
A High-Precision Deep Learning Algorithm to Localize Idiopathic Ventricular Arrhythmias

 , , ,
, , ,
Abstract
:1. Introduction
- (1)
- This present study has the largest cohort for deep learning to localize idiopathic VAs.
- (2)
- Among the studies trying to solve VAs localization with deep learning or machine learning methods, our study has the largest number of cases for testing.
- (3)
- We are among the first studies to used 2D-CNN for VAs localization.
- (4)
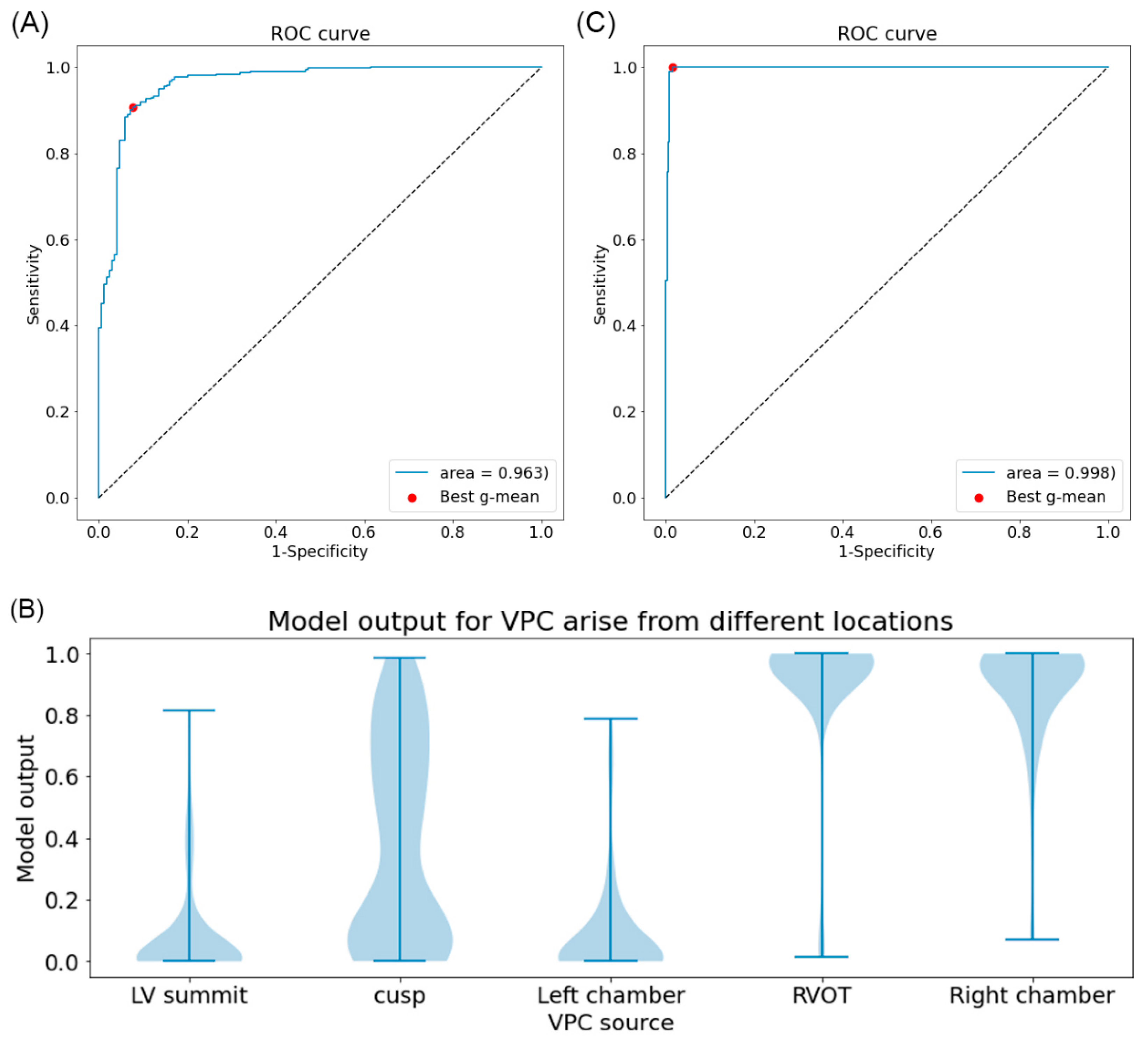
- With violin plot, we can identify that VAs from the cusp area are the main source of errors.
