
Interprofessional Collaboration and Diabetes Management in Primary Care: A Systematic Review and Meta-Analysis of Patient-Reported Outcomes

 , , ,
, , , {kind=link}
{kind=link}
Abstract
:1. Background
2. Materials and Methods
2.1. Study Design and Literature Search
2.2. Study Selection
2.3. Quality Assessment
2.4. Data Extraction and Data Analysis
3. Results
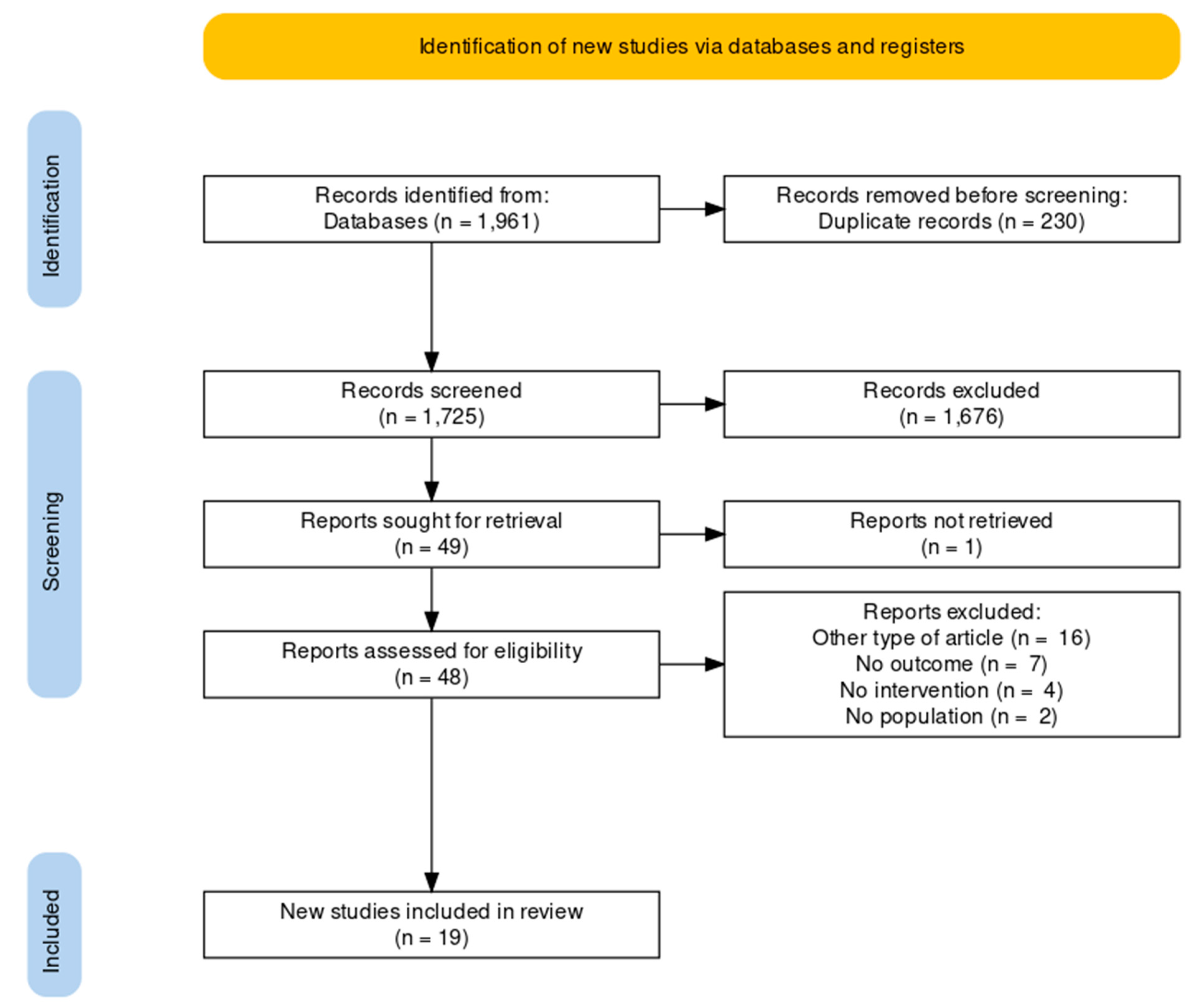
3.1. Study Selection
3.2. Characteristics of the Studies
3.3. Quality Assessment
