
Survey on Use of Local and Systemic Corticosteroids in the Management of Chronic Rhinosinusitis with Nasal Polyps: Identification of Unmet Clinical Needs

 , , , , , , , , ,
, , , , , , , , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Survey Distribution
3. Results
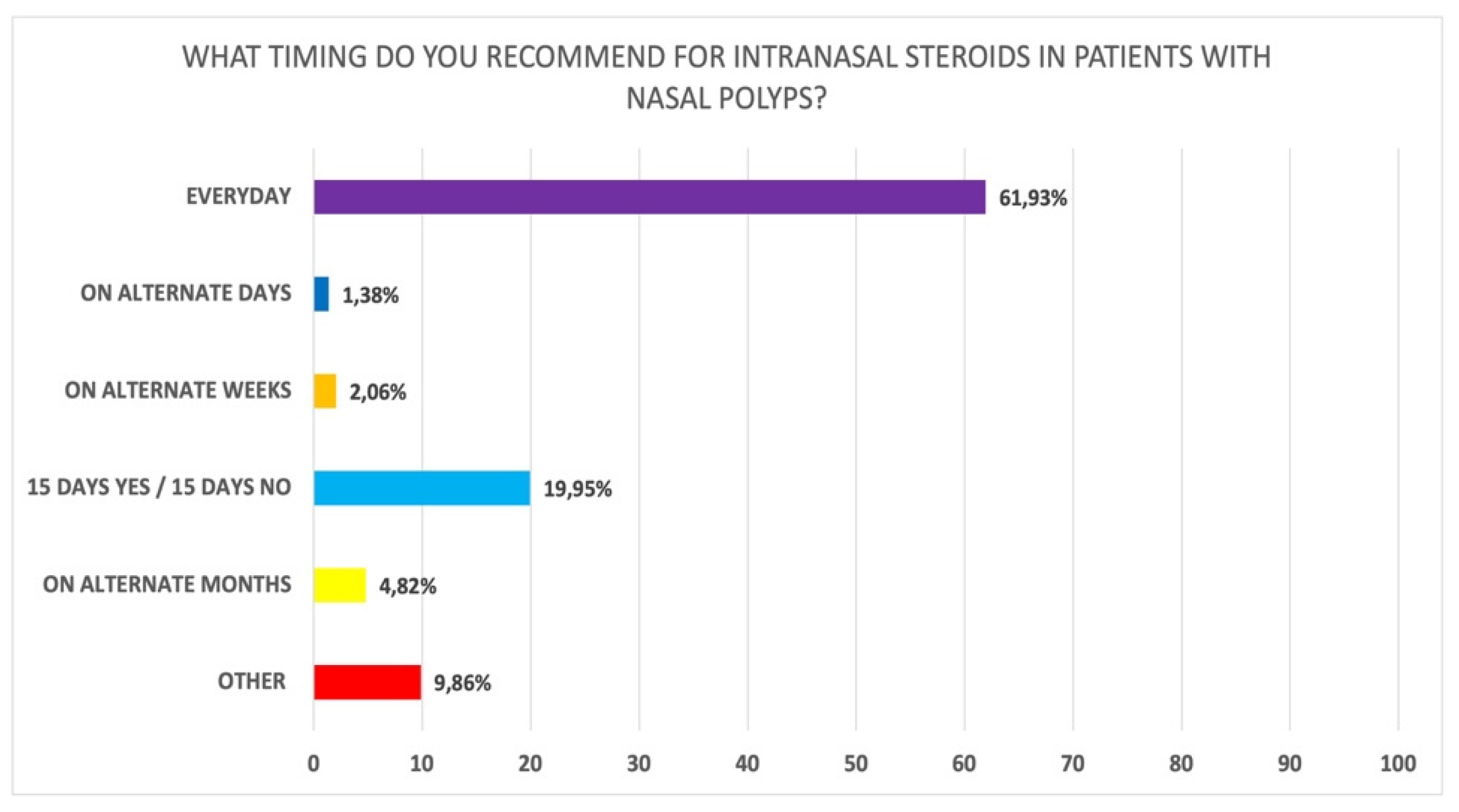
3.1. Use of Local Steroids in CRSwNP
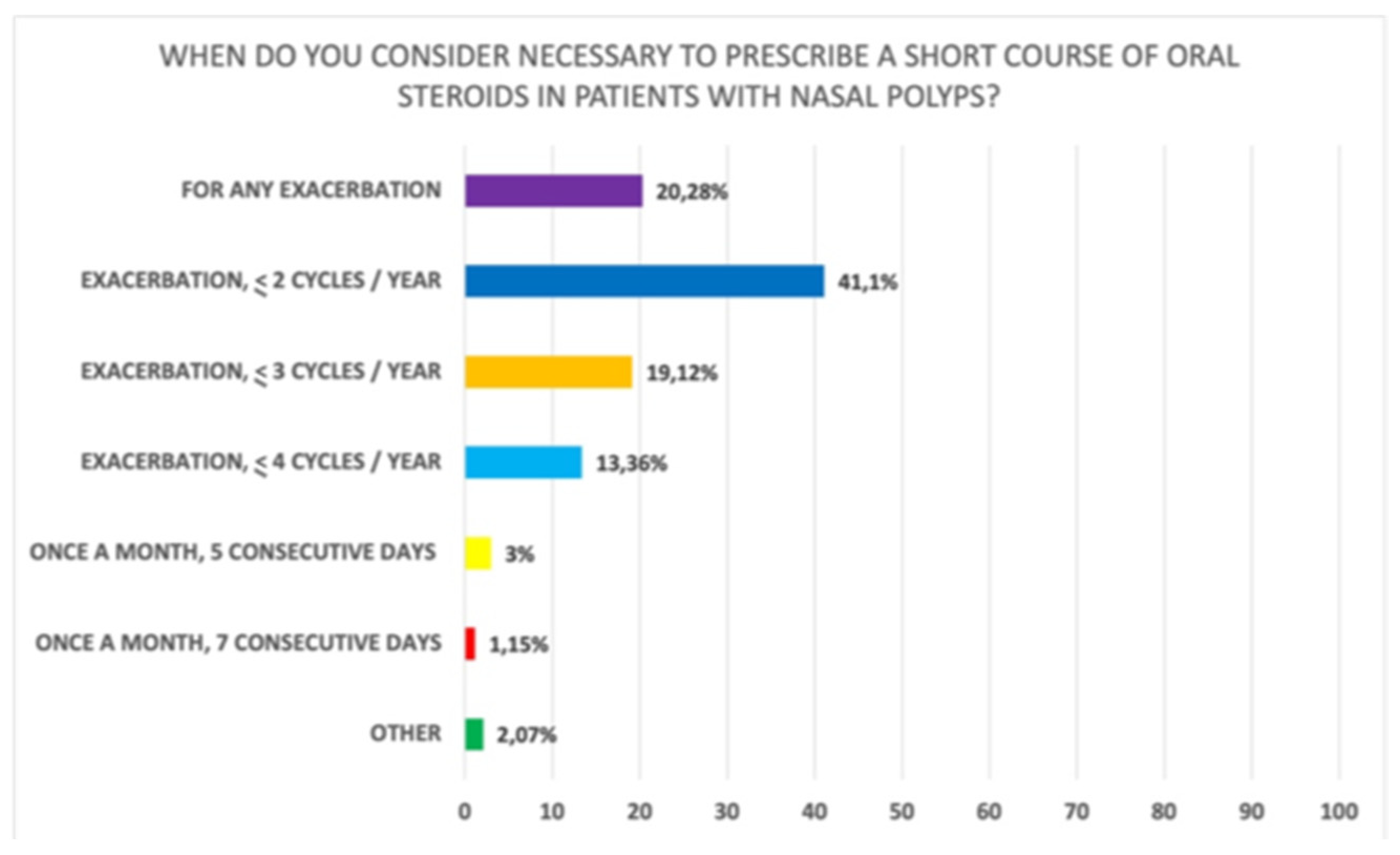
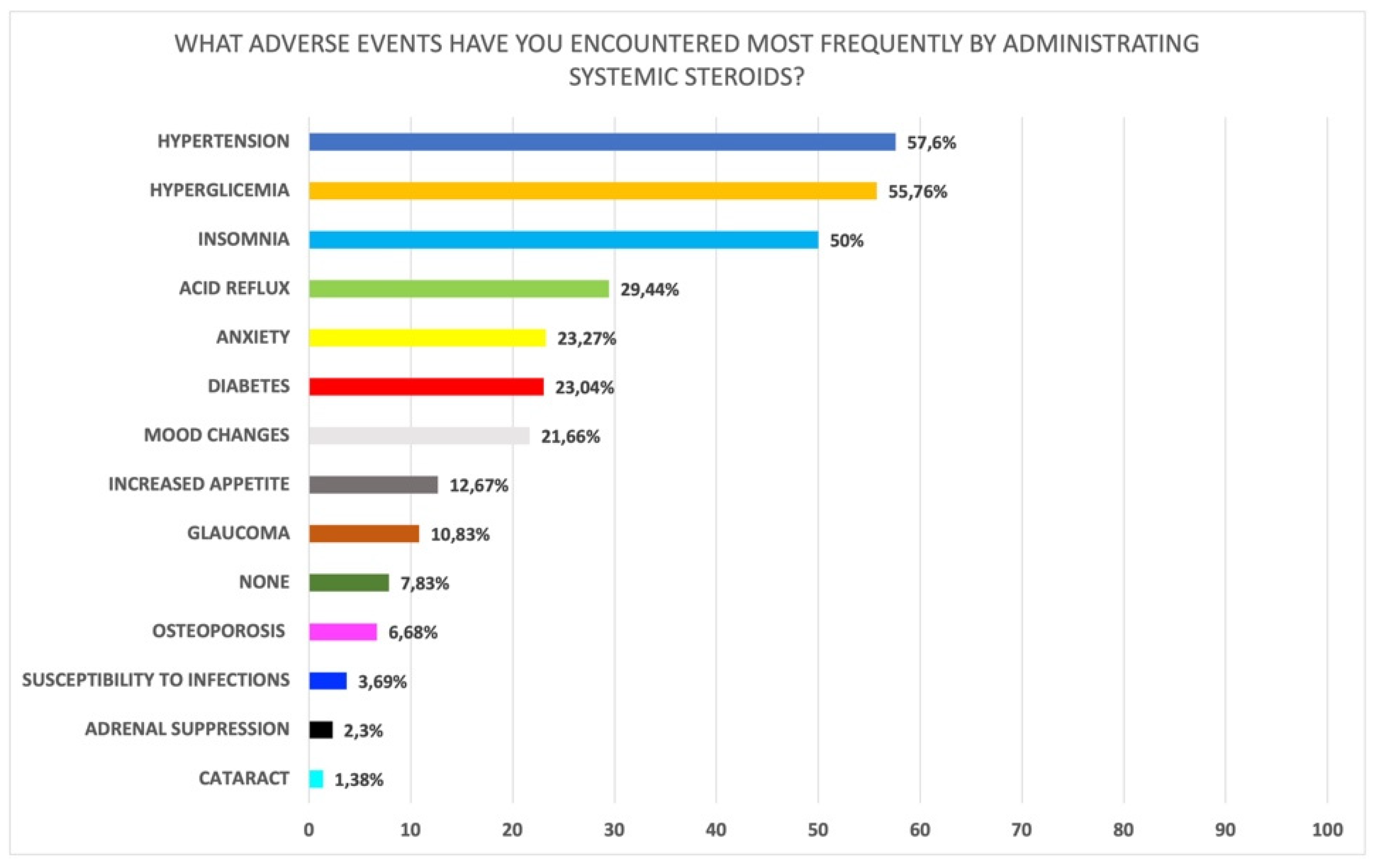
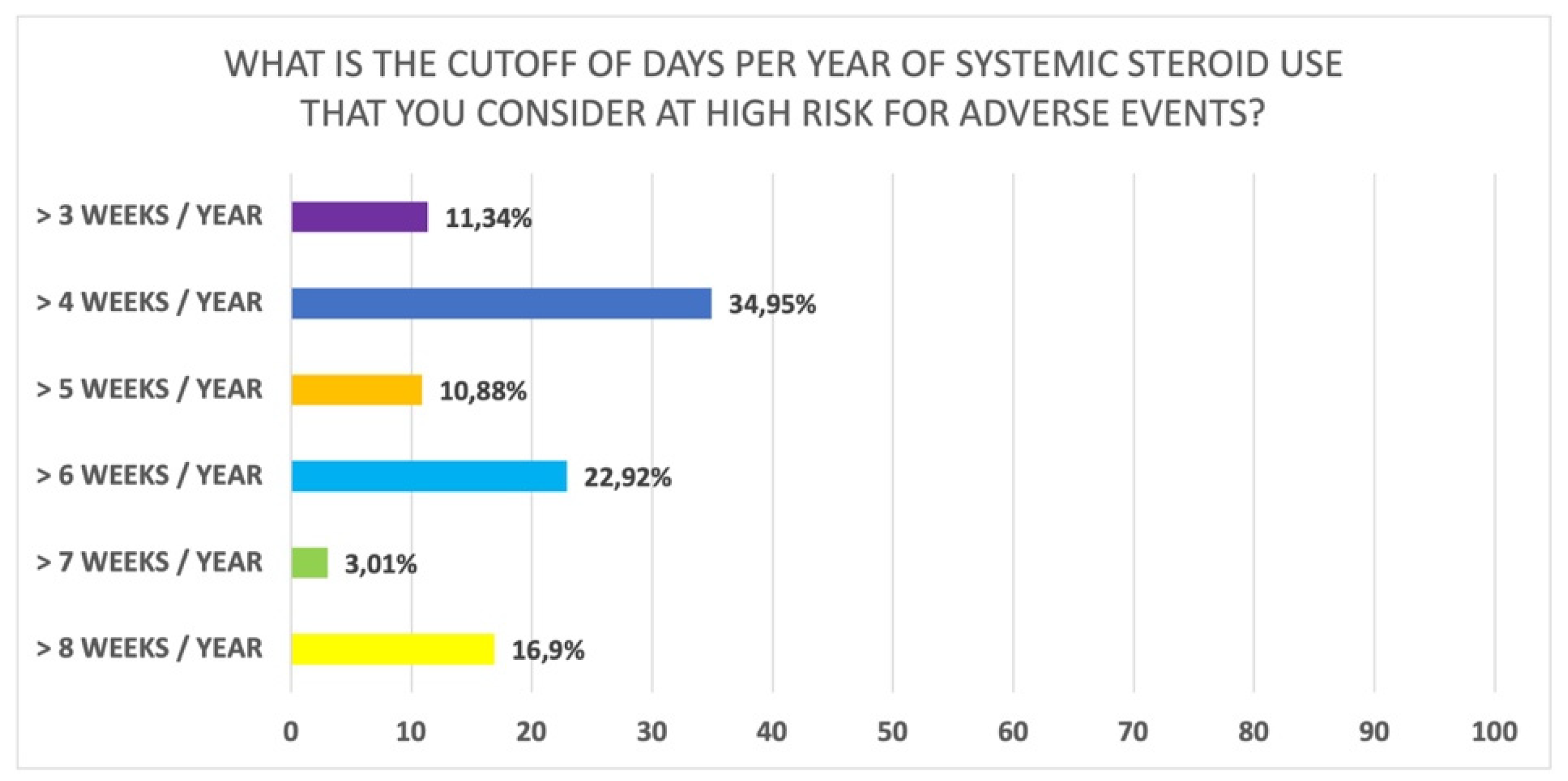
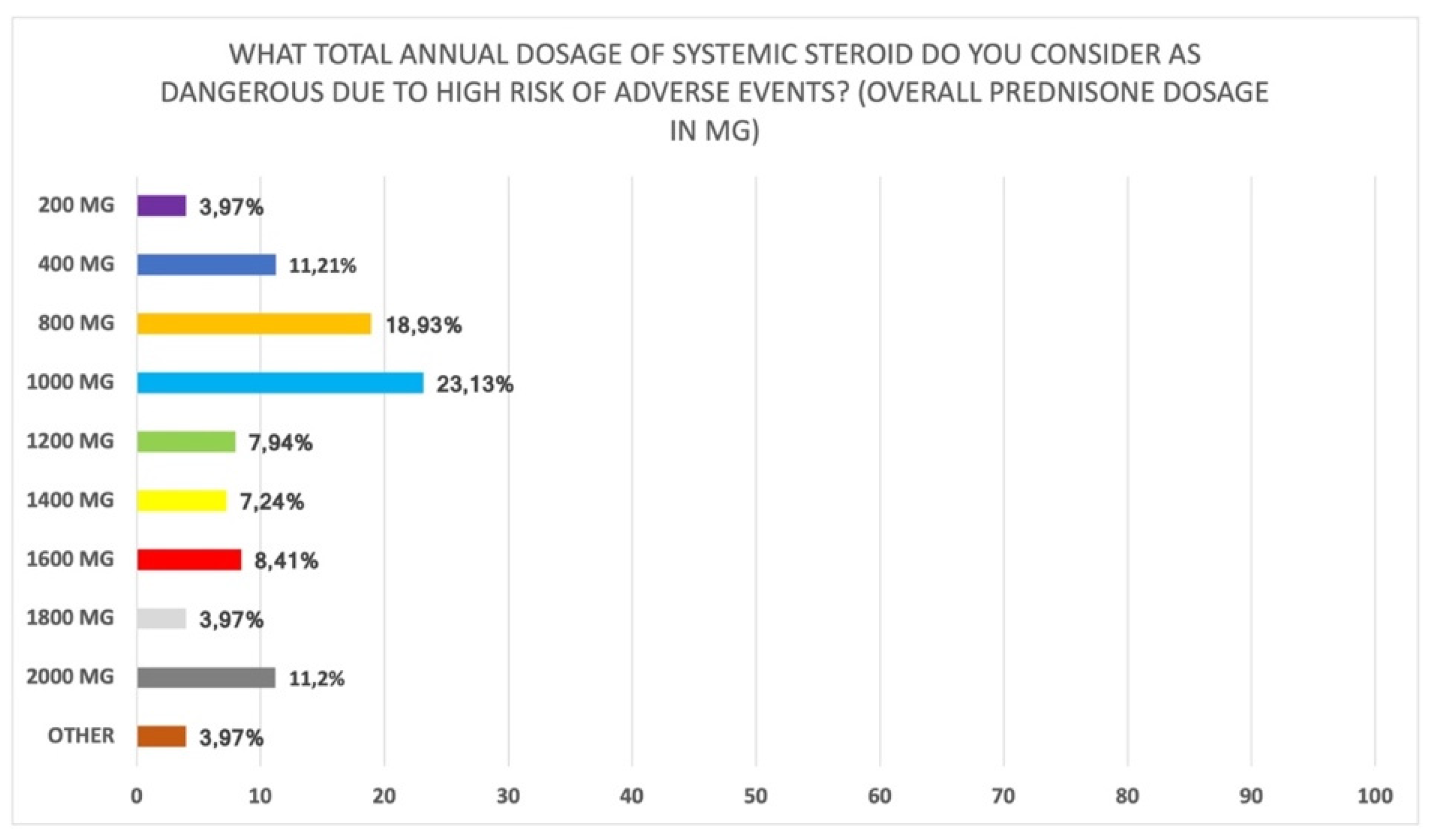
3.2. Use of Systemic Steroids in CRSwNP
3.3. Definition of Disease Control Based on Steroid Use
3.4. Perioperative Use of Local and Systemic Steroids
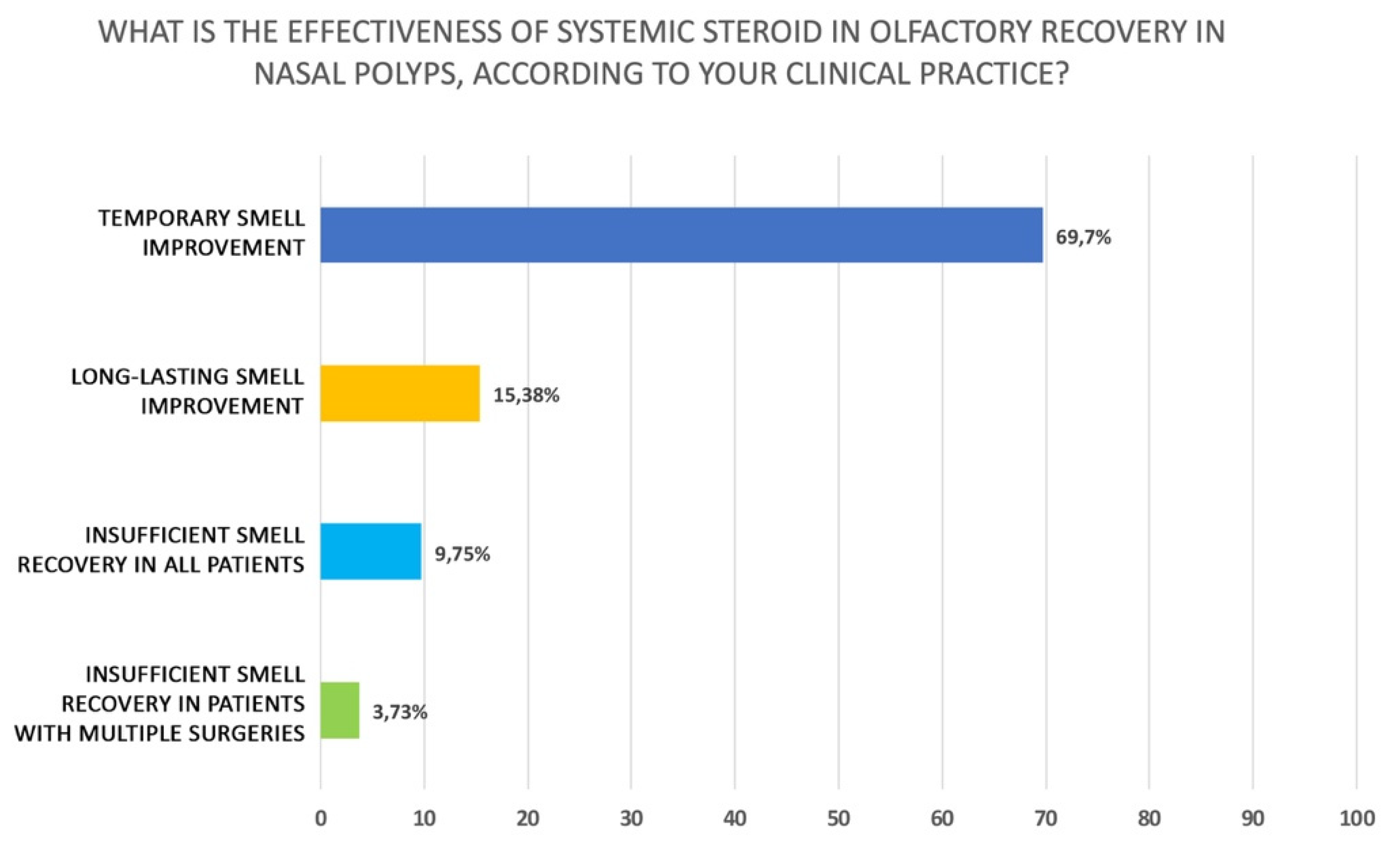
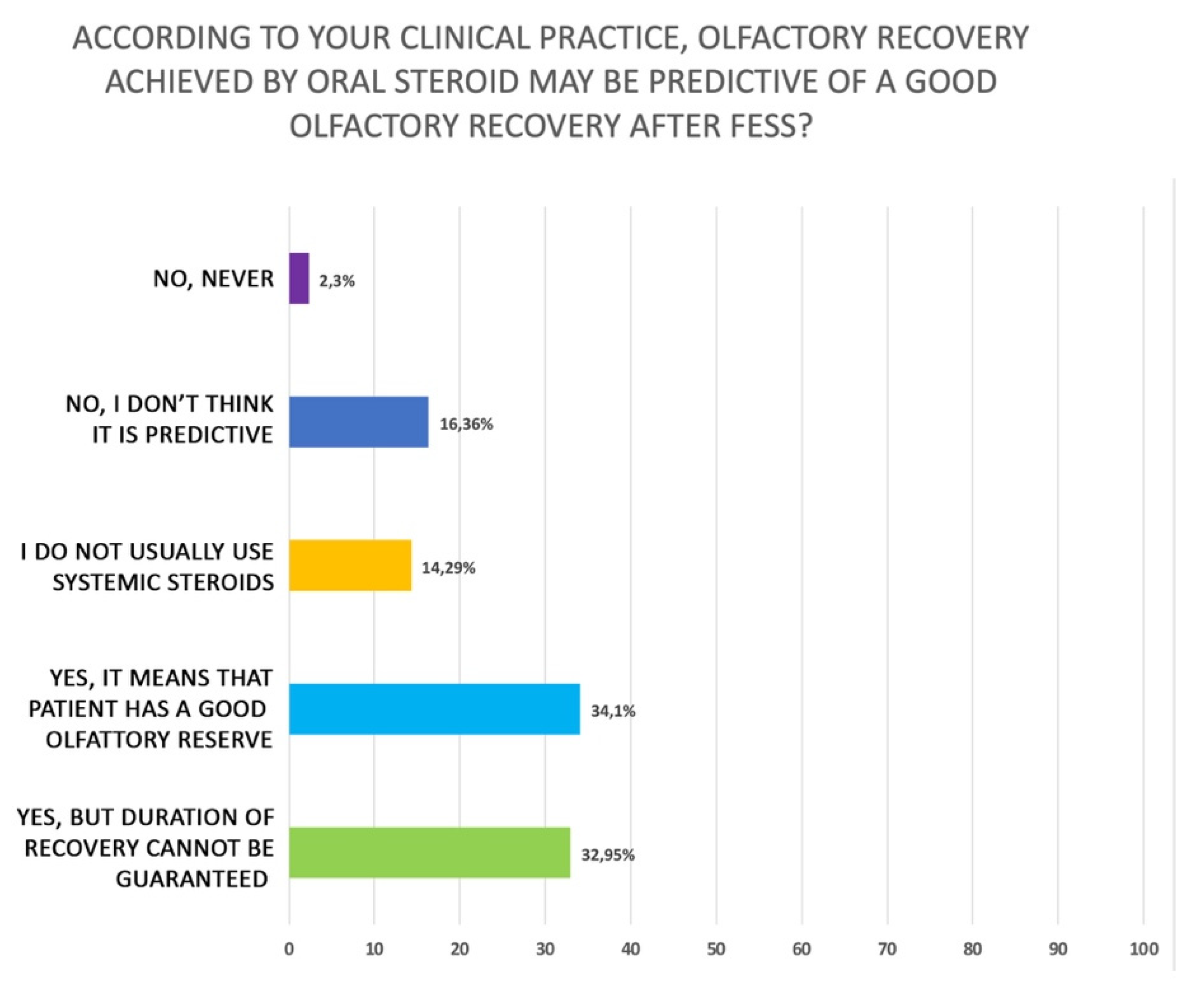
3.5. Use of Steroids in Olfactory Dysfunction Associated with Polyposis
4. Discussion
4.1. Use of Local Steroids in CRSwNP
4.2. Use of Systemic Steroids in CRSwNP
4.3. Definition of Disease Control Based on Steroid Use
4.4. Perioperative Use of Local and Systemic Steroids
4.5. Use of Steroids in Olfactive Dysfunction Associated with Polyposis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hopkins, C. Chronic Rhinosinusitis with Nasal Polyps. N. Engl. J. Med. 2019, 381, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharyya, N.; Villeneuve, S.; Joish, V.N.; Amand, C.; Mannent, L.; Amin, N.; Rowe, P.; Maroni, J.; Eckert, L.; Yang, T.; et