- (5)
- This is the first study for a deep learning algorithm to differentiate VAs from LV summit, with a sensitivity of 100% and a specificity of 98%.
- (6)
- Accurate prediction of VAs from LV summit before the procedure would be helpful for the operator to optimize the whole procedure.
2. Method
2.1. Study Design
2.2. Mapping and Ablation Procedure
2.3. Data Preprocessing
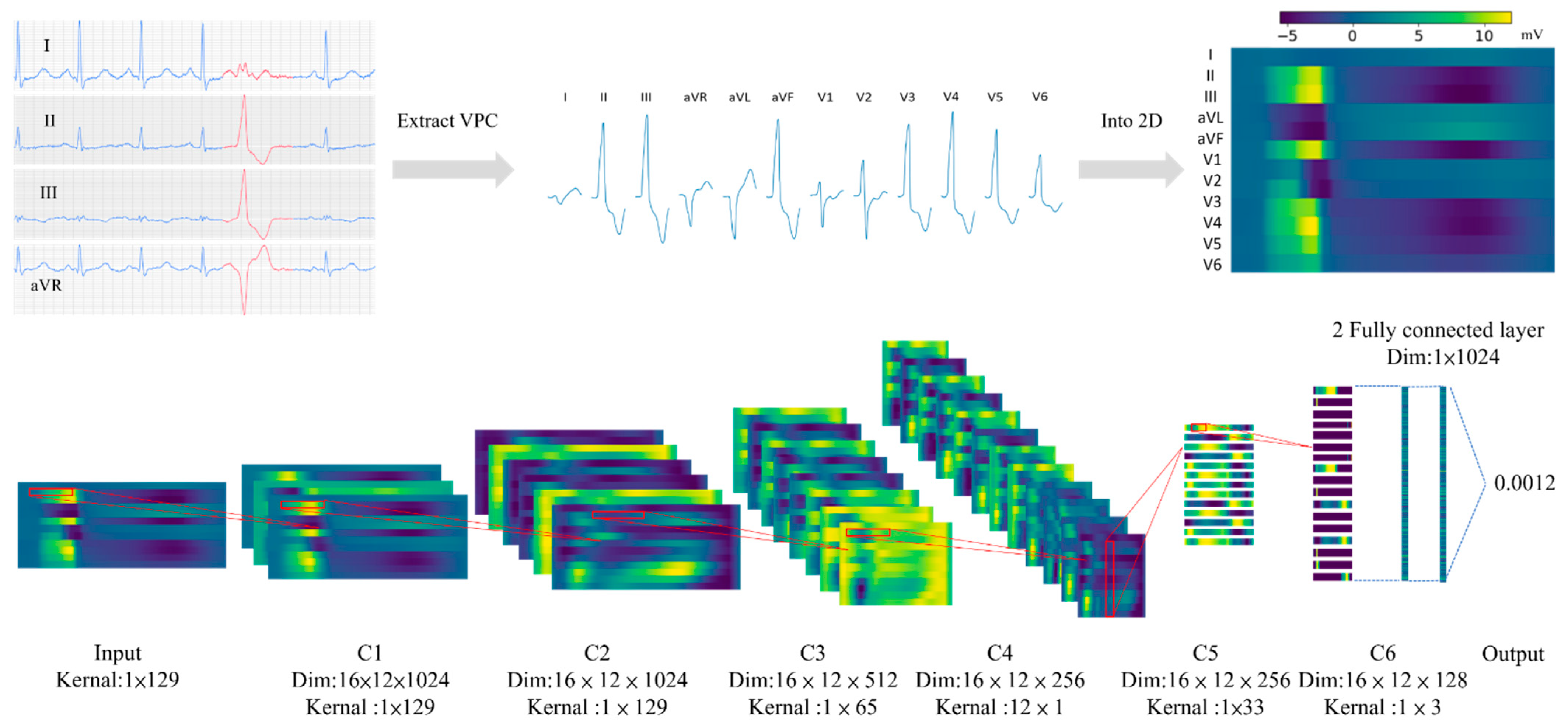
2.4. Input Format and Model Structure
2.5. Data Allocation
2.6. Model Training
2.6.1. For Binary Classifying Right- and Left-Sided VPC Source
2.6.2. For Classifying Summit of Ventricle from Other VPC Sources
2.6.3. Hyperparameter Tuning, Training Policy, and Other Training Methods Used
2.7. Model Evaluation
2.8. Combining Two Models for VPC Site Identification
2.9. Implementation of Model Building, Training, and Model Evaluation
3. Results
3.1. Study Population
3.2. Training and Testing Data Descriptions
3.3. Model Performance for Classifying Right- and Left-Sided VPC Source
3.4. Model Performance for Identifying VPC from LV Summit
3.5. Data Size and Model Performance
3.6. Combining Model for Left-Right Classification and LV Summit Identification
4. Discussion
4.1. Previous Studies of Manual Measurement and Machine Learning in the Localization of Ventricular Arrhythmia
4.2. The Current Study in Comparison with Previous Artificial Intelligence Studies
4.3. Application of Current Findings into Clinical Practice
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dukes, J.W.; Dewland, T.A.; Vittinghoff, E.; Mandyam, M.C.; Heckbert, S.R.; Siscovick, D.S.; Stein, P.K.; Psaty, B.M.; Sotoodehnia, N.; Gottdiener, J.S.; et al. Ventricular Ectopy as a Predictor of Heart Failure. and Death. J. Am. Coll Cardiol. 2015, 66, 101–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cronin, E.M.; Bogun, F.M.; Maury, P.; Peichl, P.; Chen, M.; Namboodiri, N.; Aguinaga, L.; Leite, L.R.; Al-Khatib, S.M.; Anter, E.; et al. 2019 Hrs/Ehra/Aphrs/Lahrs expert consensus statement on catheter ablation of ventricular arrhythmias. Europace 2019, 21, 1143–1144. [Google Scholar] [CrossRef] [PubMed]
- Chung, F.-P.; Lin, C.-Y.; Shirai, Y.; Futyma, P.; Santangeli, P.; Lin, Y.-J.; Chang, S.-L.; Lo, L.-W.; Hu, Y.-F.; Chang, H.-Y.; et al. Outcomes of catheter ablation of ventricular arrhythmia originating from the left ventricular summit: A multicenter study. Heart Rhythm. 2020, 17, 1077–1083. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.D.; Kumar, S.; Parameswaran, R.; Wong, G.; Voskoboinik, A.; Sugumar, H.; Watts, T.; Sparks, P.B.; Morton, J.B.; McLellan, A.; et al. Differentiating Right- and Left-Sided Outflow Tract Ventricular Arrhythmias: Classical ECG Signatures and Prediction Algorithms. Circ. Arrhythm. Electrophysiol. 2019, 12, e007392. [Google Scholar] [CrossRef]
