
Misjudgment of Skills in Clinical Examination Increases in Medical Students Due to a Shift to Exclusively Online Studies during the COVID-19 Pandemic


Abstract
:1. Introduction
2. Materials and Methods
2.1. Curricular Concept of Teaching
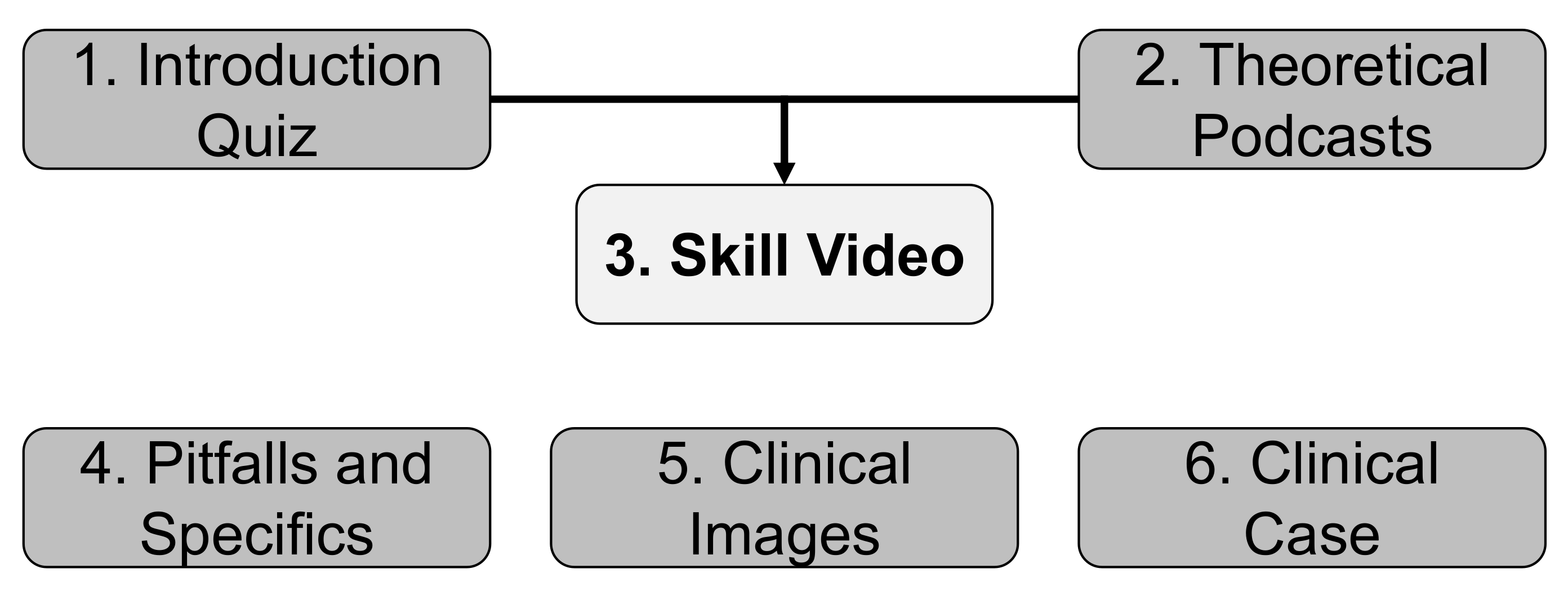
2.2. Concept of the Online Courses
2.3. Self-Evaluation Questionnaire and Objective Structured Clinical Exam
2.4. Data and Statistical Analysis
3. Results
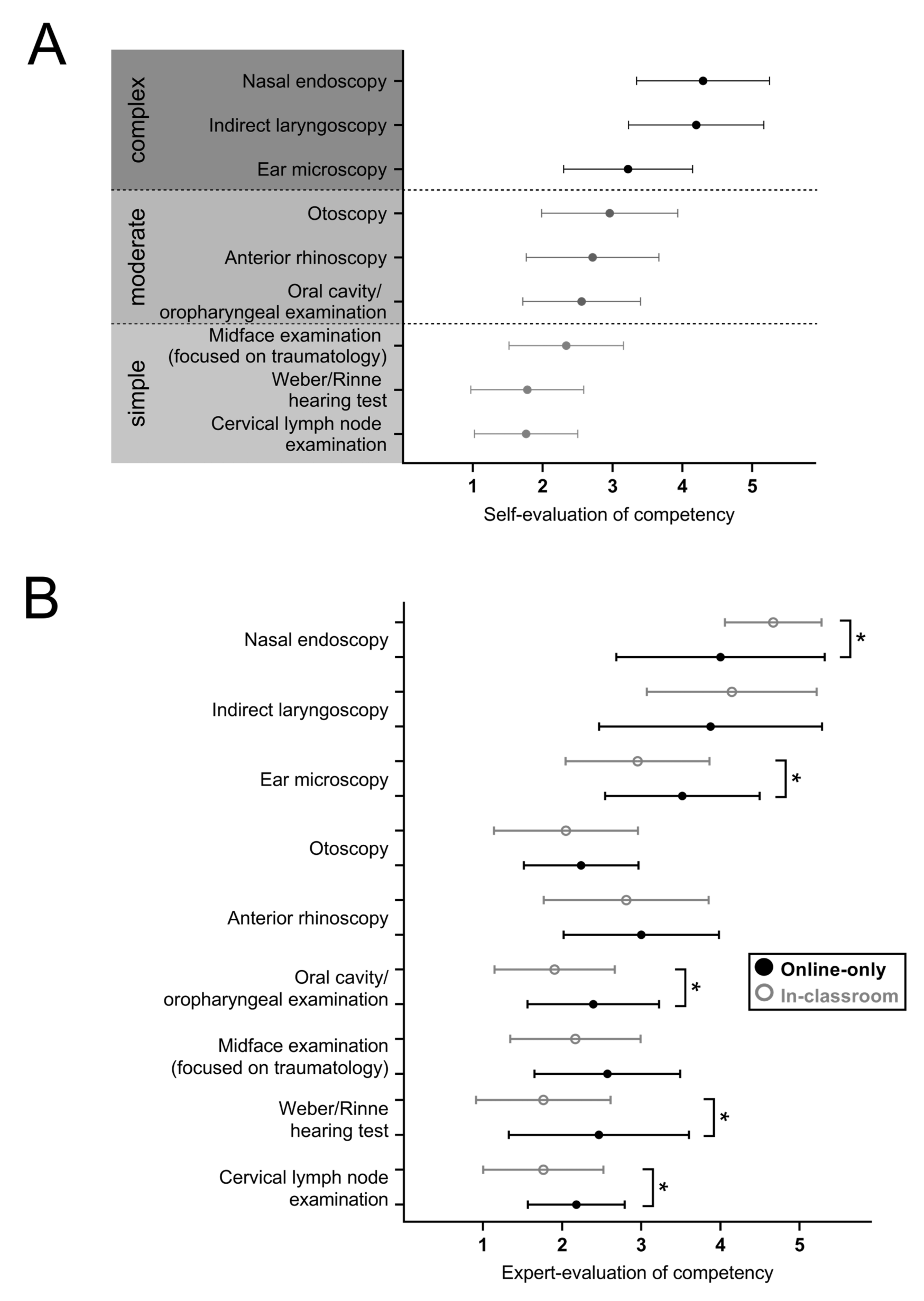
3.1. Overall Self-Evaluation of Examination Competency Does Not Differ Significantly after Online-Only and In-Classroom ENT Skill Teaching
3.2. Objective Examination Performance of Students Varies after In-Classroom and Online Teaching in Single Examination Items While Overall Assessment Remains Comparable
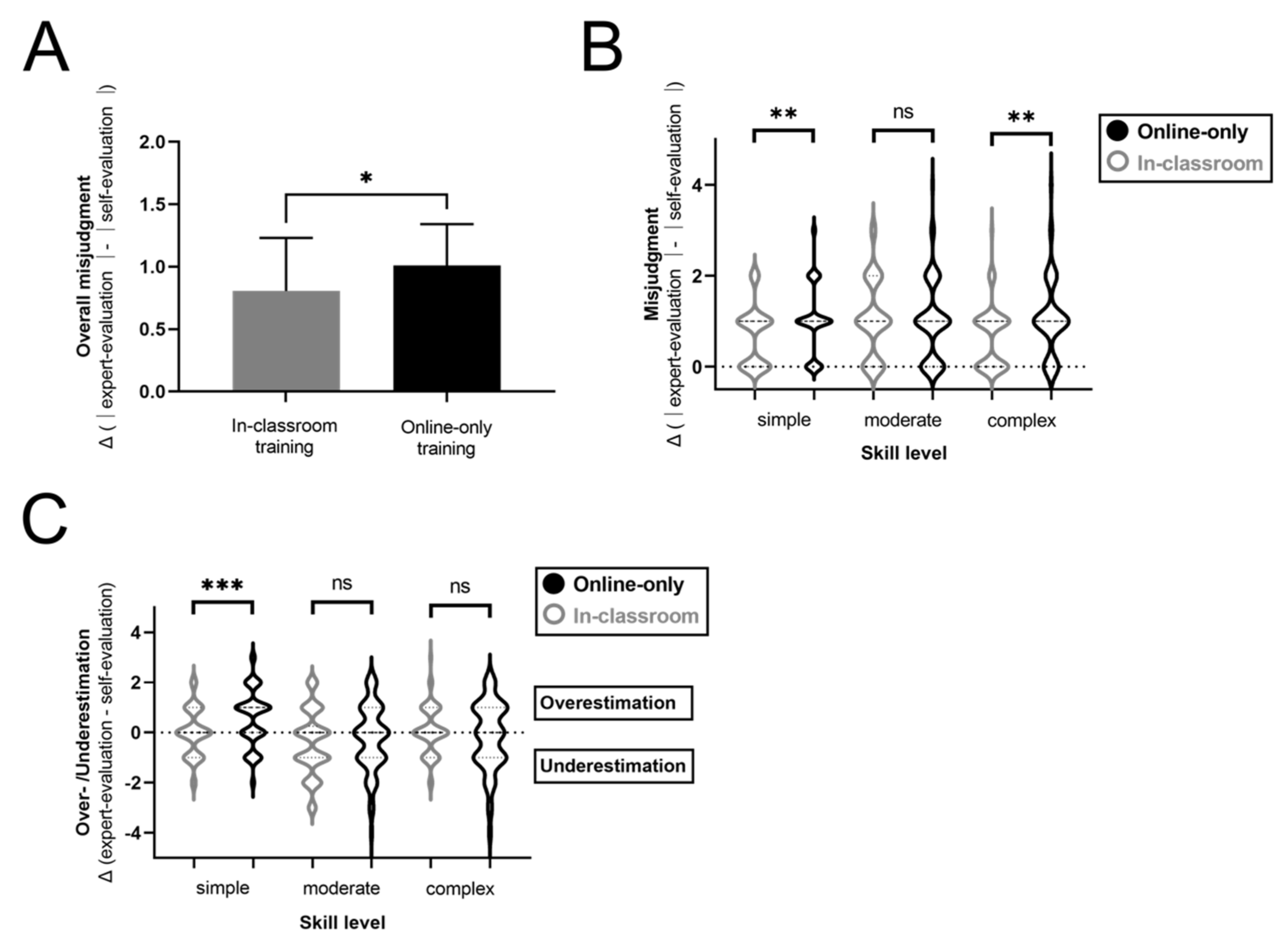
3.3. Misjudgment of One’s Skill Level Increases after Online-Only Training Compared to in-Classroom Teaching
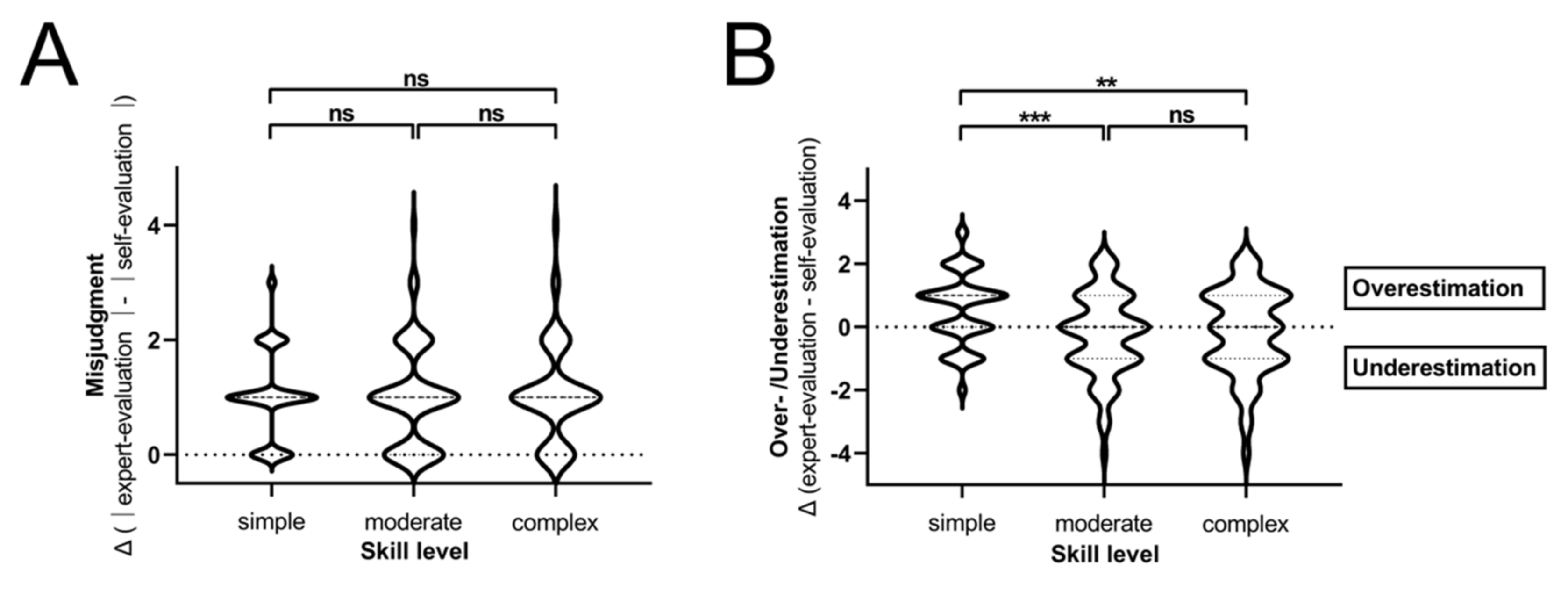
3.4. Highest Levels of Overestimation Are Observed after Online Training in Simple Tasks
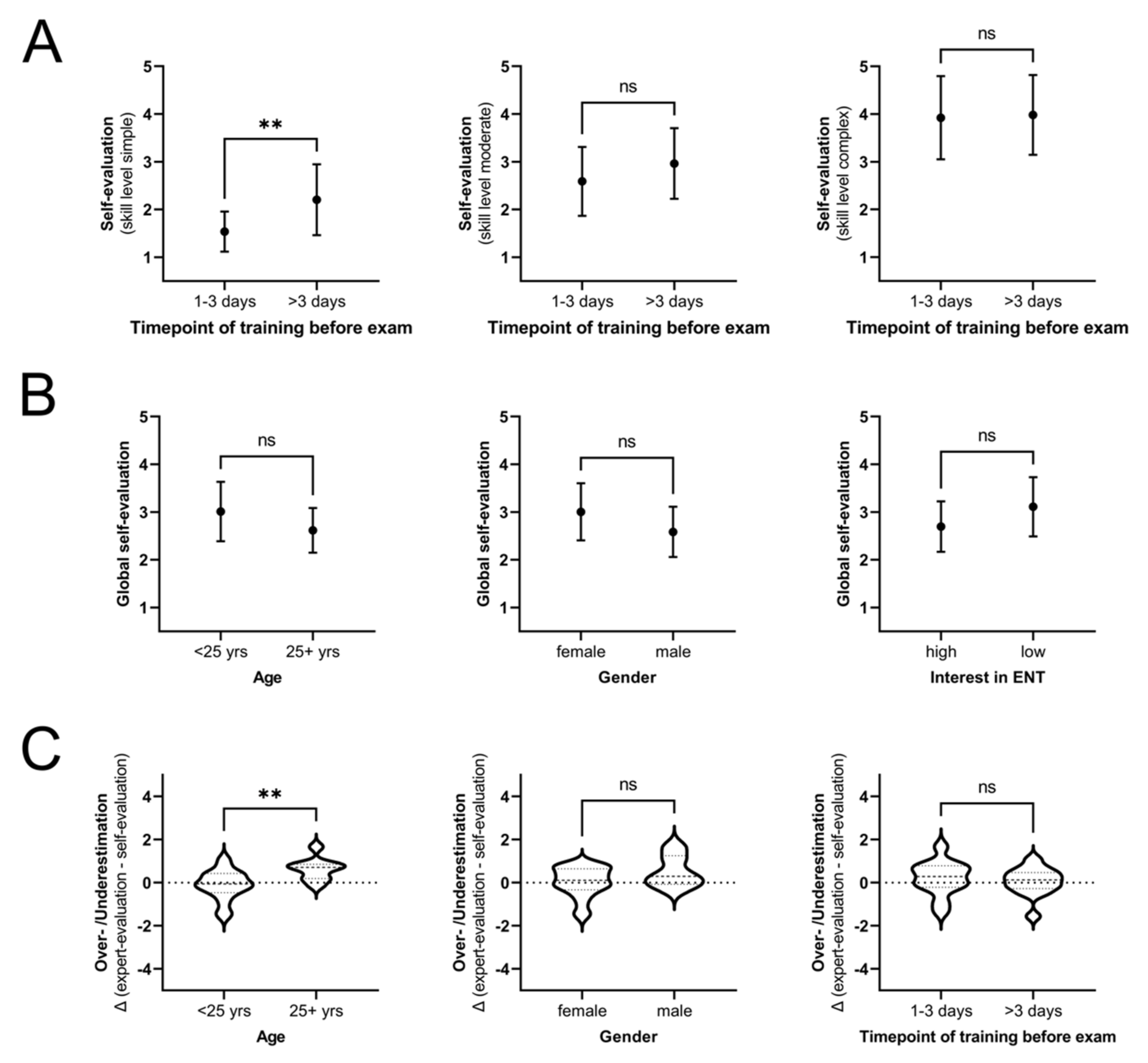
3.5. While Gender and Interest in ENT Do Not Influence Self-Evaluation and Misjudgment, Higher Age of Participants Is Associated with an Overestimation of Skills
3.6. What Is the Student’s Opinion on Online Training?
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hussain, S.; Almas, T. Impact of COVID-19 on Medical Students Aspiring Toward a Career in Otolaryngology: A Medical Student’s Perspective. Otolaryngol. Head Neck Surg. 2021, 165, 385–386. [Google Scholar] [CrossRef] [PubMed]
- Bachmann, C.; Paz Hernandez, A.L.; Müller, S.; Khalatbarizamanpoor, S.; Tschiesche, T.; Reißmann, F.; Kiesow, L.; Ebbert, D.; Smirnow, W.; Wilken, A.; et al. Digital teaching and learning of surgical skills (not only) during the pandemic: A report on a blended learning project. GMS J. Med. Educ. 2020, 37, Doc68. [Google Scholar] [CrossRef] [PubMed]
