
Detection of Intraocular Hypertension during Opportunity Screening (Check-Up Medical Inspections)

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical and Legal Issues
2.2. Data Collection
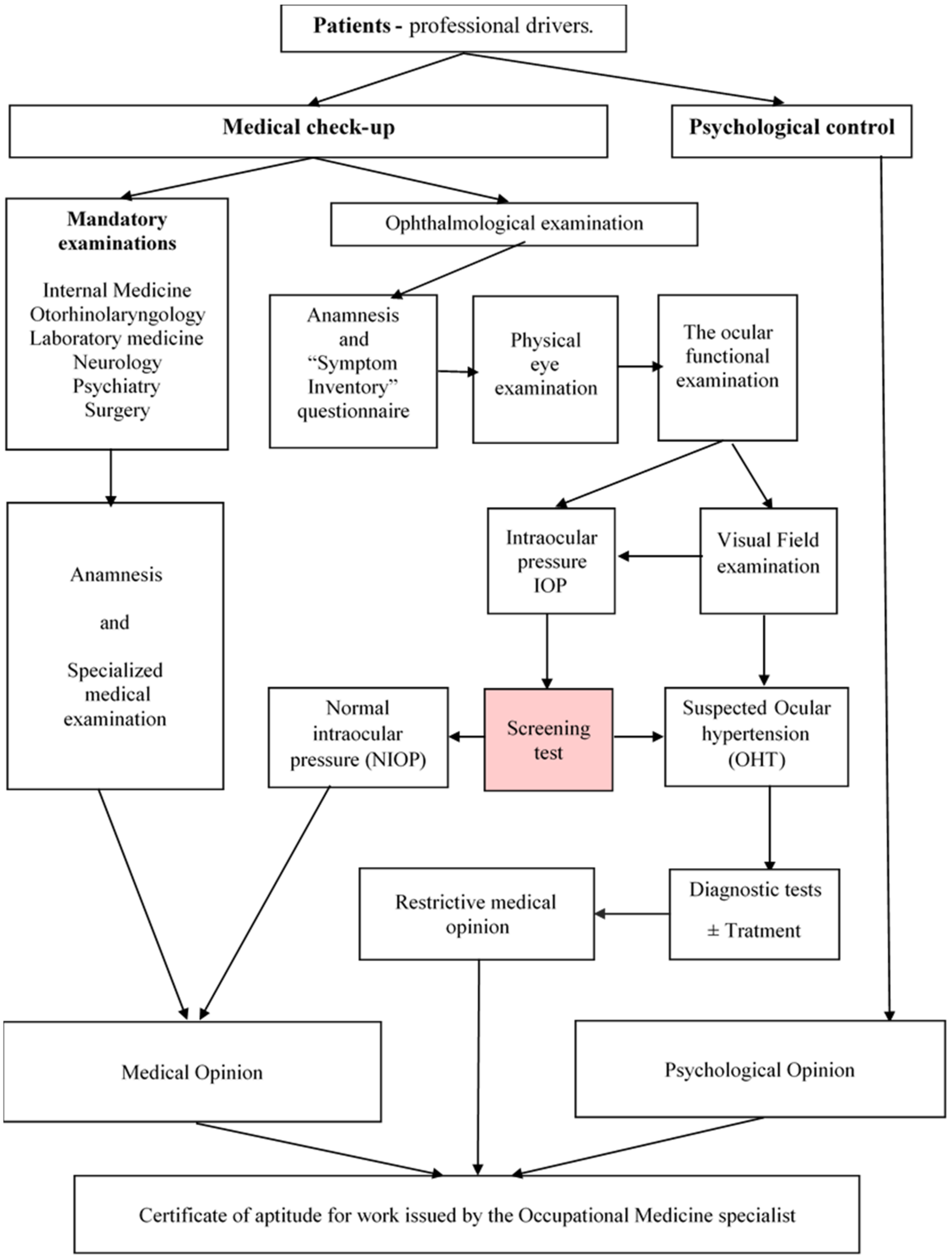
2.3. Study Design
2.4. Methodology
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Yanoff, M. Treatise on Ophthalmology, [ro. Tratat de oftalmologie], 5th ed.; Publishing House Prior: Bucharest, Romania, 2020; Volume 2, p. 1055. [Google Scholar]
- Dumitrache, M.; Filip, M.; Filip, A. Treatise on Ophthalmology; [ro. Tratat de oftalmologie]; Universitara Carol Davila: Bucharest, Romania, 2013; pp. 158–194. [Google Scholar]
- Bocșan, I.S. Practical Epidemiology for Family Physicians; [ro. Epidemiologie practică pentru medicii de familie]; Medicală Universitară Iuliu Hațieganu: Cluj Napoca, Romania, 1999; p. 107. [Google Scholar]
- Bocșan, I.S.; Rădulescu, A. Basic Knowledge for Public Health Managers; [ro. Cunoștințe fundamentale pentru manageri în sănătate publică]; Alma-Mater: Cluj Napoca, Romania, 2002; Volume 1, pp. 109–110. [Google Scholar]
- Enachescu, D.; Marcu, G.M. Public Health and Health Management; [ro. Sănătate publică și management sanitar]; ALL: Bucharest, Romania, 1994; pp. 78–143. [Google Scholar]
- Minister’s Order, no. 1257/1391/2013, Official Gazette, Part I no. 745 of 02/12/2013. Available online: http://www.monitoruljuridic.ro/an/2021/ (accessed on 10 February 2019).