- Enriquez, A.; Baranchuk, A.; Briceno, D.; Saenz, L.; Garcia, F. How to use the 12-lead ECG to predict the site of origin of idiopathic ventricular arrhythmias. Heart Rhythm. 2019, 16, 1538–1544. [Google Scholar] [CrossRef]
- Betensky, B.P.; Park, R.E.; Marchlinski, F.E.; Hutchinson, M.D.; Garcia, F.C.; Dixit, S.; Callans, D.J.; Cooper, J.M.; Bala, R.; Lin, D.; et al. The V(2) transition ratio: A new electrocardiographic criterion for distinguishing left from right ventricular outflow tract tachycardia origin. J. Am. Coll. Cardiol. 2011, 57, 2255–2262. [Google Scholar] [CrossRef] [Green Version]
- Cheng, D.; Ju, W.; Zhu, L.; Chen, K.; Zhang, F.; Chen, H.; Yang, G.; Li, X.; Li, M.; Gu, K.; et al. V3R/V7 Index: A Novel Electrocardiographic Criterion for Differentiating Left From Right Ventricular Outflow Tract Arrhythmias Origins. Circ. Arrhythm. Electrophysiol. 2018, 11, e006243. [Google Scholar] [CrossRef]
- He, Z.; Liu, M.; Yu, M.; Lu, N.; Li, J.; Xu, T.; Zhu, J.; O’Gara, M.C.; O’Meara, M.; Ye, H.; et al. An electrocardiographic diagnostic model for differentiating left from right ventricular outflow tract tachycardia origin. J. Cardiovasc. Electrophysiol. 2018, 29, 908–915. [Google Scholar] [CrossRef]
- Xie, S.; Kubala, M.; Liang, J.J.; Hayashi, T.; Park, J.; Padros, I.L.; Garcia, F.C.; Santangeli, P.; Supple, G.E.; Frankel, D.S.; et al. Lead I R-wave amplitude to differentiate idiopathic ventricular arrhythmias with left bundle branch block right inferior axis originating from the left versus right ventricular outflow tract. J. Cardiovasc. Electrophysiol. 2018, 29, 1515–1522. [Google Scholar] [CrossRef]
- Xia, Y.; Liu, Z.; Liu, J.; Li, X.; Zhang, H.; Fu, L.; Yu, M.; Fang, P. Amplitude of QRS complex within initial 40 ms in V2 (V2QRSi40): Novel electrocardiographic criterion for predicting accurate localization of outflow tract ventricular arrhythmia origin. Heart Rhythm. 2020, 17, 2164–2171. [Google Scholar] [CrossRef]
- Komatsu, Y.; Nogami, A.; Shinoda, Y.; Masuda, K.; Machino, T.; Kuroki, K.; Yamasaki, H.; Sekiguchi, Y.; Aonuma, K. Idiopathic Ventricular Arrhythmias Originating From the Vicinity of the Communicating Vein of Cardiac Venous Systems at the Left Ventricular Summit. Circ. Arrhythm. Electrophysiol. 2018, 11, e005386. [Google Scholar] [CrossRef] [PubMed]
- Liao, H.; Wei, W.; Tanager, K.S.; Miele, F.; Upadhyay, G.A.; Beaser, A.D.; Aziz, Z.; Nayak, H.M.; Ozcan, C.; Nishimura, T.; et al. Left ventricular summit arrhythmias with an abrupt V3 transition: Anatomy of the aortic interleaflet triangle vantage point. Heart Rhythm. 2021, 18, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Gabriels, J.K.; Abdelrahman, M.; Nambiar, L.; Kim, J.; Ip, J.E.; Thomas, G.; Liu, C.F.; Markowitz, S.M.; Lerman, B.B.; Cheung, J.W. Reappraisal of electrocardiographic criteria for localization of idiopathic outflow region ventricular arrhythmias. Heart Rhythm. 2021, 18, 1959–1965. [Google Scholar] [CrossRef] [PubMed]
