; Lancé, M.; Langenveld, J.; Rijnders, R.; Smits, L.; Wassen, M.; Henskens, Y.; Scheepers, H. Restrictive Versus Massive Fluid Resuscitation Strategy (REFILL study), influence on blood loss and hemostatic parameters in obstetric hemorrhage: Study protocol for a randomized controlled trial. Trials 2018, 19, 166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kabon, B.; Sessler, D.I.; Kurz, A. Crystalloid-Colloid Study Team: Effect of Intraoperative Goal-directed Balanced Crystalloid versus Colloid Administration on Major Postoperative Morbidity: A Randomized Trial. Anesthesiology 2019, 130, 728–744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, N.; Statkevicius, S.; Asgeirsson, B.; Schött, U. Effects of different colloid infusions on ROTEM and Multiplate during elective brain tumour neurosurgery. Perioper Med. 2015, 4, 9. [Google Scholar] [CrossRef] [Green Version]
- Pfortmueller, C.A.; Funk, G.C.; Reiterer, C.; Schrott, A.; Zotti, O.; Kabon, B.; Fleischmann, E.; Lindner, G. Normal saline versus a balanced crystalloid for goal-directed perioperative fluid therapy in major abdominal surgery: A double-blind randomised controlled study. Br. J. Anaesth. 2018, 120, 274–283. [Google Scholar] [CrossRef] [Green Version]
- Krzych, Ł.J.; Czempik, P.F. Hooves better than potatoes: In vitro effects of balanced crystalloid and colloids on functional parameters of coagulation and fibrinolysis. Pol. Arch. Intern. Med. 2017, 127, 209–211. [Google Scholar] [CrossRef] [Green Version]
- Q.F.A. Thrombin (Bovine)—0020301800 (2 mL)/0020301700 (5 mL), Printed Insert Sheet: 303725, Revision: R10, Issued: 06/2017, C.O.: 481068; Instrumentation Laboratory Company: Bedford, MA, USA, 2017. [Google Scholar]
- Simurda, T.; Casini, A.; Stasko, J.; Hudecek, J.; Skornova, I.; Vilar, R.; Neerman-Arbez, M.; Kubisz, P. Perioperative management of a severe congenital hypofibrinogenemia with thrombotic phenotype. Thromb. Res. 2020, 188, 1–4. [Google Scholar] [CrossRef]
- Winstedt, D.; Thomas, O.D.; Nilsson, F.; Olanders, K.; Schött, U. Correction of hypothermic and dilutional coagulopathy with concentrates of fibrinogen and factor XIII: An in vitro study with ROTEM. Scand. J. Trauma Resusc. Emerg. Med. 2014, 22, 73. [Google Scholar] [CrossRef] [Green Version]
- Boer, C.; Meesters, M.I.; Milojevic, M.; Benedetto, U.; Bolliger, D.; von Heymann, C.; Jeppsson, A.; Koster, A.; Osnabrugge, R.L.; Ranucci, M.; et al. Task Force on Patient Blood Management for Adult Cardiac Surgery of the European Association for Cardio-Thoracic Surgery (EACTS) and the European Association of Cardiothoracic Anaesthesiology (EACTA). 2017 EACTS/EACTA Guidelines on patient blood management for adult cardiac surgery. J. Cardiothorac. Vasc. Anesth. 2018, 32, 88–120. [Google Scholar] [CrossRef] [Green Version]
