
Intravoxel Incoherent Motion (IVIM) MR Quantification in Locally Advanced Cervical Cancer (LACC): Preliminary Study on Assessment of Tumor Aggressiveness and Response to Neoadjuvant Chemotherapy

 ,
,  , , , , , ,
, , , , , ,
Abstract
:1. Introduction
1.1. Background
1.2. Purpose
2. Materials and Methods
2.1. Patients
2.2. MR Protocol
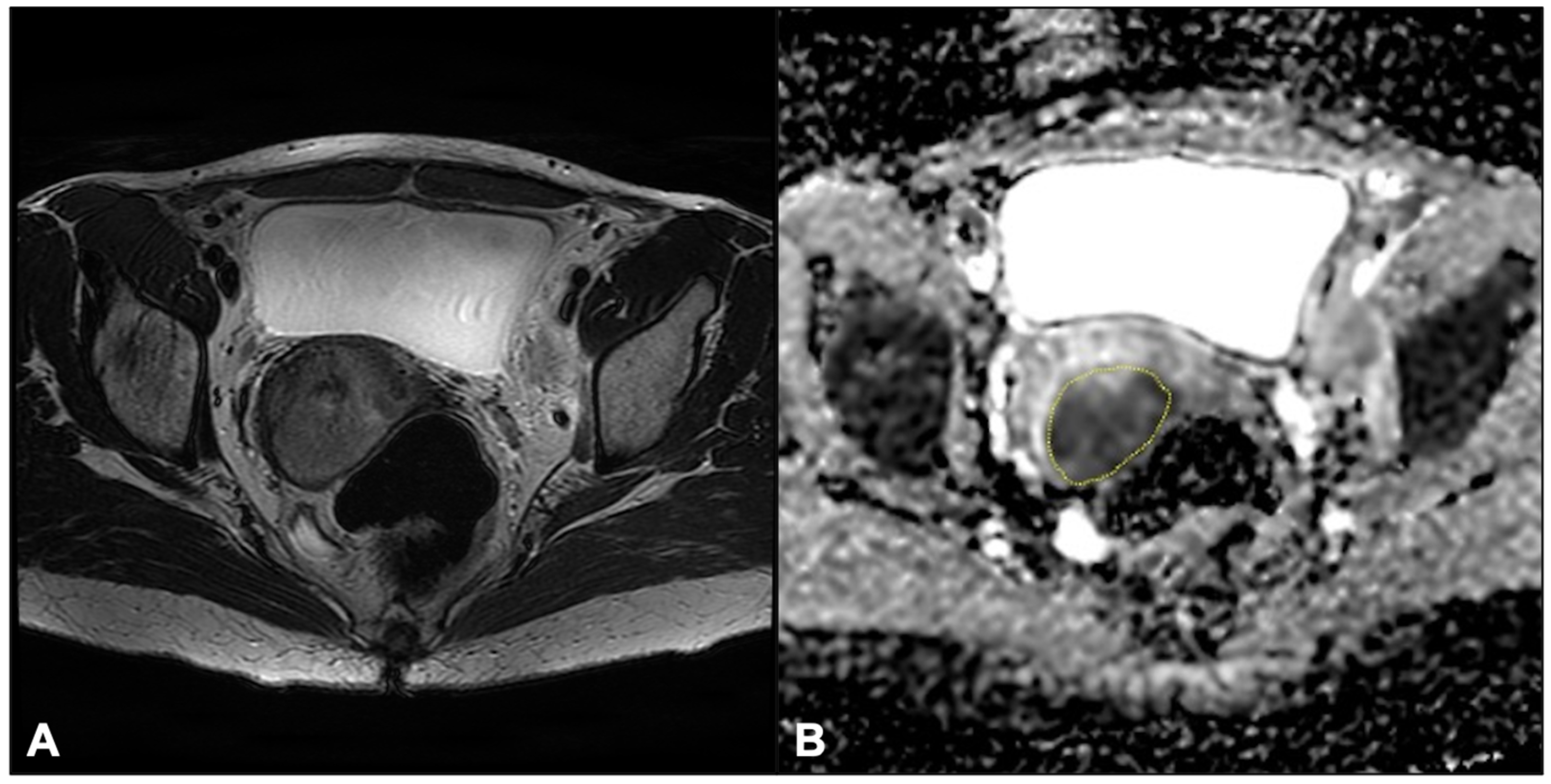
2.3. Image Analysis
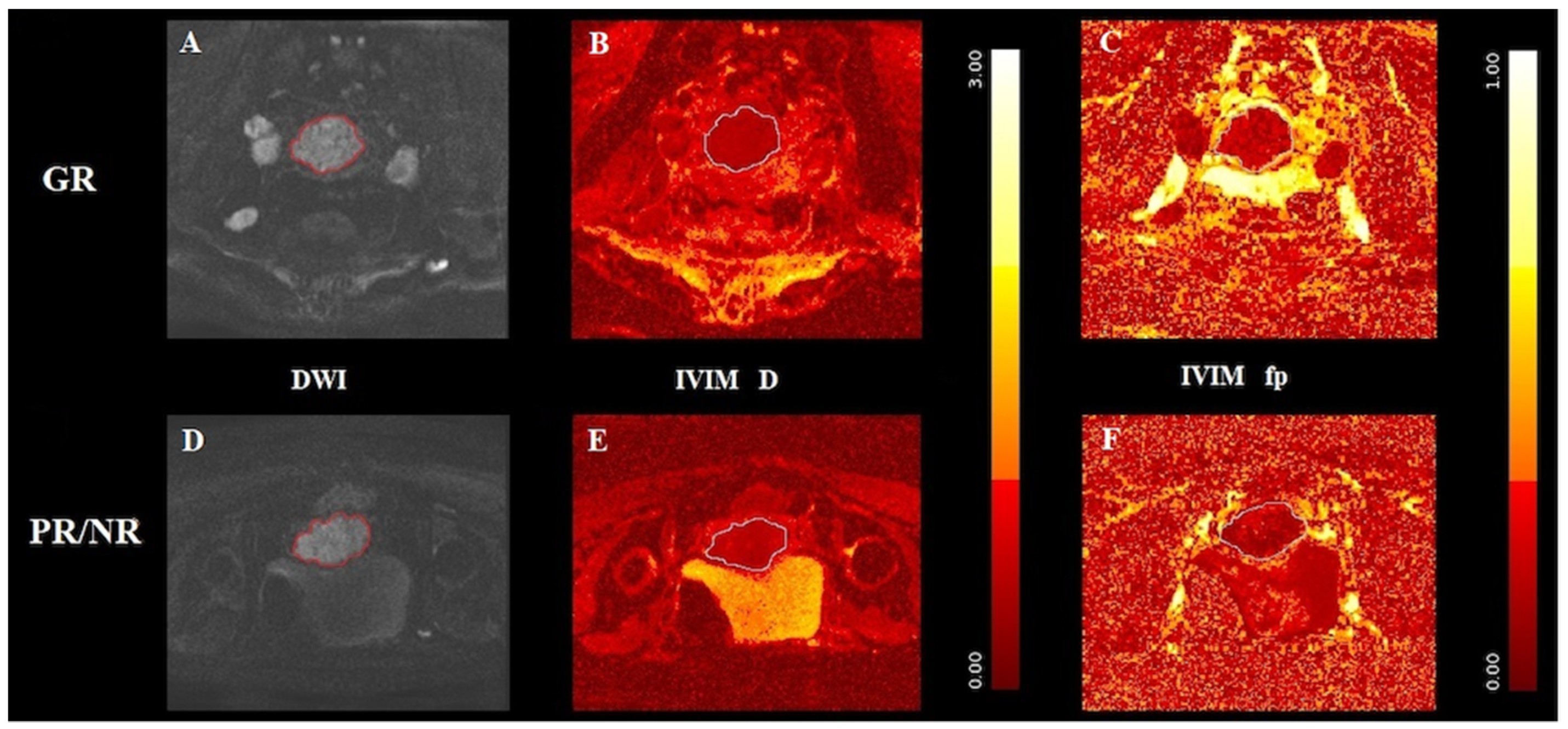
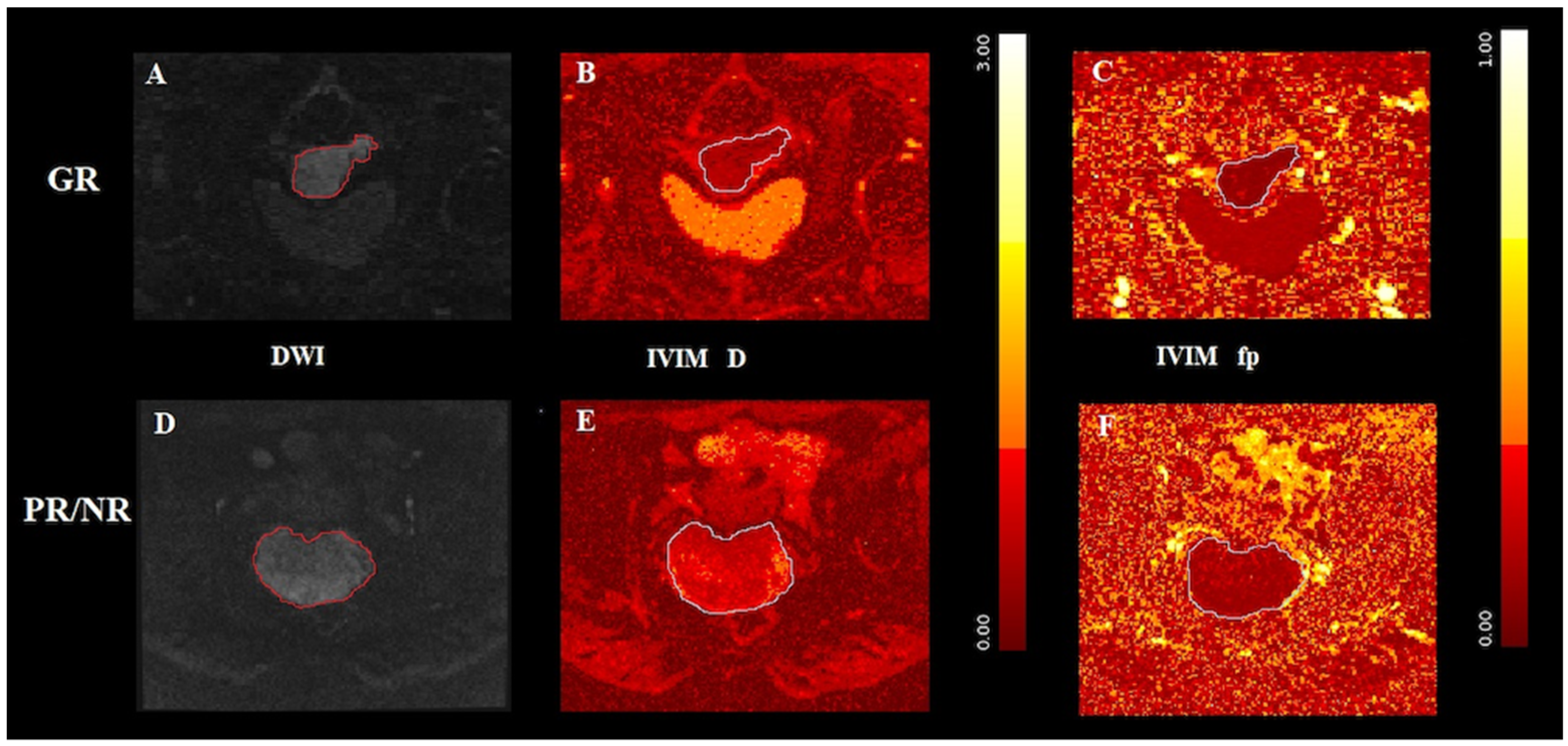
2.3.1. DWI-IVIM
2.3.2. ADC
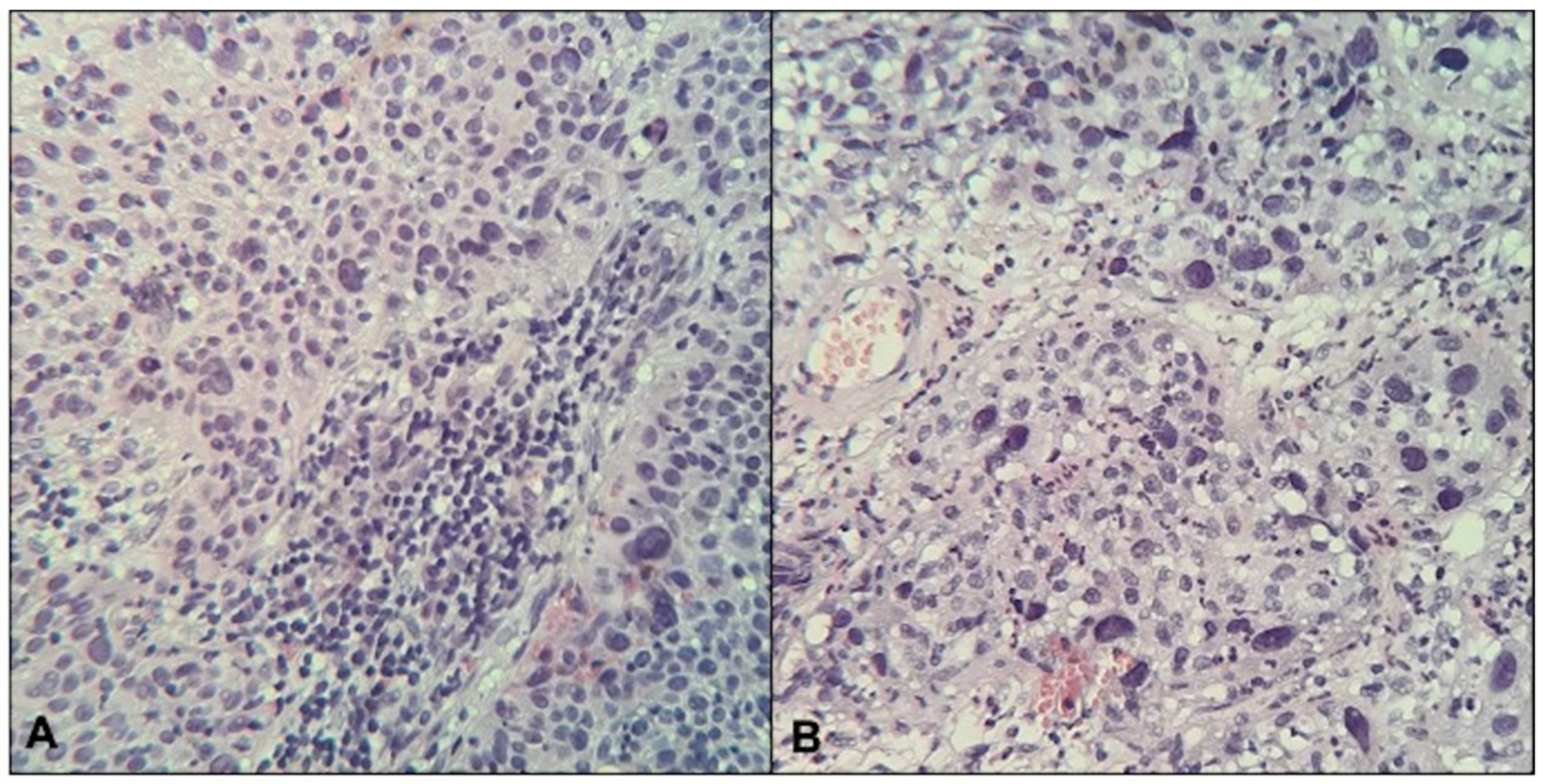
2.4. Histological Analysis
2.5. Statistical Analysis
3. Results
3.1. Patients and Histological Features
3.2. MR Quantitative Data
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Arbyn, M.; Weiderpass, E.; Bruni, L.; de Sanjosé, S.; Saraiya, M.; Ferlay, J.; Bray, F. Estimates of Incidence and Mortality of Cervical Cancer in 2018: A Worldwide Analysis. Lancet Glob. Health 2020, 8, e191–e203. [Google Scholar] [CrossRef] [Green Version]
- Brisson, M.; Kim, J.J.; Canfell, K.; Drolet, M.; Gingras, G.; Burger, E.A.; Martin, D.; Simms, K.T.; Bénard, É.; Boily, M.-C.; et al. Impact of HPV Vaccination and Cervical Screening on Cervical Cancer Elimination: A Comparative Modelling Analysis in 78 Low-Income and Lower-Middle-Income Countries. Lancet 2020, 395, 575–590. [Google Scholar] [CrossRef] [Green Version]
- Shrestha, A.D.; Neupane, D.; Vedsted, P.; Kallestrup, P. Cervical Cancer Prevalence, Incidence and Mortality in Low and Middle Income Countries: A Systematic Review. Asian Pac. J. Cancer Prev. 2018, 19, 319. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global Cancer Statistics 2018: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Bhatla, N.; Berek, J.S.; Cuello Fredes, M.; Denny, L.A.; Grenman, S.; Karunaratne, K.; Kehoe, S.T.; Konishi, I.; Olawaiye, A.B.; Prat, J.; et al. Revised FIGO Staging for Carcinoma of the Cervix Uteri. Int. J. Gynecol. Obstet. 2019, 145, 129–135. [Google Scholar] [CrossRef]
- Koh, W.-J.; Abu-Rustum, N.R.; Bean, S.; Bradley, K.; Campos, S.M.; Cho, K.R.; Chon, H.S.; Chu, C.; Clark, R.; Cohn, D.; et al. Cervical Cancer, Version 3.2019, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc. Netw. 2019, 17, 64–84. [Google Scholar] [CrossRef] [Green Version]