- Attia, Z.I.; Harmon, D.M.; Behr, E.R.; Friedman, P.A. Application of artificial intelligence to the electrocardiogram. Eur Heart, J. 2021, 42, 4717–4730. [Google Scholar] [CrossRef] [PubMed]
- Hussain, I.; Park, S.J. Big-ECG: Cardiographic Predictive Cyber-Physical System for Stroke Management. IEEE Access. 2021, 9, 123146–123164. [Google Scholar] [CrossRef]
- Hussain, I.; Park, S.J. Quantitative Evaluation of Task-Induced Neurological Outcome after Stroke. Brain Sci. 2021, 11, 900. [Google Scholar] [CrossRef]
- Zheng, J.; Fu, G.; Anderson, K.; Chu, H.; Rakovski, C. A 12-Lead ECG database to identify origins of idiopathic ventricular arrhythmia containing 334 patients. Sci Data. 2020, 7, 98. [Google Scholar] [CrossRef]
- Lin, C.-Y.; Chung, F.-P.; Lin, Y.-J.; Chong, E.; Chang, S.-L.; Lo, L.-W.; Hu, Y.-F.; Tuan, T.-C.; Chao, T.-F.; Liao, J.-N.; et al. Radiofrequency catheter ablation of ventricular arrhythmias originating from the continuum between the aortic sinus of Valsalva and the left ventricular summit: Electrocardiographic characteristics and correlative anatomy. Heart Rhythm. 2016, 13, 111–121. [Google Scholar] [CrossRef] [Green Version]
- Chung, F.-P.; Chong, E.; Lin, Y.-J.; Chang, S.-L.; Lo, L.-W.; Hu, Y.-F.; Tuan, T.-C.; Chao, T.-F.; Liao, J.-N.; Huang, Y.-C.; et al. Different characteristics and electrophysiological properties between early and late recurrences after acute successful catheter ablation of idiopathic right ventricular outflow tract arrhythmias during long-term follow-up. Heart Rhythm. 2014, 11, 1760–1769. [Google Scholar] [CrossRef]
- Chung, F.-P.; Lin, Y.-J.; Chang, S.-L.; Lo, L.-W.; Hu, Y.-F.; Chen, Y.-Y.; Chiou, C.-W.; Chen, S.-A. Long-Term Follow-Up of Catheter Ablation of Ventricular Arrhythmias: Experiences from a Tertiary Referral Center in Taiwan. Acta Cardiol. Sin. 2015, 31, 8–17. [Google Scholar]
- Park, K.M.; Kim, Y.H.; Marchlinski, F.E. Using the surface electrocardiogram to localize the origin of idiopathic ventricular tachycardia. Pacing Clin. Electrophysiol. 2012, 35, 1516–1527. [Google Scholar] [CrossRef] [PubMed]
- Attia, Z.I.; Friedman, P.A.; Noseworthy, P.A.; Lopez-Jimenez, F.; Ladewig, D.J.; Satam, G.; Pellikka, P.A.; Munger, T.M.; Asirvatham, S.J.; Scott, C.G.; et al. Age and Sex Estimation Using Artificial Intelligence From Standard 12-Lead ECGs. Circ. Arrhythm. Electrophysiol. 2019, 12, e007284. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.N. Cyclical Learning Rates for Training Neural Networks. arXiv 2017, arXiv:1506.01186v6, 464–472. [Google Scholar]