- Brunclikova, M.; Simurda, T.; Zolkova, J.; Sterankova, M.; Skornova, I.; Dobrotova, M.; Kolkova, Z.; Loderer, D.; Grendar, M.; Hudecek, J.; et al. Heterogeneity of Genotype-Phenotype in Congenital Hypofibrinogenemia-A Review of Case Reports Associated with Bleeding and Thrombosis. J. Clin. Med. 2022, 11, 1083. [Google Scholar] [CrossRef] [PubMed]
- Neerman-Arbez, M.; Casini, A. Clinical Consequences and Molecular Bases of Low Fibrinogen Levels. Int. J. Mol. Sci. 2018, 19, 192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tynngård, N.; Berlin, G.; Samuelsson, A.; Berg, S. Low dose of hydroxyethyl starch impairs clot formation as assessed by viscoelastic devices. Scand. J. Clin. Lab. Investig. 2014, 74, 344–350. [Google Scholar] [CrossRef] [PubMed]
- Curry, N. Fibrinogen Replacement in Haemostatic Resuscitation: Dose, Laboratory Targets and Product Choice. Transfus. Med. Rev. 2021, 35, 104–107. [Google Scholar] [CrossRef] [PubMed]
- Siegemund, M.; Hollinger, A.; Gebhard, E.C.; Scheuzger, J.D.; Bolliger, D. The value of volume substitution in patients with septic and haemorrhagic shock with respect to the microcirculation. Swiss Med. Wkly. 2019, 149, w20007. [Google Scholar] [CrossRef]
- Marx, G.; Zacharowski, K.; Ichai, C.; Asehnoune, K.; Černý, V.; Dembinski, R.; Roca, R.F.; Fries, D.; Molnar, Z.; Rosenberger, P.; et al. Efficacy and safety of early target-controlled plasma volume replacement with a balanced gelatine solution versus a balanced electrolyte solution in patients with severe sepsis/septic shock: Study protocol, design, and rationale of a prospective, randomized, controlled, double-blind, multicentric, international clinical trial: GENIUS-Gelatine use in ICU and sepsis. Trials 2021, 22, 376. [Google Scholar] [CrossRef]
- Larsen, J.B.; Hvas, A.M. Predictive Value of Whole Blood and Plasma Coagulation Tests for Intra- and Postoperative Bleeding Risk: A Systematic Review. Semin. Thromb. Hemost. 2017, 43, 772–805. [Google Scholar] [CrossRef]
- Abdelfattah, K.; Cripps, M.W. Thromboelastography and Rotational Thromboelastometry use in trauma. Int. J. Surg. 2016, 33, 196–201. [Google Scholar] [CrossRef]
- Volod, O.; Bunch, C.M.; Zackariya, N.; Moore, E.E.; Moore, H.B.; Kwaan, H.C.; Neal, M.D.; Al-Fadhl, M.D.; Patel, S.S.; Wiarda, G.; et al. Viscoelastic Hemostatic Assays: A Primer on Legacy and New Generation Devices. J. Clin. Med. 2022, 11, 860. [Google Scholar] [CrossRef]
- Casutt, M.; Kristoffy, A.; Schuepfer, G.; Spahn, D.R.; Konrad, C. Effects on coagulation of balanced (130/0.42) and non-balanced (130/0.4) hydroxyethyl starch or gelatin compared with balanced Ringer’s solution: An in vitro study using two different viscoelastic coagulation tests ROTEMTM and SONOCLOTTM. Br. J. Anaesth. 2010, 105, 273–281. [Google Scholar] [CrossRef] [Green Version]