3.4. Data Synthesis
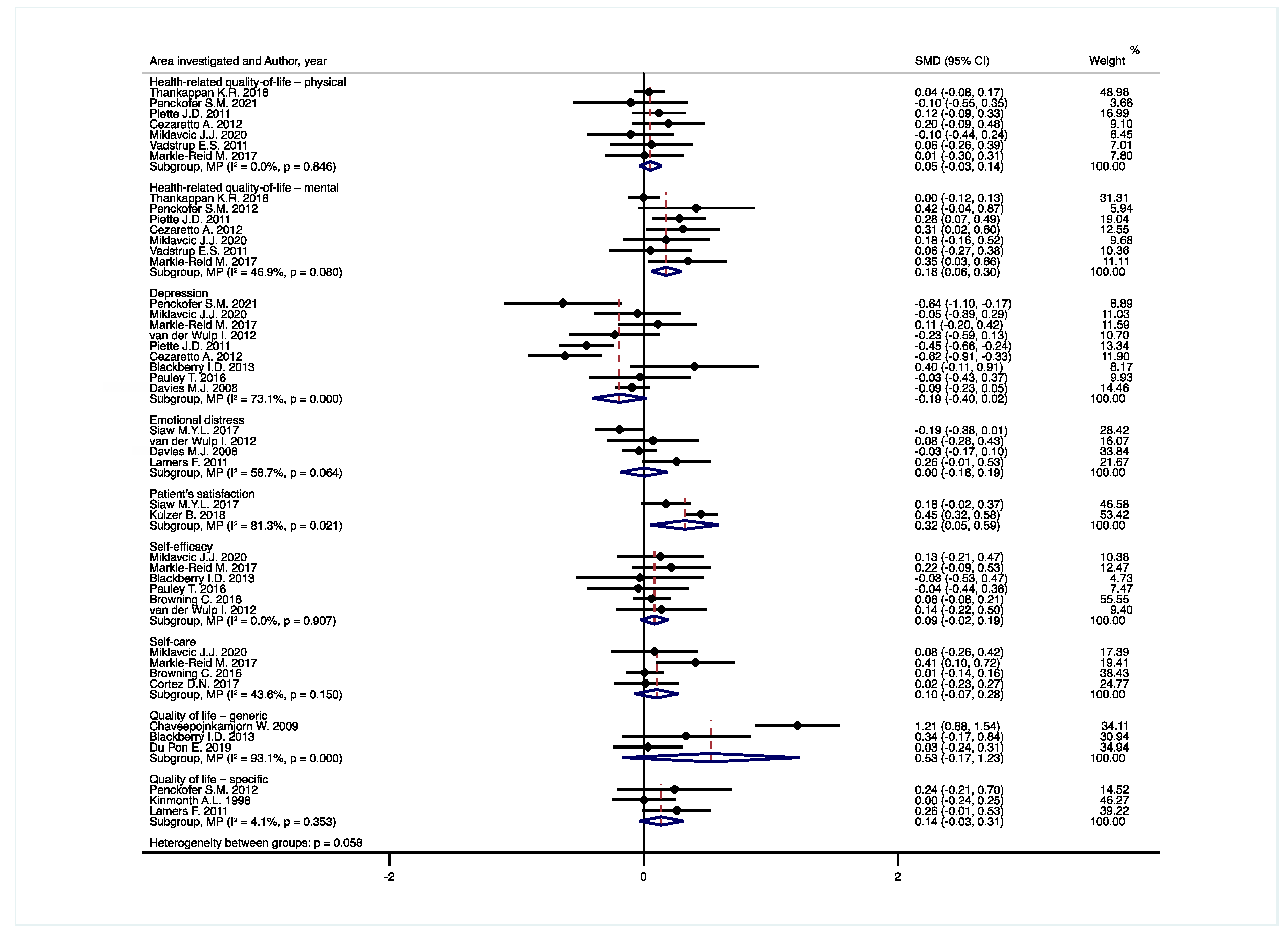
3.4.1. Health-Related Quality-of-Life—Physical
3.4.2. Health-Related Quality-of-Life—Mental
3.4.3. Depression
3.4.4. Emotional Distress
3.4.5. Patient’s Satisfaction
3.4.6. Self-Efficacy
3.4.7. Self-Care
3.4.8. Quality of Life—Generic
3.4.9. Quality of Life—Specific
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Noncommunicable Diseases. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 15 January 2022).
