
Effectiveness of Multicomponent Home-Based Rehabilitation in Elderly Patients after Hip Fracture Surgery: A Randomized Controlled Trial



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Ethical Approval
2.3. Participants
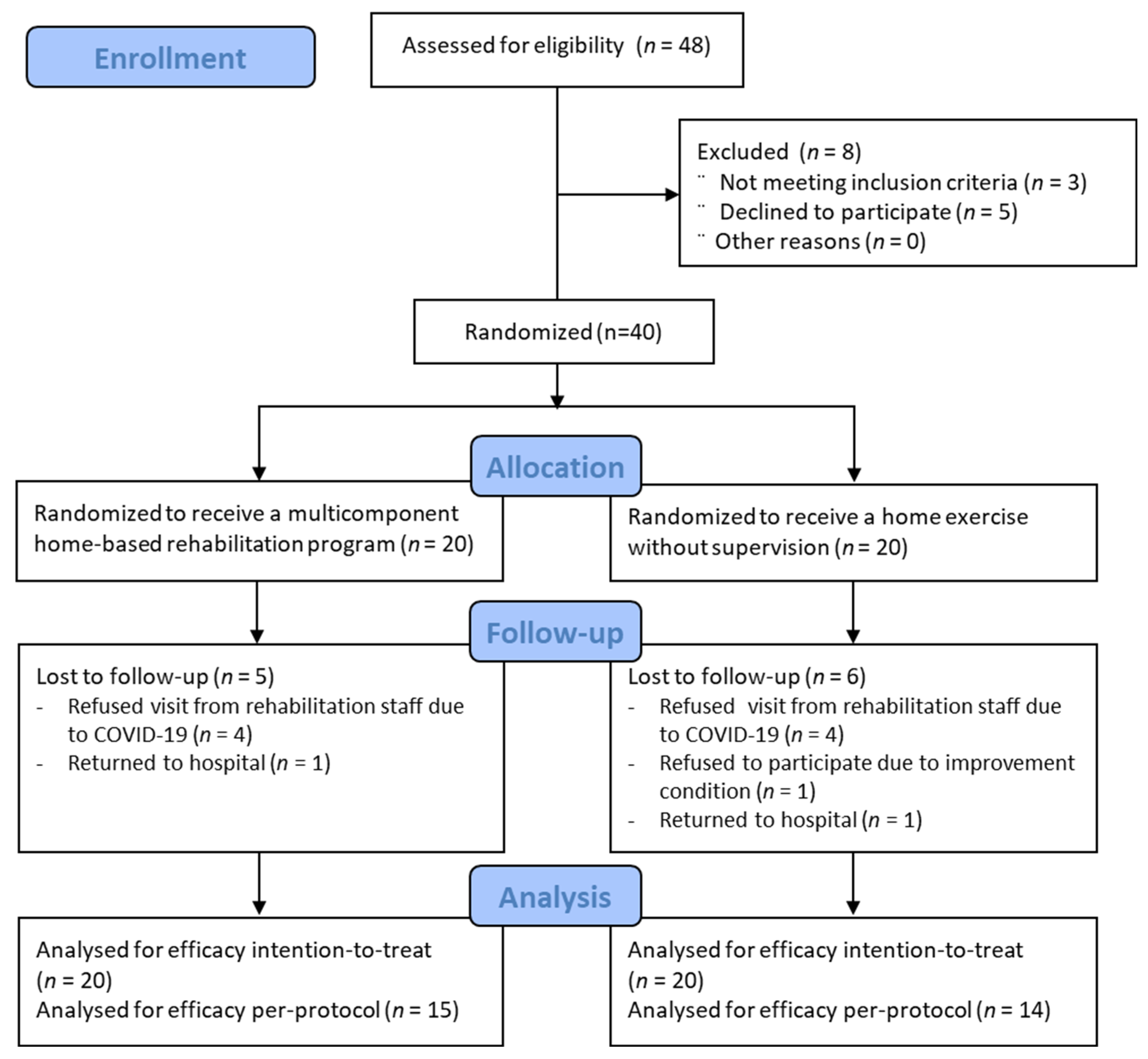
2.4. Randomization and Blinding
2.5. Intervention
2.6. Outcome Measures
2.7. Sample Size
2.8. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rapp, K.; Büchele, G.; Dreinhöfer, K.; Bücking, B.; Becker, C.; Benzinger, P. Epidemiology of hip fractures. Z. Gerontol. Geriatr. 2019, 52, 10–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Negrete-Corona, J.; Alvarado-Soriano, J.; Reyes-Santiago, L.J.A.o.m. Hip fracture as risk factor for mortality in patients over 65 years of age. Case Control Study 2014, 28, 352–362. [Google Scholar]
- Chen, J.; Zhu, X.; Jiang, J.; Qi, Y.; Shi, Y. Needs of Chinese patients undergoing home-based rehabilitation after hip replacement: A qualitative study. PLoS ONE 2019, 14, e0220304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.; Lee, S.H. Analysis of Home-Based Rehabilitation Awareness, Needs and Preferred Components of Elderly Patients with Hip Fracture Surgery in South Korea. Int. J. Environ. Res. Public Health 2021, 18, 7632. [Google Scholar] [CrossRef] [PubMed]
- Invernizzi, M.; de Sire, A.; D’Andrea, F.; Carrera, D.; Renò, F.; Migliaccio, S.; Iolascon, G.; Cisari, C. Effects of essential amino acid supplementation and rehabilitation on functioning in hip fracture patients: A pilot randomized controlled trial. Aging Clin. Exp. Res. 2019, 31, 1517–1524. [Google Scholar] [CrossRef]
- Tian, Y.; Zhu, Y.; Zhang, K.; Tian, M.; Qin, S.; Li, X.; Zhang, Y. Incidence and risk factors for postoperative pneumonia following surgically treated hip fracture in geriatric patients: A retrospective cohort study. J. Orthop. Surg. Res. 2022, 17, 179. [Google Scholar] [CrossRef]
- Mehta, S.P.; Roy, J.-S. Systematic review of home physiotherapy after hip fracture surgery. J. Rehabil. Med. 2011, 43, 477–480. [Google Scholar] [CrossRef] [Green Version]
- Salpakoski, A.; Törmäkangas, T.; Edgren, J.; Kallinen, M.; Sihvonen, S.E.; Pesola, M.; Vanhatalo, J.; Arkela, M.; Rantanen, T.; Sipilä, S. Effects of a multicomponent home-based physical rehabilitation program on mobility recovery after hip fracture: A randomized controlled trial. J. Am. Med. Dir. Assoc. 2014, 15, 361–368. [Google Scholar] [CrossRef] [Green Version]
- Okamoto, T.; Ridley, R.J.; Edmondston, S.J.; Visser, M.; Headford, J.; Yates, P.J. Day-of-surgery mobilization reduces the length of stay after elective hip arthroplasty. J. Arthroplast. 2016, 31, 2227–2230. [Google Scholar] [CrossRef]