- Annex no. 3. Order of the Minister of Transport no. 1.151/2021/Order of the Minister of Health no.1.752/2021, Chapter II, Methods Used for Medical Examination of Personnel with Responsibilities in Transport Safety and Minimum Equipment for Compulsory Medical Specialties, 3. Ophthalmology. Available online: https://mt.ro/web14/domenii-gestionate/medical/medical-reglementari (accessed on 17 February 2021).
- Speechley, M.; Kunnilathu, A.; Aluckal, E.; Balakrishna, M.S.; Mathew, B.; George, E.K. Screening in Public Health and Clinical Care: Similarities and Differences in Definitions, Types, and Aims—A Systematic Review. J. Clin. Diagn. Res. 2017, 11, LE01–LE04. [Google Scholar] [CrossRef] [PubMed]
- Chiseliță, D. Primitive Open-Angle Glaucoma, Critical Thoughts and Syntheses; [ro. Sănătate publică și management sanitar]; Cermi: Iași, Romania, 2020; Volume 2, pp. 9–10. [Google Scholar]
- Vistamehr, S.; Shelsta, H.N.; Palmisano, P.C.; Filardo, G.; Bashford, K.; Chaudhri, K.; Forster, S.H.; Shafranov, G.; Bruce Shields, M. Glaucoma screening in a high-risk population. J. Glaucoma 2006, 15, 534–540. [Google Scholar] [CrossRef] [PubMed]
- Yamada, M.; Hiratsuka, Y.; Nakano, T.; Kita, Y.; Watanabe, T.; Tamura, H.; Kawasaki, R.; Yokoyama, T.; Takano, S. Detection of Glaucoma and Other Vision-Threatening Ocular Diseases in the Population Recruited at Specific Health Checkups in Japan. Clin. Epidemiol. 2020, 12, 1381–1388. [Google Scholar] [CrossRef] [PubMed]
- Minister’s Order no. 1.151/2021. Health Minister’s Order no. nr.1.752/2021. Available online: https://lege5.ro/Gratuit/ha4dcmrwge3a/ordinul-nr-1151-1752-2021-pentru-aprobarea-cadrului-general-privind-examinarea-medicala-si-psihologica-a-personalului-cu-atributii-in-siguranta-transporturilor (accessed on 12 March 2021).
