
Genetic and Clinical Factors Associated with Olokizumab Treatment in Russian Patients with Rheumatoid Arthritis

 , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. Characteristics of Olokizumab Efficacy and Safety
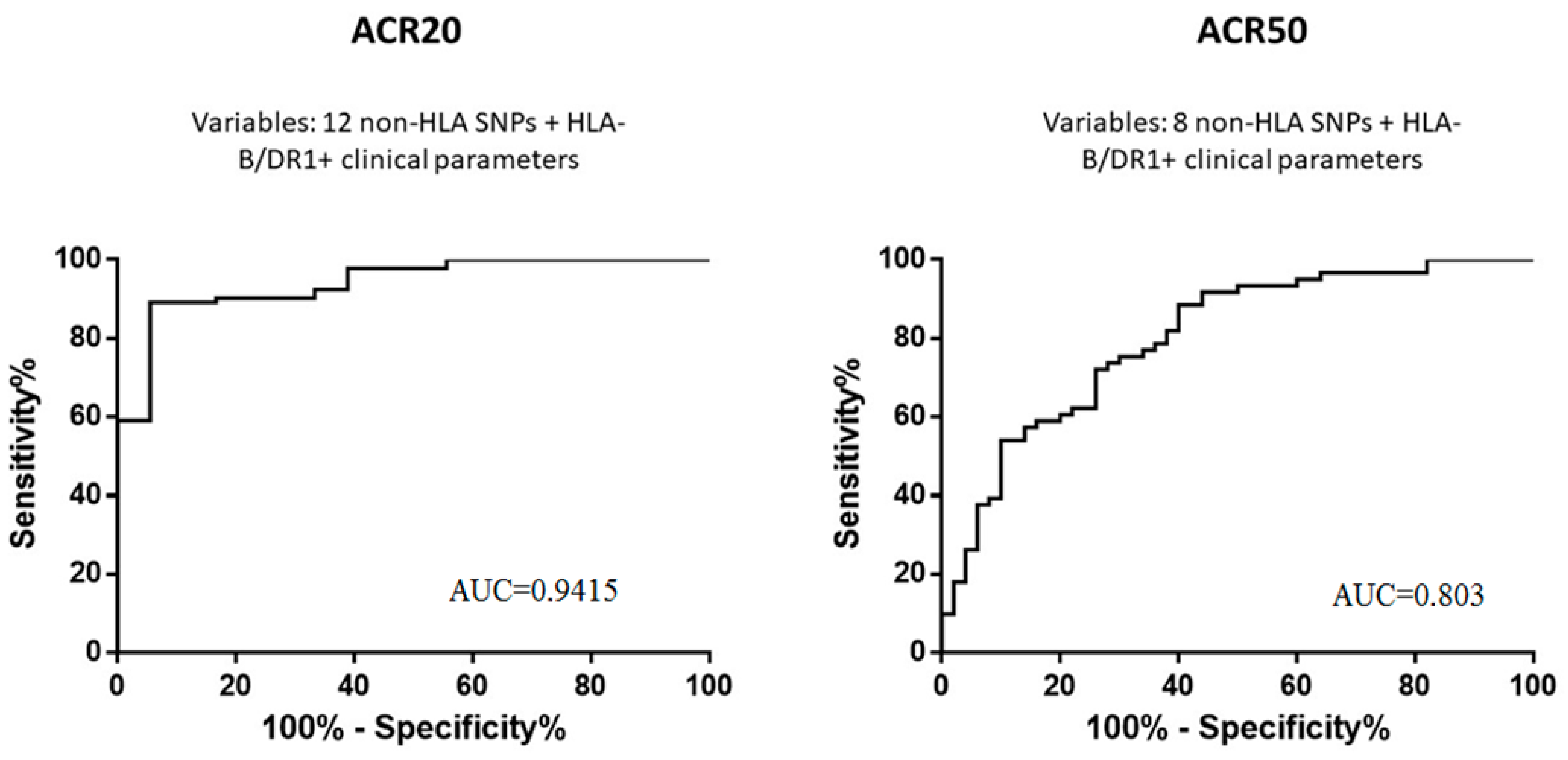
2.2. Associations between Polymorphisms and Characteristics of Olokizumab Efficacy and Safety
2.3. Associations of Polymorphisms with Safety Indicators of Olokizumab Therapy
3. Discussion
4. Materials and Methods
4.1. Sample Characteristics
4.2. DNA Extraction
4.3. HLA Genotyping
4.4. Non-HLA Genotyping
4.5. Statistical Data Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Giannini, D.; Antonucci, M.; Petrelli, F.; Bilia, S.; Alunno, A.; Puxeddu, I. One Year in Review 2020: Pathogenesis of Rheumatoid Arthritis. Clin. Exp. Rheumatol. 2020, 38, 387–397. [Google Scholar] [PubMed]
- Mikhaylenko, D.S.; Nemtsova, M.V.; Bure, I.V.; Kuznetsova, E.B.; Alekseeva, E.A.; Tarasov, V.V.; Lukashev, A.N.; Beloukhova, M.I.; Deviatkin, A.A.; Zamyatnin, A.A. Genetic Polymorphisms Associated with Rheumatoid Arthritis Development and Antirheumatic Therapy Response. Int. J. Mol. Sci. 2020, 21, 4911. [Google Scholar] [CrossRef] [PubMed]
- Smolen, J.S.; Landewé, R.B.M.; Bijlsma, J.W.J.; Burmester, G.R.; Dougados, M.; Kerschbaumer, A.; McInnes, I.B.; Sepriano, A.; van Vollenhoven, R.F.; de Wit, M.; et al. EULAR Recommendations for the Management of Rheumatoid Arthritis with Synthetic and Biological Disease-Modifying Antirheumatic Drugs: 2019 Update. Ann. Rheum. Dis. 2020, 79, 685–699. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szostak, B.; Machaj, F.; Rosik, J.; Pawlik, A. Using Pharmacogenetics to Predict Methotrexate Response in Rheumatoid Arthritis Patients. Expert. Opin. Drug Metab. Toxicol. 2020, 16, 617–626. [Google Scholar] [CrossRef]
- Dedmon, L.E. The Genetics of Rheumatoid Arthritis. Rheumatology 2020, 59, 2661–2670. [Google Scholar] [CrossRef]
- Pallio, G.; Mannino, F.; Irrera, N.; Eid, A.H.; Squadrito, F.; Bitto, A. Polymorphisms Involved in Response to Biological Agents Used in Rheumatoid Arthritis. Biomolecules 2020, 10, 1203. [Google Scholar] [CrossRef]
- Shaw, S.; Bourne, T.; Meier, C.; Carrington, B.; Gelinas, R.; Henry, A.; Popplewell, A.; Adams, R.; Baker, T.; Rapecki, S.; et al. Discovery and Characterization of Olokizumab: A Humanized Antibody Targeting Interleukin-6 and Neutralizing Gp130-Signaling. MAbs 2014, 6, 774–782. [Google Scholar] [CrossRef] [Green Version]