- Chao, T.N.; Frost, A.S.; Brody, R.M.; Byrnes, Y.M.; Cannady, S.B.; Luu, N.N.; Rajasekaran, K.; Shanti, R.M.; Silberthau, K.R.; Triantafillou, V.; et al. Creation of an Interactive Virtual Surgical Rotation for Undergraduate Medical Education during the COVID-19 Pandemic. J. Surg. Educ. 2021, 78, 346–350. [Google Scholar] [CrossRef] [PubMed]
- Dow, N.; Wass, V.; Macleod, D.; Muirhead, L.; McKeown, J. ‘GP Live’-recorded General Practice consultations as a learning tool for junior medical students faced with the COVID-19 pandemic restrictions. Educ. Prim. Care 2020, 31, 377–381. [Google Scholar] [CrossRef]
- Kidess, M.; Schmid, S.C.; Pollak, S.; Gschwend, J.E.; Berberat, P.O.; Autenrieth, M.E. Virtual skills-training in urology: Teaching at the Technical University of Munich during the COVID-19-pandemic. Urologe 2021, 60, 484–490. [Google Scholar] [CrossRef]
- Knie, K.; Schwarz, L.; Frehle, C.; Schulte, H.; Taetz-Harrer, A.; Kiessling, C. To zoom or not to zoom—the training of communicative competencies in times of COVID 19 at Witten/Herdecke University illustrated by the example of “sharing information”. GMS J. Med. Educ. 2020, 37, Doc83. [Google Scholar] [CrossRef]
- Koelkebeck, K.; Baessler, F.; Bittner, R.; Frodl, T.; Gradl-Dietsch, G.; Janowitz, D.; Jordan, K.D.; Kluge, I.; Matthes, O.; Pinilla, S.; et al. Medical education in psychosocial disciplines in times of the COVID-19 pandemic-first experiences. Fortschr. Neurol. Psychiatr. 2021, 89, 573–577. [Google Scholar] [CrossRef]