- Annex no. 3. 4.2., Minister’s Order no. 1.151/2021. Health Minister’s Order no. 1.752/2021. Available online: https://legislatie.just.ro/Public/DetaliiDocumentAfis/246042 (accessed on 12 March 2021).
- Health Minister’s Order no. 1390/2013. Available online: http://mt.ro/web14/domenii-gestionate/medical/medical-reglementari (accessed on 9 February 2021).
- Optopol Technology, User‘s Manual Automated Perimeter PTS 910 Series. Available online: https://docplayer.net/42059342-Automated-perimeter-pts-910-910-by.html (accessed on 24 January 2021).
- Brusini, P.; Johnson, C.A. Staging functional damage in glaucoma: Review of Different Classification Methods. Surv. Ophthalmol. 2007, 52, 156–179. [Google Scholar] [CrossRef]
- Romanian Government Decision no. 355/2007, Regarding the Surveillance of the Workers’ Health, Published in: Official Gazette, Bucharest, Romania, 2007. Available online: https://www.ilo.org/wcmsp5/groups/public/@ed_protect/@protrav/@safework/documents/normativeinstrument/wcms_177384.pdf (accessed on 22 January 2021).
- Popa, M. Multivariate Statistics Applied in Psychology; [ro. Statistici multivariate aplicate în psihologie]; Polirom: Iași, Romania, 2010; pp. 89–121. [Google Scholar]
- Jaba, E.; Grama, A. Statistical Analysis with SPSS under Windows; Polirom: Bucharest, Romania, 2004; pp. 202–243. [Google Scholar]
- Achimaș-Cadariu, A. Methodology of Medical Scientific Research; Iuliu Hațieganu University Publishing House: Cluj Napoca, Romania, 2000; pp. 44–46. [Google Scholar]
- Grzybowski, A.; Mianowany, M. Statistics in ophthalmology revisited: The (effect) size matters. Acta Ophthalmol. 2018, 96, e885–e888. [Google Scholar] [CrossRef] [Green Version]
- Popovic, M.M.; Schlenker, M.B. Analysis of Comparative Clinical Data in Ophthalmology: An Approach. Curr. Eye Res. 2021, 46, 1449–1451. [Google Scholar] [CrossRef]
- Martens, J.B. Comparing experimental conditions using modern statistics. Behav. Res. Methods. 2021, 53, 1240–1261. [Google Scholar] [CrossRef]
- European Glaucoma Society. Guidelines—European Glaucoma Society. Paris, France, 2021, 97. Available online: https://www.eugs.org (accessed on 16 January 2022).
- Kang, J.M.; Tanna, A.P. Glaucoma. Med. Clin. North Am. 2021, 105, 493–510. [Google Scholar] [CrossRef]
- Mincă, D.G.; Marcu, M.G. Sănătate Publică și Management Sanitar, Note de Curs pentru Invățământul Postuniversitar, 2nd ed.; Editura Universitară Carol Davila: Bucharest, Romania, 2005; p. 2. [Google Scholar]
- Boey, P.Y.; Mansberger, S.L. Ocular hypertension: An approach to assessment and management. Can. J. Ophthalmol. 2014, 49, 489–496. [Google Scholar] [CrossRef]
- Hoffmann, E.M.; Lamparter, J. Abgrenzung der okulären Hypertension. [Differentiation of ocular hypertension]. Ophthalmologe 2016, 113, 715–728. [Google Scholar] [CrossRef]
- Abitbol, O. Dépistage et prévention des glaucomes. [Glaucoma screening and prevention]. Rev. Prat. 2016, 66, 496–498. [Google Scholar]
- Schuster, A.K.; Wagner, F.M.; Pfeiffer, N.; Hoffmann, E.M. Risk factors for open-angle glaucoma and recommendations for glaucoma screening. Ophthalmologe 2021, 118, 145–152. [Google Scholar] [CrossRef]
- Jonas, J.B.; Aung, T.; Bourne, R.R.; Bron, A.M.; Ritch, R.; Panda-Jonas, S. Glaucoma. Lancet 2017, 390, 2183–2193. [Google Scholar] [CrossRef]