al. Cost burden and resource utilization in patients with chronic rhinosinusitis and nasal polyps. Laryngoscope 2019, 129, 1969–1975. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fokkens, W.J.; Lund, V.J.; Mullol, J.; Bachert, C.; Alobid, I.; Baroody, F.; Cohen, N.; Cervin, A.; Douglas, R.; Gevaert, P.; et al. EPOS 2012: European position paper on rhinosinusitis and nasal polyps 2012. A summary for otorhinolaryngologists. Rhinology 2012, 50, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Stevens, W.W.; Schleimer, R.P.; Kern, R.C. Chronic Rhinosinusitis with Nasal Polyps. J. Allergy Clin. Immunol. Pract. 2016, 4, 565–572. [Google Scholar] [CrossRef] [Green Version]
- Fokkens, W.J.; Lund, V.J.; Hopkins, C.; Hellings, P.W.; Kern, R.; Reitsma, S.; Toppila-Salmi, S.; Bernal-Sprekelsen, M.; Mullol, J. Executive summary of EPOS 2020 including integrated care pathways. Rhinology 2020, 58, 82–111. [Google Scholar] [CrossRef]
- Hox, V.; Lourijsen, E.; Jordens, A.; Aasbjerg, K.; Agache, I.; Alobid, I.; Bachert, C.; Boussery, K.; Campo, P.; Fokkens, W.; et al. Benefits and harm of systemic steroids for short- and long-term use in rhinitis and rhinosinusitis: An EAACI position paper. Clin. Transl. Allergy 2020, 10, 1. [Google Scholar] [CrossRef]