- Gadducci, A.; Cosio, S. Neoadjuvant Chemotherapy in Locally Advanced Cervical Cancer: Review of the Literature and Perspectives of Clinical Research. Anticancer Res. 2020, 40, 4819–4828. [Google Scholar] [CrossRef]
- Marth, C.; Landoni, F.; Mahner, S.; McCormack, M.; Gonzalez-Martin, A.; Colombo, N. Cervical Cancer: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2017, 28, iv72–iv83. [Google Scholar] [CrossRef]
- Takeda, N.; Sakuragi, N.; Takeda, M.; Okamoto, K.; Kuwabara, M.; Negishi, H.; Oikawa, M.; Yamamoto, R.; Yamada, H.; Fujimoto, S. Multivariate Analysis of Histopathologic Prognostic Factors for Invasive Cervical Cancer Treated with Radical Hysterectomy and Systematic Retroperitoneal Lymphadenectomy: Prognostic Factors for Patients with Cervical Cancer Treated with Radical Hysterectomy. Acta Obstet. Gynecol. Scand. 2002, 81, 1144–1151. [Google Scholar] [CrossRef]
- Jeong, S.Y.; Park, H.; Kim, M.S.; Kang, J.H.; Paik, E.S.; Lee, Y.-Y.; Kim, T.J.; Lee, J.W.; Kim, B.-G.; Bae, D.S.; et al. Pretreatment Lymph Node Metastasis as a Prognostic Significance in Cervical Cancer: Comparison between Disease Status. Cancer Res. Treat. 2020, 52, 516–523. [Google Scholar] [CrossRef]
- Matsutani, S.; Shibutani, M.; Maeda, K.; Nagahara, H.; Fukuoka, T.; Nakao, S.; Hirakawa, K.; Ohira, M. Significance of Tumor-infiltrating Lymphocytes before and after Neoadjuvant Therapy for Rectal Cancer. Cancer Sci. 2018, 109, 966–979. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stanton, S.E.; Disis, M.L. Clinical Significance of Tumor-Infiltrating Lymphocytes in Breast Cancer. J. Immunother. Cancer 2016, 4, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Jong, R.A.; Leffers, N.; Boezen, H.M.; ten Hoor, K.A.; van der Zee, A.G.J.; Hollema, H.; Nijman, H.W. Presence of Tumor-Infiltrating Lymphocytes Is an Independent Prognostic Factor in Type I and II Endometrial Cancer. Gynecol. Oncol. 2009, 114, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Meng, Y.; Liang, H.; Hu, J.; Liu, S.; Hao, X.; Wong, M.S.K.; Li, X.; Hu, L. PD-L1 Expression Correlates With Tumor Infiltrating Lymphocytes And Response To Neoadjuvant Chemotherapy In Cervical Cancer. J. Cancer 2018, 9, 2938–2945. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Li, Z.; Gao, A.; Wen, Q.; Sun, Y. The Prognostic Landscape of Tumor-Infiltrating Immune Cells in Cervical Cancer. Biomed. Pharmacother. 2019, 120, 109444. [Google Scholar] [CrossRef] [PubMed]