- Karlsson, Å.; Lindelöf, N.; Olofsson, B.; Berggren, M.; Gustafson, Y.; Nordström, P.; Stenvall, M. Effects of geriatric interdisciplinary home rehabilitation on independence in activities of daily living in older people with hip fracture: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2020, 101, 571–578. [Google Scholar] [CrossRef] [Green Version]
- Wu, D.; Zhu, X.; Zhang, S. Effect of home-based rehabilitation for hip fracture: A meta-analysis of randomized controlled trials. J. Rehabil. Med. 2018, 50, 481–486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edgren, J.; Salpakoski, A.; Sihvonen, S.E.; Portegijs, E.; Kallinen, M.; Arkela, M.; Jäntti, P.; Vanhatalo, J.; Pekkonen, M.; Rantanen, T.; et al. Effects of a home-based physical rehabilitation program on physical disability after hip fracture: A randomized controlled trial. J. Am. Med. Dir. Assoc. 2015, 16, e351–e357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hill, K.D.; Hunter, S.W.; Batchelor, F.A.; Cavalheri, V.; Burton, E. Individualized home-based exercise programs for older people to reduce falls and improve physical performance: A systematic review and meta-analysis. Maturitas 2015, 82, 72–84. [Google Scholar] [CrossRef]
- Kuijlaars, I.A.; Sweerts, L.; Nijhuis-van der Sanden, M.W.; van Balen, R.; Staal, J.B.; van Meeteren, N.L.; Hoogeboom, T.J. Effectiveness of supervised home-based exercise therapy compared to a control intervention on functions, activities, and participation in older patients after hip fracture: A systematic review and meta-analysis. Arch. Phys. Med. Rehabil. 2019, 100, 101–114.e106. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Lee, S.H. Effectiveness of multicomponent home-based rehabilitation in older patients after hip fracture surgery: A systematic review and meta-analysis. J. Clin. Nurs. 2022, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Giusti, A.; Barone, A.; Oliveri, M.; Pizzonia, M.; Razzano, M.; Palummeri, E.; Pioli, G. An analysis of the feasibility of home rehabilitation among elderly people with proximal femoral fractures. Arch. Phys. Med. Rehabil. 2006, 87, 826–831. [Google Scholar] [CrossRef]
- Berggren, M.; Karlsson, Å.; Lindelöf, N.; Englund, U.; Olofsson, B.; Nordström, P.; Gustafson, Y.; Stenvall, M. Effects of geriatric interdisciplinary home rehabilitation on complications and readmissions after hip fracture: A randomized controlled trial. Clin. Rehabil. 2019, 33, 64–73. [Google Scholar] [CrossRef]
- Shyu, Y.I.; Liang, J.; Tseng, M.Y.; Li, H.J.; Wu, C.C.; Cheng, H.S.; Chou, S.W.; Chen, C.Y.; Yang, C.T. Enhanced interdisciplinary care improves self-care ability and decreases emergency department visits for older Taiwanese patients over 2 years after hip-fracture surgery: A randomised controlled trial. Int. J. Nurs. Stud. 2016, 56, 54–62. [Google Scholar] [CrossRef]