- Boyle, J.V.; Lam, K.; Han, J.K. Dupilumab in the treatment of chronic rhinosinusitis with nasal polyposis. Immunotherapy 2020, 12, 111–121. [Google Scholar] [CrossRef]
- Licari, A.; Castagnoli, R.; Marseglia, A.; Olivero, F.; Votto, M.; Ciprandi, G.; Marseglia, G.L. Dupilumab to Treat Type 2 Inflammatory Diseases in Children and Adolescents. Paediatr. Drugs 2020, 22, 295–310. [Google Scholar] [CrossRef]
- Sastre, J.; Davila, I. Dupilumab: A New Paradigm for the Treatment of Allergic Diseases. J. Investig. Allergol. Clin. Immunol. 2018, 28, 139–150. [Google Scholar] [CrossRef] [Green Version]
- Gelardi, M.; Iannuzzi, L.; De Giosa, M.; Taliente, S.; De Candia, N.; Quaranta, N.; De Corso, E.; Seccia, V.; Ciprandi, G. Non-surgical management of chronic rhinosinusitis with nasal polyps based on clinical-cytological grading: A precision medicine-based approach. Acta Otorhinolaryngol. Ital. 2017, 37, 38–45. [Google Scholar] [CrossRef]
- Lombardi, C.; Asero, R.; Bagnasco, D.; Blasi, F.; Bonini, M.; Bussi, M.; Canevari, R.F.; Canonica, G.W.; Castelnuovo, P.; Cecchi, L.; et al. ARIA-ITALY multidisciplinary consensus on nasal polyposis and biological treatments. World Allergy Organ. J. 2021, 14, 100592. [Google Scholar] [CrossRef] [PubMed]