- Paszke, A.; Gross, S.; Massa, F.; Lerer, A.; Bradbury, J.; Chanan, G.; Killeen, T.; Lin, Z.; Gimelshein, N.; Antiga, L.; et al. PyTorch: An imperative style, high-performance deep learning library. Adv. Neural Inf. Processing Syst. 2019, 32, 8026–8037. [Google Scholar]
- Yang, Y.; Saenz, L.C.; Varosy, P.D.; Badhwar, N.; Justin, H.T.; Kilicaslan, F.; Keung, E.C.; Natale, A.; Marrouche, N.F.; Scheinman, M.M. Using the initial vector from surface electrocardiogram to distinguish the site of outflow tract tachycardia. Pacing Clin. Electrophysiol. 2007, 30, 891–898. [Google Scholar] [CrossRef]
- Yamada, T.; McElderry, H.T.; Doppalapudi, H.; Okada, T.; Murakami, Y.; Yoshida, Y.; Yoshida, N.; Inden, Y.; Murohara, T.; Plumb, V.J.; et al. Idiopathic ventricular arrhythmias originating from the left ventricular summit: Anatomic concepts relevant to ablation. Circ. Arrhythm. Electrophysiol. 2010, 3, 616–623. [Google Scholar] [CrossRef] [Green Version]
- Yoshida, N.; Inden, Y.; Uchikawa, T.; Kamiya, H.; Kitamura, K.; Shimano, M.; Tsuji, Y.; Hirai, M.; Murohara, T. Novel transitional zone index allows more accurate differentiation between idiopathic right ventricular outflow tract and aortic sinus cusp ventricular arrhythmias. Heart Rhythm. 2011, 8, 349–356. [Google Scholar] [CrossRef]
- Yoshida, N.; Yamada, T.; McElderry, H.T.; Inden, Y.; Shimano, M.; Murohara, T.; Kumar, V.; Doppalapudi, H.J.; Plumb, V.; Kay, G.N. A novel electrocardiographic criterion for differentiating a left from right ventricular outflow tract tachycardia origin: The V2S/V3R index. J. Cardiovasc. Electrophysiol. 2014, 25, 747–753. [Google Scholar] [CrossRef]
- Nakamura, T.; Nagata, Y.; Nitta, G.; Okata, S.; Nagase, M.; Mitsui, K.; Watanabe, K.; Miyazaki, R.; Kaneko, M.; Nagamine, S.; et al. Prediction of premature ventricular complex origins using artificial intelligence-enabled algorithms. Cardiovasc. Digit. Health J. 2021, 2, 76–83. [Google Scholar] [CrossRef]
- He, K.; Nie, Z.; Zhong, G.; Yang, C.; Sun, J. Localization of origins of premature ventricular contraction in the whole ventricle based on machine learning and automatic beat recognition from 12-lead ECG. Physiol Meas. 2020, 41, 055007. [Google Scholar] [CrossRef]
- Zheng, J.; Fu, G.; Abudayyeh, I.; Yacoub, M.; Chang, A.; Feaster, W.W.; Ehwerhemuepha, L.; El-Askary, H.; Du, X.; He, B.; et al. A High-Precision Machine Learning Algorithm to Classify Left and Right Outflow Tract Ventricular Tachycardia. Front. Physiol. 2021, 12, 641066. [Google Scholar] [CrossRef]
- Sapp, J.L.; Bar-Tal, M.; Howes, A.J.; Toma, J.E.; El-Damaty, A.; Warren, J.W.; MacInnis, P.J.; Zhou, S.; Horáček, B.M. Real-Time Localization of Ventricular Tachycardia Origin From the 12-Lead Electrocardiogram. JACC Clin. Electrophysiol. 2017, 3, 687–699. [Google Scholar] [CrossRef]