- Jaén Díaz, J.; Sanz Alcolea, I.; López De Castro, F.; Pérez Martínez, T.; Ortega Campos, P.; Corral Morales, R. Glaucoma e hipertensión ocular en atención primaria [Glaucoma and ocular hypertension in primary care]. Atención Primaria 2001, 28, 23–30. [Google Scholar] [CrossRef] [Green Version]
- Friedman, D.S. Issues in screening for glaucoma. Ophthalmic Epidemiol. 2007, 14, 101–102. [Google Scholar] [CrossRef]
- Zhao, D.; Guallar, E.; Gajwani, P.; Swenor, B.; Crews, J.; Saaddine, J.; Mudie, L.; Varadaraj, V.; Friedman, D.S. SToP Glaucoma Study Group. Optimizing Glaucoma Screening in High-Risk Population: Design and 1-Year Findings of the Screening to Prevent (SToP) Glaucoma Study. Am. J. Ophthalmol. 2017, 180, 18–28. [Google Scholar] [CrossRef]
- Glaucoma World Week. Available online: https://societateadeglaucom.ro/manifestari/saptamana-mondiala-a-glaucomului/ (accessed on 23 January 2022).
- Wu, Z.; Medeiros, F.A. Recent developments in visual field testing for glaucoma. Curr. Opin. Ophthalmol. 2018, 29, 141–146. [Google Scholar] [CrossRef]
- Munteanu, G.Z.; Munteanu, Z.V.I.; Roiu, G.; Daina, C.M.; Moraru, R.; Moraru, L.; Trambitas, C.; Badau, D.; Daina, L.G. Aspects of Tertiary Prevention in Patients with Primary Open Angle Glaucoma. J. Pers. Med. 2021, 11, 830. [Google Scholar] [CrossRef]
- Gordon, M.O.; Kass, M.A. The Ocular Hypertension Treatment Study: Design and baseline description of the participants. Arch. Ophthalmol. 1999, 117, 573–583. [Google Scholar] [CrossRef] [Green Version]
- Tchabi-Hounnou, S.; Agbahoungba, L.; Sounouvou, I.; Yèhouessi, L.; Alamou, S.; Doutetien, C.; Bassabi, S.K. Hypertonie oculaire et glaucome primitif à angle ouvert [High intraocular pressure and open angle glaucoma]. J. Fr. Ophtalmol. 2012, 35, 523–528. [Google Scholar] [CrossRef]
- Komori, S.; Ishida, K.; Yamamoto, T. Results of long-term monitoring of normal-tension glaucoma patients receiving medical therapy: Results of an 18-year follow-up. Graefe’s Arch. Clin. Exp. Ophthalmol. 2014, 252, 1963–1970. [Google Scholar] [CrossRef]
- De Moraes, C.G.; Liebmann, J.M.; Levin, L.A. Detection and measurement of clinically meaningful visual field progression in clinical trials for glaucoma. Prog. Retin. Eye Res. 2017, 56, 107–147. [Google Scholar] [CrossRef] [Green Version]
- Rossetti, L.; Goni, F.; Denis, P.; Bengtsson, B.; Martinez, A.; Heijl, A. Focusing on glaucoma progression and the clinical importance of progression rate measurement: A review. Eye 2010, 24, S1–S7. [Google Scholar] [CrossRef]
- Capilna, M.E.; Szabo, B.; Rusu, S.C.; Becsi, J.; Moldovan, B.; Neagoe, R.M.; Muhlfay, G. Anatomical variations of the obturator veins and their surgical implications. Eur. J. Gynaecol. Oncol. 2017, 38, 263–265. [Google Scholar]
- Muhlfay, G.; Fabian, Z.; Neagoe, R.M.; Horvath, K.U. Applications of 3D Planning, Plastic Materials and Additive Manufacturing in Functional Rehabilitations in the Head and Neck Surgery. Mater. Plast. 2018, 55, 431–433. [Google Scholar] [CrossRef]
- Neagoe, R.M.; Sala, D.; Voidazan, S.; Bancu, S.; Kiss, L.; Suciu, H. Transthoracic versus Transhiatal esophagectomy: A Permanent Dilemma. Our 15-Year Experience. Chirurgia 2013, 108, 780–787. [Google Scholar]
- Ministry of Transport and Infrastructure. Approved Medical/Psychological Units and Authorized Psychological Units. Available online: http://mt.ro/web14/domenii-gestionate/medical/medical-anunturi (accessed on 25 April 2022).