- D’Alessandris, N.; Palaia, I.; Pernazza, A.; Tomao, F.; Di Pinto, A.; Musacchio, L.; Leopizzi, M.; Di Maio, V.; Pecorella, I.; Benedetti Panici, P.; et al. PD-L1 Expression Is Associated with Tumor Infiltrating Lymphocytes That Predict Response to NACT in Squamous Cell Cervical Cancer. Virchows Arch. 2021, 478, 517–525. [Google Scholar] [CrossRef]
- Palaia, I.; Tomao, F.; Di Pinto, A.; Pernazza, A.; Santangelo, G.; D’Alessandris, N.; Manganaro, L.; Arno, A.; Donato, V.D.; Perniola, G.; et al. Response to Neoadjuvant Chemotherapy in Locally Advanced Cervical Cancer: The Role of Immune-Related Factors. In Vivo 2021, 35, 1277–1283. [Google Scholar] [CrossRef]
- Manganaro, L.; Lakhman, Y.; Bharwani, N.; Gui, B.; Gigli, S.; Vinci, V.; Rizzo, S.; Kido, A.; Cunha, T.M.; Sala, E.; et al. Staging, Recurrence and Follow-up of Uterine Cervical Cancer Using MRI: Updated Guidelines of the European Society of Urogenital Radiology after Revised FIGO Staging 2018. Eur. Radiol. 2021, 31, 7802–7816. [Google Scholar] [CrossRef]
- Kato, F.; Kudo, K.; Yamashita, H.; Baba, M.; Shimizu, A.; Oyama-Manabe, N.; Kinoshita, R.; Li, R.; Shirato, H. Predicting Metastasis in Clinically Negative Axillary Lymph Nodes with Minimum Apparent Diffusion Coefficient Value in Luminal A-like Breast Cancer. Breast Cancer 2019, 26, 628–636. [Google Scholar] [CrossRef]
- Boraschi, P.; Donati, F.; Cervelli, R.; Pacciardi, F.; Tarantini, G.; Castagna, M.; Urbani, L.; Lencioni, R. Colorectal Liver Metastases: ADC as an Imaging Biomarker of Tumor Behavior and Therapeutic Response. Eur. J. Radiol. 2021, 137, 109609. [Google Scholar] [CrossRef]
- Zhang, P.; Cui, Y.; Li, W.; Ren, G.; Chu, C.; Wu, X. Diagnostic Accuracy of Diffusion-Weighted Imaging with Conventional MR Imaging for Differentiating Complex Solid and Cystic Ovarian Tumors at 1.5T. World J. Surg. Onc. 2012, 10, 237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Ye, Z.; Sun, H.; Bai, R. Grading of Uterine Cervical Cancer by Using the ADC Difference Value and Its Correlation with Microvascular Density and Vascular Endothelial Growth Factor. Eur. Radiol. 