- International Diabetes Federation. IDF Diabetes Atlas. Available online: https://diabetesatlas.org/data/en/world/ (accessed on 15 January 2022).
- World Health Organization. Diabetes—Key Facts. Available online: https://www.who.int/en/news-room/fact-sheets/detail/diabetes (accessed on 15 January 2022).
- Kirkman, M.S.; Briscoe, V.J.; Clark, N.; Florez, H.; Haas, L.B.; Halter, J.B.; Huang, E.S.; Korytkowski, M.T.; Munshi, M.N.; Odegard, P.S.; et al. Consensus Development Conference on Diabetes and Older Adults. Diabetes in Older Adults: A Consensus Report. J. Am. Geriatr. Soc. 2012, 60, 2342–2356. [Google Scholar] [CrossRef] [PubMed]
- Sinnige, J.; Braspenning, J.; Schellevis, F.; Stirbu-Wagner, I.; Westert, G.; Korevaar, J. The Prevalence of Disease Clusters in Older Adults with Multiple Chronic Diseases—A Systematic Literature Review. PLoS ONE 2013, 8, e79641. [Google Scholar] [CrossRef] [PubMed]
- Willi, C.; Bodenmann, P.; Ghali, W.A.; Faris, P.D.; Cornuz, J. Active Smoking and the Risk of Type 2 Diabetes: A Systematic Review and Meta-Analysis. JAMA 2007, 298, 2654–2664. [Google Scholar] [CrossRef] [PubMed]
- Fisher, K.; Griffith, L.; Gruneir, A.; Panjwani, D.; Gandhi, S.; Sheng, L.L.; Gafni, A.; Chris, P.; Markle-Reid, M.; Ploeg, J. Comorbidity and Its Relationship with Health Service Use and Cost in Community-Living Older Adults with Diabetes: A Population-Based Study in Ontario, Canada. Diabetes Res. Clin. Pract. 2016, 122, 113–123. [Google Scholar] [CrossRef] [PubMed]
- Egede, L.E. Major Depression in Individuals with Chronic Medical Disorders: Prevalence, Correlates and Association with Health Resource Utilization, Lost Productivity and Functional Disability. Gen. Hosp. Psychiatry 2007, 29, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Perrin, N.E.; Davies, M.J.; Robertson, N.; Snoek, F.J.; Khunti, K. The Prevalence of Diabetes-Specific Emotional Distress in People with Type 2 Diabetes: A Systematic Review and Meta-Analysis. Diabet. Med. 2017, 34, 1508–1520. [Google Scholar] [CrossRef]
- Gonzalez, J.S.; Safren, S.A.; Cagliero, E.; Wexler, D.J.; Delahanty, L.; Wittenberg, E.; Blais, M.A.; Meigs, J.B.; Grant, R.W. Depression, Self-Care, and Medication Adherence in Type 2 Diabetes: Relationships across the Full Range of Symptom Severity. Diabetes Care 2007, 30, 2222–2227. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez, J.S.; Peyrot, M.; McCarl, L.A.; Collins, E.M.; Serpa, L.; Mimiaga, M.J.; Safren, S.A. Depression and Diabetes Treatment Nonadherence: A Meta-Analysis. Diabetes Care 2008, 31, 2398–2403. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez, J.S.; Shreck, E.; Psaros, C.; Safren, S.A. Distress and Type 2 Diabetes-Treatment Adherence: A Mediating Role for Perceived Control. Health Psychol. 2015, 34, 505–513. [Google Scholar] [CrossRef] [Green Version]