- Shin, H.J.; Park, H.Y.; Na, H.S.; Hong, J.P.; Lee, G.W.; Do, S.H. The effects of Plasma-Lyte 148 solution on blood coagulation: An in-vitro, volunteer study using rotational thromboelastometry. Blood Coagul. Fibrinolysis 2018, 29, 446–450. [Google Scholar] [CrossRef] [PubMed]
- Getrajdman, C.; Sison, M.; Lin, H.M.; Katz, D. The impact of crystalloid versus colloid on coagulation as measured by thromboelastometry in term parturients: An in vitro study. J. Matern. Fetal. Neonatal Med. 2021, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Mittermayr, M.; Streif, W.; Haas, T.; Fries, D.; Velik-Salchner, C.; Klingler, A.; Oswald, E.; Bach, C.; Schnapka-Koepf, M.; Innerhofer, P. Hemostatic changes after crystalloid or colloid fluid administration during major orthopedic surgery: The role of fibrinogen administration. Anesth. Analg. 2007, 105, 905–917. [Google Scholar] [CrossRef] [PubMed]
- Innerhofer, P.; Fries, D.; Margreiter, J.; Klingler, A.; Kühbacher, G.; Wachter, B.; Oswald, E.; Salner, E.; Frischhut, B.; Schobersberger, W. The effects of perioperatively administered colloids and crystalloids on primary platelet-mediated hemostasis and clot formation. Anesth. Analg. 2002, 95, 858–865. [Google Scholar] [CrossRef]
- Fries, D.; Streif, W.; Margreiter, J.; Klingler, A.; Kühbacher, G.; Schobersberger, W.; Wirleitner, B.; Innerhofer, P. The effects of perioperatively administered crystalloids and colloids on concentrations of molecular markers of activated coagulation and fibrinolysis. Blood Coagul. Fibrinolysis. 2004, 15, 213–219. [Google Scholar] [CrossRef] [PubMed]
- de Jonge, E.; Levi, M.; Berends, F.; van der Ende, A.E.; ten Cate, J.W.; Stoutenbeek, C.P. Impaired haemostasis by intravenous administration of a gelatin-based plasma expander in human subjects. Thromb. Haemost. 1998, 79, 286–290. [Google Scholar]
- Aguirre, J.A.; Lucchinetti, E.; Clanachan, A.S.; Plane, F.; Zaugg, M. Unraveling Interactions Between Anesthetics and the Endothelium: Update and Novel Insights. Anesth. Analg. 2016, 122, 330–348. [Google Scholar] [CrossRef]
- Evans, P.A.; Hawkins, K.; Lawrence, M.; Williams, R.; Barrow, M.; Thirumalai, N.; Williams, P. Rheometry and associated techniques for blood coagulation studies. Med. Eng. Phys. 2008, 30, 671–679. [Google Scholar] [CrossRef]
- Ogawa, S.; Szlam, F.; Bolliger, D.; Nishimura, T.; Chen, E.P.; Tanaka, K.A. The impact of hematocrit on fibrin clot formation assessed by rotational thromboelastometry. Anesth. Analg. 2012, 115, 16–21. [Google Scholar] [CrossRef]
- Napolitano, L.M. Hemostatic defects in massive transfusion: An update and treatment recommendations. Expert Rev. Hematol. 2021, 14, 219–239. [Google Scholar] [CrossRef]