2013, 23, 757–765. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.; Qiang, J.W.; Tian, H.P.; Chen, B.; Wang, A.J.; Zhao, J.G. Minimum Apparent Diffusion Coefficient for Predicting Lymphovascular Invasion in Invasive Cervical Cancer: ADC for Predicting Lymphovascular Invasion. J. Magn. Reson. Imaging 2017, 45, 1771–1779. [Google Scholar] [CrossRef] [PubMed]
- Song, Q.; Yu, Y.; Zhang, X.; Zhu, Y.; Luo, Y.; Yu, T.; Sun, J.; Liu, F.; Dong, Y. Value of MRI and Diffusion Weighted Imaging in Diagnosing Normal-Sized Pelvic Lymph Nodes Metastases in Patients with Cervical Cancer. BJR 2020, 93, 20200203. [Google Scholar] [CrossRef] [PubMed]
- Akkus Yildirim, B.; Onal, C.; Erbay, G.; Cem Guler, O.; Karadeli, E.; Reyhan, M.; Koc, Z. Prognostic Values of ADCmean and SUVmax of the Primary Tumour in Cervical Cancer Patients Treated with Definitive Chemoradiotherapy. J. Obstet. Gynaecol. 2019, 39, 224–230. [Google Scholar] [CrossRef]
- Wang, Y.-T.; Li, Y.-C.; Yin, L.-L.; Pu, H. Can Diffusion-Weighted Magnetic Resonance Imaging Predict Survival in Patients with Cervical Cancer? A Meta-Analysis. Eur. J. Radiol. 2016, 85, 2174–2181. [Google Scholar] [CrossRef]
- Gu, K.; Kim, C.K.; Choi, C.H.; Yoon, Y.C.; Park, W. Prognostic Value of ADC Quantification for Clinical Outcome in Uterine Cervical Cancer Treated with Concurrent Chemoradiotherapy. Eur. Radiol. 2019, 29, 6236–6244. [Google Scholar] [CrossRef]
- Capuani, S.; Guerreri, M.; Antonelli, A.; Bernardo, S.; Porpora, M.G.; Giancotti, A.; Catalano, C.; Manganaro, L. Diffusion and Perfusion Quantified by Magnetic Resonance Imaging Are Markers of Human Placenta Development in Normal Pregnancy. Placenta 2017, 58, 33–39. [Google Scholar] [CrossRef]
- Satta, S.; Dolciami, M.; Celli, V.; Di Stadio, F.; Perniola, G.; Palaia, I.; Pernazza, A.; Della Rocca, C.; Rizzo, S.; Catalano, C.; et al. Quantitative Diffusion and Perfusion MRI in the Evaluation of Endometrial Cancer: Validation with Histopathological Parameters. BJR 2021, 94, 20210054. [Google Scholar] [CrossRef]
- Le Bihan, D.; Breton, E.; Lallemand, D.; Aubin, M.L.; Vignaud, J.; Laval-Jeantet, M. Separation of Diffusion and Perfusion in Intravoxel Incoherent Motion MR Imaging. Radiology 1988, 168, 497–505. [Google Scholar] [CrossRef]