- Kretsos, K.; Golor, G.; Jullion, A.; Hickling, M.; McCabe, S.; Shaw, S.; Jose, J.; Oliver, R. Safety and Pharmacokinetics of Olokizumab, an Anti-IL-6 Monoclonal Antibody, Administered to Healthy Male Volunteers: A Randomized Phase I Study. Clin. Pharmacol. Drug Dev. 2014, 3, 388–395. [Google Scholar] [CrossRef]
- Kretsos, K.; Jullion, A.; Zamacona, M.; Harari, O.; Shaw, S.; Boulanger, B.; Oliver, R. Model-Based Optimal Design and Execution of the First-Inpatient Trial of the Anti-IL-6, Olokizumab. CPT Pharmacomet. Syst. Pharmacol. 2014, 3, e119. [Google Scholar] [CrossRef]
- Takeuchi, T.; Tanaka, Y.; Yamanaka, H.; Amano, K.; Nagamine, R.; Park, W.; Shiozawa, K.; Tsukano, M.; Wei, J.C.-C.; Shao, J.; et al. Efficacy and Safety of Olokizumab in Asian Patients with Moderate-to-Severe Rheumatoid Arthritis, Previously Exposed to Anti-TNF Therapy: Results from a Randomized Phase II Trial. Mod. Rheumatol. 2016, 26, 15–23. [Google Scholar] [CrossRef]
- Tanaka, Y.; Martin Mola, E. IL-6 Targeting Compared to TNF Targeting in Rheumatoid Arthritis: Studies of Olokizumab, Sarilumab and Sirukumab. Ann. Rheum. Dis. 2014, 73, 1595–1597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaplon, H.; Reichert, J.M. Antibodies to Watch in 2021. MAbs 2021, 13, 1860476. [Google Scholar] [CrossRef] [PubMed]
- Karateev, D.E.; Luchikhina, E.L.; Tiurina, L.N.; Chemeris, N.A.; Pogozheva, E.I.; Lukina, G.V.; Potanin, A.I.; Shostak, N.A.; Kogan, K.M.; Demidova, N.V.; et al. Early diagnosis of rheumatoid arthritis in modern clinical practice (results of a follow-up of a Moscow cohort of early arthritis patients participating in the program RADICAL). Ter. Arkh. 2008, 80, 8–13. [Google Scholar] [PubMed]
- Guseva, I.A.; Smirnov, A.V.; Demidova, N.V.; Krylov, M.Y.; Avdeeva, A.S.; Samarkina, E.Y.; Luchikhina, E.L.; Karateev, D.E.; Abramov, D.D.; Nasonov, E.L. Association of Polymorphisms of HLA-DRB1 and TNF-308 G/A with Radiographic Joint Damage in Patients with Early Rheumatoid Arthritis with High Inflammatory Activity, Treated According to the Principle of “Treat to Target” (REMARKA Study). Ter. Arkh. 2018, 90, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, K.; Okada, Y.; Suzuki, A.; Kochi, Y. Genetic Studies of Rheumatoid Arthritis. Proc. Jpn. Acad. Ser. B Phys. Biol. Sci. 2015, 91, 410–422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mukhtar, M.; Sheikh, N.; Batool, A.; Khawar, M.B.; Fatima, N.; Mehmood, R. Novel Functional Polymorphism on PADI-4 Gene and Its Association with Arthritis Onset. Saudi J. Biol. Sci. 2022, 29, 1227–1233. [Google Scholar] [CrossRef]