- Lateef, F.; Suppiah, M.; Chandra, S.; Yi, T.X.; Darmawan, W.; Peckler, B.; Tucci, V.; Tirado, A.; Mendez, L.; Moreno, L.; et al. Simulation Centers and Simulation-Based Education during the Time of COVID 19: A Multi-Center Best Practice Position Paper by the World Academic Council of Emergency Medicine. J. Emerg. Trauma Shock 2021, 14, 3–13. [Google Scholar] [CrossRef]
- Lenes, A.; Klasen, M.; Adelt, A.; Göretz, U.; Proch-Trodler, C.; Schenkat, H.; Sopka, S. Crisis as a chance. A digital training of social competencies with simulated persons at the Medical Faculty of RWTH Aachen, due to the lack of attendance teaching in the SARS-Cov-2 pandemic. GMS J. Med. Educ. 2020, 37, Doc82. [Google Scholar] [CrossRef]
- Motte-Signoret, E.; Labbé, A.; Benoist, G.; Linglart, A.; Gajdos, V.; Lapillonne, A. Perception of medical education by learners and teachers during the COVID-19 pandemic: A cross-sectional survey of online teaching. Med. Educ. Online 2021, 26, 1919042. [Google Scholar] [CrossRef]
- Nourkami-Tutdibi, N.; Hofer, M.; Zemlin, M.; Abdul-Khaliq, H.; Tutdibi, E. TEACHING MUST GO ON: Flexibility and advantages of peer assisted learning during the COVID-19 pandemic for undergraduate medical ultrasound education—perspective from the “sonoBYstudents” ultrasound group. GMS J. Med. Educ. 2021, 38, Doc5. [Google Scholar] [CrossRef]
- Röhle, A.; Horneff, H.; Willemer, M.C. Practical teaching in undergraduate human and dental medical training during the COVID-19 crisis. Report on the COVID-19-related transformation of peer-based teaching in the Skills Lab using an Inverted Classroom Model. GMS J. Med. Educ. 2021, 38, Doc2. [Google Scholar] [CrossRef]
- Rüllmann, N.; Lee, U.; Klein, K.; Malzkorn, B.; Mayatepek, E.; Schneider, M.; Döing, C. Virtual auscultation course for medical students via video chat in times of COVID-19. GMS J. Med. Educ. 2020, 37, Doc102. [Google Scholar] [CrossRef]