- Enriquez, A.; Malavassi, F.; Saenz, L.C.; Supple, G.; Santangeli, P.; Marchlinski, F.E.; Garcia, F.C. How to map and ablate left ventricular summit arrhythmias. Heart Rhythm. 2017, 14, 141–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanagaratnam, L.; Tomassoni, G.; Schweikert, R.; Pavia, S.; Bash, D.; Beheiry, S.; Niebauer, M.; Saliba, W.; Chung, M.; Tchou, P.; et al. Ventricular tachycardias arising from the aortic sinus of valsalva: An under-recognized variant of left outflow tract ventricular tachycardia. J. Am. Coll Cardiol. 2001, 37, 408–414. [Google Scholar] [CrossRef] [Green Version]
- Yokokawa, M.; Jung, D.Y.; Hero, A.O.; Baser, K., III; Morady, F.; Bogun, F. Single- and dual-site pace mapping of idiopathic septal intramural ventricular arrhythmias. Heart Rhythm. 2016, 13, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Asirvatham, S.J. Correlative anatomy for the invasive electrophysiologist: Outflow tract and supravalvar arrhythmia. J. Cardiovasc Electrophysiol. 2009, 20, 955–968. [Google Scholar] [CrossRef]
- Yamada, T.; Murakami, Y.; Yoshida, N.; Okada, T.; Shimizu, T.; Toyama, J.; Yoshida, Y.; Tsuboi, N.; Muto, M.; Inden, Y.; et al. Preferential conduction across the ventricular outflow septum in ventricular arrhythmias originating from the aortic sinus cusp. J. Am. Coll Cardiol. 2007, 50, 884–891. [Google Scholar] [CrossRef]
- Shirai, Y.; Do, J.J.L.; Garcia, F.C.; Supple, G.E.; Callans, D.J.; Zado, E.S.; Marchlinski, F.E.; Santangeli, P. QRS morphology shift following catheter ablation of idiopathic outflow tract ventricular arrhythmias: Prevalence, mapping features, and ablation outcomes. J. Cardiovasc Electrophysiol. 2018, 29, 1664–1671. [Google Scholar] [CrossRef]
- Futyma, P.; Santangeli, P.; Pürerfellner, H.; Pothineni, N.V.; Głuszczyk, R.; Ciąpała, K.; Moroka, K.; Martinek, M.; Futyma, M.; Marchlinski, F.E.; et al. Anatomic approach with bipolar ablation between the left pulmonic cusp and left ventricular outflow tract for left ventricular summit arrhythmias. Heart Rhythm. 2020, 17, 1519–1527. [Google Scholar] [CrossRef]
- Tavares, L.; Lador, A.; Fuentes, S.; Da-Wariboko, A.; Blaszyk, K.; Malaczynska-Rajpold, K.; Papiashvili, G.; Korolev, S.; Peichl, P.; Josef Kautzner, J.; et al. Intramural Venous Ethanol Infusion for Refractory Ventricular Arrhythmias: Outcomes of a Multicenter Experience. JACC Clin. Electrophysiol. 2020, 6, 1420–1431. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Locations | Training/Validation Data | Testing Data | - | Training/Validation Data | Testing Data | ||||
|---|---|---|---|---|---|---|---|---|---|
| Subject Number (TPE/ZJ)% | Wave Number (TPE/ZJ)% | Subject Number TPE (%) | Wave Number TPE (%) | Detailed Location | Subject Number (TPE/ZJ) % | Wave Number (TPE/ZJ) % | Subject Number TPE (%) | Wave Number TPE (%) | |
