
Chemokine Expression-Based Endotype Clustering of Chronic Rhinosinusitis


 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Patients’ Material
2.3. Measurement of Inflammatory Markers
- negative IL-5 level when under the concentration of 12.98 pg/mL (assay detection limit)
- low IL-5 level (IL-5 < 100 pg/mL)
- moderate IL-5 level (IL-5 100 to 151 pg/mL)
- high IL-5 level (IL-5 > 151 pg/mL)
2.4. Statistical Methods
3. Results
3.1. Comparison of CRS and Control Subjects
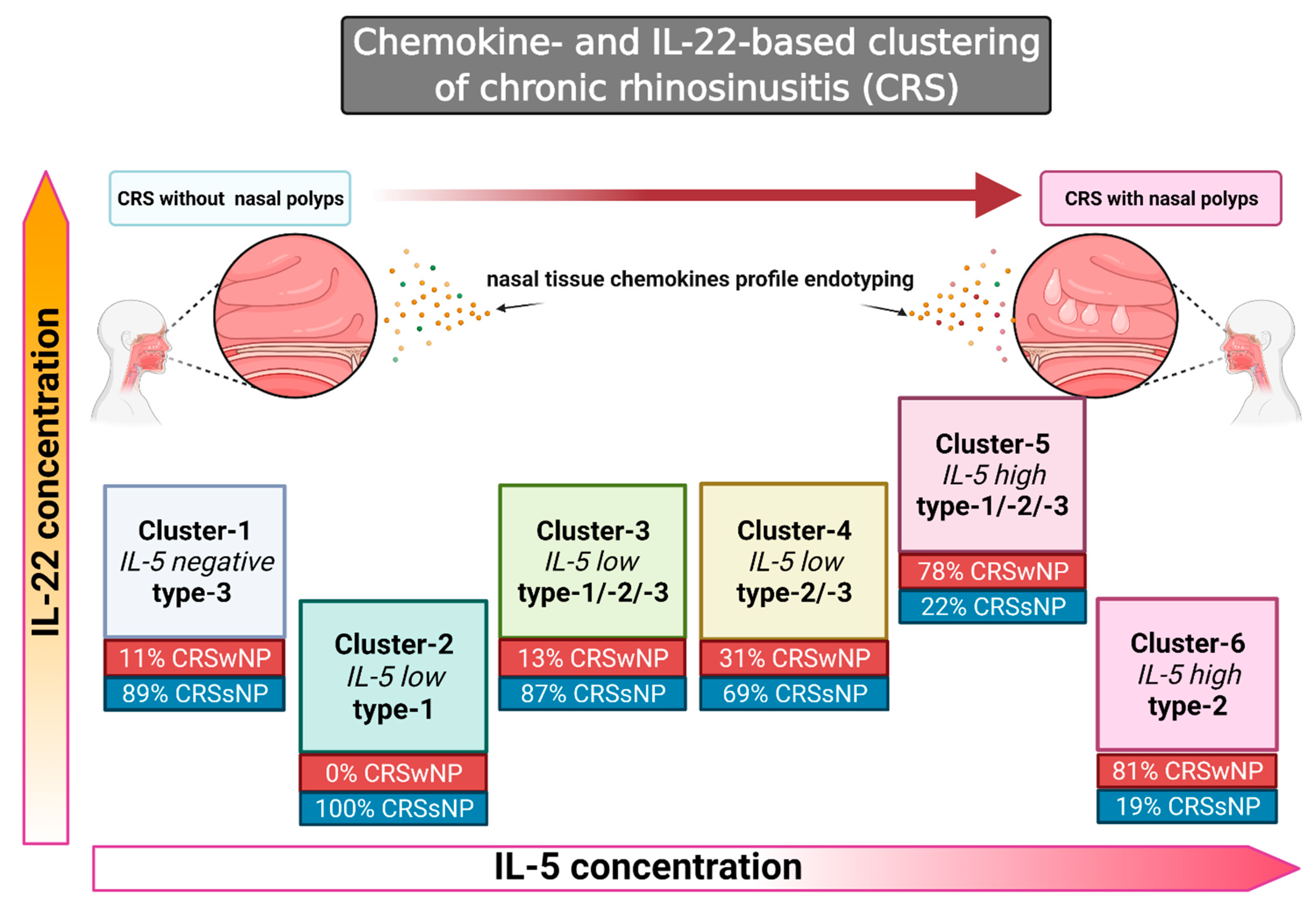
3.2. Cluster Analysis Reveals Six Clusters of the Chemokine Expression Pattern
3.3. Negative or Low IL-5 Concentration Found in Clusters 1–4
Characterization of Clusters
- Cluster-1 (9 CRS cases): No significant differences were detected between the chemokine levels. The concentration of IL-22 (type-3) was significantly higher than in ≥2 clusters (noninflammatory/type-3-based pattern).
- Cluster-2 (11 CRS cases): ENA-78 (neutrophilic parameter), and IP-10 (expressed by type-1) were significantly higher than in ≥2 clusters (neutrophilic, type-1-based inflammatory pattern).
- Cluster-3 (8 CRS cases): The IP-10, MCP-3 (type-1/type-2), and MIP-1α (type-1/type-2) concentrations were significantly higher than in ≥4 clusters. The levels of ENA-78 and type-2-related chemokines TARC and PARC were significantly higher than in the two or more other clusters. IL-22 was significantly higher than in two or more other clusters (mixed neutrophilic type-1- > type-2-, type-3- inflammatory pattern).