- Takata, Y.; Inoue, H.; Sato, A.; Tsugawa, K.; Miyatake, K.; Hamada, D.; Shinomiya, F.; Nakano, S.; Yasui, N.; Tanahashi, T.; et al. Replication of Reported Genetic Associations of PADI4, FCRL3, SLC22A4 and RUNX1 Genes with Rheumatoid Arthritis: Results of an Independent Japanese Population and Evidence from Meta-Analysis of East Asian Studies. J. Hum. Genet. 2008, 53, 163–173. [Google Scholar] [CrossRef] [Green Version]
- Baños-Hernández, C.J.; Navarro-Zarza, J.E.; Parra-Rojas, I.; Vázquez-Villamar, M.; Ramón Padilla-Gutiérrez, J.; Valle, Y.; Reyes-Castillo, Z.; Magdalena Torres-Carrillo, N.; García-Arellano, S.; Brennan-Bourdon, L.M.; et al. PADI4 Polymorphisms and the Functional Haplotype Are Associated with Increased Rheumatoid Arthritis Susceptibility: A Replication Study in a Southern Mexican Population. Human Immunol. 2017, 78, 553–558. [Google Scholar] [CrossRef]
- Zhang, L.; Yuan, X.; Zhou, Q.; Shi, J.; Song, Z.; Quan, R.; Zhang, D. Associations Between TNFAIP3 Gene Polymorphisms and Rheumatoid Arthritis Risk: A Meta-Analysis. Arch. Med. Res. 2017, 48, 386–392. [Google Scholar] [CrossRef]
- Magyari, L.; Varszegi, D.; Kovesdi, E.; Sarlos, P.; Farago, B.; Javorhazy, A.; Sumegi, K.; Banfai, Z.; Melegh, B. Interleukins and Interleukin Receptors in Rheumatoid Arthritis: Research, Diagnostics and Clinical Implications. World J. Orthop. 2014, 5, 516–536. [Google Scholar] [CrossRef]
- Vetchinkina, E.A.; Mikhaylenko, D.S.; Kuznetsova, E.B.; Deryagina, T.A.; Alekseeva, E.A.; Bure, I.V.; Zamyatnin, A.A.; Nemtsova, M.V. Genetic Factors of Predisposition and Clinical Characteristics of Rheumatoid Arthritis in Russian Patients. J. Pers. Med. 2021, 11, 469. [Google Scholar] [CrossRef] [PubMed]
- Verma, R.; Yadav, M.; Pradhan, D.; Bhuyan, R.; Aggarwal, S.; Nayek, A.; Jain, A.K. Probing Binding Mechanism of Interleukin-6 and Olokizumab: In Silico Design of Potential Lead Antibodies for Autoimmune and Inflammatory Diseases. J. Recept. Signal. Transduct. Res. 2016, 36, 601–616. [Google Scholar] [CrossRef] [PubMed]
- Nasonov, E.; Fatenejad, S.; Feist, E.; Ivanova, M.; Korneva, E.; Krechikova, D.G.; Maslyanskiy, A.L.; Samsonov, M.; Stoilov, R.; Zonova, E.V.; et al. Olokizumab, a Monoclonal Antibody against Interleukin 6, in Combination with Methotrexate in Patients with Rheumatoid Arthritis Inadequately Controlled by Methotrexate: Efficacy and Safety Results of a Randomised Controlled Phase III Study. Ann. Rheum. Dis. 2022, 81, 469–479. [Google Scholar] [CrossRef] [PubMed]