{kind=link}
| Bebie Curve Type I | Extensive and Deep Damage to the “Visual Field” |
|---|---|
| Bebie Curve type II | No real defects in the “Field of View”–happy trigger |
| Bebie Curve type III | Small but deep defects of “Visual Field” |
| Bebie Curve type IV | A “Visual Field” with a very large and shallow defect |
| Bebie Curve type V | A “Visual Field-Almost Normal” |
| Parameters | Results | ||||||
|---|---|---|---|---|---|---|---|
| Patients Suspected of Having OHT | Patients with Normal IOP | Total Patients | |||||
| n | % | n | % | n | % | ||
| Number of Cases | 71 | 749 | 820 | 100 | |||
| Sex | Male | 64 | 90.14 | 690 | 92.12 | 754 | 91.95 |
| Female | 7 | 9.86 | 59 | 7.88 | 66 | 8.05 | |
| Age | 43.27 ±9.92 | min = 18 max = 62 | 39.60 ±10.90 | min = 18 max = 64 | 39.92 ±10.86 | min = 18 max = 64 | |
| Residence | Urban area | 50 | 70.42 | 623 | 83.18 | 673 | 82.07 |
| Rural area | 21 | 29.58 | 126 | 16.82 | 147 | 17.93 | |
| Marital status | Married | 43 | 60.56 | 513 | 68.49 | 556 | 67.80 |
| Un-married | 21 | 29.58 | 153 | 20.43 | 174 | 21.22 | |
| Widow | 1 | 1.41 | 34 | 4.54 | 35 | 4.27 | |
| Divorced | 6 | 8.45 | 49 | 6.54 | 55 | 6.71 | |
| Studies | Primary Cycle | 4 | 5.63 | 28 | 3.74 | 32 | 3.90 |
| Gymnasium cycle | 3 | 4.23 | 52 | 6.94 | 55 | 6.71 | |
| Professional school | 10 | 14.08 | 132 | 17.62 | 142 | 17.32 | |
| High school | 26 | 36.62 | 307 | 40.99 | 333 | 40.61 | |
| Post High school | 3 | 4.23 | 111 | 14.82 | 114 | 13.90 | |
| Higher education | 20 | 28.17 | 76 | 10.15 | 96 | 11.71 | |
| Post -university | 5 | 7.04 | 43 | 5.74 | 48 | 5.85 | |
| Activity status | Professional driver | 65 | 91.55 | 634 | 84.65 | 699 | 85.25 |
| Driving instructor | 5 | 7.04 | 36 | 4.81 | 41 | 5.00 | |
| Transport manager | 0 | 0.00 | 78 | 10.41 | 78 | 9.51 | |
| Retired car instructor | 1 | 1.41 | 1 | 0.13 | 2 | 0.24 | |
| Parameters | Initial Consultation | Final Consultation | z | p * |
|---|---|---|---|---|
| IOP-Re | 25.36 ± 3.21 | 21.46 ± 3.78 | −3.432 b | 0.001 |
| IOP-Le | 25.52 ± 3.81 | 20.25 ± 3.29 | −3.622 b | 0.000 |
| IOP–Re + Le | 25.44 ± 3.04 | 20.88 ± 3.15 | −3.621 b | 0.000 |
| Credibility Indices | Patients Suspected of Having OHT | Patients with IOP within Normal Limits (NIOP) | z | p * |
|---|---|---|---|---|
| Average duration (minutes) Re | 6.64 ± 1.49 | 7.12 ± 8.01 | −0.906 | 0.365 |
| Average duration (minutes) Le | 6.47 ± 1.15 | 6.75 ± 1.42 | −1.315 | 0.189 |