- Cluster-4 (13 CRS cases): The concentrations of type-2-related chemokines TARC and PARC were significantly higher than in two or more clusters. ENA-78 was increased significantly compared to two or more other clusters. The concentration of MPO (neutrophilic) was higher than in three or more other clusters, and IL-22 was higher than in two or more other clusters (neutrophilic > type-2 > type-3 inflammatory pattern).
3.4. Association of Endotypes with Phenotypes in Clusters 1–4
3.5. High Concentrations of IL-5: Clusters 5 and 6
- Cluster-5 (9 CRS cases): The levels of type-2 related chemokines eotaxin, TARC, and PARC were significantly higher than in four or more clusters. The concentration of MCP-3 was higher than in two other clusters, and MIP-1α was significantly higher than in four or more clusters (type-1, type-2). MPO and IL-22 (type-3) were significantly elevated (three or more other clusters), SAE (type-2) (not included in the cluster analysis) was present (strong Th1/Th2/Th3-pattern).
- Cluster-6 (16 CRS cases): The levels of PARC and eotaxin (four or more other clusters), as well as TARC (two or more other clusters), were significantly elevated. In contrast, no increased concentrations of MCP-3, MIP-1α, ENA-78, or IP-10 were noted. SAE (not included in the cluster analysis) was detected (type-2 inflammatory pattern).
3.6. Association of Endotypes with Phenotypes in Clusters 5 and 6
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bachert, C.; Hellings, P.W.; Mullol, J.; Hamilos, D.L.; Gevaert, P.; Naclerio, R.M.; Joish, V.N.; Chao, J.; Mannent, L.P.; Amin, N.; et al. Dupilumab improves health-related quality of life in patients with chronic rhinosinusitis with nasal polyposis. Allergy 2020, 75, 148–157. [Google Scholar] [CrossRef] [PubMed]
- Fokkens, W.J.; Lund, V.J.; Hopkins, C.; Hellings, P.W.; Kern, R.; Reitsma, S.; Toppila-Salmi, S.; Bernal-Sprekelsen, M.; Mullol, J. Executive summary of EPOS 2020 including integrated care pathways. Rhinology 2020, 58, 82–111. [Google Scholar] [CrossRef]
- Hastan, D.; Fokkens, W.J.; Bachert, C.; Newson, R.B.; Bislimovska, J.; Bockelbrink, A.; Bousquet, P.J.; Brozek, G.; Bruno, A.; Dahlen, S.E.; et al. Chronic rhinosinusitis in Europe--an underestimated disease. A GA(2)LEN study. Allergy 2011, 66, 1216–1223. [Google Scholar] [CrossRef] [PubMed]
- Jarvis, D.; Newson, R.; Lotvall, J.; Hastan, D.; Tomassen, P.; Keil, T.; Gjomarkaj, M.; Forsberg, B.; Gunnbjornsdottir, M.; Minov, J.; et al. Asthma in adults and its association with chronic rhinosinusitis: The GA2LEN survey in Europe. Allergy 2012, 67, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Tomassen, P.; Vandeplas, G.; Van Zele, T.; Cardell, L.O.; Arebro, J.; Olze, H.; Forster-Ruhrmann, U.; Kowalski, M.L.; Olszewska-Ziaber, A.; Holtappels, G.; et al. Inflammatory endotypes of chronic rhinosinusitis based on cluster analysis of biomarkers. J Allergy Clin. Immunol. 2016, 137, 1449–1456.e1444. [Google Scholar] [CrossRef] [Green Version]
- Zhang, N.; Van Zele, T.; Perez-Novo, C.; Van Bruaene, N.; Holtappels, G.; DeRuyck, N.; Van Cauwenberge, P.; Bachert, C. Different types of T-effector cells orchestrate mucosal inflammation in chronic sinus disease. J. Allergy Clin. Immunol. 2008, 122, 961–968. [Google Scholar] [CrossRef]
- Delemarre, T.; Bochner, B.S.; Simon, H.U.; Bachert, C. Rethinking neutrophils and eosinophils in chronic rhinosinusitis. J. Allergy Clin. Immunol. 2021, 148, 327–335. [Google Scholar] [CrossRef]
- Wang, M.; Zhang, N.; Zheng, M.; Li, Y.; Meng, L.; Ruan, Y.; Han, J.; Zhao, N.; Wang, X.; Zhang, L.; et al. Cross-talk between TH2 and TH17 pathways in patients with chronic rhinosinusitis with nasal polyps. J. Allergy Clin. Immunol. 2019, 144, 1254–1264. [Google Scholar] [CrossRef] [Green Version]
