
Do the Successive Waves of SARS-CoV-2, Vaccination Status and Place of Infection Influence the Clinical Picture and COVID-19 Severity among Patients with Persistent Clinical Symptoms? The Retrospective Study of Patients from the STOP-COVID Registry of the PoLoCOV-Study


 , ,
, ,  ,
,  , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Patients and Eligibility Criteria
- SARS-CoV-2 virus infection (asymptomatic, mild, moderate, and severe course, hospitalization) confirmed by the RT-PCR test result;
- age ≥ 18;
- consent of the respondent to participate in the study;
- there are no contraindications to participate in the study.
- Group 1 (II wave) cases–from 1 September 2020 to 30 January 2021;
- Group 2 (III wave) cases–from 1 February 2021 to 30 August 2021;
- Group 3 (IV wave) cases–from 1 September 2021 to the end of the follow-up period.
- 1
- Asymptomatic:
- no symptoms;
- parainfluenza symptoms of upper respiratory tract infection for up to 3 days.
- 2
- Mild:
- home course of infection;
- subjective evaluation by the patient as a light course (“1” on a 1–3 scale);
- duration of symptoms up to 7 days.
- 3
- Moderate:
- subjective evaluation by the patient as moderate/severe course (“2 or 3” on a 1–3 scale);
- duration of symptoms more than 7 days but less than 14 days;
- temperature > 38 °C and dyspnea
- 4
- Severe:
- one of the following: hospitalization with diagnosis: pneumonia, respiratory failure, intensive care unit, assisted breathing, thromboembolic complications during hospitalization or;
- home course with symptoms lasting >14 days, subjective evaluation by the patient as severe (“3” on a scale of 1–3), with temperature >38 °C, dyspnea or saturation below 94 lasting more than 3 days.
2.2. Statistical Analysis
3. Results
3.1. Study Group Characteristics
3.2. COVID-19 Clinical Symptom Characteristics
3.3. Summary of the Clinical Symptoms in Patients Subjected to Home Isolation and Hospitalisation
3.4. The Impact of Vaccination on COVID-19 Clinical Manifestations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Adil, M.T.; Rahman, R.; Whitelaw, D.; Jain, V.; Al-Taan, O.; Rashid, F.; Munasinghe, A.; Jambulingam, P. SARS-CoV-2 and the pandemic of COVID-19. Postgrad. Med. J. 2021, 97, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Rathi, H.; Burman, V.; Datta, S.K.; Rana, S.V.; Mirza, A.A.; Saha, S.; Kumar, R.; Naithani, M. Review on COVID-19 Etiopathogenesis, Clinical Presentation and Treatment Available with Emphasis on ACE2. Indian J. Clin. Biochem. 2021, 36, 3–22. [Google Scholar] [CrossRef] [PubMed]
- Beyerstedt, S.; Casaro, E.B.; Rangel, E.B. COVID-19: Angiotensin-converting enzyme 2 (ACE2) expression and tissue susceptibility to SARS-CoV-2 infection. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 905–919. [Google Scholar] [CrossRef] [PubMed]