- Passali, D.; Cingi, C.; Cambi, J.; Passali, F.; Muluk, N.B.; Bellussi, M.L. A survey on chronic rhinosinusitis: Opinions from experts of 50 countries. Eur. Arch. Otorhinolaryngol. 2016, 273, 2097–2109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, K.A.; Rudmik, L. Delivery of Topical Therapies. Adv. Otorhinolaryngol. 2016, 79, 114–120. [Google Scholar] [PubMed]
- Wallace, D.V. Treatment options for chronic rhinosinusitis with nasal polyps. Allergy Asthma Proc. 2021, 42, 450–460. [Google Scholar] [CrossRef]
- Passali, D.; Spinosi, M.C.; Crisanti, A.; Belussi, L.M. Mometasone furoate nasal spray: A systematic review. Multidiscip. Respir. Med. 2016, 11, 18. [Google Scholar] [CrossRef] [Green Version]
- Snidvongs, K.; Kalish, L.; Sacks, R.; Sivasubramaniam, R.; Cope, D.; Harvey, R.J. Sinus Surgery and Delivery Method Influence the Effectiveness of Topical Corticosteroids for Chronic Rhinosinusitis: Systematic Review and Meta-Analysis. Am. J. Rhinol. Allergy 2013, 27, 221–233. [Google Scholar] [CrossRef] [Green Version]
- De Corso, E.; Settimi, S.; Tricarico, L.; Mele, D.A.; Masrapasqua, R.F.; Di Cesare, T.; Salvati, A.; Trozzi, L.; De Vita, C.; Romanello, M.; et al. Predictors of Disease Control After Endoscopic Sinus Surgery Plus Long-Term Local Corticosteroids in CRSwNP. Am. J. Rhinol. Allergy 2021, 35, 77–85. [Google Scholar] [CrossRef]