- Van Dieren, S.; Beulens, J.W.J.; van der Schouw, Y.T.; Grobbee, D.E.; Neal, B. The Global Burden of Diabetes and Its Complications: An Emerging Pandemic. Eur. J. Cardiovasc. Prev. Rehabil. 2010, 17, S3–S8. [Google Scholar] [CrossRef]
- O’Connell, J.M.; Manson, S.M. Understanding the Economic Costs of Diabetes and Prediabetes and What We May Learn about Reducing the Health and Economic Burden of These Conditions. Diabetes Care 2019, 42, 1609–1611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagner, E.H. Chronic Disease Management: What Will It Take to Improve Care for Chronic Illness? Eff. Clin. Pract. 1998, 1, 2–4. [Google Scholar] [PubMed]
- Wagner, E.H.; Austin, B.T.; Davis, C.; Hindmarsh, M.; Schaefer, J.; Bonomi, A. Improving Chronic Illness Care: Translating Evidence into Action. Health Aff. 2001, 20, 64–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coleman, K.; Austin, B.T.; Brach, C.; Wagner, E.H. Evidence on the Chronic Care Model in the New Millennium. Health Aff. 2009, 28, 75–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davy, C.; Bleasel, J.; Liu, H.; Tchan, M.; Ponniah, S.; Brown, A. Effectiveness of Chronic Care Models: Opportunities for Improving Healthcare Practice and Health Outcomes: A Systematic Review. BMC Health Serv. Res. 2015, 15, 194. [Google Scholar] [CrossRef] [Green Version]
- Petrelli, F.; Cangelosi, G.; Nittari, G.; Pantanetti, P.; Debernardi, G.; Scuri, S.; Sagaro, G.G.; Nguyen, C.T.T.; Grappasonni, I. Chronic Care Model in Italy: A Narrative Review of the Literature. Prim. Health Care Res. Dev. 2021, 22, e32. [Google Scholar] [CrossRef]
- Mitchell, P.; Wynia, M.; Golden, R.; McNellis, B.; Okun, S.; Webb, E.; Rohrbach, V.; Von Kohorn, I. Core Principles & Values of Effective Team-Based Health Care; Institute of Medicine: Washington, DC, USA, 2021. [Google Scholar]
- Reeves, S.; Pelone, F.; Harrison, R.; Goldman, J.; Zwarenstein, M. Interprofessional Collaboration to Improve Professional Practice and Healthcare Outcomes. Cochrane Database Syst. Rev. 2017, 6, CD000072. [Google Scholar] [CrossRef]
- Pascucci, D.; Sassano, M.; Nurchis, M.C.; Cicconi, M.; Acampora, A.; Park, D.; Morano, C.; Damiani, G. Impact of Interprofessional Collaboration on Chronic Disease Management: Findings from a Systematic Review of Clinical Trial and Meta-Analysis. Health Policy 2021, 125, 191–202. [Google Scholar] [CrossRef]
- Bauer, U.E.; Briss, P.A.; Goodman, R.A.; Bowman, B.A. Prevention of Chronic Disease in the 21st Century: Elimination of the Leading Preventable Causes of Premature Death and Disability in the USA. Lancet 2014, 384, 45–52. [Google Scholar] [CrossRef]
- Baumann, L.C.; Dang, T.T.N. Helping Patients with Chronic Conditions Overcome Barriers to Self-Care. Nurse Pract. 2012, 37, 32–38. [Google Scholar] [CrossRef] [Green Version]
- Food and Drug Administration. Guidance for Industry Patient-Reported Outcome Measures: Use in Medical Product Development to Support Labeling Claims; Food and Drug Administration: Silver Spring, MD, USA, 2009; pp. 1–35.