- Rokni, M.; Ghasemi, V.; Tavakoli, Z. Immune responses and pathogenesis of SARS-CoV-2 during an outbreak in Iran: Comparison with SARS and MERS. Rev. Med. Virol. 2020, 30, e2107. [Google Scholar] [CrossRef] [Green Version]
- Zhou, P.; Yang, X.L.; Wang, X.G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.R.; Zhu, Y.; Li, B.; Huang, C.L.; et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef] [Green Version]
- Schweitzer, F.; Kleineberg, N.N.; Goreci, Y.; Onur, O.A.; Franke, C.; Warnke, C. Neuro-COVID-19 is more than anosmia: Clinical presentation, neurodiagnostics, therapies, and prognosis. Curr. Opin. Neurol. 2021, 34, 423–431. [Google Scholar] [CrossRef]
- AlJishi, J.M.; Alhajjaj, A.H.; Alkhabbaz, F.L.; AlAbduljabar, T.H.; Alsaif, A.; Alsaif, H.; Alomran, K.S.; Aljanobi, G.A.; Alghawi, Z.; Alsaif, M.; et al. Clinical characteristics of asymptomatic and symptomatic COVID-19 patients in the Eastern Province of Saudi Arabia. J. Infect. Public Health 2021, 14, 6–11. [Google Scholar] [CrossRef]
- Chen, G.; Wu, D.; Guo, W.; Cao, Y.; Huang, D.; Wang, H.; Wang, T.; Zhang, X.; Chen, H.; Yu, H.; et al. Clinical and immunological features of severe and moderate coronavirus disease 2019. J. Clin. Investig. 2020, 130, 2620–2629. [Google Scholar] [CrossRef] [Green Version]
- Chavez, S.; Long, B.; Koyfman, A.; Liang, S.Y. Coronavirus Disease (COVID-19): A primer for emergency physicians. Am. J. Emerg. Med. 2021, 44, 220–229. [Google Scholar] [CrossRef]
- Wong, S.H.; Lui, R.N.; Sung, J.J. COVID-19 and the digestive system. J. Gastroenterol. Hepatol. 2020, 35, 744–748. [Google Scholar] [CrossRef]
- Lechien, J.R.; Chiesa-Estomba, C.M.; De Siati, D.R.; Horoi, M.; Le Bon, S.D.; Rodriguez, A.; Dequanter, D.; Blecic, S.; El Afia, F.; Distinguin, L.; et al. Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (COVID-19): A multicenter European study. Eur. Arch. Otorhinolaryngol. 2020, 277, 2251–2261. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.D.; Ding, M.; Dong, X.; Zhang, J.J.; Kursat Azkur, A.; Azkur, D.; Gan, H.; Sun, Y.L.; Fu, W.; Li, W.; et al. Risk factors for severe and critically ill COVID-19 patients: A review. Allergy 2021, 76, 428–455. [Google Scholar] [CrossRef] [PubMed]
- Yek, C.; Warner, S.; Wiltz, J.L.; Sun, J.; Adjei, S.; Mancera, A.; Silk, B.J.; Gundlapalli, A.V.; Harris, A.M.; Boehmer, T.K.; et al. Risk Factors for Severe COVID-19 Outcomes Among Persons Aged >/=18 Years Who Completed a Primary COVID-19 Vaccination Series—465 Health Care Facilities, United States, December 2020-October 2021. MMWR Morb. Mortal Wkly. Rep. 2022, 71, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Jordan, R.E.; Adab, P.; Cheng, K.K. COVID-19: Risk factors for severe disease and death. BMJ 2020, 368, m1198. [Google Scholar] [CrossRef] [Green Version]