- Bure, I.V.; Mikhaylenko, D.S.; Kuznetsova, E.B.; Alekseeva, E.A.; Bondareva, K.I.; Kalinkin, A.I.; Lukashev, A.N.; Tarasov, V.V.; Zamyatnin, A.A.; Nemtsova, M.V. Analysis of MiRNA Expression in Patients with Rheumatoid Arthritis during Olokizumab Treatment. J. Pers. Med. 2020, 10, 205. [Google Scholar] [CrossRef] [PubMed]
- Birkner, B.; Rech, J.; Stargardt, T. Cost-Utility Analysis of de-Escalating Biological Disease-Modifying Anti-Rheumatic Drugs in Patients with Rheumatoid Arthritis. PLoS ONE 2020, 15, e0226754. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Gene | SNP | Genotype | OR (CI 95%) | p | Model | Sample | Effect |
|---|---|---|---|---|---|---|---|
| ACR20 | |||||||
| TNFRSF1A | rs767455 | C/C | 5.62 (1.42–22.29) | 0.0140 | R | A | ↑ |
| IL23R | rs1884444 | T/T | 5.47 (1.65–18.14) | 0.0055 | R | A | ↑ |
| IL1B | rs1143634 | G/A | 2.90 (1.05–8.01) | 0.0403 | OD | A | ↑ |
| ABCB1 | rs2032582 | A/C-C/C | 2.63 (1.00–6.91) | 0.0493 | D | UA | ↑ |
| FPGS | rs10987742 * | C/T | 2.47 (1.07–5.68) | 0.0334 | OD | UA | ↑ |
| AMPD1 | rs17602729 * | A/A | 0.12 (0.02–0.89) | 0.0384 | R | A | ↓ |
| PADI4 | rs2240336 * | C/T-T/T | 0.28 (0.10–0.78) | 0.0142 | D | A | ↓ |
| ABCC1 | rs3784864 * | A/A | 0.31 (0.13–0.75) | 0.0095 | R | A | ↓ |
| IL6R | rs2228145 * | A/C-C/C | 0.38 (0.16–0.94) | 0.0372 | D | A | ↓ |
| TLR5 | rs5744174 | A/G | 0.41 (0.17–0.98) | 0.0458 | OD | A | ↓ |
| ACR50 | |||||||
| IL17A | rs1974226 | C/T-T/T | 2.38 (1.08–5.26) | 0.0319 | D | UA | ↑ |
| IL1B | rs16944 | G/G | 2.18 (1.02–4.66) | 0.0447 | R | A | ↑ |
| ABCB1 | rs1045642 | A/G | 2.18 (1.06–4.49) | 0.0349 | OD | UA | ↑ |
| AMPD1 | rs17602729 * | G/A-A/A | 0.38 (0.16–0.91) | 0.0309 | D | A | ↓ |
| ABCC1 | rs3784864 * | A/A | 0.43 (0.18–1.00) | 0.0488 | R | UA | ↓ |
| IL1B | rs1143623 | C/G-G/G | 0.46 (0.22–0.99) | 0.0457 | D | A | ↓ |
| DAS28-CRP | |||||||
| FPGS | rs10987742 * | C/T-T/T | 2.20 (1.05–4.61) | 0.0359 | D | UA | ↑ |
| IL6R | rs2228145 * | A/C-C/C | 0.38 (0.17–0.84) | 0.0170 | D | A | ↓ |
| PADI4 | rs2240336 * | C/T-T/T | 0.39 (0.17–0.89) | 0.0247 | D | A | ↓ |
| Gene | SNP | Genotype | OR (95% CI) | p | Model | Sample | Effect |
|---|---|---|---|---|---|---|---|
| ACR20 | |||||||
| PADI4 | rs1748032 * | T/T | 5.23 (1.09–25.04) | 0.0382 | CD | A | ↑ |
| IL23R | rs7539625 | G/A-A/A | 3.07 (1.03–9.15) | 0.0446 | D | A | ↑ |
| PADI4 | rs2240336 | C/T-T/T | 3.00 (1.07–8.47) | 0.0375 | D | A | ↑ |
| PADI4 | rs2301888 * | G/A-A/A | 2.94 (1.06–8.15) | 0.0387 | D | A | ↑ |