| Average duration (minutes) Re + Le | 6.56 ± 1.18 | 6.93 ± 4.10 | −1.554 | 0.120 |
| False positive-Re | 3.59 ± 7.39 | 4.15 ± 6.53 | −1.125 | 0.260 |
| False positive-Le | 4.52 ± 8.55 | 4.00 ± 6.12 | −0.163 | 0.871 |
| False positive-Re + Le | 4.05 ± 6.92 | 4.07 ± 4.82 | −0.952 | 0.341 |
| False negative-Re | 7.23 ± 10.25 | 4.93 ± 7.01 | −1.348 | 0.178 |
| False negative-Le | 6.03 ± 8.17 | 4.49 ± 6.96 | −1.395 | 0.163 |
| False negative-Re + Le | 6.62 ± 7.21 | 4.70 ± 5.25 | −1.670 | 0.095 |
| Parameters | Patients Suspected of Having OHT | Patients with IOP within Normal Limits (NIOP) | z | p * |
|---|---|---|---|---|
| Tested points-Re + Le | 295.01 ± 40.56 | 295.09 ± 40.54 | −0.193 | 0.847 |
| Visual slope at 10°-Re + Le | 2.91 ± 0.71 | 2.87 ± 0.82 | −0.367 | 0.714 |
| Calculated HOV-Re + Le | 24.16 ± 2.47 | 24.93 ± 2.34 | −2.460 | 0.014 |
| PD (Pattern defect)-Re + Le | 0.46 ± 0.60 | 0.34 ± 0.38 | −1396 | 0.163 |
| AD (Average defect)-Re + Le | −0.19 ± 0.9 | −0.02 ± 0.18 | −3.221 | 0.001 |
| Bebie Curve Modes | Suspected OHT Patients | NIOP Patients | ||||||
|---|---|---|---|---|---|---|---|---|
| Re | Le | Re | Le | |||||
| n | % | n | % | n | % | n | % | |
| Bebie Curve type I | 2 | 2.8 | 3 | 4.2 | 0 | 0.0 | 3 | 0.4 |
| Bebie Curve type II | 2 | 2.8 | 3 | 4.2 | 1 | 0.1 | 4 | 0.5 |
| Bebie Curve type III | 56 | 78.9 | 52 | 73.2 | 576 | 76.9 | 570 | 76.1 |
| Bebie Curve type IV | 2 | 2.8 | 3 | 4.2 | 9 | 1.2 | 9 | 1.2 |
| Bebie Curve type V | 9 | 12.7 | 10 | 14.2 | 163 | 21.8 | 163 | 21.8 |
| Total | 71 | 100 | 71 | 100 | 749 | 100 | 749 | 100 |
| Correlations | Corelated Variables | Suspected OHT Patients Correlations | NIOP Patients Correlations | ||
|---|---|---|---|---|---|
| Spearman′s rho | Sig. 2-tailed | Spearman′s rho | Sig. 2-tailed | ||
| Pozitive correlation coefficients between VF parameters in OHT suspects and NIOP pacients | Average test duration-Average of the tested points | 0.824 ** | 0.000 | 0.782 ** | 0.000 |
| Average Slope at 10°-False Negative Average | 0.446 ** | 0.000 | - | - | |
| Average test duration-PD Average | 0.429 ** | 0.000 | 0.261 ** | 0.000 | |
| AD Average-False Positive Average | 0.387 ** | 0.001 | 0.094 ** | 0.010 | |
| HOV Calculated Average-AD Average | 0.376 ** | 0.001 | 0.466 ** | 0.000 | |
| Average of the tested points-PD Average | 0.367 ** | 0.002 | 0.345 ** | 0.000 | |
| Negative correlation coefficients between VF parameters in NIOP patients | Average test duration-AD Average | - | - | −0.186 ** | 0.000 |