- Reilev, M.; Kristensen, K.B.; Pottegard, A.; Lund, L.C.; Hallas, J.; Ernst, M.T.; Christiansen, C.F.; Sorensen, H.T.; Johansen, N.B.; Brun, N.C.; et al. Characteristics and predictors of hospitalization and death in the first 11 122 cases with a positive RT-PCR test for SARS-CoV-2 in Denmark: A nationwide cohort. Int. J. Epidemiol. 2020, 49, 1468–1481. [Google Scholar] [CrossRef]
- Krishnan, A.; Hamilton, J.P.; Alqahtani, S.A.; Woreta, T.A. COVID-19: An overview and a clinical update. World J. Clin. Cases 2021, 9, 8–23. [Google Scholar] [CrossRef]
- Lauring, A.S.; Hodcroft, E.B. Genetic Variants of SARS-CoV-2-What Do They Mean? JAMA 2021, 325, 529–531. [Google Scholar] [CrossRef]
- SeyedAlinaghi, S.; Mirzapour, P.; Dadras, O.; Pashaei, Z.; Karimi, A.; MohsseniPour, M.; Soleymanzadeh, M.; Barzegary, A.; Afsahi, A.M.; Vahedi, F.; et al. Characterization of SARS-CoV-2 different variants and related morbidity and mortality: A systematic review. Eur. J. Med. Res. 2021, 26, 51. [Google Scholar] [CrossRef]
- Lindner-Pawlowicz, K.; Mydlikowska-Smigorska, A.; Lampika, K.; Sobieszczanska, M. COVID-19 Vaccination Acceptance among Healthcare Workers and General Population at the Very Beginning of the National Vaccination Program in Poland: A Cross-Sectional, Exploratory Study. Vaccines 2021, 10, 66. [Google Scholar] [CrossRef]
- Mohammed, I.; Nauman, A.; Paul, P.; Ganesan, S.; Chen, K.H.; Jalil, S.M.S.; Jaouni, S.H.; Kawas, H.; Khan, W.A.; Vattoth, A.L.; et al. The efficacy and effectiveness of the COVID-19 vaccines in reducing infection, severity, hospitalization, and mortality: A systematic review. Hum. Vaccines Immunother. 2022, 18, 2027160. [Google Scholar] [CrossRef]
- Jain, V.; Yuan, J.M. Predictive symptoms and comorbidities for severe COVID-19 and intensive care unit admission: A systematic review and meta-analysis. Int. J. Public Health 2020, 65, 533–546. [Google Scholar] [CrossRef] [PubMed]
- Chams, N.; Chams, S.; Badran, R.; Shams, A.; Araji, A.; Raad, M.; Mukhopadhyay, S.; Stroberg, E.; Duval, E.J.; Barton, L.M.; et al. COVID-19: A Multidisciplinary Review. Front. Public Health 2020, 8, 383. [Google Scholar] [CrossRef] [PubMed]
- Bhatraju, P.K.; Ghassemieh, B.J.; Nichols, M.; Kim, R.; Jerome, K.R.; Nalla, A.K.; Greninger, A.L.; Pipavath, S.; Wurfel, M.M.; Evans, L.; et al. COVID-19 in Critically Ill Patients in the Seattle Region—Case Series. N. Engl. J. Med. 2020, 382, 2012–2022. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Gomez-Ochoa, S.A.; Franco, O.H.; Rojas, L.Z.; Raguindin, P.F.; Roa-Diaz, Z.M.; Wyssmann, B.M.; Guevara, S.L.R.; Echeverria, L.E.; Glisic, M.; Muka, T. COVID-19 in Health-Care Workers: A Living Systematic Review and Meta-Analysis of Prevalence, Risk Factors, Clinical Characteristics, and Outcomes. Am. J. Epidemiol. 2021, 190, 161–175. [Google Scholar] [CrossRef]