- Ruthberg, J.S.; Quereshy, H.A.; Ahmadmehrabi, S.; Trudeau, S.; Chaudry, E.; Hair, B.; Kominsky, A.; Otteson, T.D.; Bryson, P.C.; Mowry, S.E. A Multimodal Multi-institutional Solution to Remote Medical Student Education for Otolaryngology during COVID-19. Otolaryngol. Head Neck Surg. 2020, 163, 707–709. [Google Scholar] [CrossRef]
- Schleicher, I.; Davids, L.; Latta, N.; Kreiß, A.F.; Kreuder, J. Training of physical examination techniques in video conferences. GMS J. Med. Educ. 2021, 38, Doc6. [Google Scholar] [CrossRef]
- Steehler, A.J.; Pettitt-Schieber, B.; Studer, M.B.; Mahendran, G.; Pettitt, B.J.; Henriquez, O.A. Implementation and Evaluation of a Virtual Elective in Otolaryngology in the Time of COVID-19. Otolaryngol. Head Neck Surg. 2021, 164, 556–561. [Google Scholar] [CrossRef]
- Von Lengerke, T.; Afshar, K.; Just, I.; Lange, K. Classroom teaching with simulated patients during COVID-19: The communication skills course in the second year of the model medical curriculum HannibaL. GMS J. Med. Educ. 2020, 37, Doc81. [Google Scholar] [CrossRef]
- Wallace, D.; Sturrock, A.; Gishen, F. ‘You’ve got mail!’: Clinical and practical skills teaching re-imagined during COVID-19. Future Healthc. J. 2021, 8, e50–e53. [Google Scholar] [CrossRef]
- Wickemeyer, J.L.; Yu, J. A Model for Undergraduate Medical Student Education in Otolaryngology During the Post-COVID-19 Era. Otolaryngol. Head Neck Surg. 2021, 164, 562–565. [Google Scholar] [CrossRef]
- Wiedenmann, C.; Wacker, K.; Böhringer, D.; Maier, P.; Reinhard, T. Online examination course instead of classroom teaching: Adaptation of medical student teaching during the COVID-19 pandemic. Ophthalmologe 2021, 119, 11–18. [Google Scholar] [CrossRef]
