
Aortic Risks Prediction Models after Cardiac Surgeries Using Integrated Data


Abstract
:1. Introduction
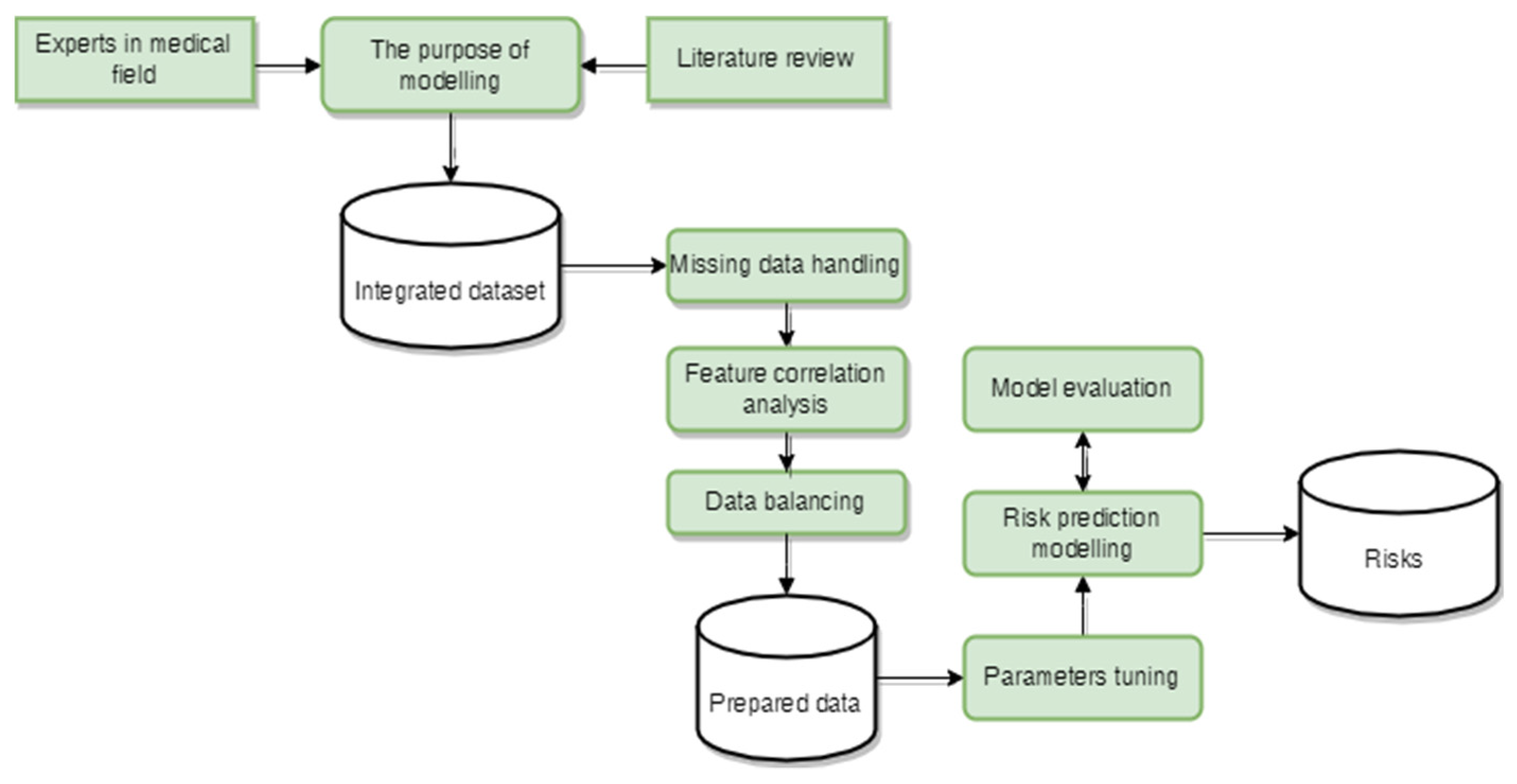
2. Materials and Methods
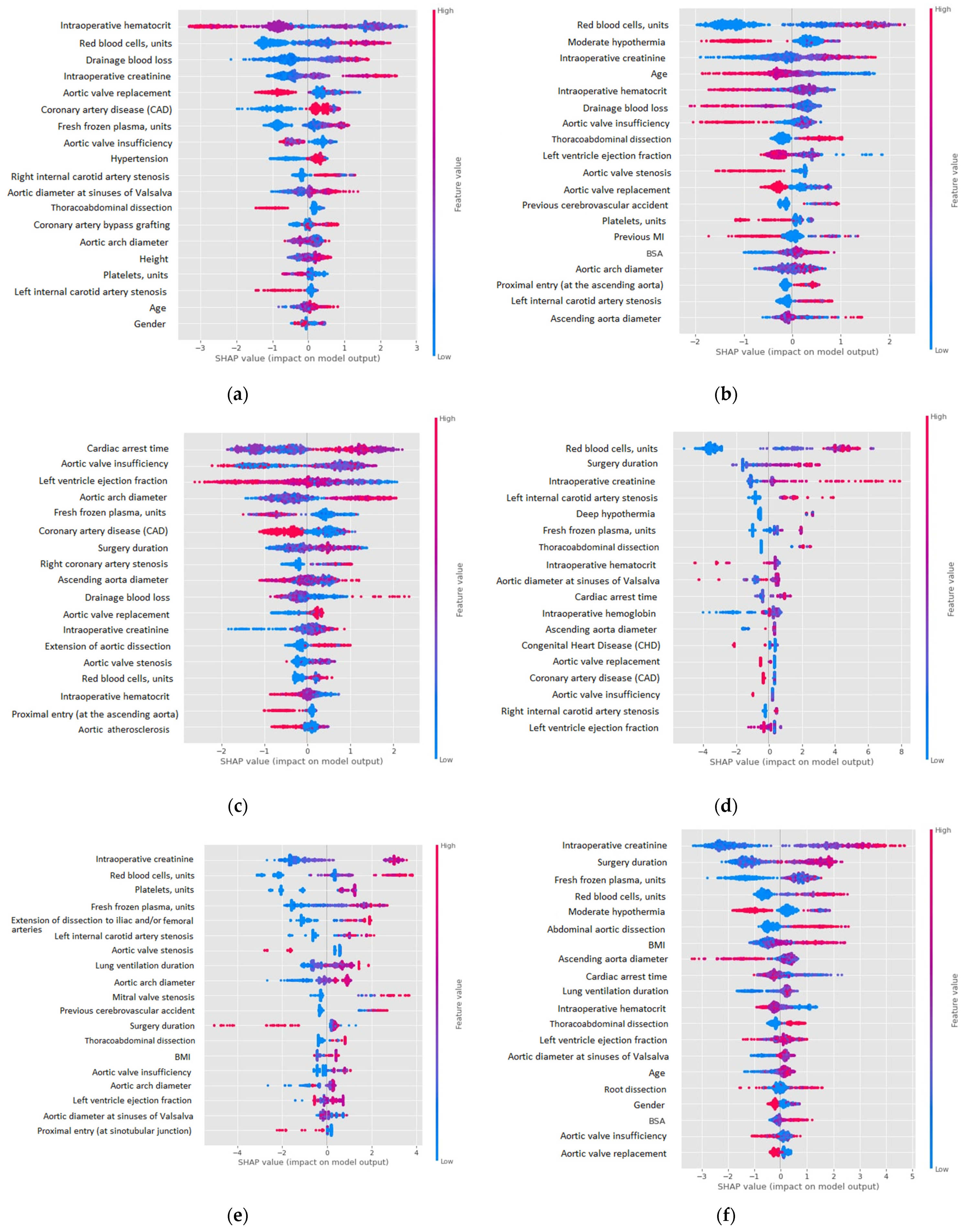
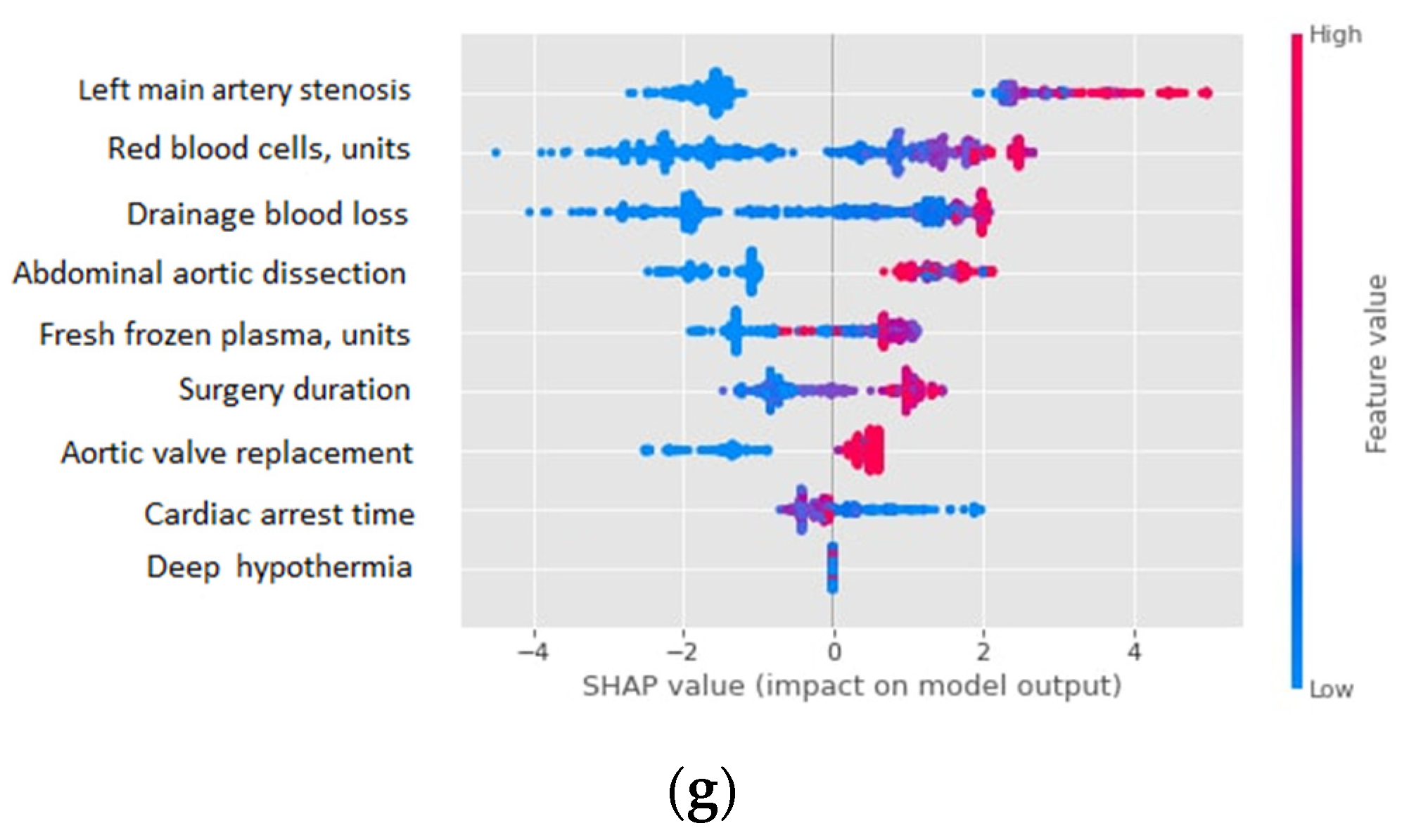
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- In-hospital mortality;
- Temporary neurological deficit (TND);
- Permanent neurological deficit (PND);
- Prolonged lung ventilation (LV) (>7 days);
- Renal replacement therapy (RRT);
- Myocardial infarction (MI);
- Multiple organ failure (MOF).
- Gender;
- Age;
- Height;
- Weight;
- Body mass index (BMI);
- Body surface area (BSA).
- Congenital heart disease (CHD);
- Hypertension;
- Coronary artery disease (CAD);
- Previous MI;
- Previous cerebrovascular accident;
- Chronic obstructive pulmonary disease (COPD);
- Marfan syndrome;
- Aortic atherosclerosis.
- Preoperative hematocrit;
- Preoperative urea;
- Preoperative creatinine;
- Preoperative glomerular filtration rate (GFR).
- Left main artery stenosis (LMA);
- Right coronary artery stenosis (RCA);
- Obtuse margin artery stenosis (OMA);
- Left anterior descending artery (LAD).
- Left internal carotid artery stenosis;
- Right internal carotid artery stenosis;
- Left ventricle ejection fraction;
- Aortic valve stenosis;
- Aortic valve insufficiency;
- Mitral valve stenosis;
- Mitral valve insufficiency;
- Aortic diameter at sinuses of Valsalva.