| Average of the tested points-AD Average | - | - | −0.154 ** | 0.000 | |
| PD Average-AD Average | - | - | −0.125 ** | 0.001 | |
| Risk Factor | Parameter Estimate | SE | Wald ꭓ2 | df | Sig | Exp(B) | 95% CI | |
|---|---|---|---|---|---|---|---|---|
| >Lower | >Upper | |||||||
| IOP (1640 eyes) | 1.424 | 0.140 | 102.931 | 1 | 0.000 | 4.154 | 3.155 | 5.469 |
| Sex (male/female) | −0.246 | 0.421 | 0.343 | 1 | 0.558 | 0.782 | 0.343 | 1.783 |
| Age (>40 years/<40 years) | −0.896 | 0.274 | 10.712 | 1 | 0.001 | 0.408 | 0.239 | 0.698 |
| Hereditary history of diabetes | −1.882 | 0.741 | 6.445 | 1 | 0.011 | 0.152 | 0.036 | 0.651 |
| Hereditary history of hypertension | −3.297 | 0.615 | 28.716 | 1 | 0.000 | 0.037 | 0.011 | 0.124 |
| History of diabetes | −2.698 | 0.774 | 12.138 | 1 | 0.000 | 0.067 | 0.015 | 0.307 |
| History of high blood pressure | −4.404 | 1.077 | 16.726 | 1 | 0.000 | 0.012 | 0.001 | 0.101 |
| Tobacco consumption | −1.920 | 0.532 | 13.009 | 1 | 0.000 | 0.147 | 0.052 | 0.416 |
| Alcohol consumption | −2.939 | 0.585 | 25.239 | 1 | 0.000 | 0.053 | 0.017 | 0.167 |
| Drug use | −3.343 | 0.846 | 15.595 | 1 | 0.000 | 0.035 | 0.007 | 0.186 |
| Duration of VF performing | −0.117 | 0.067 | 3.075 | 1 | 0.079 | 0.889 | 0.780 | 1.014 |
| False Positive | −0.004 | 0.014 | 0.085 | 1 | 0.771 | 0.996 | 0.970 | 1.023 |
| False Negative | 0.031 | 0.011 | 8.905 | 1 | 0.003 | 1.032 | 1.011 | 1.053 |
| Tested Points | 0.000 | 0.002 | 0.016 | 1 | 0.899 | 1.000 | 0.996 | 1.004 |
| Slope 10gr | 0.335 | 0.113 | 8.833 | 1 | 0.003 | 1.397 | 1.121 | 1.742 |
| HOV | −0.099 | 0.031 | 10.231 | 1 | 0.001 | 0.906 | 0.853 | 0.962 |
| PD | 0.388 | 0.136 | 8.167 | 1 | 0.004 | 1.475 | 1.130 | 1.925 |
| AD | −1.103 | 0.399 | 7.634 | 1 | 0.006 | 0.332 | 0.152 | 0.726 |
| Symptoms Questioned | Answers “Yes” OHT Patients (71) | Answers “Yes” NIOP Patients (749) | Answers “Yes” Total Patients (820) | |||
|---|---|---|---|---|---|---|
| Number | % | Number | % | Number | % | |
| Tearing | 34 | 28.10 | 15 | 28.31 | 49 | 28.17 |
| Sensation of dry eyes | 12 | 9.92 | 5 | 9.43 | 17 | 9.77 |
| Sensation of tension in the eye-Eye strain | 15 | 12.40 | 2 | 3.77 | 17 | 9.77 |
| Scotomas-the lack of a part of the visual field | 5 | 4.13 | 2 | 3.77 | 7 | 4.02 |
| Limited view: tube/tunnel view | 2 | 1.65 | 1 | 1.89 | 3 | 1.72 |
| Difficulty in short distance sight | 18 | 14.88 | 7 | 13.21 | 25 | 14.37 |
| Difficulty in remote view (to see at a distance) | 4 | 3.31 | 5 | 9.43 | 9 | 5.17 |