- Ganesh, V.; Banigo, A.; McMurran, A.E.L.; Shakeel, M.; Ram, B. Does intranasal steroid spray technique affect side effects and compliance? Results of a patient survey. J. Laryngol. Otol. 2017, 131, 991–996. [Google Scholar] [CrossRef]
- Valverde-Monge, M.; Barroso, B.; Ortega-Martin, L.; Betancor, D.; Santillan, J.; Villacampa, J.; Sastre, J. Exploring adherence to treatment in nasal polyposis. J. Investig. Allergol. Clin. Immunol. 2021, 32. online ahead of print. [Google Scholar] [CrossRef]
- Loh, C.Y.; Chao, S.S.; Chan, Y.H.; Wang, D.Y. A clinical survey on compliance in the treatment of rhinitis using nasal steroids. Allergy 2004, 59, 1168–1172. [Google Scholar] [CrossRef]
- Ocak, E.; Acar, B.; Kocaöz, D. Medical adherence to intranasal corticosteroids in adult patients. Braz. J. Otorhinolaryngol. 2017, 83, 558–562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phillips, K.M.; Hoehle, L.P.; Caradonna, D.S.; Gray, S.T.; Sedaghat, A.R. Intranasal corticosteroids and saline: Usage and adherence in chronic rhinosinusitis patients. Laryngoscope 2020, 130, 852–856. [Google Scholar] [CrossRef] [PubMed]
- Jamil, W.; Alahwal, A.; Suman, R.; Naz, F.; Beech, T. Do patients correctly use steroid nose spray? A patient-reported survey of the nasal spray technique and patient compliance. Authorea 2020. [Google Scholar] [CrossRef]