- Iima, M.; Le Bihan, D. Clinical Intravoxel Incoherent Motion and Diffusion MR Imaging: Past, Present, and Future. Radiology 2016, 278, 13–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, E.Y.P.; Yu, X.; Chu, M.M.Y.; Ngan, H.Y.S.; Siu, S.W.K.; Soong, I.S.; Chan, Q.; Khong, P.-L. Perfusion and Diffusion Characteristics of Cervical Cancer Based on Intraxovel Incoherent Motion MR Imaging-a Pilot Study. Eur. Radiol. 2014, 24, 1506–1513. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Song, J.; Zhou, S.; Lu, Y.; Lin, W.; Koh, T.S.; Hou, Z.; Yan, Z. A Comparative Study of Methods for Determining Intravoxel Incoherent Motion Parameters in Cervix Cancer. Cancer Imaging 2021, 21, 12. [Google Scholar] [CrossRef]
- Song, J.; Lu, Y.; Wang, X.; Peng, W.; Lin, W.; Hou, Z.; Yan, Z. A Comparative Study of Four Diffusion-Weighted Imaging Models in the Diagnosis of Cervical Cancer. Acta Radiol. 2021, 63, 028418512110020. [Google Scholar] [CrossRef]
- Xu, C.; Li, X.; Shi, Y.; Wang, B.; Sun, H. Combinative Evaluation of Primary Tumor and Lymph Nodes to Predict Pelvic Lymphatic Metastasis in Cervical Cancer: An Integrated PET-IVIM MRI Study. Cancer Imaging 2020, 20, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, C.; Du, S.; Zhang, S.; Wang, B.; Dong, C.; Sun, H. Value of Integrated PET-IVIM MR in Assessing Metastases in Hypermetabolic Pelvic Lymph Nodes in Cervical Cancer: A Multi-Parameter Study. Eur. Radiol. 2020, 30, 2483–2492. [Google Scholar] [CrossRef] [PubMed]
- Perucho, J.A.U.; Chiu, K.W.H.; Wong, E.M.F.; Tse, K.Y.; Chu, M.M.Y.; Chan, L.W.C.; Pang, H.; Khong, P.-L.; Lee, E.Y.P. Diffusion-Weighted Magnetic Resonance Imaging of Primary Cervical Cancer in the Detection of Sub-Centimetre Metastatic Lymph Nodes. Cancer Imaging 2020, 20, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perucho, J.A.U.; Wang, M.; Vardhanabhuti, V.; Tse, K.Y.; Chan, K.K.L.; Lee, E.Y.P. Association between IVIM Parameters and Treatment Response in Locally Advanced Squamous Cell Cervical Cancer Treated by Chemoradiotherapy. Eur. Radiol. 2021, 31, 7845–7854. [Google Scholar] [CrossRef]