- Black, N. Patient Reported Outcome Measures Could Help Transform Healthcare. BMJ 2013, 346, f167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Black, N.; Jenkinson, C. Measuring Patients’ Experiences and Outcomes. BMJ 2009, 339, b2495. [Google Scholar] [CrossRef] [PubMed]
- Montgomery, N.; Howell, D.; Ismail, Z.; Bartlett, S.J.; Brundage, M.; Bryant-Lukosius, D.; Krzyzanowska, M.; Moody, L.; Snyder, C.; Barbera, L.; et al. Selecting, Implementing and Evaluating Patient-Reported Outcome Measures for Routine Clinical Use in Cancer: The Cancer Care Ontario Approach. J. Patient Rep. Outcomes 2020, 4, 101. [Google Scholar] [CrossRef] [PubMed]
- Aiyegbusi, O.L. Key Methodological Considerations for Usability Testing of Electronic Patient-Reported Outcome (EPRO) Systems. Qual. Life Res. 2020, 29, 325–333. [Google Scholar] [CrossRef] [Green Version]
- Thestrup Hansen, S.; Kjerholt, M.; Friis Christensen, S.; Brodersen, J.; Hølge-Hazelton, B. User Experiences on Implementation of Patient Reported Outcome Measures (PROMs) in a Haematological Outpatient Clinic. J. Patient Rep. Outcomes 2020, 4, 87. [Google Scholar] [CrossRef]
- Richardson, W.S.; Wilson, M.C.; Nishikawa, J.; Hayward, R.S. The Well-Built Clinical Question: A Key to Evidence-Based Decisions. ACP J. Club 1995, 123, A12–A13. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Reeves, S.; Perrier, L.; Goldman, J.; Freeth, D.; Zwarenstein, M. Interprofessional Education: Effects on Professional Practice and Healthcare Outcomes (Update). Cochrane Database Syst. Rev. 2013, 3, CD002213. [Google Scholar] [CrossRef]
- Yorganci, E.; Evans, C.J.; Johnson, H.; Barclay, S.; Murtagh, F.E.; Yi, D.; Gao, W.; Pickles, A.; Koffman, J. Understanding Usual Care in Randomised Controlled Trials of Complex Interventions: A Multi-Method Approach. Palliat. Med. 2020, 34, 667–679. [Google Scholar] [CrossRef] [Green Version]
- National Heart, Lung, and Blood Institute. Study Quality Assessment Tools. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 2 December 2021).
- Hedges, L.V. Distribution Theory for Glass’s Estimator of Effect Size and Related Estimators. J. Educ. Stat. 1981, 6, 107–128. [Google Scholar] [CrossRef]
- Paule, R.C.; Mandel, J. Consensus Values and Weighting Factors. J. Res. Natl. Bur. Stand. 1982, 87, 377–385. [Google Scholar] [CrossRef] [PubMed]
- Veroniki, A.A.; Jackson, D.; Viechtbauer, W.; Bender, R.; Bowden, J.; Knapp, G.; Kuss, O.; Higgins, J.P.T.; Langan, D.; Salanti, G. Methods to Estimate the Between-Study Variance and Its Uncertainty in Meta-Analysis. Res. Synth. Methods 2016, 7, 55–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DerSimonian, R.; Laird, N. Meta-Analysis in Clinical Trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.T. Measuring Inconsistency in Meta-Analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thankappan, K.R.; Sathish, T.; Tapp, R.J.; Shaw, J.E.; Lotfaliany, M.; Wolfe, R.; Absetz, P.; Mathews, E.; Aziz, Z.; Williams, E.D.; et al. A Peer-Support Lifestyle Intervention for Preventing Type 2 Diabetes in India: A Cluster-Randomized Controlled Trial of the Kerala Diabetes Prevention Program. PLoS Med. 2018, 15, e1002575. [Google Scholar] [CrossRef] [PubMed]
- Penckofer, S.M.; Ferrans, C.; Mumby, P.; Byrn, M.; Emanuele, M.A.; Harrison, P.R.; Durazo-Arvizu, R.A.; Lustman, P. A Psychoeducational Intervention (SWEEP) for Depressed Women with Diabetes. Ann. Behav. Med. 2012, 44, 192–206. [Google Scholar] [CrossRef] [Green Version]