- Ascending aorta diameter;
- Aortic arch diameter;
- Segment A diameter = proximal descending aortic diameter;
- Segment B diameter = distal descending aortic diameter;
- Segment C diameter = abdominal aortic diameter;
- Proximal entry (at sinotubular junction);
- Proximal entry (at the ascending aorta);
- Proximal entry (at the aortic arch);
- Proximal entry behind the left subclavian artery = type B aortic dissection;
- Involvement aortic root in dissection;
- Involvement ascending aortic in dissection;
- Involvement aortic arch in dissection;
- Thoracoabdominal dissection;
- Abdominal aortic dissection;
- Extension of aortic dissection down to iliac and/or femoral arteries.
- Cardiac arrest time;
- Antegrade cerebral perfusion time;
- Circulatory arrest time;
- Deep hypothermia;
- Moderate hypothermia;
- Re-sternotomy for bleeding;
- Surgery duration;
- Red blood cells, units;
- Fresh frozen plasma, units;
- Platelets, units;
- Drainage blood loss;
- Intraoperative hematocrit.
- Intraoperative creatinine.
- Coronary artery bypass grafting;
- Aortic valve replacement;
- Mitral valve replacement.
References
- Saeyeldin, A.A.; Velasquez, C.A.; Mahmood, S.U.B.; Brownstein, A.J.; Zafar, M.A.; Ziganshin, B.A.; Elefteriades, J.A. Thoracic aortic aneurysm: Unlocking the “silent killer” secrets. Gen. Thorac. Cardiovasc. Surg. 2019, 67, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Orandi, B.J.; Dimick, J.B.; Deeb, G.M.; Patel, H.J.; Upchurch, G.R. A population-based analysis of endovascular versus open thoracic aortic aneurysm repair. J. Vasc. Surg. 2009, 49, 1112–1116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Czerny, M.; Siepe, M.; Beyersdorf, F.; Feisst, M.; Gabel, M.; Pilz, M.; Pöling, J.; Dohle, D.S.; Sarvanakis, K.; Luehr, M.; et al. Prediction of mortality rate in acute type A dissection: The German Registry for Acute Type A Aortic Dissection score. Eur. J. Cardiothorac. Surg. 2020, 58, 700–706. [Google Scholar] [CrossRef] [PubMed]
- Wagner, M.A.; Wang, H.; Benrashid, E.; Keenan, J.E.; Ganapathi, A.M.; Englum, B.R.; Hughes, G.C. Risk Prediction Model for Major Adverse Outcome in Proximal Thoracic Aortic Surgery. Ann. Thorac. Surg. 2019, 107, 795–801. [Google Scholar] [CrossRef] [PubMed]
- Weng, S.F.; Reps, J.; Kai, J.; Garibaldi, J.M.; Qureshi, N. Can Machine-learning improve cardiovascular risk prediction using routine clinical data? PLoS ONE 2017, 12, e0174944. [Google Scholar] [CrossRef] [Green Version]
- Lareyre, F.; Adam, C.; Carrier, M.; Raffort, J. Prediction of Abdominal Aortic Aneurysm Growth and Risk of Rupture in the Era of Machine Learning. Angiology 2020, 71, 767. [Google Scholar] [CrossRef] [Green Version]
- Hirata, K.; Nakaura, T.; Nakagawa, M.; Kidoh, M.; Oda, S.; Utsunomiya, D.; Yamashita, Y. Machine Learning to Predict the Rapid Growth of Small Abdominal Aortic Aneurysm. J. Comput. Assist. Tomogr. 2020, 44, 37–42. [Google Scholar] [CrossRef]
- Lee, R.; Jarchi, D.; Perera, R.; Jones, A.; Cassimjee, I.; Handa, A.; Clifton, D.A.; Bellamkonda, K.; Woodgate, F.; Killough, N.; et al. Applied Machine Learning for the Prediction of Growth of Abdominal Aortic Aneurysm in Humans. EJVES Short Rep. 2018, 39, 24–28. [Google Scholar] [CrossRef]
- Estrera, A.L.; Miller, C.C.; Lee, T.Y.; Shah, P.; Safi, H.J. Ascending and transverse aortic arch repair: The impact of retrograde cerebral perfusion. Circulation 2008, 118, S160–S166. [Google Scholar] [CrossRef] [Green Version]