- Polk, M.L.; Lailach, S.; Kemper, M.; Bendas, A.; Zahnert, T.; Neudert, M. Lernkurve der HNO-Spiegeluntersuchung. HNO 2020, 68, 238–247. [Google Scholar] [CrossRef]
- Sharaf, K.; Felicio-Briegel, A.; Widmann, M.; Huber, J.; Eggersmann, T.K.; Stadlberger, U.; Schrötzlmair, F.; Canis, M.; Lechner, A. ToSkORL: Self-and objective assessment of examination skills in the head and neck region. HNO 2021, 70, 295–303. [Google Scholar] [CrossRef]
- Binks, A.P.; LeClair, R.J.; Willey, J.M.; Brenner, J.M.; Pickering, J.D.; Moore, J.S.; Huggett, K.N.; Everling, K.M.; Arnott, J.A.; Croniger, C.M.; et al. Changing Medical Education, Overnight: The Curricular Response to COVID-19 of Nine Medical Schools. Teach. Learn. Med. 2021, 33, 334–342. [Google Scholar] [CrossRef]
- Bock, A.; Kniha, K.; Goloborodko, E.; Lemos, M.; Rittich, A.B.; Möhlhenrich, S.C.; Rafai, N.; Hölzle, F.; Modabber, A. Effectiveness of face-to-face, blended and e-learning in teaching the application of local anaesthesia: A randomised study. BMC Med. Educ. 2021, 21, 137. [Google Scholar] [CrossRef]
- Bolatov, A.K.; Gabbasova, A.M.; Baikanova, R.K.; Igenbayeva, B.B.; Pavalkis, D. Online or Blended Learning: The COVID-19 Pandemic and First-Year Medical Students’ Academic Motivation. Med. Sci. Educ. 2021, 32, 221–228. [Google Scholar] [CrossRef]
- Bornkamm, K.; Koch, C.; Dietterle, J.; Steiert, M.; Fleig, A.; Weiller, C.; Brich, J. Teaching the Neurologic Examination: A Prospective Controlled Study to Compare a Blended Learning Approach With Face-to-Face Instruction. Neurology 2021, 97, e2032–e2038. [Google Scholar] [CrossRef]
- Hanke, L.I.; Wachter, N.; Boedecker, C.; Penzkofer, L.; Koch, M.; Dietz, S.O.; König, T.T.; Heinemann, M.K.; Neulen, A.; Kurz, S.; et al. Surgical Education of Medical Students in Times of COVID-19—Necessary Adjustments are Chances for the Future. Zent. Chir. 2021, 146, 586–596. [Google Scholar] [CrossRef]