| LVOT Cusp | 111 (40/71) 18.88 | 750 (448/302) 24.23 | 15 (27.27) | 139 (28.90) | Supravalvular LCC | 56 (17/39) 9.52 | 389 (232/148) 10.70 | 6 (10.90) | 49 (10.19) |
| Supravalvular RCC | 15 (8/7) 2.55 | 108 (76/32) 2.98 | 3 (5.45) | 24 (4.99) | |||||
| Supravalvular LCC/RCC junction | 20 (13/7) 3.40 | 172 (138/34) 4.74 | 5 (9.09) | 62 (12.89) | |||||
| Infravalvular AMC | 18 (0/18) 3.06 | 88 (0/88) 2.43 | 1 (1.82) | 4 (0.83) | |||||
| Supravalvular Septo-parahisian | 2 (2/0) 0.0 | 2 (2/0) 0.06 | 0 (0.0) | 0 (0.0) | |||||
| LV Summit | 69 (64/5) 13.73 | 641 (625/16) 17.67 | 10 (18.18) | 103 (21.41) | LVOT Epicardial AIV/CGV | 69 (64/5) 11.73 | 641 (625/16) 17.67 | 10 (18.18) | 103 (21.41) |
| LV chamber | 24 (22/0) 3.74 | 199 (199/0) 5.49 | 3 (5.45) | 70 (14.55) | MA | 4 (4/0) 0.68 | 12 (12/0) 0.33 | 1 (1.82) | 55 (11.43) |
| PPM Anterolateral | 6 (6/0) 0.68 | 28 (28/0) 0.77 | 0 (0.0) | 0 | |||||
| PPM Posteromedial | 1 (1/0) 0.17 | 10 (10/0) 0.28 | 1 (1.82) | 9 (1.87) | |||||
| Crux | 1 (1/0) 0.17 | 4 (4/0) 0.11 | 0 (0.0) | 0 | |||||
| Fascicular Left posterior fascicle | 3 (3/0) 0.51 | 14 (14/0) 0.39 | 0 (0.0) | 0 | |||||
| Fascicular Left anterior fascicle | 9 (9/0) 1.53 | 131 (131/0) 3.60 | 1 (1.82) | 6 (1.25) | |||||
| RVOT | 226 (135/91) 38.44 | 1273 (930/343) 35.09 | 17 (30.91) | 99 (20.58) | RVOT | 226 (135/91) 38.44 | 1273 (930/343) 35.09 | 17 (30.91) | 99 (20.58) |
| RV chamber | 167 (40/120) 27.21 | 765 (316/449) 21.09 | 10 (18.18) | 70 (14.55) | Parahisian | 2 (2/0) 0.34 | 2 (2/0) 0.06 | 1 (1.82) | 1 (0.21) |
| TA | 13 (13/0) 2.21 | 99 (99/0) 2.73 | 3 (5.45) | 4 (0.83) | |||||
| PA | 144 (24/120) 24.49 | 645 (196/449) 17.78 | 4 (7.27) | 24 (4.99) | |||||
| PPM | 1 (1/0) 0.17 | 19 (19/0) 0.52 | 2 (3.63) | 41 (8.52) | |||||
| total | 588 | 3628 | 55 | 481 | - | 588 (301/287) | 3628 (2518/1110) | 55 | 481 |
| Marker | Input Size | Layer | Output Size | Number of Feature Maps | Kernel Size | Stride | Activation |
|---|---|---|---|---|---|---|---|
| - | - | ECG in 2D | 12 × 1024 | - | - | - | - |
| C1 | 12 × 1024 | Convolution | 16 × 12 × 1024 | 16 | 1 × 129 | 1 | ReLU |
| C2 | 16 × 12 × 1024 | Convolution | 16 × 12 × 1024 | 16 | 1 × 129 | 1 | ReLU |
| - | 16 × 12 × 1024 | Average pooling | 16 × 12 × 512 | 16 | - | 2 | - |
| C3 | 16 × 12 × 512 | Convolution | 16 × 12 × 512 | 16 | 1 × 65 | 1 | ReLU |
| - | 32 × 12 × 512 | Average pooling | 16 × 12 × 256 | 16 | - | 2 | - |
| C4 | 32 × 12 × 256 | Convolution | 32 × 12 × 256 | 32 | 1 × 33 | 1 | ReLU |
| - | 64 × 12 × 128 | Average pooling | 64 × 12 × 64 | 64 | - | 2 | - |
| C5 | 128 × 12 × 64 | Convolution | 128 × 1 × 64 | 128 | 12 × 1 | 1 | ReLU |
| C6 | 128 × 1 × 64 | Convolution | 128 × 1 × 64 | 128 | 1 × 3 | 1 | ReLU |