- Fernandez-de-Las-Penas, C.; Palacios-Cena, D.; Gomez-Mayordomo, V.; Florencio, L.L.; Cuadrado, M.L.; Plaza-Manzano, G.; Navarro-Santana, M. Prevalence of post-COVID-19 symptoms in hospitalized and non-hospitalized COVID-19 survivors: A systematic review and meta-analysis. Eur. J. Intern. Med. 2021, 92, 55–70. [Google Scholar] [CrossRef]
- Alimohamadi, Y.; Sepandi, M.; Taghdir, M.; Hosamirudsari, H. Determine the most common clinical symptoms in COVID-19 patients: A systematic review and meta-analysis. J. Prev. Med. Hyg. 2020, 61, E304–E312. [Google Scholar] [CrossRef]
- Touisserkani, S.K.; Ayatollahi, A. Oral Corticosteroid Relieves Post-COVID-19 Anosmia in a 35-Year-Old Patient. Case Rep. Otolaryngol. 2020, 2020, 5892047. [Google Scholar] [CrossRef]
- Rashid, R.A.; Zgair, A.; Al-Ani, R.M. Effect of nasal corticosteroid in the treatment of anosmia due to COVID-19: A randomised double-blind placebo-controlled study. Am. J. Otolaryngol. 2021, 42, 103033. [Google Scholar] [CrossRef]
- Matsunaga, N.; Hayakawa, K.; Asai, Y.; Tsuzuki, S.; Terada, M.; Suzuki, S.; Ohtsu, H.; Kitajima, K.; Toyoda, A.; Suzuki, K.; et al. Clinical characteristics of the first three waves of hospitalized patients with COVID-19 in Japan prior to the widespread use of vaccination: A nationwide observational study. Lancet Reg. Health West Pac. 2022, 22, 100421. [Google Scholar] [CrossRef]
- Hamdan, M.; Badrasawi, M.; Zidan, S.; Sayarah, A.; Zahra, L.A.; Dana, S.; Almasry, T. Risk factors associated with hospitalization owing to COVID-19: A cross-sectional study in Palestine. J. Int. Med. Res. 2021, 49, 3000605211064405. [Google Scholar] [CrossRef]
- Vaira, L.A.; De Vito, A.; Lechien, J.R.; Chiesa-Estomba, C.M.; Mayo-Yàñez, M.; Calvo-Henrìquez, C.; Saussez, S.; Madeddu, G.; Babudieri, S.; Boscolo-Rizzo, P.; et al. New Onset of Smell and Taste Loss Are Common Findings Also in Patients with Symptomatic COVID-19 after Complete Vaccination. Laryngoscope 2022, 132, 419–421. [Google Scholar] [CrossRef] [PubMed]
- Avcı, H.; Karabulut, B.; Eken, H.D.; Faraşoğlu, A.; Çakil, T.; Çoruk, S.; Özel, H.; Kaya, N.K.; Özbalta, S.Ö. Otolaryngology-Specific Symptoms May Be Highly Observed in Patients with a History of COVID-19 Infection after Inactivated Coronavirus Vaccination. Ear Nose Throat J. 2021, 8, 1455613211028493. [Google Scholar] [CrossRef] [PubMed]
- Moghadas, S.M.; Vilches, T.N.; Zhang, K.; Wells, C.R.; Shoukat, A.; Singer, B.H.; Meyers, L.A.; Neuzil, K.M.; Langley, J.M.; Fitzpatrick, M.C.; et al. The Impact of Vaccination on Coronavirus Disease 2019 (COVID-19) Outbreaks in the United States. Clin. Infect. Dis. 2021, 73, 2257–2264. [Google Scholar] [CrossRef] [PubMed]
- Antonelli, M.; Penfold, R.S.; Merino, J.; Sudre, C.H.; Molteni, E.; Berry, S.; Canas, L.S.; Graham, M.S.; Klaser, K.; Modat, M.; et al. Risk Factors and Disease Profile of Post-Vaccination SARS-CoV-2 Infection in UK Users of the COVID Symptom Study App: A Prospective, Community-Based, Nested, Case-Control Study. Lancet Infect. Dis. 2022, 22, 43–55. [Google Scholar] [CrossRef]