- Ghincea, C.V.; Reece, T.B.; Eldeiry, M.; Roda, G.F.; Bronsert, M.R.; Jarrett, M.J.; Pal, J.D.; Cleveland, J.C.; Fullerton, D.A.; Aftab, M. Predictors of Acute Kidney Injury Following Aortic Arch Surgery. J. Surg. Res. 2019, 242, 40–46. [Google Scholar] [CrossRef]
- Wang, X.; Yang, F.; Zhu, J.; Liu, Y.; Sun, L.; Hou, X. Aortic arch surgery with hypothermic circulatory arrest and unilateral antegrade cerebral perfusion: Perioperative outcomes. J. Thorac. Cardiovasc. Surg. 2020, 159, 374–387.e4. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Yoon, H.; Nam, K.; Cho, Y.; Kim, T.; Kim, W.; Bahk, J. Derivation and Validation of Machine Learning Approaches to Predict Acute Kidney Injury after Cardiac Surgery. J. Clin. Med. 2018, 7, 322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhong, Z.; Yuan, X.; Liu, S.; Yang, Y.; Liu, F.F. Machine learning prediction models for prognosis of critically ill patients after open-heart surgery. Sci. Rep. 2021, 11, 3384. [Google Scholar] [CrossRef] [PubMed]
- Allyn, J.; Allou, N.; Augustin, P.; Philip, I.; Martinet, O.; Belghiti, M.; Provenchere, S.; Montravers, P.; Ferdynus, C. A comparison of a machine learning model with EuroSCORE II in predicting mortality after elective cardiac surgery: A decision curve analysis. PLoS ONE 2017, 12, e169772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandes, M.P.B.; Armengol de la Hoz, M.; Rangasamy, V.; Subramaniam, B. Machine Learning Models with Preoperative Risk Factors and Intraoperative Hypotension Parameters Predict Mortality After Cardiac Surgery. J. Cardiothorac. Vasc. Anesth. 2021, 35, 857–865. [Google Scholar] [CrossRef] [PubMed]
- Coulson, T.; Bailey, M.; Pilcher, D.; Reid, C.M.; Seevanayagam, S.; Williams-Spence, J.; Bellomo, R. Predicting Acute Kidney Injury After Cardiac Surgery Using a Simpler Model. J. Cardiothorac. Vasc. Anesth. 2021, 35, 866–873. [Google Scholar] [CrossRef]
- Hanley, J.A.; McNeil, B.J. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology 1982, 143, 29–36. [Google Scholar] [CrossRef] [Green Version]
- Pedregosa Fabianpedregosa, F.; Michel, V.; Grisel Oliviergrisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Vanderplas, J.; Cournapeau, D.; Pedregosa, F.; Varoquaux, G.; et al. Scikit-learn: Machine Learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- Prokhorenkova, L.; Gusev, G.; Vorobev, A.; Dorogush, A.V.; Gulin, A. CatBoost: Unbiased boosting with categorical features. In Proceedings of the NIPS’18: Proceedings of the 32nd International Conference on Neural Information Processing Systems, Montréal, QC, Canada, 3–8 December 2018; pp. 6639–6649. [Google Scholar] [CrossRef]
- Waskom, M.L. seaborn: Statistical data visualization. J. Open Source Softw. 2021, 6, 3021. [Google Scholar] [CrossRef]
- Hunter, J.D. Matplotlib: A 2D graphics environment. Comput. Sci. Eng. 2007, 9, 90–95. [Google Scholar] [CrossRef]
- Chawla, N.V.; Bowyer, K.W.; Hall, L.O.; Kegelmeyer, W.P. SMOTE: Synthetic minority over-sampling technique. J. Artif. Intell. Res. 2002, 16, 321–357. [Google Scholar] [CrossRef]
- Lundberg, S.M.; Lee, S.-I. A Unified Approach to Interpreting Model Predictions. In Proceedings of the NIPS’17: Proceedings of the 31st International Conference on Neural Information Processing Systems, Long Beach, CA, USA, 4–9 December 2017; pp. 4768–4777. [Google Scholar] [CrossRef]
- Kartal, E.; Balaban, M.E. Machine learning techniques in cardiac risk assessment. Turkish J. Thorac. Cardiovasc. Surg. 2018, 26, 394. [Google Scholar] [CrossRef] [PubMed]
- Lenivtceva, I.; Grechishcheva, S.; Kopanitsa, G.; Panfilov, D.; Kozlov, B. Predicting the Aortic Aneurysm Postoperative Risks Based on Russian Integrated Data. Stud. Health Technol. Inform. 2021, 285, 88–93. [Google Scholar] [CrossRef] [PubMed]