| - | 128 × 1 × 64 | Average pooling | 128 × 1 × 64 | 128 | - | 2 | - |
| - | 1 × 8192 | Fully connected | 1 × 1024 | - | - | - | ReLU |
| - | 1 × 1024 | Fully connected | 1 | - | - | - | Sigmoid |
| Clinical Features | Taipei Veterans General Hospital (n = 397) | Chapman University and Ningbo First Hospital of Zhejiang University (n = 334) |
|---|---|---|
| Age (years) | 48.7 ± 15.6 | 46.1 ± 13.1 |
| Male (n,%) | 173 (43.6%) | 104 (32%) |
| Dyslipidemia (n,%) | 43 (10.8%) | - |
| Diabetes mellitus (n,%) | 29 (7.3%) | - |
| Hypertension (n,%) | 85 (21.4%) | - |
| Chronic Kidney Disease (n,%) | 5 (1.3%) | - |
| Old stroke (n,%) | 3 (0.8%) | - |
| Atrial Fibrillation (n,%) | 13 (3.3%) | - |
| OSAS (n,%) | 8 (2.1%) | - |
| Method Type | Methods | Classification | Cases for Testing | Accuracy Sensitivity/Specificity % | Reference |
|---|---|---|---|---|---|
| Deep Learning | CNN | Left vs. Right side | 55 | 91/92 | Current Study |
| Deep Learning | CNN | LV summit vs. others | 55 | 100/98 | Current Study |
| Deep Learning | CNN | Left vs. Right side | 21 | 100/92 | Ref. [29] |
| Machine Learning | SVM | Left vs. Right side | 21 | 100/82 | Ref. [29] |
| Machine Learning | SVM | LVOT vs. others | 117 | 64/? * | Ref. [30] |
| Machine Learning | ECG Feature extraction + SVM | LVOT vs. RVOT | 42 | 96/100 | Ref. [31] |
| Manual Rules | RBBB pattern, aVL/aVR amplitude ratio and S wave in V5 or V6 | LV summit vs. others | 27 | 87/100 | Ref. [26] |
| Manual Rules | The earliest onset of QRS and peak/nadir in V2 | LVOT vs. RVOT | 45 | 92/88 | Ref. [25] |
| Manual Rules | Combined TZ index and V2S/V3R | LVOT vs. RVOT | 695 | 90/87 | Ref. [8] |
| Manual Rules | V2S/V3R index ≤1.5 predicting LVOT origin | LVOT vs. RVOT | 207 | 89/94 | Ref. [28] |
| Manual Rules | Transition zone index <0 predicting LVOT origin | LVOT vs. RVOT | 112 | 88/82 | Ref. [27] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, T.-Y.; Chen, K.-W.; Liu, C.-M.; Chang, S.-L.; Lin, Y.-J.; Lo, L.-W.; Hu, Y.-F.; Chung, F.-P.; Lin, C.-Y.; Kuo, L.; et al. A High-Precision Deep Learning Algorithm to Localize Idiopathic Ventricular Arrhythmias. J. Pers. Med. 2022, 12, 764. https://doi.org/10.3390/jpm12050764
Chang T-Y, Chen K-W, Liu C-M, Chang S-L, Lin Y-J, Lo L-W, Hu Y-F, Chung F-P, Lin C-Y, Kuo L, et al. A High-Precision Deep Learning Algorithm to Localize Idiopathic Ventricular Arrhythmias. Journal of Personalized Medicine. 2022; 12(5):764. https://doi.org/10.3390/jpm12050764
Chicago/Turabian StyleChang, Ting-Yung, Ke-Wei Chen, Chih-Min Liu, Shih-Lin Chang, Yenn-Jiang Lin, Li-Wei Lo, Yu-Feng Hu, Fa-Po Chung, Chin-Yu Lin, Ling Kuo, and et al. 2022. "A High-Precision Deep Learning Algorithm to Localize Idiopathic Ventricular Arrhythmias" Journal of Personalized Medicine 12, no. 5: 764. https://doi.org/10.3390/jpm12050764