- Jawaid, M.; Baig, L.; Aly, S.M. Comparison of OSCE scores of surgical clinical education after face-to-face vs. blended learning methods among undergraduate medical students. J. Pak. Med. Assoc. 2021, 71, 1535–1539. [Google Scholar] [CrossRef]
- Tiedemann, E.; Simmenroth, A. Teaching alcohol and smoking counselling in times of COVID-19 to 6(th)-semester medical students: Experiences with a digital-only and a blended learning teaching approach using role-play and feedback. GMS J. Med. Educ. 2021, 38, Doc117. [Google Scholar] [CrossRef]
- Krauss, F.; Giesler, M.; Offergeld, C. On the effectiveness of digital teaching of practical skills in curricular ENT education. HNO 2021, 70, 287–294. [Google Scholar] [CrossRef]
- Blanch-Hartigan, D. Medical students’ self-assessment of performance: Results from three meta-analyses. Patient Educ. Couns. 2011, 84, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Hodges, B.; Regehr, G.; Martin, D. Difficulties in recognizing one’s own incompetence: Novice physicians who are unskilled and unaware of it. Acad. Med. 2001, 76, S87–S89. [Google Scholar] [CrossRef] [PubMed]
- Ochsmann, E.B.; Zier, U.; Drexler, H.; Schmid, K. Well prepared for work? Junior doctors’ self-assessment after medical education. BMC Med. Educ. 2011, 11, 99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tokuda, Y.; Goto, E.; Otaki, J.; Jacobs, J.; Omata, F.; Obara, H.; Shapiro, M.; Soejima, K.; Ishida, Y.; Ohde, S.; et al. Undergraduate educational environment, perceived preparedness for postgraduate clinical training, and pass rate on the National Medical Licensure Examination in Japan. BMC Med. Educ. 2010, 10, 35. [Google Scholar] [CrossRef] [Green Version]