- Zheng, X.; Guo, W.; Dong, J.; Qian, L. Prediction of Early Response to Concurrent Chemoradiotherapy in Cervical Cancer: Value of Multi-Parameter MRI Combined with Clinical Prognostic Factors. Magn. Reson. Imaging 2020, 72, 159–166. [Google Scholar] [CrossRef]
- Zhang, H.; Zhou, Y.; Li, J.; Zhang, P.; Li, Z.; Guo, J. The Value of DWI in Predicting the Response to Synchronous Radiochemotherapy for Advanced Cervical Carcinoma: Comparison among Three Mathematical Models. Cancer Imaging 2020, 20, 8. [Google Scholar] [CrossRef]
- Wang, Y.-C.; Hu, D.-Y.; Hu, X.-M.; Shen, Y.-Q.; Meng, X.-Y.; Tang, H.; Li, Z. Assessing the Early Response of Advanced Cervical Cancer to Neoadjuvant Chemotherapy Using Intravoxel Incoherent Motion Diffusion-Weighted Magnetic Resonance Imaging: A Pilot Study. Chin. Med. J. 2016, 129, 665–671. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New Response Evaluation Criteria in Solid Tumours: Revised RECIST Guideline (Version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Maiuro, A.; Antonelli, A.; Manganaro, L.; Capuani, S. Molecular Diffusion and Perfusion of Biological Water Quantified by MRI for the Diagnosis of Pathological Human Placentas. Il Nuovo Cim. C 2020, 43, 1–5. [Google Scholar] [CrossRef]
- Hendry, S.; Salgado, R.; Gevaert, T.; Russell, P.A.; John, T.; Thapa, B.; Christie, M.; van de Vijver, K.; Estrada, M.V.; Gonzalez-Ericsson, P.I.; et al. Assessing Tumor-Infiltrating Lymphocytes in Solid Tumors: A Practical Review for Pathologists and Proposal for a Standardized Method from the International Immuno-Oncology Biomarkers Working Group: Part 2: TILs in Melanoma, Gastrointestinal Tract Carcinomas, Non–Small Cell Lung Carcinoma and Mesothelioma, Endometrial and Ovarian Carcinomas, Squamous Cell Carcinoma of the Head and Neck, Genitourinary Carcinomas, and Primary Brain Tumors. Adv. Anat. Pathol. 2017, 24, 311–335. [Google Scholar] [CrossRef]
- Badalamenti, G.; Fanale, D.; Incorvaia, L.; Barraco, N.; Listì, A.; Maragliano, R.; Vincenzi, B.; Calò, V.; Iovanna, J.L.; Bazan, V.; et al. Role of Tumor-Infiltrating Lymphocytes in Patients with Solid Tumors: Can a Drop Dig a Stone? Cell. Immunol. 2019, 343, 103753. [Google Scholar] [CrossRef]