- Skivington, K.; Matthews, L.; Simpson, S.A.; Craig, P.; Baird, J.; Blazeby, J.M.; Boyd, K.A.; Craig, N.; French, D.P.; McIntosh, E.; et al. A new framework for developing and evaluating complex interventions: Update of Medical Research Council guidance. BMJ 2021, 374, n2061. [Google Scholar] [CrossRef]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.J.; Elbourne, D.; Egger, M.; Altman, D.G. CONSORT 2010 Explanation and Elaboration: Updated guidelines for reporting parallel group randomised trials. J. Clin. Epidemiol. 2010, 63, e1–e37. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taraldsen, K.; Thingstad, P.; Døhl, Ø.; Follestad, T.; Helbostad, J.L.; Lamb, S.E.; Saltvedt, I.; Sletvold, O.; Halsteinli, V. Short and long-term clinical effectiveness and cost-effectiveness of a late-phase community-based balance and gait exercise program following hip fracture. The EVA-Hip Randomised Controlled Trial. PLoS ONE 2019, 14, e0224971. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thingstad, P.; Taraldsen, K.; Hagen, G.; Sand, S.; Saltvedt, I.; Sletvold, O.; Helbostad, J.L. Effectiveness of task specific gait and balance exercise 4 months after hip fracture: Protocol of a randomized controlled trial--the Eva-hip study. Physiother. Res. Int. J. Res. Clin. Phys. Ther. 2015, 20, 87–99. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.C.; Lai, J.I.; Lu, M.C.; Lin, K.H.; Wang, W.S.; Lo, S.S.; Lai, Y.C. Reduction in the incidence of pneumonia in elderly patients after hip fracture surgery: An inpatient pulmonary rehabilitation program. Medicine 2018, 97, e11845. [Google Scholar] [CrossRef]
- Sherrington, C.; Lord, S.R. Reliability of simple portable tests of physical performance in older people after hip fracture. Clin. Rehabil. 2005, 19, 496–504. [Google Scholar] [CrossRef]
- Duncan, P.W.; Weiner, D.K.; Chandler, J.; Studenski, S. Functional reach: A new clinical measure of balance. J. Gerontol. 1990, 45, M192–M197. [Google Scholar] [CrossRef]
- De Waroquier-Leroy, L.; Bleuse, S.; Serafi, R.; Watelain, E.; Pardessus, V.; Tiffreau, A.V.; Thevenon, A. The Functional Reach Test: Strategies, performance and the influence of age. Ann. Phys. Rehabil. Med. 2014, 57, 452–464. [Google Scholar] [CrossRef] [Green Version]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef]
- Ingemarsson, A.H.; Frändin, K.; Mellström, D.; Möller, M. Walking ability and activity level after hip fracture in the elderly—A follow-up. J. Rehabil. Med. 2003, 35, 76–83. [Google Scholar] [CrossRef] [Green Version]
- Bohannon, R.W. Reference values for the timed up and go test: A descriptive meta-analysis. J. Geriatr. Phys. Ther. 2006, 29, 64–68. [Google Scholar] [CrossRef] [Green Version]
- Shumway-Cook, A.; Brauer, S.; Woollacott, M. Predicting the probability for falls in community-dwelling older adults using the Timed Up & Go Test. Phys. Ther. 2000, 80, 896–903. [Google Scholar] [PubMed] [Green Version]