- Chaveepojnkamjorn, W.; Pichainarong, N.; Schelp, F.P.; Mahaweerawat, U. A Randomized Controlled Trial to Improve the Quality of Life of Type 2 Diabetic Patients Using a Self-Help Group Program. Southeast Asian J. Trop. Med. Public Health 2009, 40, 169–176. [Google Scholar]
- Piette, J.D.; Richardson, C.; Himle, J.; Duffy, S.; Torres, T.; Vogel, M.; Barber, K.; Valenstein, M. A Randomized Trial of Telephonic Counseling plus Walking for Depressed Diabetes Patients. Med. Care 2011, 49, 641–648. [Google Scholar] [CrossRef] [Green Version]
- Cezaretto, A.; Siqueira-Catania, A.; de Barros, C.R.; Salvador, E.P.; Ferreira, S.R.G. Benefits on Quality of Life Concomitant to Metabolic Improvement in Intervention Program for Prevention of Diabetes Mellitus. Qual. Life Res. 2012, 21, 105–113. [Google Scholar] [CrossRef]
- Miklavcic, J.J.; Fraser, K.D.; Ploeg, J.; Markle-Reid, M.; Fisher, K.; Gafni, A.; Griffith, L.E.; Hirst, S.; Sadowski, C.A.; Thabane, L.; et al. Effectiveness of a Community Program for Older Adults with Type 2 Diabetes and Multimorbidity: A Pragmatic Randomized Controlled Trial. BMC Geriatr. 2020, 20, 174. [Google Scholar] [CrossRef]
- Blackberry, I.D.; Furler, J.S.; Best, J.D.; Chondros, P.; Vale, M.; Walker, C.; Dunning, T.; Segal, L.; Dunbar, J.; Audehm, R.; et al. Effectiveness of General Practice Based, Practice Nurse Led Telephone Coaching on Glycaemic Control of Type 2 Diabetes: The Patient Engagement and Coaching for Health (PEACH) Pragmatic Cluster Randomised Controlled Trial. BMJ 2013, 347, f5272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du Pon, E.; Kleefstra, N.; Cleveringa, F.; van Dooren, A.; Heerdink, E.R.; van Dulmen, S. Effects of the Proactive Interdisciplinary Self-Management (PRISMA) Program on Self-Reported and Clinical Outcomes in Type 2 Diabetes: A Pragmatic Randomized Controlled Trial. BMC Endocr. Disord. 2019, 19, 139. [Google Scholar] [CrossRef] [PubMed]
- Vadstrup, E.S.; Frølich, A.; Perrild, H.; Borg, E.; Røder, M. Health-Related Quality of Life and Self-Related Health in Patients with Type 2 Diabetes: Effects of Group-Based Rehabilitation versus Individual Counselling. Health Qual. Life Outcomes 2011, 9, 110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pauley, T.; Gargaro, J.; Chenard, G.; Cavanagh, H.; McKay, S.M. Home-Based Diabetes Self-Management Coaching Delivered by Paraprofessionals: A Randomized Controlled Trial. Home Health Care Serv. Q. 2016, 35, 137–154. [Google Scholar] [CrossRef] [PubMed]
- Siaw, M.Y.L.; Ko, Y.; Malone, D.C.; Tsou, K.Y.K.; Lew, Y.-J.; Foo, D.; Tan, E.; Chan, S.C.; Chia, A.; Sinaram, S.S.; et al. Impact of Pharmacist-Involved Collaborative Care on the Clinical, Humanistic and Cost Outcomes of High-Risk Patients with Type 2 Diabetes (IMPACT): A Randomized Controlled Trial. J. Clin. Pharm. Ther. 2017, 42, 475–482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kulzer, B.; Daenschel, W.; Daenschel, I.; Schramm, W.; Messinger, D.; Weissmann, J.; Vesper, I.; Parkin, C.G.; Heinemann, L. Integrated Personalized Diabetes Management Improves Glycemic Control in Patients with Insulin-Treated Type 2 Diabetes: Results of the PDM-ProValue Study Program. Diabetes Res. Clin. Pract. 2018, 144, 200–212. [Google Scholar] [CrossRef] [Green Version]