- Rosvall, B.R.; Singer, Z.; Fung, K.; Chin, C.J. Do Medical Students Receive Adequate Otolaryngology Training? A Canadian Perspective. Ann. Otol. Rhinol. Laryngol. 2020, 129, 1095–1100. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Chapter | Basic Course | Advanced Course |
|---|---|---|
| Otology | Key skill: Examination of the ear using an otoscope Supplementary skills: Subjective audiometry using a tune fork (Weber and Rinne testing) | Key skill: Examination of the ear using an ear microscope Supplementary skills: Ear wax/foreign body removal; subjective and objective audiometry |
| Rhinology | Key skill: Anterior rhinoscopy using a nasal speculum Supplementary skills: bipolar coagulation of nosebleed | Key skill: Endoscopy of the nose and sinuses Supplementary skills: percussion of the sinuses and cranial nerve testing |
| Laryngology/Stomatology | Key skill: Examination of oral cavity and oropharynx using spatula Supplementary skills: Examination of the salivary glands | Key skill: Examination of hypopharynx and larynx using 70° endoscopes Supplementary skills: Transnasal flexible laryngoscopy |
| Head and Neck | Key skill: Examination of the cervical lymph nodes and swellings Supplementary skills: Examination of the thyroid gland | Key skill: Trauma examination of the head and neck Supplementary skills: Examination of different cranial nerves |
| Occupational interest | Introduction into the history of Otorhinolaryngology | Educational aspects to become and occupational profile of an Otorhinolaryngologist |
| Online-Only Teaching | In-Classroom Teaching | ||
|---|---|---|---|
| Number of students | n = 31 | n = 91 | |
| Age 1 | 25 ± 3.1 years | 26 ± 4.1 years | |
| Gender 2 | Female | 23 (74.2%) | 46 (50.5%) |