- Goodnough, L.T.; Spain, D.A.; Maggio, P. Logistics of transfusion support for patients with massive hemorrhage. Curr. Opin. Anaesthesiol. 2013, 26, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Vlaar, A.P.J.; Dionne, J.C.; de Bruin, S.; Wijnberge, M.; Raasveld, S.J.; van Baarle, F.E.H.P.; Antonelli, M.; Aubron, C.; Duranteau, J.; Juffermans, N.P.; et al. Transfusion strategies in bleeding critically ill adults: A clinical practice guideline from the European Society of Intensive Care Medicine. Intensive Care Med. 2021, 47, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Buscher, H.; Zhang, D.; Nair, P. A pilot, randomised controlled trial of a rotational thromboelastometry-based algorithm to treat bleeding episodes in extracorporeal life support: The TEM Protocol in ECLS Study (TEMPEST). Crit. Care Resusc. 2017, 19, 29–36. [Google Scholar]
- Hoffmann, R.F.; Horsten, S.; Mariani, M.A.; de Vries, A.J. Clinical monitoring of activated clotting time during cardiothoracic surgery: Comparing the Hemochron® Response and Hemochron® Signature Elite. Perfusion 2021, 2676591211049316. [Google Scholar] [CrossRef]
- Ise, H.; Kitahara, H.; Oyama, K.; Takahashi, K.; Kanda, H.; Fujii, S.; Kunisawa, T.; Kamiya, H. Hypothermic circulatory arrest induced coagulopathy: Rotational thromboelastometry analysis. Gen. Thorac. Cardiovasc. Surg. 2020, 68, 754–761. [Google Scholar] [CrossRef]
- Takayama, W.; Endo, A.; Koguchi, H.; Sugimoto, M.; Murata, K.; Otomo, Y. The impact of blood type O on mortality of severe trauma patients: A retrospective observational study. Crit. Care 2018, 22, 100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korkmaz, S. Mean platelet volume and platelet distribution width levels in patients with mild psoriasis vulgaris with metabolic syndrome. Postepy Dermatol. Alergol. 2018, 35, 367–371. [Google Scholar] [CrossRef]
- Gawlita, M.; Wasilewski, J.; Osadnik, T.; Reguła, R.; Bujak, K.; Gonera, M. Mean platelet volume and platelet-large cell ratio as prognostic factors for coronary artery disease and myocardial infarction. Folia Cardiol. 2015, 10, 418–422. [Google Scholar] [CrossRef] [Green Version]
- Kamal, A.H.; Tefferi, A.; Pruthi, R.K. How to interpret and pursue an abnormal prothrombin time, activated partial thromboplastin time, and bleeding time in adults. Mayo Clin. Proc. 2007, 82, 864–873. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Parameter | Median (IQR) before Optilyte® (n = 25) | Median (IQR) before Geloplasma® (n = 25) | ‘p’ |
|---|---|---|---|
| APTT (s) | 29.7 (28.2–33.0) | 30.8 (28.7–33.0) | 0.71 |
| PT (s) | 11.7 (11.4–12.0) | 11.7 (11.4–12.5) | 0.36 |
| INR | 1.01 (0.98-1.04) | 1.01 (0.95–1.08) | 0.42 |
| Fibrinogen (mg/dL) | 198 (183–243) | 200 (177–246) | 0.99 |
| D-dimer (ug/mL) | 171 (109–303) | 198 (133–222) | 0.62 |
| PLT (103/µL) | 244 (226–280) | 238 (222–262) | 0.16 |
| PDW (fl) | 11.6 (11.0–12.9) | 12.0 (10.9–13.3) | 0.73 |
| MPV (fl) | 10.2 (9.9–10.8) | 10.1 (9.8–11.0) | 0.15 |
| P-LCR (%) | 26.8 (24.1–31.3) | 27.5 (23.0–33.4) | 0.19 |