- Vivier, E.; Artis, D.; Colonna, M.; Diefenbach, A.; Di Santo, J.P.; Eberl, G.; Koyasu, S.; Locksley, R.M.; McKenzie, A.N.J.; Mebius, R.E.; et al. Innate Lymphoid Cells: 10 Years On. Cell 2018, 174, 1054–1066. [Google Scholar] [CrossRef] [Green Version]
- Ouyang, W.; O’Garra, A. IL-10 Family Cytokines IL-10 and IL-22: From Basic Science to Clinical Translation. Immunity 2019, 50, 871–891. [Google Scholar] [CrossRef]
- Eyerich, K.; Dimartino, V.; Cavani, A. IL-17 and IL-22 in immunity: Driving protection and pathology. Eur. J. Immunol. 2017, 47, 607–614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malhotra, N.; Yoon, J.; Leyva-Castillo, J.M.; Galand, C.; Archer, N.; Miller, L.S.; Geha, R.S. IL-22 derived from γδ T cells restricts Staphylococcus aureus infection of mechanically injured skin. J. Allergy Clin. Immunol. 2016, 138, 1098–1107.e1093. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stevens, W.W.; Peters, A.T.; Tan, B.K.; Klingler, A.I.; Poposki, J.A.; Hulse, K.E.; Grammer, L.C.; Welch, K.C.; Smith, S.S.; Conley, D.B.; et al. Associations Between Inflammatory Endotypes and Clinical Presentations in Chronic Rhinosinusitis. J. Allergy Clin. Immunol. Pract. 2019, 7, 2812–2820.e2813. [Google Scholar] [CrossRef]
- Vaitkus, J.; Vitkauskienė, A.; Simuntis, R.; Vaitkus, Ž.; Šiupšinskienė, N.; Vaitkus, S. Chronic Rhinosinusitis with Nasal Polyps: Age and Disease Severity Differences in the Levels of Inflammatory Markers. Medicina 2021, 57, 282. [Google Scholar] [CrossRef] [PubMed]
- Carsuzaa, F.; Béquignon, É.; Dufour, X.; de Bonnecaze, G.; Lecron, J.C.; Favot, L. Cytokine Signature and Involvement in Chronic Rhinosinusitis with Nasal Polyps. Int. J. Mol. Sci. 2021, 23, 417. [Google Scholar] [CrossRef]
- Bachert, C.; Han, J.K.; Desrosiers, M.; Hellings, P.W.; Amin, N.; Lee, S.E.; Mullol, J.; Greos, L.S.; Bosso, J.V.; Laidlaw, T.M.; et al. Efficacy and safety of dupilumab in patients with severe chronic rhinosinusitis with nasal polyps (LIBERTY NP SINUS-24 and LIBERTY NP SINUS-52): Results from two multicentre, randomised, double-blind, placebo-controlled, parallel-group phase 3 trials. Lancet 2019, 394, 1638–1650. [Google Scholar] [CrossRef] [Green Version]
- Gevaert, P.; Omachi, T.A.; Corren, J.; Mullol, J.; Han, J.; Lee, S.E.; Kaufman, D.; Ligueros-Saylan, M.; Howard, M.; Zhu, R.; et al. Efficacy and safety of omalizumab in nasal polyposis: 2 randomized phase 3 trials. J. Allergy Clin. Immunol. 2020, 146, 595–605. [Google Scholar] [CrossRef]
- Han, J.K.; Bachert, C.; Fokkens, W.; Desrosiers, M.; Wagenmann, M.; Lee, S.E.; Smith, S.G.; Martin, N.; Mayer, B.; Yancey, S.W.; et al. Mepolizumab for chronic rhinosinusitis with nasal polyps (SYNAPSE): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Respir. Med. 2021, 9, 1141–1153. [Google Scholar] [CrossRef]
- Fokkens, W.J.; Lund, V.; Bachert, C.; Mullol, J.; Bjermer, L.; Bousquet, J.; Canonica, G.W.; Deneyer, L.; Desrosiers, M.; Diamant, Z.; et al. EUFOREA consensus on biologics for CRSwNP with or without asthma. Allergy 2019, 74, 2312–2319. [Google Scholar] [CrossRef] [Green Version]
- Bachert, C.; Han, J.K.; Wagenmann, M.; Hosemann, W.; Lee, S.E.; Backer, V.; Mullol, J.; Gevaert, P.; Klimek, L.; Prokopakis, E.; et al. EUFOREA expert board meeting on uncontrolled severe chronic rhinosinusitis with nasal polyps (CRSwNP) and biologics: Definitions and management. J. Allergy Clin. Immunol. 2021, 147, 29–36. [Google Scholar] [CrossRef]
- Rossi, D.; Zlotnik, A. The biology of chemokines and their receptors. Annu. Rev. Immunol. 2000, 18, 217–242. [Google Scholar] [CrossRef] [PubMed]
- Konig, K.; Klemens, C.; Haack, M.; Nicolo, M.S.; Becker, S.; Kramer, M.F.; Groger, M. Cytokine patterns in nasal secretion of non-atopic patients distinguish between chronic rhinosinusitis with or without nasal polys. Allergy Asthma Clin. Immunol. 2016, 12, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olze, H.; Forster, U.; Zuberbier, T.; Morawietz, L.; Luger, E.O. Eosinophilic nasal polyps are a rich source of eotaxin, eotaxin-2 and eotaxin-3. Rhinology 2006, 44, 145–150. [Google Scholar] [PubMed]