- Park, D.-Y.; Choi, J.H.; Kim, D.-K.; Jung, Y.G.; Mun, S.J.; Min, H.J.; Park, S.K.; Shin, J.-M.; Yang, H.C.; Hong, S.-N.; et al. Clinical Practice Guideline: Nasal Irrigation for Chronic Rhinosinusitis in Adults. Clin. Exp. Otorhinolaryngol. 2022, 15, 5–23. [Google Scholar] [CrossRef] [PubMed]
- Head, K.; Chong, L.Y.; Hopkins, C.; Philpott, C.; Burton, M.J.; Schilder, A.G.M. Short-course oral steroids alone for chronic rhinosinusitis. Cochrane Database Syst Rev. 2016, 4, CD011991. [Google Scholar] [CrossRef] [Green Version]
- Head, K.; Chong, L.Y.; Hopkins, C.; Philpott, C.; Schilder, A.G.M.; Burton, M.J. Short-course oral steroids as an adjunct therapy for chronic rhinosinusitis. Cochrane Database Syst. Rev. 2016, 4, CD011992. [Google Scholar] [CrossRef] [Green Version]
- De Corso, E.; Bellocchi, G.; De Benedetto, M.; Lombardo, N.; Macchi, A.; Malvezzi, L.; Motta, G.; Pagella, F.; Vicini, C.; Passalini, D. Biologics for severe uncontrolled chronic rhinosinusitis with nasal polyps: A change management approach. Consensus of the Joint Committee of Italian Society of Otorhinolaryngology on biologics in rhinology. Acta Otorhinolaryngol. Ital. 2022, 42, 1–16. [Google Scholar] [CrossRef]