- Browning, C.; Chapman, A.; Yang, H.; Liu, S.; Zhang, T.; Enticott, J.C.; Thomas, S.A. Management of Type 2 Diabetes in China: The Happy Life Club, a Pragmatic Cluster Randomised Controlled Trial Using Health Coaches. BMJ Open 2016, 6, e009319. [Google Scholar] [CrossRef] [Green Version]
- Markle-Reid, M.; Ploeg, J.; Fraser, K.D.; Fisher, K.A.; Bartholomew, A.; Griffith, L.E.; Miklavcic, J.; Gafni, A.; Thabane, L.; Upshur, R. Community Program Improves Quality of Life and Self-Management in Older Adults with Diabetes Mellitus and Comorbidity. J. Am. Geriatr. Soc. 2018, 66, 263–273. [Google Scholar] [CrossRef]
- van der Wulp, I.; de Leeuw, J.R.J.; Gorter, K.J.; Rutten, G.E.H.M. Effectiveness of Peer-Led Self-Management Coaching for Patients Recently Diagnosed with Type 2 Diabetes Mellitus in Primary Care: A Randomized Controlled Trial. Diabet. Med. 2012, 29, e390–e397. [Google Scholar] [CrossRef]
- Davies, M.J.; Heller, S.; Skinner, T.C.; Campbell, M.J.; Carey, M.E.; Cradock, S.; Dallosso, H.M.; Daly, H.; Doherty, Y.; Eaton, S.; et al. Diabetes Education and Self Management for Ongoing and Newly Diagnosed Collaborative. Effectiveness of the Diabetes Education and Self Management for Ongoing and Newly Diagnosed (DESMOND) Programme for People with Newly Diagnosed Type 2 Diabetes: Cluster Randomised Controlled Trial. BMJ 2008, 336, 491–495. [Google Scholar] [CrossRef] [Green Version]
- Cortez, D.N.; Macedo, M.M.L.; Souza, D.A.S.; Dos Santos, J.C.; Afonso, G.S.; Reis, I.A.; Torres, H. de C. Evaluating the Effectiveness of an Empowerment Program for Self-Care in Type 2 Diabetes: A Cluster Randomized Trial. BMC Public Health 2017, 17, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kinmonth, A.L.; Woodcock, A.; Griffin, S.; Spiegal, N.; Campbell, M.J. Randomised Controlled Trial of Patient Centred Care of Diabetes in General Practice: Impact on Current Wellbeing and Future Disease Risk. The Diabetes Care from Diagnosis Research Team. BMJ 1998, 317, 1202–1208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamers, F.; Jonkers, C.C.M.; Bosma, H.; Knottnerus, J.A.; van Eijk, J.T.M. Treating Depression in Diabetes Patients: Does a Nurse-Administered Minimal Psychological Intervention Affect Diabetes-Specific Quality of Life and Glycaemic Control? A Randomized Controlled Trial. J. Adv. Nurs. 2011, 67, 788–799. [Google Scholar] [CrossRef] [PubMed]
- Ismail, K.; Winkley, K.; Rabe-Hesketh, S. Systematic Review and Meta-Analysis of Randomised Controlled Trials of Psychological Interventions to Improve Glycaemic Control in Patients with Type 2 Diabetes. Lancet 2004, 363, 1589–1597. [Google Scholar] [CrossRef]
- Martinez Devesa, P.; Waddell, A.; Perera, R.; Theodoulou, M. Cognitive Behavioural Therapy for Tinnitus. Cochrane Database Syst. Rev. 2007, 1, CD005233. [Google Scholar] [CrossRef]
- McDowell, I. Measuring Health; Oxford University Press: Oxford, UK, 2006. [Google Scholar] [CrossRef]
- Alrubaiy, L.; Hutchings, H.A.; Williams, J.G. Assessing Patient Reported Outcome Measures: A Practical Guide for Gastroenterologists. United Eur. Gastroenterol. J. 2014, 2, 463–470. [Google Scholar] [CrossRef]
- Desse, T.A.; Namara, K.M.; Yifter, H.; Manias, E. Development of a Complex Intervention for Effective Management of Type 2 Diabetes in a Developing Country. JCM 2022, 11, 1149. [Google Scholar] [CrossRef]