- Teplyakov, A.; Obmolova, G.; Gilliland, G.L. Structural insights into chemokine CCL17 recognition by antibody M116. Biochem. Biophys Rep. 2018, 13, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Peterson, S.; Poposki, J.A.; Nagarkar, D.R.; Chustz, R.T.; Peters, A.T.; Suh, L.A.; Carter, R.; Norton, J.; Harris, K.E.; Grammer, L.C.; et al. Increased expression of CC chemokine ligand 18 in patients with chronic rhinosinusitis with nasal polyps. J. Allergy Clin. Immunol. 2012, 129, 119–127.e1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wright, E.D.; Frenkiel, S.; Ghaffar, O.; al-Ghamdi, K.; Luster, A.; Miotto, D.; Hamid, Q. Monocyte chemotactic protein expression in allergy and non-allergy-associated chronic sinusitis. J. Otolaryngol. 1998, 27, 281–287. [Google Scholar]
- Yoshikawa, M.; Wada, K.; Yoshimura, T.; Asaka, D.; Okada, N.; Matsumoto, K.; Moriyama, H. Increased CXCL10 expression in nasal fibroblasts from patients with refractory chronic rhinosinusitis and asthma. Allergol. Int. 2013, 62, 495–502. [Google Scholar] [CrossRef] [Green Version]
- Rudack, C.; Sachse, F.; Alberty, J. Primary role of growth-related oncogene-alpha and granulocyte chemotactic protein-2 as neutrophil chemoattractants in chronic rhinosinusitis. Clin. Exp. Allergy 2006, 36, 748–759. [Google Scholar] [CrossRef]
- Bousquet, J.; Khaltaev, N.; Cruz, A.A.; Denburg, J.; Fokkens, W.J.; Togias, A.; Zuberbier, T.; Baena-Cagnani, C.E.; Canonica, G.W.; van Weel, C.; et al. Allergic Rhinitis and its Impact on Asthma (ARIA) 2008 update (in collaboration with the World Health Organization, GA(2)LEN and AllerGen). Allergy 2008, 63 (Suppl. S86), 8–160. [Google Scholar] [CrossRef]
- Wu, D.; Zhou, J.; Bi, H.; Li, L.; Gao, W.; Huang, M.; Adcock, I.M.; Barnes, P.J.; Yao, X. CCL11 as a potential diagnostic marker for asthma? J. Asthma. 2014, 51, 847–854. [Google Scholar] [CrossRef]
- Elsner, J.; Escher, S.E.; Forssmann, U. Chemokine receptor antagonists: A novel therapeutic approach in allergic diseases. Allergy 2004, 59, 1243–1258. [Google Scholar] [CrossRef] [PubMed]
- Elsner, J.; Hochstetter, R.; Kimmig, D.; Kapp, A. Human eotaxin represents a potent activator of the respiratory burst of human eosinophils. Eur. J. Immunol. 1996, 26, 1919–1925. [Google Scholar] [CrossRef] [PubMed]
- Maurer, M.; von Stebut, E. Macrophage inflammatory protein-1. Int. J. Biochem. Cell Biol. 2004, 36, 1882–1886. [Google Scholar] [CrossRef] [PubMed]
- Van Coillie, E.; Van Damme, J.; Opdenakker, G. The MCP/eotaxin subfamily of CC chemokines. Cytokine Growth Factor Rev. 1999, 10, 61–86. [Google Scholar] [CrossRef]
- Proost, P.; Van Leuven, P.; Wuyts, A.; Ebberink, R.; Opdenakker, G.; Van Damme, J. Chemical synthesis, purification and folding of the human monocyte chemotactic proteins MCP-2 and MCP-3 into biologically active chemokines. Cytokine 1995, 7, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Walz, A.; Schmutz, P.; Mueller, C.; Schnyder-Candrian, S. Regulation and function of the CXC chemokine ENA-78 in monocytes and its role in disease. J. Leukoc. Biol. 1997, 62, 604–611. [Google Scholar] [CrossRef] [Green Version]
- Islam, S.A.; Ling, M.F.; Leung, J.; Shreffler, W.G.; Luster, A.D. Identification of human CCR8 as a CCL18 receptor. J. Exp. Med. 2013, 210, 1889–1898. [Google Scholar] [CrossRef]
- Cai, M.; Bonella, F.; He, X.; Sixt, S.U.; Sarria, R.; Guzman, J.; Costabel, U. CCL18 in serum, BAL fluid and alveolar macrophage culture supernatant in interstitial lung diseases. Respir. Med. 2013, 107, 1444–1452. [Google Scholar] [CrossRef] [Green Version]