- Hirabara, S.M.; Serdan, T.D.A.; Gorjao, R.; Masi, L.N.; Pithon-Curi, T.C.; Covas, D.T.; Curi, R.; Durigon, E.L. SARS-CoV-2 Variants: Differences and Potential of Immune Evasion. Front. Cell. Infect. Microbiol. 2021, 11, 781429. [Google Scholar] [CrossRef] [PubMed]
- Guruprasad, K. Mutations in Human SARS-CoV-2 Spike Proteins, Potential Drug Binding and Epitope Sites for COVID-19 Therapeutics Development. Curr. Res. Struct. Biol. 2022, 4, 41–50. [Google Scholar] [CrossRef]
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Rickeard, T.; Gallagher, E.; Gower, C.; Kall, M.; Groves, N.; O’Connell, A.-M.; et al. COVID-19 Vaccine Effectiveness against the Omicron (B.1.1.529) Variant. N. Engl. J. Med. 2022, 386, 1532–1546. [Google Scholar] [CrossRef]
- Bruxvoort, K.J.; Sy, L.S.; Qian, L.; Ackerson, B.K.; Luo, Y.; Lee, G.S.; Tian, Y.; Florea, A.; Aragones, M.; Tubert, J.E.; et al. Effectiveness of MRNA-1273 against Delta, Mu, and Other Emerging Variants of SARS-CoV-2: Test Negative Case-Control Study. BMJ 2021, 375, e068848. [Google Scholar] [CrossRef]
- Mahase, E. COVID-19: What Do We Know about the Delta Omicron Recombinant Variant? BMJ 2022, 376, o792. [Google Scholar] [CrossRef]
- Gao, W.; Lv, J.; Pang, Y.; Li, L.M. Role of asymptomatic and pre-symptomatic infections in COVID-19 pandemic. BMJ 2021, 375, n2342. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | The Whole Group (n = 1961) | Second Wave (n = 1069) | Third Wave (n = 782) | Fourth Wave (n = 110) | Home Insulation (n = 1619) | Hospitalization (n = 342) | Vaccinated (n = 184) | Unvaccinated (n = 708) | p * | |
|---|---|---|---|---|---|---|---|---|---|---|
| Sex | Female | 1219 (62.2) | 655 (62.3) | 489 (62.5) | 75 (68.2) | 1051 (65.5) | 168 (40.8) | 132 (28.6) | 277 (39.1) | 0.011 |
| Male | 742 (37.8) | 397 (37.7) | 293 (37.5) | 35 (31.8) | 568 (35.5) | 174 (50.2) | 53 (71.4) | 432 (60.9) | ||
| Age (M ± SD) | 52.8 ± 13.6 | 51.9 ± 13.3 | 54.3 ± 13.7 | 51.0 ± 14.9 | 51.6 ± 13.3 | 59.1 ± 13.1 | 54.04 ± 14.4 | 53.8 ± 13.7 | 0.793 | |
| Weight [kg] (M ± SD) | 79.9 ± 17.8 | 79.6 ± 17.8 | 80.8 ± 18.1 | 76.9 ± 15.5 | 79.1 ± 17.6 | 83.8 ± 18.1 | 78.1 ± 16.2 | 80.9 ± 18.2 | 0.108 | |
| Height [cm] (M ± SD) | 169 ± 9.1 | 169.7 ± 9.0 | 168.9 ± 9.1 | 168.1 ± 15.5 | 169.3 ± 8.9 | 169.1 ± 9.7 | 167.5 ± 9.5 | 169 ± 9.0 | 0.051 | |
| BMI (M ± SD) | 27.8 ± 5.5 | 27.6 ± 5.5 | 28.2 ± 5.5 | 27.3 ± 5.8 | 27.5 ± 5.5 | 29.2 ± 5.4 | 27.8 ± 5.6 | 28.8 ± 5.6 | 0.434 | |
| Chronic diseases | Hypertension | 742 (37.8) | 371 (34.7) | 331 (42.3) | 40 (36.4) | 555 (34.2) | 187 (54.7) | 76 (41.1) | 296 (41.8) | 0.924 |
| Diabetes | 210 (10.7) | 98 (9.2) | 101 (12.9) | 11 (10.0) | 147 (9.1) | 63 (18.4) | 21 (11.4) | 91 (12.9) | 0.671 | |