| Male | 8 (25.8%) | 44 (48.4%) | |
| n.a. | 0 (0.0%) | 1 (1.1%) | |
| Semester 1 | 8.9 ± 0.7 | 8.9 ± 0.6 | |
| Interest in ENT (1 = very high to 5 = very low) 3 | 2.55 ± 0.85 | 2.92 ± 0.88 | |
| Self-assessment of general physical examination skills (1 = high proficiency to 5 = low proficiency) 1 | 2.13 ± 0.76 | 2.13 ± 0.88 | |
| Timepoint of online course completion | 1–3 days prior to exam | 13 (41.9%) | |
| 4–7 days prior to exam | 6 (19.4%) | ||
| >7 days prior to exam | 11 (35.5%) | ||
| n.a. | 1 (3.2%) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lechner, A.; Haider, S.P.; Paul, B.; Escrihuela Branz, P.F.F.; Felicio-Briegel, A.; Widmann, M.; Huber, J.; Stadlberger, U.; Canis, M.; Schrötzlmair, F.; et al. Misjudgment of Skills in Clinical Examination Increases in Medical Students Due to a Shift to Exclusively Online Studies during the COVID-19 Pandemic. J. Pers. Med. 2022, 12, 781. https://doi.org/10.3390/jpm12050781
Lechner A, Haider SP, Paul B, Escrihuela Branz PFF, Felicio-Briegel A, Widmann M, Huber J, Stadlberger U, Canis M, Schrötzlmair F, et al. Misjudgment of Skills in Clinical Examination Increases in Medical Students Due to a Shift to Exclusively Online Studies during the COVID-19 Pandemic. Journal of Personalized Medicine. 2022; 12(5):781. https://doi.org/10.3390/jpm12050781
Chicago/Turabian StyleLechner, Axel, Stefan P. Haider, Benedikt Paul, Pablo F. F. Escrihuela Branz, Axelle Felicio-Briegel, Magdalena Widmann, Johanna Huber, Ursula Stadlberger, Martin Canis, Florian Schrötzlmair, and et al. 2022. "Misjudgment of Skills in Clinical Examination Increases in Medical Students Due to a Shift to Exclusively Online Studies during the COVID-19 Pandemic" Journal of Personalized Medicine 12, no. 5: 781. https://doi.org/10.3390/jpm12050781