- Visser, M.; Harris, T.B.; Fox, K.M.; Hawkes, W.; Hebel, J.R.; YuYahiro, J.; Michael, R.; Zimmerman, S.I.; Magaziner, J. Change in Muscle Mass and Muscle Strength After a Hip Fracture: Relationship to Mobility Recovery. J. Gerontol. Ser. A 2000, 55, M434–M440. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Shinkai, S. Prevalence of muscle weakness based on different diagnostic criteria in community-dwelling older adults: A comparison of grip strength dynamometers. Geriatr. Gerontol. Int. 2017, 17, 2089–2095. [Google Scholar] [CrossRef] [PubMed]
- Breivik, H.; Borchgrevink, P.C.; Allen, S.M.; Rosseland, L.A.; Romundstad, L.; Hals, E.K.; Kvarstein, G.; Stubhaug, A. Assessment of pain. Br. J. Anaesth. 2008, 101, 17–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez, C.S. Pain measurement in the elderly: A review. Pain Manag. Nurs. Off. J. Am. Soc. Pain Manag. Nurses 2001, 2, 38–46. [Google Scholar] [CrossRef]
- Jung, H.Y.; Park, B.K.; Shin, H.S.; Kang, Y.K.; Pyun, S.B.; Paik, N.J.; Kim, S.H.; Kim, T.H.; Han, T.R. Development of the Korean version of Modified Barthel Index (K-MBI): Multi-center study for subjects with stroke. J. Korean Acad. Rehabil. Med. 2007, 31, 283–297. [Google Scholar]
- Unnanuntana, A.; Jarusriwanna, A.; Nepal, S. Validity and responsiveness of Barthel index for measuring functional recovery after hemiarthroplasty for femoral neck fracture. Arch. Orthop. Trauma Surg. 2018, 138, 1671–1677. [Google Scholar] [CrossRef]
- Park, G.; Cho, B.; Kwon, I.S.; Park, B.J.; Kim, T.; Cho, K.Y.; Park, U.J.; Kim, M.J. Reliability and validity of Korean version of falls efficacy scale-international (KFES-I). J. Korean Acad. Rehabil. Med. 2010, 34, 554–559. [Google Scholar]
- Kumar, S.; Vendhan, G.V.; Awasthi, S.; Tiwari, M.; Sharma, V. Relationship between fear of falling, balance impairment and functional mobility in community dwelling elderly. Indian. J. Phys. Med. Rehabil. 2008, 19, 48–52. [Google Scholar]
- Tinetti, M.E.; Richman, D.; Powell, L. Falls efficacy as a measure of fear of falling. J. Gerontol. 1990, 45, P239–P243. [Google Scholar] [CrossRef]
- Han, C.W.; Lee, E.J.; Iwaya, T.; Kataoka, H.; Kohzuki, M. Development of the Korean version of Short-Form 36-Item Health Survey: Health related QOL of healthy elderly people and elderly patients in Korea. Tohoku J. Exp. Med. 2004, 203, 189–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ware, J.E., Jr.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E., Jr. SF-36 health survey update. Spine 2000, 25, 3130–3139. [Google Scholar] [CrossRef] [PubMed]
- Noh, S.; Kaspar, V.; Chen, X. Measuring depression in Korean immigrants: Assessing validity of the translated Korean version of CES-D scale. Cross Cult. Res. 1998, 32, 358–377. [Google Scholar] [CrossRef]