| Coronary artery disease | 129 (6.6) | 67 (6.3) | 55 (7.0) | 7 (6.4) | 81 (5.0) | 48 (14.0) | 16 (8.7) | 46 (6.5) | 0.388 | |
| Heart failure | 67 (3.5) | 28 (2.6) | 38 (4.9) | 1 (0.9) | 50 (3.1) | 17 (5.0) | 0 (0.0) | 39 (5.5) | <0.001 | |
| Venous thromboembolism | 22 (1.2) | 13 (1.2) | 9 (1.1) | 0 (0) | 18 (1.1) | 4 (1.2) | 3 (1.5) | 6 (0.9) | 0.573 | |
| Hyperlipidemia | 414 (21.1) | 209 (19.6) | 183 (23.4) | 22 (20.0) | 340 (21.0) | 74 (21.6) | 41 (22.2) | 165 (23.3) | 0.817 | |
| Asthma | 182 (9.3) | 98 (9.2) | 72 (9.2) | 12 (10.9) | 140 (8.7) | 42 (12.3) | 16 (8.7) | 68 (9.6) | 0.791 | |
| COPD * | 49 (2.5) | 17 (1.6) | 31 (3.9) | 1 (0.9) | 35 (2.2) | 14 (4.1) | 7 (3.8) | 25 (3.5) | 0.954 | |
| Thyroid disease | 326 (16.7) | 176 (16.5) | 127 (16.2) | 21 (19.1) | 269(16.5) | 58 (16.5) | 33 (17.8) | 116 (16.2) | 0.246 | |
| A place of isolation | Home | 1619 (82.5) | 909 (85.0) | 614 (78.5) | 96 (87.3) | 1619 (100) | 0 (0.0) | 156 (84.3) | 555 (78.4) | 0.050 |
| Hospital-without pneumonia | 63 (1.5) | 38 (3.6) | 24 (3.1) | 1 (0.9) | 0 (0.0) | 63 (18.4) | 3 (1.6) | 8 (1.1) | 0.868 | |
| Hospital-with pneumonia | 272 (13.9) | 120 (11.2) | 139 (17.8) | 13 (11.8) | 0 (0.0) | 272 (79.5) | 25 (13.5) | 127 (17.9) | 0.188 | |
| Hospital-ICU | 7 (0.4) | 2 (0.2) | 5 (0.6) | 0 (0.0) | 0 (0.0) | 7 (2.1) | 1 (0.5) | 4 (0.6) | 0.966 | |
| Flu vaccinations in the previous season | 164 (8.4) | 84 (7.9) | 70 (8.9) | 10 (9.3) | 132 (8.2) | 32 (9.5) | 30 (16.3) | 50 (7.1) | <0.001 | |
| Symptom | Second Wave (n = 1069) | Third Wave (n = 782) | Fourth Wave (n = 110) | p * | The Whole Group (n = 1961) | |
|---|---|---|---|---|---|---|
| Patient with clinical symptoms | 1060 (99.2) | 779 (99.6) | 110 (100.0) | 0.320 | 1949 (99.4) | |
| Temperature < 36.6 °C | 166 (15.5) | 128 (16.4) | 14 (12.8) | 0.599 | 308 (15.7) | |
| Temperature 36.6–37.5 °C | 249 (23.3) | 162 (20.7) | 26 (23.6) | 0.551 | 437 (22.3) | |
| Temperature > 37.5 °C | 554 (51.8) | 439 (56.1) | 61 (55.5) | 0.172 | 1054 (53.7) | |
| Cough | 653 (61.1) | 541 (69.2) | 87 (79.0) | <0.001 | 1281 (65.3) | |
| Dyspnoea | 499 (46.7) | 433 (55.4) | 48 (43.6) | <0.001 | 980 (49.9) | |
| Rhinitis | 310 (29.0) | 276 (35.3) | 58 (52.7) | <0.001 | 644 (32.8) | |
| Isolated olfactory dysfunction | 118 (11.0) | 50 (6.4) | 16 (14.6) | <0.001 | 184 (9.4) | |
| Isolated taste dysfunction | 57 (5.3) | 48 (6.1) | 8 (7.3) | 0.598 | 113 (5.8) | |
| Taste and olfactory dysfunction | 544 (50.9) | 283 (36.2) | 61 (55.5) | <0.001 | 888 (45.3) | |
| Taste and/or olfactory dysfunction | 679 (63.5) | 349 (44.6) | 27 (24.6) | <0.001 | 1055 (53.8) | |
| Weakness | 793 (74.2) | 625 (79.9) | 84 (76.4) | 0.015 | 1502 (76.6) | |
| Chest pain | 465 (43.5) | 393 (50.3) | 50 (45.5) | 0.016 | 908 (46.3) | |
| Back pain | 594 (55.6) | 433 (55.4) | 53 (48.2) | 0.326 | 1080 (55.1) | |