- Bellinghausen, I.; Reuter, S.; Martin, H.; Maxeiner, J.; Luxemburger, U.; Tureci, O.; Grabbe, S.; Taube, C.; Saloga, J. Enhanced production of CCL18 by tolerogenic dendritic cells is associated with inhibition of allergic airway reactivity. J. Allergy Clin. Immunol. 2012, 130, 1384–1393. [Google Scholar] [CrossRef]
- Mazzi, V.; Fallahi, P. Allergic rhinitis and CXCR3 chemokines. Clin. Ter. 2017, 168, e54–e58. [Google Scholar] [CrossRef]
- Medoff, B.D.; Sauty, A.; Tager, A.M.; Maclean, J.A.; Smith, R.N.; Mathew, A.; Dufour, J.H.; Luster, A.D. IFN-gamma-inducible protein 10 (CXCL10) contributes to airway hyperreactivity and airway inflammation in a mouse model of asthma. J. Immunol. 2002, 168, 5278–5286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gevaert, P.; Calus, L.; Van Zele, T.; Blomme, K.; De Ruyck, N.; Bauters, W.; Hellings, P.; Brusselle, G.; De Bacquer, D.; van Cauwenberge, P.; et al. Omalizumab is effective in allergic and nonallergic patients with nasal polyps and asthma. J. Allergy Clin. Immunol. 2013, 131, 110–116.e111. [Google Scholar] [CrossRef] [PubMed]
- Yip, J.; Monteiro, E.; Chan, Y. Endotypes of chronic rhinosinusitis. Curr. Opin. Otolaryngol. Head Neck Surg. 2019, 27, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Berghi, N.O.; Dumitru, M.; Vrinceanu, D.; Ciuluvica, R.C.; Simioniuc-Petrescu, A.; Caragheorgheopol, R.; Tucureanu, C.; Cornateanu, R.S.; Giurcaneanu, C. Relationship between chemokines and T lymphocytes in the context of respiratory allergies (Review). Exp. Ther. Med. 2020, 20, 2352–2360. [Google Scholar] [CrossRef]
- Persson, T.; Monsef, N.; Andersson, P.; Bjartell, A.; Malm, J.; Calafat, J.; Egesten, A. Expression of the neutrophil-activating CXC chemokine ENA-78/CXCL5 by human eosinophils. Clin. Exp. Allergy 2003, 33, 531–537. [Google Scholar] [CrossRef]
- Booth, V.; Keizer, D.W.; Kamphuis, M.B.; Clark-Lewis, I.; Sykes, B.D. The CXCR3 binding chemokine IP-10/CXCL10: Structure and receptor interactions. Biochemistry 2002, 41, 10418–10425. [Google Scholar] [CrossRef]
- Sallusto, F.; Lenig, D.; Mackay, C.R.; Lanzavecchia, A. Flexible programs of chemokine receptor expression on human polarized T helper 1 and 2 lymphocytes. J. Exp. Med. 1998, 187, 875–883. [Google Scholar] [CrossRef]
- Rot, A.; Krieger, M.; Brunner, T.; Bischoff, S.C.; Schall, T.J.; Dahinden, C.A. RANTES and macrophage inflammatory protein 1 alpha induce the migration and activation of normal human eosinophil granulocytes. J. Exp. Med. 1992, 176, 1489–1495. [Google Scholar] [CrossRef] [Green Version]
- Kapitany, A.; Beke, G.; Nagy, G.; Doan-Xuan, Q.M.; Bacso, Z.; Gaspar, K.; Boros, G.; Dajnoki, Z.; Biro, T.; Rajnavolgyi, E.; et al. CD1c+ Blood Dendritic Cells in Atopic Dermatitis are Premature and Can Produce Disease-specific Chemokines. Acta Derm. Venereol. 2017, 97, 325–331. [Google Scholar] [CrossRef] [Green Version]
- Kim, B.; Lee, H.J.; Im, N.R.; Lee, D.Y.; Kim, H.K.; Kang, C.Y.; Park, I.H.; Lee, S.H.; Lee, H.M.; Lee, S.H.; et al. Decreased expression of CCL17 in the disrupted nasal polyp epithelium and its regulation by IL-4 and IL-5. PLoS ONE 2018, 13, e0197355. [Google Scholar] [CrossRef] [Green Version]
- Tsybikov, N.N.; Egorova, E.V.; Kuznik, B.I.; Fefelova, E.V.; Magen, E. Biomarker assessment in chronic rhinitis and chronic rhinosinusitis: Endothelin-1, TARC/CCL17, neopterin, and alpha-defensins. Allergy Asthma Proc. 2016, 37, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Poposki, J.A.; Klingler, A.I.; Tan, B.K.; Soroosh, P.; Banie, H.; Lewis, G.; Hulse, K.E.; Stevens, W.W.; Peters, A.T.; Grammer, L.C.; et al. Group 2 innate lymphoid cells are elevated and activated in chronic rhinosinusitis with nasal polyps. Immun. Inflamm. Dis. 2017, 5, 233–243. [Google Scholar] [CrossRef] [PubMed]