| Disorders in color perception changes in color intensity | 4 | 3.31 | 1 | 1.89 | 5 | 2.87 |
| Ebluisare-blindness in bright light | 14 | 11.56 | 9 | 16.98 | 23 | 13.22 |
| Ebluisare-blindness when passing from light to darkness | 13 | 10.74 | 6 | 11.32 | 19 | 10.92 |
| Symptoms Questioned | Parameter Estimate | SE | Wald ꭓ2 | df | Sig | Exp(B) | 95% CI | |
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| Tearing | −2.576 | 0.467 | 30.497 | 1 | 0.000 | 0.076 | 0.030 | 0.190 |
| Sensation of dry eyes | −0.156 | 0.863 | 0.033 | 1 | 0.856 | 0.856 | 0.158 | 4.639 |
| Sensation of tension in the eye-Eye strain | −2.379 | 0.956 | 6.201 | 1 | 0.013 | 0.093 | 0.014 | 0.603 |
| Scotomas | −0.025 | 1.651 | 0.000 | 1 | 0.988 | 0.975 | 0.038 | 24.788 |
| Limited view: tube/tunnel view | −0.666 | 2.304 | 0.084 | 1 | 0.773 | 0.514 | 0.006 | 46.942 |
| Difficulty in short distance sight | −2.407 | 0.624 | 14.869 | 1 | 0.000 | 0.090 | 0.026 | 0.306 |
| Difficulty in remote view (to see at a distance) | 1.120 | 1.663 | 0.454 | 1 | 0.501 | 3.065 | 0.118 | 79.841 |
| Disorders in color perception-in color intensity | −2.131 | 1.821 | 1.369 | 1 | 0.242 | 0.119 | 0.003 | 4.214 |
| Ebluisare-blindness in bright light | −0.798 | 0.696 | 1.315 | 1 | 0.252 | 0.450 | 0.115 | 1.761 |
| Ebluisare-blindness-passing from light to darkness | −0.736 | 0.798 | 0.851 | 1 | 0.356 | 0.479 | 0.100 | 2.287 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Munteanu, G.Z.; Munteanu, Z.V.I.; Roiu, G.; Daina, C.M.; Daina, L.G.; Coroi, M.C.; Domnariu, C.; Neculoiu, D.C.; Cotovanu, A.S.; Badau, D. Detection of Intraocular Hypertension during Opportunity Screening (Check-Up Medical Inspections). J. Pers. Med. 2022, 12, 777. https://doi.org/10.3390/jpm12050777
Munteanu GZ, Munteanu ZVI, Roiu G, Daina CM, Daina LG, Coroi MC, Domnariu C, Neculoiu DC, Cotovanu AS, Badau D. Detection of Intraocular Hypertension during Opportunity Screening (Check-Up Medical Inspections). Journal of Personalized Medicine. 2022; 12(5):777. https://doi.org/10.3390/jpm12050777
Chicago/Turabian StyleMunteanu, Gabriel Zeno, Zeno Virgiliu Ioan Munteanu, George Roiu, Cristian Marius Daina, Lucia Georgeta Daina, Mihaela Cristina Coroi, Carmen Domnariu, Daniela Carmen Neculoiu, Adrian Sebastian Cotovanu, and Dana Badau. 2022. "Detection of Intraocular Hypertension during Opportunity Screening (Check-Up Medical Inspections)" Journal of Personalized Medicine 12, no. 5: 777. https://doi.org/10.3390/jpm12050777