| Leg pain | 484 (45.3) | 374 (47.8) | 48 (43.6) | 0.474 | 906 (46.2) | |
| Headache | 614 (57.4) | 458 (58.6) | 61 (55.5) | 0.781 | 1138 (57.8) | |
| Arthralgia | 449 (42.0) | 375 (48.0) | 44 (40.0) | 0.025 | 868 (44.3) | |
| Diarrhoea | 222 (20.8) | 171 (21.9) | 23 (20.9) | 0.845 | 416 (21.2) | |
| Vomits | 66 (6.2) | 64 (8.2) | 8 (7.3) | 0.247 | 138 (7.0) | |
| Chills | 399 (37.3) | 316 (40.4) | 45 (40.9) | 0.361 | 760 (38.8) | |
| Labile blood pressure values | 150 (14.0) | 138 (17.7) | 20 (18.2) | 0.082 | 308 (15.7) | |
| Hearing dysfunction | 92 (8.6) | 103 (13.2) | 16 (14.6) | 0.003 | 211 (10.8) | |
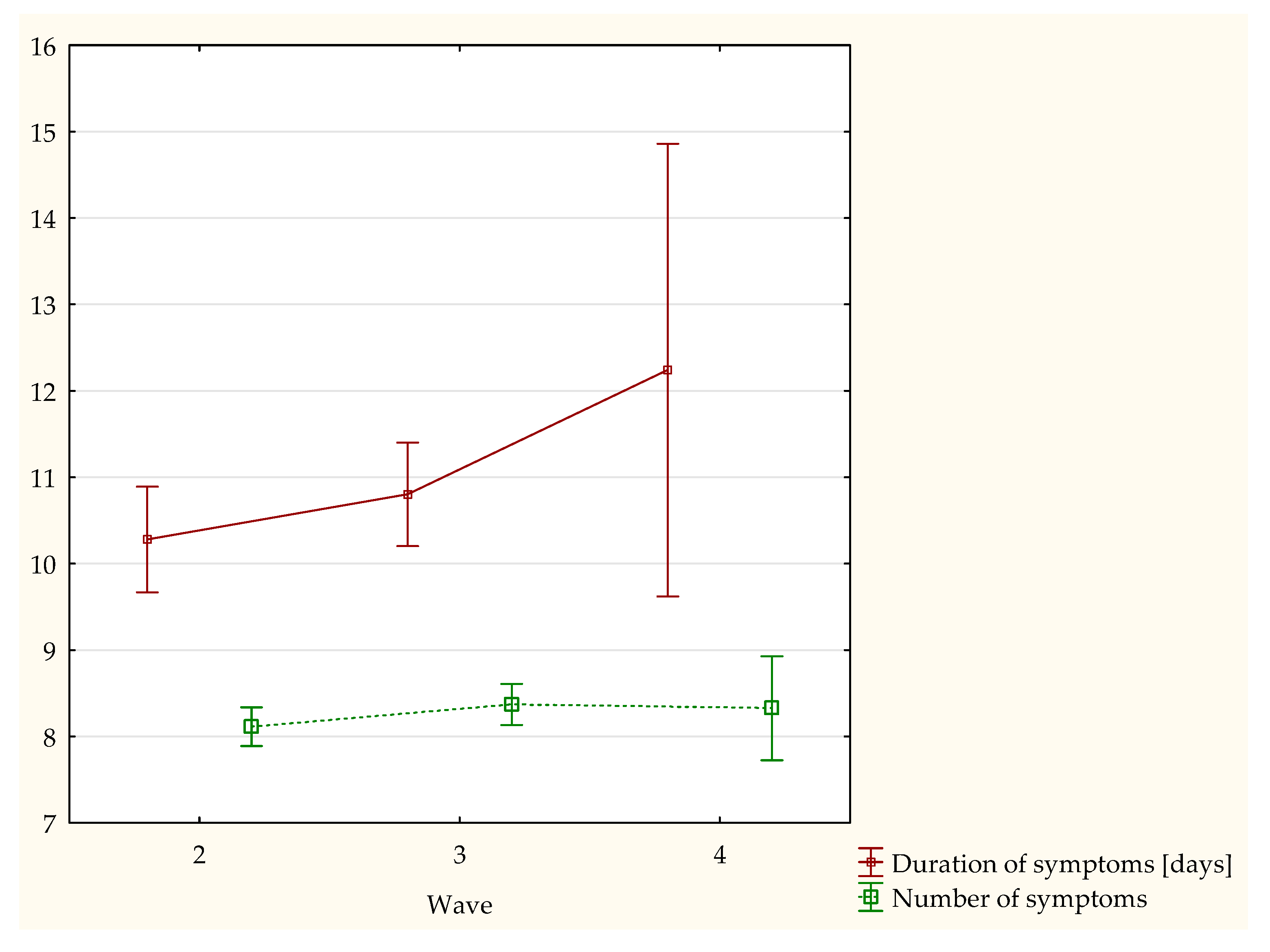
| Average number of symptoms | 8.11 ± 3.7 | 8.4 ± 3.4 | 8.32 ± 3.2 | 0.973 ** | 8.22 ± 3.6 | |
| Duration of symptoms [days] | 10.3 ± 9.9 | 10.8 ± 8.1 | 12.2 ± 8.5 | 0.298 ** | 10.6 ± 9.4 | |
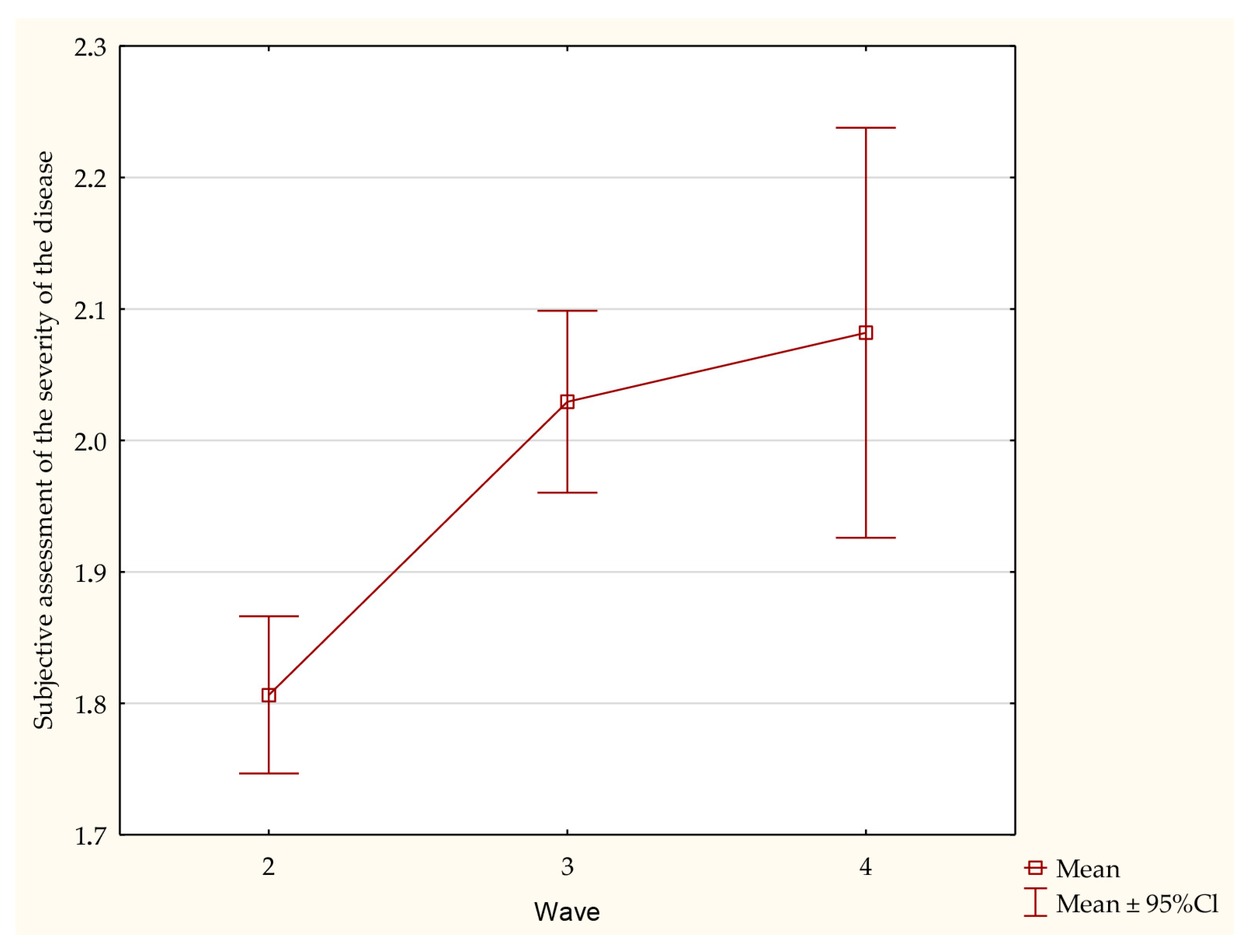
| Subjective assessment of the severity of the disease | 0 | 105 (9.8) | 64 (8.2) | 0 (0.0) | <0.001 | 169 (8.6) |
| 1 | 340 (31.8) | 176 (22.5) | 33 (30.0) | 549 (28.0) | ||
| 2 | 281 (26.3) | 215 (27.5) | 35 (31.8) | 531 (27.1) | ||
| 3 | 343 (32.1) | 327 (41.8) | 42 (38.2) | 712 (36.3) | ||
| M SD | 1.81 ± 0.9 | 2.03 ± 0.9 | 2.08 ± 0.8 | <0.001 ** | 1.9 ± 0.9 | |
| Symptom | Home Insulation | Hospitalization | p * |
|---|---|---|---|
| Patient with clinical symptoms | 1607 (99.3) | 342 (100.0) | 0.110 |
| Temperature < 36.6 °C | 284 (17.5) | 24 (7.0) | <0.001 |
| Temperature 36.6–37.5 °C | 389 (24.0) | 48 (14.0) | <0.001 |
| Temperature > 37.5 °C | 809 (49.9) | 245 (71.6) | <0.001 |
| Cough | 1033 (63.8) | 248 (72.5) | <0.001 |
| Dyspnoea | 730 (45.1) | 250 (73.1) | <0.001 |
| Rhinitis | 572 (35.3) | 72 (21.1) | <0.001 |
| Isolated olfactory dysfunction | 171 (10.5) | 13 (3.8) | <0.001 |
| Isolated taste dysfunction | 91 (5.6) | 22 (6.4) | 0.558 |
| Taste and olfactory dysfunction | 772 (47.7) | 116 (33.9) | <0.001 |
| Taste and/or olfactory dysfunction | 934 (57.7) | 121 (35.4) | <0.001 |
| Weakness | 1224 (75.6) | 278 (81.3) | 0.024 |
| Chest pain | 751 (46.4) | 157 (45.9) | 0.871 |
| Back pain | 893 (55.2) | 187 (54.6) | 0.872 |
| Leg pain | 749 (46.3) | 157 (45.9) | 0.904 |
| Headache | 974 (60.2) | 159 (46.5) | <0.001 |
| Arthralgia | 719 (44.4) | 149 (43.6) | 0.775 |
| Diarrhoea | 336 (20.8) | 80 (23.4) | 0.278 |
| Vomits | 110 (6.8) | 28 (8.2) | 0.360 |
| Chills | 632 (39.0) | 128 (37.4) | 0.578 |
| Labile blood pressure values | 244 (15.1) | 64 (18.7) | 0.095 |
| Hearing dysfunction | 171 (10.6) | 40 (11.7) | 0.548 |
| Average number of symptoms | 8.28 ± 3.6 | 7.98 ± 3.51 | 0.239 ** |
| Duration of symptoms [days] | 10.49 ± 9.3 | 11.05 ± 10.1 | 0.509 ** |
| Subjective assessment of the severity of the disease | 1.8 ± 0.9 | 2.50 ± 1.1 | <0.001 ** |
| Symptom | Vaccinated (n = 184) | Unvaccinated (n = 708) | p * |
|---|---|---|---|