- Halim, T.Y.; Hwang, Y.Y.; Scanlon, S.T.; Zaghouani, H.; Garbi, N.; Fallon, P.G.; McKenzie, A.N. Group 2 innate lymphoid cells license dendritic cells to potentiate memory TH2 cell responses. Nat. Immunol. 2016, 17, 57–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yao, T.; Kojima, Y.; Koyanagi, A.; Yokoi, H.; Saito, T.; Kawano, K.; Furukawa, M.; Kusunoki, T.; Ikeda, K. Eotaxin-1, -2, and -3 immunoreactivity and protein concentration in the nasal polyps of eosinophilic chronic rhinosinusitis patients. Laryngoscope 2009, 119, 1053–1059. [Google Scholar] [CrossRef] [Green Version]
- Jonstam, K.; Swanson, B.N.; Mannent, L.P.; Cardell, L.O.; Tian, N.; Wang, Y.; Zhang, D.; Fan, C.; Holtappels, G.; Hamilton, J.D.; et al. Dupilumab reduces local type 2 pro-inflammatory biomarkers in chronic rhinosinusitis with nasal polyposis. Allergy 2019, 74, 743–752. [Google Scholar] [CrossRef] [Green Version]
- Bonecchi, R.; Bianchi, G.; Bordignon, P.P.; D’Ambrosio, D.; Lang, R.; Borsatti, A.; Sozzani, S.; Allavena, P.; Gray, P.A.; Mantovani, A.; et al. Differential expression of chemokine receptors and chemotactic responsiveness of type 1 T helper cells (Th1s) and Th2s. J. Exp. Med. 1998, 187, 129–134. [Google Scholar] [CrossRef]
- Bullone, M.; Carriero, V.; Bertolini, F.; Folino, A.; Mannelli, A.; Di Stefano, A.; Gnemmi, I.; Torchio, R.; Ricciardolo, F.L.M. Elevated serum IgE, oral corticosteroid dependence and IL-17/22 expression in highly neutrophilic asthma. Eur. Respir. J. 2019, 54, 1900068. [Google Scholar] [CrossRef]
- Sonnenberg, G.F.; Nair, M.G.; Kirn, T.J.; Zaph, C.; Fouser, L.A.; Artis, D. Pathological versus protective functions of IL-22 in airway inflammation are regulated by IL-17A. J. Exp. Med. 2010, 207, 1293–1305. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, K.; Hirose, K.; Kawashima, S.; Niwa, Y.; Wakashin, H.; Iwata, A.; Tokoyoda, K.; Renauld, J.C.; Iwamoto, I.; Nakayama, T.; et al. IL-22 attenuates IL-25 production by lung epithelial cells and inhibits antigen-induced eosinophilic airway inflammation. J. Allergy Clin. Immunol. 2011, 128, 1067–1076.e1061–1066. [Google Scholar] [CrossRef]
- Kim, D.K.; Jo, A.; Lim, H.S.; Kim, J.Y.; Eun, K.M.; Oh, J.; Kim, J.K.; Cho, S.H.; Kim, D.W. Enhanced Type 2 Immune Reactions by Increased IL-22/IL-22Ra1 Signaling in Chronic Rhinosinusitis with Nasal Polyps. Allergy Asthma Immunol. Res. 2020, 12, 980–993. [Google Scholar] [CrossRef]
- Kim, D.W.; Eun, K.M.; Roh, E.Y.; Shin, S.; Kim, D.K. Chronic Rhinosinusitis without Nasal Polyps in Asian Patients Shows Mixed Inflammatory Patterns and Neutrophil-Related Disease Severity. Mediat. Inflamm. 2019, 2019, 7138643. [Google Scholar] [CrossRef] [PubMed]
- Yao, Y.; Zeng, M.; Liu, Z. Revisiting Asian chronic rhinosinusitis in the era of type 2 biologics. Clin. Exp. Allergy 2022, 52, 231–243. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.K.; Eun, K.M.; Kim, M.K.; Cho, D.; Han, S.A.; Han, S.Y.; Seo, Y.; Lee, D.H.; Cho, S.H.; Kim, D.W. Comparison Between Signature Cytokines of Nasal Tissues in Subtypes of Chronic Rhinosinusitis. Allergy Asthma Immunol. Res. 2019, 11, 201–211. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Zhang, N.; Bo, M.; Holtappels, G.; Zheng, M.; Lou, H.; Wang, H.; Zhang, L.; Bachert, C. Diversity of T(H) cytokine profiles in patients with chronic rhinosinusitis: A multicenter study in Europe, Asia, and Oceania. J. Allergy Clin. Immunol. 2016, 138, 1344–1353. [Google Scholar] [CrossRef] [Green Version]
- Zhang, N.; Holtappels, G.; Gevaert, P.; Patou, J.; Dhaliwal, B.; Gould, H.; Bachert, C. Mucosal tissue polyclonal IgE is functional in response to allergen and SEB. Allergy 2011, 66, 141–148. [Google Scholar] [CrossRef]
- Klingler, A.I.; Stevens, W.W.; Tan, B.K.; Peters, A.T.; Poposki, J.A.; Grammer, L.C.; Welch, K.C.; Smith, S.S.; Conley, D.B.; Kern, R.C.; et al. Mechanisms and biomarkers of inflammatory endotypes in chronic rhinosinusitis without nasal polyps. J. Allergy Clin. Immunol. 2021, 147, 1306–1317. [Google Scholar] [CrossRef]