- Radloff, L.S. The CES-D Scale: A Self-Report Depression Scale for Research in the General Population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Zidén, L.; Kreuter, M.; Frändin, K. Long-term effects of home rehabilitation after hip fracture—1-year follow-up of functioning, balance confidence, and health-related quality of life in elderly people. Disabil. Rehabil. 2010, 32, 18–32. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: London, UK, 2013. [Google Scholar]
- Doll, H.; Gentile, B.; Bush, E.N.; Ballinger, R. Evaluation of the Measurement Properties of Four Performance Outcome Measures in Patients with Elective Hip Replacements, Elective Knee Replacements, or Hip Fractures. Value Health J. Int. Soc. Pharm. Outcomes Res. 2018, 21, 1104–1114. [Google Scholar] [CrossRef] [Green Version]
- Crotty, M.; Whitehead, C.; Miller, M.; Gray, S. Patient and caregiver outcomes 12 months after home-based therapy for hip fracture: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2003, 84, 1237–1239. [Google Scholar] [CrossRef]
- Tsauo, J.Y.; Leu, W.S.; Chen, Y.T.; Yang, R.S. Effects on function and quality of life of postoperative home-based physical therapy for patients with hip fracture. Arch. Phys. Med. Rehabil. 2005, 86, 1953–1957. [Google Scholar] [CrossRef]
- Min, K.; Beom, J.; Kim, B.R.; Lee, S.Y.; Lee, G.J.; Lee, J.H.; Lee, S.Y.; Won, S.J.; Ahn, S.; Bang, H.J.; et al. Clinical Practice Guideline for Postoperative Rehabilitation in Older Patients with Hip Fractures. Ann. Rehabil. Med. 2021, 45, 225–259. [Google Scholar] [CrossRef]
- Elmer, T.; Stadtfeld, C. Depressive symptoms are associated with social isolation in face-to-face interaction networks. Sci. Rep. 2020, 10, 1444. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| MHR Group (n = 20) | Home Exercise Group (n = 20) | p-Value | |
|---|---|---|---|
| Age, years | 78.9 ± 11.7 | 74.3 ± 9.2 | 0.174 |
| Women, n (%) | 15 (75.0) | 15 (75.0) | |
| Height, cm | 158.3 ± 9.3 | 155.2 ± 7.3 | 0.260 |
| Weight, kg | 55.4 ± 8.7 | 53.8 ± 10.3 | 0.612 |
| BMI, kg/m2 | 22.0 ± 3.1 | 22.2 ± 3.4 | 0.926 |
| Living status, n (%) | 0.999 | ||
| Living alone | 2 (10.0) | 2 (10.0) | |
| Living with family | 18 (90.0) | 18 (90.0) | |
| Time since surgery, days | 55.0 ± 36.3 | 63.1 ± 26.2 | 0.439 |
| Involved side, n (%) | 0.337 | ||
| Right | 13 (65.0) | 10 (50.0) | |
| Left | 7 (35.0) | 10 (50.0) | |
| Type of surgery, n (%) | 0.109 | ||
| Internal fixation | 5 (25.0) | 11 (55.0) | |
| Total hip arthroplasty | 12 (60.0) | 7 (35.0) | |
| Hemi arthroplasty | 3 (15.0) | 2 (10.0) | |
| Function Reach Test, cm | 17.5 ± 8.1 | 18.9 ± 8.0 | 0.616 |
| Timed Up-and-Go Test, sec | 37.1 ± 10.5 | 34.3 ± 7.8 | 0.365 |
| Pain Numeric Rating Scale (0–10) | 4.9 ± 1.3 | 4.6 ± 1.5 | 0.551 |