| PADI4 | rs2240335 | C/A-A/A | 2.85 (1.04–7.78) | 0.0415 | D | A | ↑ |
| IL17A | rs1974226 | A/A | 0.12 (0.02–0.79) | 0.0274 | R | A | ↓ |
| IL1B | rs1143634 * | A/A | 0.21 (0.05–0.93) | 0.0400 | R | A | ↓ |
| GLCCI1 | rs37972 | C/C | 0.23 (0.08–0.64) | 0.0047 | R | A | ↓ |
| DHODH | rs3213422 * | A/C | 0.30 (0.11–0.88) | 0.0283 | OD | A | ↓ |
| CCR6 | rs3093024 | A/G | 0.32 (0.12–0.87) | 0.0261 | OD | UA | ↓ |
| TNFAIP3 | rs6920220 | G/A-A/A | 0.35 (0.13–0.95) | 0.0393 | D | A | ↓ |
| ACR50 | |||||||
| IL18 | rs360722 | G/G | 2.75 (1.09–6.94) | 0.0322 | R | A | ↑ |
| IL1RN | rs419598 * | T/C | 2.24 (1.01–5.01) | 0.0483 | OD | A | ↑ |
| ABCB1 | rs2032582 | A/C | 2.18 (1.03–4.63) | 0.0418 | OD | A | ↑ |
| PADI4 | rs2301888 * | G/A | 2.17 (1.00–4.70) | 0.0489 | OD | A | ↑ |
| IL1B | rs1143634 * | A/A | 0.13 (0.02–0.83) | 0.0313 | R | A | ↓ |
| TLR5 | rs5744174 | A/G-G/G | 0.31 (0.12–0.77) | 0.0124 | D | A | ↓ |
| DHODH | rs3213422 * | A/C | 0.41 (0.19–0.88 | 0.0218 | OD | A | ↓ |
| ABCC1 | rs3784864 | A/A | 0.42 (0.18–0.97) | 0.0428 | R | A | ↓ |
| DAS28-CRP | |||||||
| PADI4 | rs1748032 * | C/T-T/T | 4.78(1.30–17.54) | 0.0184 | D | A | ↑ |
| IL1B | rs16944 | G/G | 2.43 (1.10–5.35) | 0.0279 | R | A | ↑ |
| IL1RN | rs419598 * | C/C | 0.21 (0.04–0.94) | 0.0412 | R | A | ↓ |
| TNFRSF1A | rs1800692 | A/G-G/G | 0.37 (0.14–1.00) | 0.0495 | D | A | ↓ |
| Gene | SNP | Genotype | OR (95% CI) | p | Model | Risk |
|---|---|---|---|---|---|---|
| Infectious complications | ||||||
| IL2RB | rs3218253 | A/A | 8.87 (1.39–56.54) | 0.0210 | R | ↑ |
| DHODH | rs3213422 | C/C | 3.53 (1.31–9.54) | 0.0128 | R | ↑ |
| TNFRSF1A | rs767455 * | T/C | 3.03 (1.09–8.41) | 0.0331 | OD | ↑ |
| IL17A | rs1974226 * | C/T-T/T | 0.16 (0.03–0.93) | 0.0406 | D | ↓ |
| IL1B | rs16944 | G/G | 0.22 (0.06–0.88) | 0.0323 | CD | ↓ |
| TNFRSF1A | rs1800692 | G/G | 0.26 (0.08–0.87) | 0.0293 | R | ↓ |
| Potential hepatotoxicity | ||||||
| IL17A | rs1974226 * | C/T-T/T | 10.44 (2.37–46.03) | 0.0019 | D | ↑ |
| PADI4 | rs874881 | G/C | 7.40 (1.25–43.63) | 0.0270 | OD | ↑ |
| IL2RA | rs2104286 | C/C | 7.29 (1.19–44.56) | 0.0316 | R | ↑ |
| IL18 | rs360718 | C/C | 5.91 (1.03–33.84) | 0.0460 | R | ↑ |
| IL23R | rs1884444 | G/T | 4.57 (1.05–19.84) | 0.0426 | OD | ↑ |
| PADI4 | rs2240340 | T/C | 2.43 (1.16–5.10) | 0.0184 | OD | ↑ |
| PADI4 | rs11203366 | G/A | 2.31 (1.10–4.83) | 0.0263 | OD | ↑ |
| TNFRSF1A | rs767455 * | T/C | 2.10 (1.01–4.37) | 0.0467 | OD | ↑ |
| STAT4 | rs7574865 | T/G-G/G | 0.11 (0.02–0.53) | 0.0062 | D | ↓ |