{kind=link}
| Chemokine | Motif | Receptor | Origin | Main Immune Function |
|---|---|---|---|---|
| Eotaxin-1/CCL11 | CC | CCR3 | secreted by epithelial, mesenchymal, endothelial cells, and eosinophils [30] | attracts eosinophils [31] and basophils, selective on CCR3 receptor [32] |
| MIP1α/CCL3 (macrophage inflammatory protein-1α) | CC | CCR1, CCR5 | secreted by T- and B-lymphocytes, neutrophils, dendritic cells, mast cells, and NK cells [33] | attracts IFNγ-activated neutrophils and a small subpopulation of CCR1 expressing eosinophils [33] |
| MCP-3/CCL7 (monocyte chemotactic protein-3) | CC | CCR1, CCR2, CCR3 | secreted by mononuclear cells [34] | attracts monocytes, dendritic cells, lymphocytes, NK cells, eosinophils, basophils, and neutrophils [35] |
| ENA-78/CXCL5 (epithelial-derived neutrophil-activating peptide 78) | CXC | CXCR2 | secreted by monocytes, endothelial cells, mast cells, keratinocytes, fibroblasts [36] | attracts neutrophils [36] |
| TARC/CCL17 (thymus- and activation-regulated chemokine) | CC | CCR4 | secreted by monocytes, dendritic and epithelial cells [24] | attracts T lymphocytes (Th2) |
| PARC/CCL18 (pulmonary and activation- regulated chemokine) [37] | CC | CCR8 | secreted by dendritic cells, monocytes, macrophages, mast cells, eosinophils, and neutrophils [38] | attracts naive CD4+ and CD8+ T cells, B cells, and immature dendritic cells [37,39] |
| IP-10/CXCL10 (IFNγ-inducible protein 10) | CXC | CXCR3 | secreted by monocytes, T-lymphocytes, fibroblasts, keratinocytes [40] in response to the Th1-cytokine IFNγ | attracts activated Th1-lymphocytes [41] |
| Marker | Cutoff Values * | Interpretation of Increased Concentrations |
|---|---|---|
| Eotaxin/CCL11 | NA | Type-2 immunity |
| MCP-3/CCL7 | NA | Associated with type-1 and type-2 immunity |
| MIP-1 α/CCL3 | NA | Associated with type-1 and type-2 immunity |
| ENA-78/CXCL5 | NA | Neutrophilic inflammation |
| TARC/CCL17 | NA | Type-2 immunity |
| PARC/CCL18 | NA | Type-2 immunity |
| IP-10/CXCL10 | NA | Type-1 immunity |
| ECP | NA | Type-2 immunity |
| IgE | NA | Type-2 immunity |
| SE-IgE | 3.85 kUA/L * | Marker of superantigen effect on local mucosa |
| IL-5 | 12.98 pg/mL * | Type-2 immunity |
| MPO | NA | Neutrophilic activity |
| IL-22 | NA | Type-3 immunity |
| TNF-α | 38.94 pg/mL * | Type-1 immunity |
| IL-17 | 25.06 pg/mL * | Type-3 immunity |
| IFN-ɣ | 85.8 pg/mL * | Type-1 immunity |
| Patients | Controls | Significance | ||
|---|---|---|---|---|
| MV Min–Max (SD) | MV Min–Max (SD) | |||
| Number | 66 | 25 | ||
| Clinic | Age (mean) | 42.3 25–65 (10.0) | 31.4 18–60 (12.1) | p < 0.001 1 |
| Gender male % | 62.1 | 52.0 | p = 0.475 2 | |
| Ever smoked % | 69.7 | 48.0 | p = 0.086 2 | |
| Smoker current % | 39.4 | 36.0 | p = 0.814 2 | |
| Allergy % | 33.3 | 16.0 | p = 0.124 2 | |
| Asthma % | 19.7 | 8.0 | p = 0.222 2 | |
| N-ERD % | 7.6 | 0.0 | p = 0.317 | |
| Laboratory Findings | Eotaxin/CCL11 pg/mL | 37.7 2.5–677.7 (85.9) | 11.7 1.8–52.5 (11.6) | p = 0.001 1 |
| MCP-3/CCL7 pg/mL | 3.3 0.4–14.3 (2.5) | 5.7 0.8–47.5 (12.1) | p = 0.147 1 | |
| MIP-1α/CCL3 pg/mL | 3.8 0.9–19.3 (3.1) | 5.9 1.4–45.8 (9.5) | p = 0.545 1 | |
| ENA-78/CXCL5 pg/mL | 43.0 3.7–215.6 (49.6) | 113.2 5.9–1263.5 (262.4) | p = 0.140 1 | |
| TARC/CCL17 pg/mL | 8.3 1.4–40.9 (8.0) | 5.9 0.8–54.9 (12.8) | p < 0.0011 | |
| PARC/CCL18 pg/mL | 409.4 10.8-3246.5 (626.7) | 119.0 40.2-235.6 (50.8) | p = 0.016 1 | |
| IP-10/CXCL10 pg/mL | 330.5 15.2-4510.2 (620.9) | 274.3 25.0-1208.4 (257.4) | p = 0.240 1 | |
| Total IgE kU/L | 262.2 0.0–3641.0 (604.3) | 30.0 1.7–293.7 (60.6) | p = 0.0011 | |
| ECP pg/mL | 4971.0 11.0–32,725.0 (7499.4) | 194.4 11.0–1254.0 (313.6) | p < 0.001 1 | |
| IL-5 pg/mL | 136.5 6.5–963.7 (215.6) | 6.5 6.5–6.5 (0) | p < 0.001 1 | |