- Williams, N.L.; Werner, T.L.; Jarboe, E.A.; Gaffney, D.K. Adenocarcinoma of the Cervix: Should We Treat It Differently? Curr. Oncol. Rep. 2015, 17, 17. [Google Scholar] [CrossRef]
- Winfield, J.M.; Orton, M.R.; Collins, D.J.; Ind, T.E.J.; Attygalle, A.; Hazell, S.; Morgan, V.A.; deSouza, N.M. Separation of Type and Grade in Cervical Tumours Using Non-Mono-Exponential Models of Diffusion-Weighted MRI. Eur. Radiol. 2017, 27, 627–636. [Google Scholar] [CrossRef] [Green Version]
- Becker, A.S.; Perucho, J.A.; Wurnig, M.C.; Boss, A.; Ghafoor, S.; Khong, P.-L.; Lee, E.Y.P. Assessment of Cervical Cancer with a Parameter-Free Intravoxel Incoherent Motion Imaging Algorithm. Korean J. Radiol. 2017, 18, 510. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| TR/TE (ms) | FOV (mm) | NEX | Matrix Size | Slice Thickness (mm) | Intersection Gap (mm) | B-Values (s/mm2) | |
|---|---|---|---|---|---|---|---|
| Sagittal FSE T2WI | 4000/125 | 320 × 320 | 2 | 320 × 224 | 4 | 1 | / |
| Para-axial, para-coronal FSE T2WI | 5000/125 | 240 × 240 | 2 | 320 × 224 | 4 | 1 | / |
| Para-axial FSE T1WI (w/wo FS) | 400/10 | 240 × 240 | 2 | 320 × 244 | 4 | 1 | / |
| Axial FSE T2WI | 5000/125 | 310 × 310 | 2 | 320 × 244 | 4 | 1 | / |
| Axial DWI | 2000/57 | 240 × 240 | 2 | 160 × 80 | 3.5 | 0 | 0, 1000 |
| Para-axial SE-EPI DWI (IVIM) | 2000/77 | 300 × 300 | 2 | 160 × 192 | 6 | 1 | 0, 30, 50, 150, 500, 800, 1000, 1500 |
| Total Population (n = 20) | GR Group (n = 11) | PR/NR Group (n = 9) | |
|---|---|---|---|
| Age (years) * | 54 (±13) | 55 (±15) | 53 (±10) |
| FIGO stage | |||
| 4 (20.0%) | 3 (27.3%) | 1 (11.1%) |
| 11 (55.0%) | 8 (72.7%) | 3 (33.3%) |
| 2 (10.0%) | 0 (0.0%) | 2 (22.2%) |
| 3 (15.0%) | 0 (0.0%) | 3 (33.3%) |
| Histotype | |||
| 17 (85.0%) | 10 (90.9%) | 7 (77.8%) |
| 3 (15.0%) | 1 (9.1%) | 2 (22.2%) |
| Grading | |||
| 1 (5.0%) | 0 (0%) | 1 (11.1%) |
| 10 (50.0%) | 5 (45.5%) | 5 (55.6%) |
| 9 (45.0%) | 6 (54.5%) | 3 (33.3%) |
| LVI | |||
| 7 (35.0%) | 5 (45.5%) | 2 (22.2%) |
| 13 (65.0%) | 6 (54.5%) | 7 (77.8%) |
| TILs | |||
| 9 (45.0%) | 7 (63.6%) | 2 (22.2%) |
| 11 (55.0%) | 4 (36.4%) | 7 (77.8%) |
| IVIM | ADC (×10−6 mm2/s) | |||
|---|---|---|---|---|
| D (×1−3 mm2/s) | D* (×10−3 mm2/s) | fp (%) | ||
| Histotype | ||||
| 1.23 (±0.14) | 27.22 (±3.21) | 15.61 (±1.12) | 937.56 (±114.19) |