- Hopkins, C.; McKenzie, J.; Anari, S.; Carrie, S.; Ramakrishnan, Y.; Kara, N.; Philpott, C.; Hobson, J.; Qureishi, A.; Stew, B.; et al. British Rhinological Society Consensus Guidance on the use of biological therapies for chronic rhinosinusitis with nasal polyps. Clin. Otolaryngol. 2021, 46, 1037–1043. [Google Scholar] [CrossRef]
- Alobid, I.; Benítez, P.; Cardelús, S.; Callejas, F.D.B.; Lehrer-Coriat, E.; Pujols, L.; Picado, C.; Mullol, J. Oral plus nasal corticosteroids improve smell, nasal congestion, and inflammation in sino-nasal polyposis. Laryngoscope 2014, 124, 50–56. [Google Scholar] [CrossRef]
- Hellings, P.W.; Rombaux, P. Medical therapy and smell dysfunction. B-ENT 2009, 5 (Suppl. S13), 71–75. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Options | Answers% |
|---|---|
| How to use the nasal spray | 0.69% |
| How to position the device | 58.62% |
| Position of the body | 33.33% |
| Time of day to administer it | 39.77% |
| When to do it with respect to nasal washing (before or after) | 68.51% |
| Other | 2.53% |
| Options | Answers% |
|---|---|
| Teach the patient how to use it correctly | 49.89% |
| Discontinue the drug for at least 10 days per month | 39.31% |
| Administration in alternate weeks | 3.68% |
| Administration 15 days yes and 15 no | 15.40% |
| Administration on alternate days | 58.39% |
| Use of adjuvant drugs (hyaluronic acid, emollients, etc.) | 49.89% |