| SAE kU/L | 0.8 0.0–8.7 (2.1) | 0.0 0.0–0.0 (0.0) | p = 0.095 1 | |
| IL-22 pg/mL | 537.1 140.3–1680.5 (294.4 | 494.6 254.7–1473.9 (256.2) | p = 0.577 1 | |
| MPO ng/mL | 4198.1 166.2–56,996.5 (7560.1) | 1160.4 158.1–4683.1 (1100.7) | p < 0.001 1 | |
| TNF-α pg/mL (>Threshold %) | 3.0 | 0.0 | p = 1.000 2 | |
| IL-17 pg/mL (>Threshold %) | 4.5 | 4.0 | p = 1.000 2 | |
| IFN-γ pg/mL (>Threshold %) | 9.7 | 4.2 | p = 0.668 2 |
| Variables Used in Cluster Analysis | Variables Not Used in Cluster Analysis | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ENA_78/CXCL5 | MPO | IP-10/CXCL10 | MIP1a/CCL3 | MCP-3/CCL7 | TARC/CCL17 | PARC/CCL18 | Eotaxin/CCL11 | ECP | IL-5 | Total-IgE | IL-22 | SAE | SAE Ratio | Ratio IL5 | TNF-α-Categorial | IL-17-Categorial | IFN-γ-Categorial | |
| Cluster (Number of Cases) | Mean | Mean | Mean | Mean | Mean | Mean | Mean | Mean | Mean | Mean | Mean | Mean | Mean | Ratio Positive | Ratio Positive | Ratio Positive | Ratio Positive | Ratio Positive |
| 1 (n = 9) | 32.91 | 2866.26 | 332.78 | 1.26 | 1.36 | 3.33 | 80.58 | 6.57 | 686.46 | 6.49 | 42.74 | 693.74 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.29 |
| 2 (n = 11) | 53.37 | 1982.33 | 346.33 | 2.91 | 3.02 | 3.16 | 127.10 | 9.59 | 373.86 | 30.69 | 17.19 | 372.86 | 0.00 | 0.00 | 0.18 | 0.00 | 0.09 | 0.00 |
| 3 (n = 8) | 82.27 | 2426.66 | 1110.10 | 8.49 | 6.60 | 6.32 | 168.23 | 18.47 | 1294.99 | 17.74 | 66.89 | 530.65 | 0.00 | 0.00 | 0.25 | 0.00 | 0.00 | 0.00 |
| 4 (n = 13) | 45.04 | 4034.73 | 264.41 | 2.61 | 2.65 | 6.77 | 155.50 | 21.37 | 2673.59 | 83.46 | 142.84 | 640.02 | 0.00 | 0.00 | 0.54 | 0.08 | 0.15 | 0.08 |
| 5 (n = 9) | 59.712 | 13031.6 | 142.68 | 6.34 | 4.72 | 21.44 | 1072.15 | 114.79 | 12793.00 | 204.76 | 710.55 | 981.71 | 2.34 | 0.33 | 0.89 | 0.11 | 0.00 | 0.13 |
| 6 (n = 16) | 10.73 | 2795.16 | 87.72 | 3.10 | 2.65 | 9.57 | 742.61 | 54.09 | 9846.44 | 346.29 | 524.4 | 312.85 | 1.46 | 0.27 | 1.00 | 0.00 | 0.00 | 0.13 |
| Cluster | Number of Cases | IL-5 | IL-5 Positive Ratio % | IL-5 | ECP | Total IgE | PARC (CCL18) | TARC (CCL17) | Eotaxin (CCL11) | MCP3 (CCL7) | MIP1α (CCL3) | ENA-78 (CCL5) | MPO | IP-10 (CXCL10) | IL-22 | NP | Average Number of Surgeries | Asthma | Allergic Rhinitis | N-ERD |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 9 | negative | 0.0% | >2 | 1/9 (11%) | 1 | 2/9 (22%) | 3/9 (33%) | 0/9 (0%) | |||||||||||
| 2 | 11 | low | 18.2% | >2 | > 2 | 0/11 (0%) | 1 | 1/11 (9%) | 3/11 (27%) | 0/11 (0%) | ||||||||||
| 3 | 8 | 25.0% | >2 | >2 | >4 | >4 | >2 | >4 | >2 | 1/8 (13%) | 1 | 0/8 (0%) | 2/8 (25%) | 0/8 (0%) | ||||||
| 4 | 13 | 53.8% | >2 | >2 | >2 | >2 | >2 | >3 | >2 | 4/13 (31%) | 1 | 3/13 (23%) | 8/13 (62%) | 0/13 (0%) | ||||||
| 5 | 9 | high | 8.9% | >4 | >4 | >4 | >4 | >4 | >4 | >2 | >4 | >3 | >3 | 7/9 (78%) | 1.7 | 4/9 (44%) | 1/9 (11%) | 2/9 (22%) | ||
| 6 | 16 | 100.0% | >4 | >4 | >3 | >4 | >2 | >4 | 13/16 (81%) | 1.7 | 3/16 (19%) | 6/16 (38%) | 3/16 (19%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Förster-Ruhrmann, U.; Szczepek, A.J.; Pierchalla, G.; Fluhr, J.W.; Artuc, M.; Zuberbier, T.; Bachert, C.; Olze, H. Chemokine Expression-Based Endotype Clustering of Chronic Rhinosinusitis. J. Pers. Med. 2022, 12, 646. https://doi.org/10.3390/jpm12040646
Förster-Ruhrmann U, Szczepek AJ, Pierchalla G, Fluhr JW, Artuc M, Zuberbier T, Bachert C, Olze H. Chemokine Expression-Based Endotype Clustering of Chronic Rhinosinusitis. Journal of Personalized Medicine. 2022; 12(4):646. https://doi.org/10.3390/jpm12040646
Chicago/Turabian StyleFörster-Ruhrmann, Ulrike, Agnieszka J. Szczepek, Greta Pierchalla, Joachim W. Fluhr, Metin Artuc, Torsten Zuberbier, Claus Bachert, and Heidi Olze. 2022. "Chemokine Expression-Based Endotype Clustering of Chronic Rhinosinusitis" Journal of Personalized Medicine 12, no. 4: 646. https://doi.org/10.3390/jpm12040646