- Jansink, R.; Braspenning, J.; Keizer, E.; van der Weijden, T.; Elwyn, G.; Grol, R. No Identifiable Hb1Ac or Lifestyle Change after a Comprehensive Diabetes Programme Including Motivational Interviewing: A Cluster Randomised Trial. Scand. J. Prim. Health Care 2013, 31, 119–127. [Google Scholar] [CrossRef]
- Renders, C.M.; Valk, G.D.; Griffin, S.J.; Wagner, E.; van Eijk, J.T.; Assendelft, W.J. Interventions to Improve the Management of Diabetes Mellitus in Primary Care, Outpatient and Community Settings. Cochrane Database Syst. Rev. 2000, 1, CD001481. [Google Scholar] [CrossRef]
- McCarney, R.; Warner, J.; Iliffe, S.; van Haselen, R.; Griffin, M.; Fisher, P. The Hawthorne Effect: A Randomised, Controlled Trial. BMC Med. Res. Methodol. 2007, 7, 30. [Google Scholar] [CrossRef] [Green Version]
- Hamasaki, H. Daily Physical Activity and Type 2 Diabetes: A Review. World J. Diabetes 2016, 7, 243–251. [Google Scholar] [CrossRef] [PubMed]
- Rawlinson, C.; Carron, T.; Cohidon, C.; Arditi, C.; Hong, Q.N.; Pluye, P.; Peytremann-Bridevaux, I.; Gilles, I. An Overview of Reviews on Interprofessional Collaboration in Primary Care: Barriers and Facilitators. Int. J. Integr. Care 2021, 21, 32. [Google Scholar] [CrossRef] [PubMed]
- Tan, G.D.; Kozlowska, O.; Rea, R.D. Integrated Care and Diabetes: Challenges, Principles and Opportunities. Clin. Integr. Care 2021, 4, 100037. [Google Scholar] [CrossRef]
- World Health Organization. Integrated Care Models: An Overview; World Health Organization: Copenhagen, Denmark, 2016; pp. 1–26.
- Lewis, R.Q.; Rosen, R.; Goodwin, N.; Dixon, J. Where next for Integrated Care Organisations in the English NHS. The Nuffield Trust 2010, 1, 4–34. [Google Scholar]
- Snyder, C.F.; Aaronson, N.K.; Choucair, A.K.; Elliott, T.E.; Greenhalgh, J.; Halyard, M.Y.; Hess, R.; Miller, D.M.; Reeve, B.B.; Santana, M. Implementing Patient-Reported Outcomes Assessment in Clinical Practice: A Review of the Options and Considerations. Qual. Life Res. 2012, 21, 1305–1314. [Google Scholar] [CrossRef]
- Haugstvedt, A.; Hernar, I.; Strandberg, R.B.; Richards, D.A.; Nilsen, R.M.; Tell, G.S.; Graue, M. Use of Patient-Reported Outcome Measures (PROMs) in Clinical Diabetes Consultations: Study Protocol for the DiaPROM Randomised Controlled Trial Pilot Study. BMJ Open 2019, 9, e024008. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nurchis, M.C.; Sessa, G.; Pascucci, D.; Sassano, M.; Lombi, L.; Damiani, G. Interprofessional Collaboration and Diabetes Management in Primary Care: A Systematic Review and Meta-Analysis of Patient-Reported Outcomes. J. Pers. Med. 2022, 12, 643. https://doi.org/10.3390/jpm12040643
Nurchis MC, Sessa G, Pascucci D, Sassano M, Lombi L, Damiani G. Interprofessional Collaboration and Diabetes Management in Primary Care: A Systematic Review and Meta-Analysis of Patient-Reported Outcomes. Journal of Personalized Medicine. 2022; 12(4):643. https://doi.org/10.3390/jpm12040643
Chicago/Turabian StyleNurchis, Mario Cesare, Giorgio Sessa, Domenico Pascucci, Michele Sassano, Linda Lombi, and Gianfranco Damiani. 2022. "Interprofessional Collaboration and Diabetes Management in Primary Care: A Systematic Review and Meta-Analysis of Patient-Reported Outcomes" Journal of Personalized Medicine 12, no. 4: 643. https://doi.org/10.3390/jpm12040643