| None of the above | 3.91% |
| Other | 1.61% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Corso, E.; Pipolo, C.; Cantone, E.; Ottaviano, G.; Gallo, S.; Canevari, F.R.M.; Macchi, A.; Monti, G.; Cavaliere, C.; La Mantia, I.; et al. Survey on Use of Local and Systemic Corticosteroids in the Management of Chronic Rhinosinusitis with Nasal Polyps: Identification of Unmet Clinical Needs. J. Pers. Med. 2022, 12, 897. https://doi.org/10.3390/jpm12060897
De Corso E, Pipolo C, Cantone E, Ottaviano G, Gallo S, Canevari FRM, Macchi A, Monti G, Cavaliere C, La Mantia I, et al. Survey on Use of Local and Systemic Corticosteroids in the Management of Chronic Rhinosinusitis with Nasal Polyps: Identification of Unmet Clinical Needs. Journal of Personalized Medicine. 2022; 12(6):897. https://doi.org/10.3390/jpm12060897
Chicago/Turabian StyleDe Corso, Eugenio, Carlotta Pipolo, Elena Cantone, Giancarlo Ottaviano, Stefania Gallo, Frank Rikki Mauritz Canevari, Alberto Macchi, Giulia Monti, Carlo Cavaliere, Ignazio La Mantia, and et al. 2022. "Survey on Use of Local and Systemic Corticosteroids in the Management of Chronic Rhinosinusitis with Nasal Polyps: Identification of Unmet Clinical Needs" Journal of Personalized Medicine 12, no. 6: 897. https://doi.org/10.3390/jpm12060897