| 1.00 (±0.21) | 25.88 (±9.27) | 11.05 (±1.02) | 1333.25 (±935.84) |
| p value | 0.184 | 0.794 | 0.006 | 0.460 |
| Grading | ||||
| 1.17 (±0.19) | 26.59 (±5.11) | 14.79 (±1.95) | 887.89 (±105.75) |
| 1.25 (±0.16) | 27.39 (±4.54) | 15.09 (±2.14) | 1135.65 (±581.80) |
| p value | 0.364 | 0.715 | 0.759 | 0.220 |
| LVI | ||||
| 1.29 (±0.20) | 28.62 (±3.79) | 15.73 (±0.73) | 968.86 (±192.14) |
| 1.15 (±0.14) | 26.05 (±5.11) | 14.49 (±2.33) | 1043.54 (±514.72) |
| p value | 0.147 | 0.222 | 0.095 | 0.638 |
| TILs | ||||
| 1.28 (±0.11) | 27.63 (±4.53) | 15.34 (±1.69) | 1154.44 (±613.61) |
| 1.10 (±0.18) | 26.59 (±5.32) | 14.46 (±2.39) | 908.70 (±106.67) |
| p value | 0.018 | 0.652 | 0.375 | 0.268 |
| Response to NACT | ||||
| 1.30 (±0.06) | 27.19 (±2.12) | 15.73 (±0.30) | 1098.64 (±116.45) |
| 1.13 (±0.12) | 26.66 (±6.82) | 14.35 (±2.88) | 923.43 (±104.25) |
| p value | 0.001 | 0.813 | 0.055 | 0.316 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dolciami, M.; Capuani, S.; Celli, V.; Maiuro, A.; Pernazza, A.; Palaia, I.; Di Donato, V.; Santangelo, G.; Rizzo, S.M.R.; Ricci, P.; et al. Intravoxel Incoherent Motion (IVIM) MR Quantification in Locally Advanced Cervical Cancer (LACC): Preliminary Study on Assessment of Tumor Aggressiveness and Response to Neoadjuvant Chemotherapy. J. Pers. Med. 2022, 12, 638. https://doi.org/10.3390/jpm12040638
Dolciami M, Capuani S, Celli V, Maiuro A, Pernazza A, Palaia I, Di Donato V, Santangelo G, Rizzo SMR, Ricci P, et al. Intravoxel Incoherent Motion (IVIM) MR Quantification in Locally Advanced Cervical Cancer (LACC): Preliminary Study on Assessment of Tumor Aggressiveness and Response to Neoadjuvant Chemotherapy. Journal of Personalized Medicine. 2022; 12(4):638. https://doi.org/10.3390/jpm12040638
Chicago/Turabian StyleDolciami, Miriam, Silvia Capuani, Veronica Celli, Alessandra Maiuro, Angelina Pernazza, Innocenza Palaia, Violante Di Donato, Giusi Santangelo, Stefania Maria Rita Rizzo, Paolo Ricci, and et al. 2022. "Intravoxel Incoherent Motion (IVIM) MR Quantification in Locally Advanced Cervical Cancer (LACC): Preliminary Study on Assessment of Tumor Aggressiveness and Response to Neoadjuvant Chemotherapy" Journal of Personalized Medicine 12, no. 4: 638. https://doi.org/10.3390/jpm12040638