| Assay | Parameter | Median (IQR) before Optilyte® (n = 25) | Median (IQR) before Geloplasma® (n = 25) | ‘p’ |
|---|---|---|---|---|
| EXTEM | CT (s) | 61 (58–66) | 60 (59–66) | 0.86 |
| CFT (s) | 131 (118–148) | 131 (118–147) | 0.30 | |
| AA (◦) | 65 (62–68) | 65 (63–68) | 0.52 | |
| A10 (mm) | 51 (49–54) | 51 (49–55) | 0.84 | |
| A20 (mm) | 58 (56–61) | 59 (56–61) | 0.60 | |
| MCF (mm) | 59 (57–62) | 59 (57–61) | 0.24 | |
| ML (%) | 9 (7–11) | 9 (7–10) | 0.77 | |
| MCE (dynes/cm2) | 144 (133–165) | 144 (131–158) | 0.18 | |
| ΔMCE | 138 (125–155) | 135 (122–150) | 0.14 | |
| INTEM | CT (s) | 166 (161–177) | 170 (167–178) | 0.64 |
| CFT (s) | 75 (68–83) | 75 (66–88) | 0.62 | |
| AA (◦) | 75 (74–76) | 75 (73–77) | 0.98 | |
| A10 (mm) | 56 (53–60) | 57 (53–58) | 0.59 | |
| A20 (mm) | 61 (59–65) | 61 (59–64) | 0.57 | |
| MCF (mm) | 62 (59–65) | 62 (59–65) | 0.55 | |
| ML (%) | 7 (5–8) | 7 (5–9) | 0.45 | |
| MCE (dynes/cm2) | 163 (144–188) | 163 (144–186) | 0.78 | |
| FIBTEM | CT (s) | 61 (57–68) | 64 (60–67) | 0.49 |
| A10 (mm) | 8 (7–10) | 8 (7–11) | 0.13 | |
| A20 (mm) | 9 (8–11) | 8 (7–12) | 0.18 | |
| MCF (mm) | 9 (8–11) | 8 (7–12) | 0.30 | |
| MCE (dynes/cm2) | 10 (8–13) | 9 (8–14) | 0.25 |
| Parameter | Crystalloid (Optilyte®) (n = 25) | Colloid (Geloplasma®) (n = 25) | Post-Dilution Between-Group Differences | ||||
|---|---|---|---|---|---|---|---|
| Before | After | ‘p #’ | Before | After | ‘p *’ | ‘p †’ | |
| APTT (s) | 29.7 (28.2–33.0) | 30.8 (28.7–33.8) | 0.25 | 30.8 (28.7–33.0) | 31.7 (29.7–34.0) | 0.06 | 0.22 |
| PT (s) | 11.7 (11.4–12.0) | 12.0 (11.6–12.6) | <0.0001 | 11.7 (11.4–12.5) | 12.7 (12.2–13.6) | <0.0001 | 0.0001 |
| INR | 1.01(0.98–1.04) | 1.03 (1.00–1.08) | <0.0001 | 1.01 (0.95–1.08) | 1.09 (1.05–1.17) | <0.0001 | 0.0001 |
| Fibrinogen (mg/dL) | 198 (183–243) | 173 (164–214) | <0.0001 | 200 (177–246) | 157 (138–187) | <0.0001 | <0.0001 |
| D-dimer (ug/mL) | 171 (109–303) | 182 (112–296) | 0.44 | 198 (133–222) | 184 (150–378) | 0.15 | 0.20 |
| PLT (103/µL) | 244 (226–280) | 216 (193–238) | <0.0001 | 238 (222–262) | 185 (168–201) | <0.0001 | <0.0001 |
| PDW (fl) | 11.6 (11.0–12.9) | 11.7 (10.6–12.7) | 0.23 | 12.0 (10.9–13.3) | 11.7 (10.9–13.4) | 0.41 | 0.12 |
| MPV (fl) | 10.2 (9.9–10.8) | 10.4 (9.8–10.7) | 0.67 | 10.1 (9.8–11.0) | 10.3 (10.0–11.0) | 0.39 | 0.06 |
| P-LCR (%) | 26.8 (24.1–31.3) | 28.0 (23.4–30.3) | 0.97 | 27.5 (23.0–33.4) | 27.6 (24.4–33.2) | 0.84 | 0.12 |
| Assay | Parameter | Crystalloid (Optilyte®) (n = 25) | Colloid (Geloplasma®) (n = 25) | Post-Dilution Between-Group Differences | ||||
|---|---|---|---|---|---|---|---|---|
| Before | After | ‘p #’ | Before | After | ‘p *’ | ‘p †’ | ||
| EXTEM | CT (s) | 61 (58–66) | 60 (57–65) | 0.98 | 60 (59–66) | 61 (58–65) | 0.59 | 0.88 |
| CFT (s) | 131 (118–148) | 135 (120–155) | 0.02 | 131 (118–147) | 149 (128–172) | <0.0001 | 0.0006 | |