| Modified Barthel Index (0–100) | 67.4 ± 23.6 | 78.7 ± 20.5 | 0.120 |
| Fall Efficacy Scale (0–100) | 53.4 ± 26.2 | 45.7 ± 18.6 | 0.304 |
| Short Form 36 | |||
| Physical Component Score (0–100) | 31.5 ± 9.7 | 37.3 ± 13.7 | 0.133 |
| Mental Component Score (0–100) | 40.6 ± 8.1 | 46.4 ± 14.4 | 0.123 |
| Center for Epidemiological Studies Depression Scale (0–60) | 28.7 ± 15.3 | 15.5 ±13.9 | 0.003 |
| Muscle strength | |||
| Hip flexor, kg | 49.5 ± 15.2 | 51.1 ± 12.3 | 0.720 |
| Hip abductor, kg | 57.2 ± 16.3 | 59.2 ± 12.9 | 0.671 |
| Knee flexor, kg | 54.6 ± 16.9 | 60.5 ± 15.6 | 0.267 |
| Knee extensor, kg | 63.5 ± 15.8 | 70.6 ± 15.6 | 0.165 |
| Grip strength, kg | 16.6 ± 4.7 | 17.0 ± 4.2 | 0.770 |
| Mean ± SD | Change from Baseline, Mean (95% CI) | Time × Group Interaction | |||
|---|---|---|---|---|---|
| Week 4 | Week 8 | Week 4 | Week 8 | ||
| FRT (cm) | |||||
| MHR group | 21.4 ± 8.0 | 25.1 ± 9.6 | −3.1 (−4.5 to −1.7) | −6.8 (−9.8 to −3.7) | |
| Home exercise group | 21.1 ± 7.3 | 22.8 ± 7.7 | −0.7 (−1.5 to −0.0) | −2.4 (−4.2 to −0.6) | |
| MHR vs. home exercise | 2.4 (0.9 to 3.9) | 4.4 (1.0 to 7.8) | 0.015 | ||
| TUG (s) | |||||
| MHR group | 29.1 ± 10.9 | 24.8 ± 10.0 | 8.0 (5.7 to 10.3) | 12.3 (8.9 to 15.7) | |
| Home exercise group | 29.0 ± 9.1 | 26.6 ± 7.6 | 5.2 (3.0 to 7.5) | 8.2 (5.8 to 10.5) | |
| MHR vs. home exercise | −2.8 (−5.9 to 0.3) | −4.2 (−8.0 to −0.3) | 0.036 | ||
| Mean ± SD | Change from Baseline, Mean (95% CI) | Time × Group Interaction | |||
|---|---|---|---|---|---|
| Week 4 | Week 8 | Week 4 | Week 8 | ||
| Pain NRS (0–10) | |||||
| MHR group | 3.3 ± 1.5 | 2.4 ± 1.6 | 1.6 (1.0 to 2.2) | 2.5 (1.8 to 3.1) | |
| Home exercise group | 3.3 ± 1.4 | 3.1 ± 1.6 | 1.2 (0.6 to 1.8) | 1.5 (0.8 to 2.1) | |
| MHR vs. home exercise | −0.3 (−1.1 to 0.6) | −0.9 (−1.7 to −0.0) | 0.050 | ||
| K-MBI (0–100) | |||||
| MHR group | 73.9 ± 20.2 | 80.5 ± 17.8 | −6.5 (−11.4 to −1.6) | −13.1 (−18.4 to −7.7) | |
| Home exercise group | 80.8 ± 17.6 | 87.8 ± 14.9 | −2.2 (−7.2 to 2.9) | −9.1 (−16.3 to −1.9) | |
| MHR vs. home exercise | 4.3 (−2.5 to 11.1) | 3.9 (−4.6 to 12.5) | 0.425 | ||
| K-FES (0–100) | |||||
| MHR group | 41.6 ± 27.1 | 33.9 ± 26.5 | 10.3 (4.6 to 16.1) | 17.0 (10.7 to 23.3) | |
| Home exercise group | 35.3 ± 19.8 | 30.5 ± 15.1 | 10.2 (2.5 to 17.9) | 14.9 (8.0 to 21.8) | |
| MHR vs. home exercise | −1.3 (−9.1 to 8.9) | −2.1 (−11.0 to 6.9) | 0.893 | ||
| K-SF-36 (PCS) (0–100) | |||||
| MHR group | 38.7 ± 12.6 | 44.5 ± 16.9 | −7.2 (−10.8 to −3.6) | −13.1 (−18.3 to −7.7) | |
| Home exercise group | 40.0 ± 14.7 | 42.6 ± 14.4 | −2.7 (−5.8 to 0.3) | −5.3 (−8.9 to −1.6) | |
| MHR vs. home exercise | 4.5 (0.0 to 9.1) | 7.8 (1.5 to 14.1) | 0.017 | ||
| K-SF-36 (MCS) (0–100) | |||||
| MHR group | 49.6 ± 9.5 | 52.5 ± 10.4 | −9.0 (−13.0 to −5.1) | −11.9 (−16.7 to −7.3) | |