| PADI4 | rs2240335 | A/A | 0.14 (0.02–0.82) | 0.0291 | R | ↓ |
| PADI4 | rs2301888 | A/A | 0.14 (0.02–0.82) | 0.0291 | R | ↓ |
| PADI4 | rs2240336 | T/T | 0.22 (0.05–0.90) | 0.0357 | R | ↓ |
| AMPD1 | rs17602729 | G/A-A/A | 0.39 (0.16–0.93) | 0.0345 | D | ↓ |
| PADI4 | rs11203367 | C/C | 0.39 (0.16–0.93) | 0.0345 | R | ↓ |
| IL1B | rs1143634 | G/A-A/A | 0.43 (0.20–0.94) | 0.0340 | D | ↓ |
| № | Variables | Statistical Values |
|---|---|---|
| Anthropometric data | ||
| 1 | Age (mean ± SD; min/max), years | 50.4 ± 13.14; 22/82 |
| 2 | Weight (mean ± SD ± CO; min/max), kg | 73.63 ± 16.36; 41/131 |
| RA severity | ||
| 3 | Disease duration (mean ± SD; min/max), years | 5.91 ± 1.214; 2.61/11.16 |
| 4 | Disease severity based on DAS28- CRP (mean ± SD; min/max), scores moderate (DAS28-CRP > 3.2 to ≤5.1), subjects high (DAS28-CRP > 5.1), subjects | 5.94 ± 0.64; 4.5/8.1 10 (8%) 113 (90.4%) |
| 5 | Disease severity based on CDAI (mean ± SD; min/max), scores | 39.43 ± 8.7; 24.8/69.3 |
| 6 | Disease severity based on HAQ-DI (mean ± SD; min/max), scores | 1.68 ± 0.5; 0.13/2.86 |
| Laboratory parameters | ||
| 7 | RF level (mean ± SD; min/max), IU/mL among them ≥ 15 IU/mL: | 192.2 ± 240.95; 7/1540 84% (105/125) |
| 8 | Anti-CCP level (mean ± SD; min/max), IU/mL among them > 10 ME/mL | 664.35 ± 999.31; 0.4/6044.8 80.8% 101/125 |
| 9 | CRP level (mean ± SD; min/max), mg/mL | 21.0 ± 20.83; 1/120 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mikhaylenko, D.S.; Kuznetsova, E.B.; Musatova, V.V.; Bure, I.V.; Deryagina, T.A.; Alekseeva, E.A.; Tarasov, V.V.; Zamyatnin, A.A., Jr.; Nemtsova, M.V. Genetic and Clinical Factors Associated with Olokizumab Treatment in Russian Patients with Rheumatoid Arthritis. J. Pers. Med. 2022, 12, 641. https://doi.org/10.3390/jpm12040641
Mikhaylenko DS, Kuznetsova EB, Musatova VV, Bure IV, Deryagina TA, Alekseeva EA, Tarasov VV, Zamyatnin AA Jr., Nemtsova MV. Genetic and Clinical Factors Associated with Olokizumab Treatment in Russian Patients with Rheumatoid Arthritis. Journal of Personalized Medicine. 2022; 12(4):641. https://doi.org/10.3390/jpm12040641
Chicago/Turabian StyleMikhaylenko, Dmitry S., Ekaterina B. Kuznetsova, Viktoria V. Musatova, Irina V. Bure, Tatiana A. Deryagina, Ekaterina A. Alekseeva, Vadim V. Tarasov, Andrey A. Zamyatnin, Jr., and Marina V. Nemtsova. 2022. "Genetic and Clinical Factors Associated with Olokizumab Treatment in Russian Patients with Rheumatoid Arthritis" Journal of Personalized Medicine 12, no. 4: 641. https://doi.org/10.3390/jpm12040641