| AA (◦) | 65 (62–68) | 64 (61–67) | 0.14 | 65 (63–68) | 62 (58–65) | <0.0001 | 0.0025 | |
| A10 (mm) | 51 (49–54) | 50 (47–53) | 0.002 | 51 (49–55) | 48 (44–51) | <0.0001 | 0.0047 | |
| A20 (mm) | 58 (56–61) | 57 (55–60) | 0.003 | 59 (56–61) | 56 (52–58) | <0.0001 | 0.015 | |
| MCF (mm) | 59 (57–62) | 58 (56–62) | 0.007 | 59 (57–61) | 56 (53–60) | <0.0001 | 0.016 | |
| ML (%) | 9 (7–11) | 8 (8–11) | 0.86 | 9 (7–10) | 8 (6–11) | 0.23 | 0.54 | |
| MCE (dynes/cm2) | 144 (133–165) | 138 (126–163) | 0.004 | 144 (131–158) | 127 (113–152) | 0.0001 | 0.01 | |
| ΔMCE | 138 (125–155) | 131 (118–152) | 0.013 | 135 (122–150) | 119 (106–144) | 0.0001 | 0.015 | |
| INTEM | CT (s) | 166 (161–177) | 162 (153–175) | 0.015 | 170 (167–178) | 169 (150–180) | 0.027 | 0.90 |
| CFT (s) | 75 (68–83) | 81 (69–90) | 0.25 | 75 (66–88) | 98 (88–113) | <0.0001 | <0.0001 | |
| AA (◦) | 75 (74–76) | 74 (73–76) | 0.18 | 75 (73–77) | 71 (68–73) | <0.0001 | <0.0001 | |
| A10 (mm) | 56 (53–60) | 55 (52–58) | 0.021 | 57 (53–58) | 50 (47–52) | <0.0001 | <0.0001 | |
| A20 (mm) | 61 (59–65) | 61 (58–63) | 0.032 | 61 (59–64) | 56 (53–58) | <0.0001 | <0.0001 | |
| MCF (mm) | 62 (59–65) | 61 (58–64) | 0.014 | 62 (59–65) | 56 (54–59) | <0.0001 | <0.0001 | |
| ML (%) | 7 (5–8) | 7 (5–8) | 0.28 | 7 (5–9) | 7 (5–9) | 0.95 | 0.045 | |
| MCE (dynes/cm2) | 163 (144–188) | 156 (138–176) | 0.008 | 163 (144–186) | 127 (116–144) | <0.0001 | <0.0001 | |
| FIBTEM | CT (s) | 61 (57–68) | 64 (59–67) | 0.27 | 64 (60–67) | 64 (60–71) | 0.34 | 0.62 |
| A10 (mm) | 8 (7–10) | 7 (6–9) | 0.016 | 8 (7–11) | 6 (5–8) | <0.0001 | 0.003 | |
| A20 (mm) | 9(8–11) | 8 (7–11) | 0.024 | 8 (7–12) | 7 (6–9) | <0.0001 | 0.0003 | |
| MCF (mm) | 9 (8–11) | 8 (7–10) | 0.011 | 8 (7–12) | 7 (6–8) | <0.0001 | 0.0008 | |
| MCE (dynes/cm2) | 10 (8–13) | 9 (8–11) | 0.005 | 9 (8–14) | 8 (6–9) | <0.0001 | 0.0005 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wiórek, A.; Mazur, P.K.; Żurawska, E.; Krzych, Ł.J. In Vivo Effects of Balanced Crystalloid or Gelatine Infusions on Functional Parameters of Coagulation and Fibrinolysis: A Prospective Randomized Crossover Study. J. Pers. Med. 2022, 12, 909. https://doi.org/10.3390/jpm12060909
Wiórek A, Mazur PK, Żurawska E, Krzych ŁJ. In Vivo Effects of Balanced Crystalloid or Gelatine Infusions on Functional Parameters of Coagulation and Fibrinolysis: A Prospective Randomized Crossover Study. Journal of Personalized Medicine. 2022; 12(6):909. https://doi.org/10.3390/jpm12060909
Chicago/Turabian StyleWiórek, Agnieszka, Piotr K. Mazur, Elżbieta Żurawska, and Łukasz J. Krzych. 2022. "In Vivo Effects of Balanced Crystalloid or Gelatine Infusions on Functional Parameters of Coagulation and Fibrinolysis: A Prospective Randomized Crossover Study" Journal of Personalized Medicine 12, no. 6: 909. https://doi.org/10.3390/jpm12060909