| Home exercise group | 52.3 ± 13.9 | 53.9 ± 12.9 | −5.9 (−9.7 to −2.1) | −7.5 (−12.2 to −2.8) | |
| MHR vs. home exercise | 3.1 (−2.2 to 8.5) | 4.5 (−1.9 to 10.9) | 0.242 | ||
| K-CES-D (0–60) | |||||
| MHR group | 16.1 ± 9.8 | 11.2 ± 7.7 | 12.6 (6.8 to 18.3) | 17.5 (12.0 to 23.0) | |
| Home exercise group | 12.9 ± 12.1 | 9.2 ± 8.7 | 1.1 (−3.4 to 5.6) | 4.1 (−1.0 to 9.1) | |
| MHR vs. home exercise | −11.4 (−18.5 to −4.4) | −13.4 (−20.7 to −6.1) | 0.001/0.201 † | ||
| Muscle strength | |||||
| Hip flexor (kg) | |||||
| MHR group | 61.3 ± 24.6 | 73.7 ± 25.1 | −11.9 (−20.9 to −2.9) | −24.2 (−34.6 to −13.9) | |
| Home exercise group | 59.9 ± 22.3 | 65.3 ± 21.2 | −8.9 (−16.9 to −0.8) | −14.3 (−22.5 to −6.0) | |
| MHR vs. home exercise | 3.0 (−8.8 to 14.7) | 9.9 (−2.9 to 22.8) | 0.183 | ||
| Hip abductor (kg) | |||||
| MHR group | 65.9 ± 22.0 | 76.4 ± 27.5 | −8.7 (−15.2 to −2.1) | −19.2 (−27.9 to −10.6) | |
| Home exercise group | 66.9 ± 19.1 | 71.6 ± 21.5 | −7.8 (−14.9 to −0.6) | −12.4 (−21.3 to −3.6) | |
| MHR vs. home exercise | 0.9 (−8.4 to 10.3) | 6.8 (−5.2 to 18.8) | 0.315 | ||
| Knee flexor (kg) | |||||
| MHR group | 70.7 ± 29.8 | 79.4 ± 30.2 | −16.1 (−27.7 to −4.5) | −24.8 (−35.0 to −15.5) | |
| Home exercise group | 69.7 ± 22.5 | 73..8 ±17.5 | −9.2 (−17.2 to −1.3) | −13.3 (−20.6 to −6.1) | |
| MHR vs. home exercise | 6.9 (−6.9 to 20.6) | 11.5 (0.8 to 23.7) | 0.167 | ||
| Knee extensor (kg) | |||||
| MHR group | 76.2 ± 29.5 | 91.2 ± 38.7 | −12.7 (−22.9 to −2.6) | −27.7 (−14.5 to −13.9) | |
| Home exercise group | 77.1 ± 22.0 | 85.1 ± 18.2 | −6.5 (−14.1 to 1.0) | −14.6 (−23.4 to −5.8) | |
| MHR vs. home exercise | 6.2 (−6.1 to 18.4) | 13.1 (−2.8 to 29.1) | 0.185 | ||
| Grip strength (kg) | |||||
| MHR group | 17.6 ± 5.7 | 19.1 ± 4.3 | −0.9 (−3.0 to 1.1) | −2.5 (−4.2 to −0.8) | |
| Home exercise group | 17.8 ± 6.5 | 18.5 ± 6.1 | −0.8 (−2.8 to 1.3) | −1.6 (−4.3 to −1.2) | |
| MHR vs. home exercise | 0.2 (−2.6 to 3.0) | 0.9 (−2.2 to 4.0) | 0.789 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.; Lee, S.-H. Effectiveness of Multicomponent Home-Based Rehabilitation in Elderly Patients after Hip Fracture Surgery: A Randomized Controlled Trial. J. Pers. Med. 2022, 12, 649. https://doi.org/10.3390/jpm12040649
Lee H, Lee S-H. Effectiveness of Multicomponent Home-Based Rehabilitation in Elderly Patients after Hip Fracture Surgery: A Randomized Controlled Trial. Journal of Personalized Medicine. 2022; 12(4):649. https://doi.org/10.3390/jpm12040649
Chicago/Turabian StyleLee, Haneul, and Seon-Heui Lee. 2022. "Effectiveness of Multicomponent Home-Based Rehabilitation in Elderly Patients after Hip Fracture Surgery: A Randomized Controlled Trial" Journal of Personalized Medicine 12, no. 4: 649. https://doi.org/10.3390/jpm12040649