| Patient with clinical symptoms | 180 (97.3 ) | 694 (98.0) | 0.543 |
| Temperature < 36.6 °C | 29 (15.7) | 112 (15.9) | 0.965 |
| Temperature 36.6–37.5 °C | 37 (19.8) | 150 (21.3) | 0.780 |
| Temperature > 37.5 °C | 97 (52.4) | 402 (57.0) | 0.300 |
| Cough | 132 (71.4) | 497 (70.5) | 0.891 |
| Dyspnoea | 93 (50.3) | 387 (54.9) | 0.298 |
| Rhinitis | 77 (41.6) | 257 (36.5) | 0.227 |
| Isolated olfactory dysfunction | 12 (6.5) | 54 (7.7) | 0.587 |
| Isolated taste dysfunction | 8 (4.3) | 47 (6.7) | 0.314 |
| Taste and olfactory dysfunction | 79 (42.7) | 265 (37.6) | 0.235 |
| Taste and/or olfactory dysfunction | 53 (28.7) | 322 (45.7) | <0.001 |
| Weakness | 140 (75.7) | 566 (80.3) | 0.202 |
| Chest pain | 83 (44.9) | 360 (51.1) | 0.156 |
| Back pain | 85 (45.9) | 401 (56.9) | 0.010 |
| Leg pain | 72 (38.9) | 349 (49.5) | 0.013 |
| Headache | 92 (49.7) | 425 (60.3) | 0.012 |
| Arthralgia | 75 (40.5) | 343 (48.7) | 0.059 |
| Diarrhoea | 34 (18.4) | 159 (22.6) | 0.260 |
| Vomits | 16 (8.7) | 56 (7.9) | 0.872 |
| Chills | 78 (42.2) | 282 (40.0) | 0.653 |
| Labile blood pressure values | 33 (17.8) | 125 (17.7) | 0.940 |
| Hearing dysfunction | 27 (14.6) | 91 (12.9) | 0.631 |
| Average number of symptoms | 7.8 ± 3.25 | 8.5 ± 3.38 | 0.013 ** |
| Duration of symptoms [days] | 11.8 ± 11.1 | 12.6 ± 7.32 | 0.008 ** |
| Subjective assessment of the severity of the disease | 2.0 ± 0.89 | 2.1 ± 0.98 | 0.372 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chudzik, M.; Babicki, M.; Kapusta, J.; Kołat, D.; Kałuzińska, Ż.; Mastalerz-Migas, A.; Jankowski, P. Do the Successive Waves of SARS-CoV-2, Vaccination Status and Place of Infection Influence the Clinical Picture and COVID-19 Severity among Patients with Persistent Clinical Symptoms? The Retrospective Study of Patients from the STOP-COVID Registry of the PoLoCOV-Study. J. Pers. Med. 2022, 12, 706. https://doi.org/10.3390/jpm12050706
Chudzik M, Babicki M, Kapusta J, Kołat D, Kałuzińska Ż, Mastalerz-Migas A, Jankowski P. Do the Successive Waves of SARS-CoV-2, Vaccination Status and Place of Infection Influence the Clinical Picture and COVID-19 Severity among Patients with Persistent Clinical Symptoms? The Retrospective Study of Patients from the STOP-COVID Registry of the PoLoCOV-Study. Journal of Personalized Medicine. 2022; 12(5):706. https://doi.org/10.3390/jpm12050706
Chicago/Turabian StyleChudzik, Michał, Mateusz Babicki, Joanna Kapusta, Damian Kołat, Żaneta Kałuzińska, Agnieszka Mastalerz-Migas, and Piotr Jankowski. 2022. "Do the Successive Waves of SARS-CoV-2, Vaccination Status and Place of Infection Influence the Clinical Picture and COVID-19 Severity among Patients with Persistent Clinical Symptoms? The Retrospective Study of Patients from the STOP-COVID Registry of the PoLoCOV-Study" Journal of Personalized Medicine 12, no. 5: 706. https://doi.org/10.3390/jpm12050706