- Cabitza, F.; Campagner, A. Who wants accurate models? Arguing for a different metrics to take classification models seriously. arXiv 2019, arXiv:1910.09246. [Google Scholar] [CrossRef]
- Hicks, S.A.; Strümke, I.; Strümke, S.; Thambawita, V.; Hammou, M.; Riegler, M.A.; Al Halvorsen, P.; Parasa, S. On evaluation metrics for medical applications of artificial intelligence. medRxiv 2021, 12, 5979. [Google Scholar] [CrossRef]
- Kim, W.H.; Park, M.H.; Kim, H.J.; Lim, H.Y.; Shim, H.S.; Sohn, J.T.; Kim, C.S.; Lee, S.M. Potentially modifiable risk factors for acute kidney injury after surgery on the thoracic aorta: A propensity score matched case-control study. Medicine 2015, 94, e273. [Google Scholar] [CrossRef]
- Zhou, H.; Wang, G.; Yang, L.; Shi, S.; Li, J.; Wang, M.; Zhang, C.; Li, H.; Qian, X.; Sun, X.; et al. Acute Kidney Injury After Total Arch Replacement Combined With Frozen Elephant Trunk Implantation: Incidence, Risk Factors, and Outcome. J. Cardiothorac. Vasc. Anesth. 2018, 32, 2210–2217. [Google Scholar] [CrossRef]
- Nota, H.; Asai, T.; Suzuki, T.; Kinoshita, T.; Ikegami, H.; Takashima, N. Risk factors for acute kidney injury in aortic arch surgery with selective cerebral perfusion and mild hypothermic lower body circulatory arrest. Interact. Cardiovasc. Thorac. Surg. 2014, 19, 955–961. [Google Scholar] [CrossRef] [Green Version]
- Codner, J.A.; Lou, X.; Duwayri, Y.M.; Chen, E.P.; Binongo, J.N.; Moon, R.; Jordan, W.D.; Leshnower, B.G. The distance of the primary intimal tear from the left subclavian artery predicts aortic growth in uncomplicated type B aortic dissection. J. Vasc. Surg. 2019, 69, 692–700. [Google Scholar] [CrossRef]
- Hoogmoed, R.C.; Patel, H.J.; Kim, K.M.; Williams, D.M.; Deeb, G.M.; Yang, B. Acute Kidney Injury in Acute Type B Aortic Dissection: Outcomes Over 20 Years. Ann. Thorac. Surg. 2019, 107, 486–492. [Google Scholar] [CrossRef] [Green Version]
- Heo, W.; Song, S.W.; Lee, S.Y.; Kim, T.H.; Lee, J.S.; Yoo, K.J.; Cho, B.K. Locational impact of luminal communication on aortic diameter changes and reintervention in acute type I aortic dissection. Eur. J. Cardiothorac. Surg. 2019, 55, 1037–1044. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Scheme | Algorithm | AUC-ROC | Data | Target |
|---|---|---|---|---|
| Lee, 2018 [12] | XGBoost | 0.78 | Open heart and TAA surgery | Acute kidney injury |
| Zhong, 2021 [13] | XGBoost | 0.93 | Coronary artery bypass surgery, aortic valve replacement and other heart surgeries | 30-day mortality, septic shock, liver dysfunction, and thrombocytopenia |
| Allyn, 2017 [14] | Model ensemble | 0.78 | Elective heart surgery | Postoperative mortality |
| Fernandes, 2021 [15] | XGBoost | 0.88 | Intraoperative open heart surgery data | Postoperative mortality |
| Coulson, 2020 [16] | Logistic regression | 0.78–0.85 | Open heart surgery | Acute kidney injury |
| Model | Parameters |
|---|---|
| LR* (imp. feat.) | ‘C’: 2.83, ‘solver’: ‘newton-cg’ |
| LR + SMOTE (imp. feat.) | ‘C’: 0.5, ‘solver’: ‘newton-cg’ |
| LR + SMOTE (all feat.) | ‘C’: 4.0, ‘solver’: ‘liblinear’ |
| RF (imp. feat.) | ‘criterion’: ‘gini’, ‘max_features’: ‘auto’ |
| RF + SMOTE (imp. feat.) | ‘criterion’: ‘gini’, ‘max_features’: ‘auto’ |
| RF + SMOTE (all feat.) | ‘criterion’: ‘gini’, ‘max_features’: ‘log2’ |
| CC * (all. feat.) | ‘depth’: 4, ‘l2_leaf_reg’: 3, ‘learning_rate’: 0.6 |
| CC + SMOTE (imp. feat.) | ‘depth’: 5, ‘l2_leaf_reg’: 2, ‘learning_rate’: 0.9 |
| CC + SMOTE (all feat.) | ‘depth’: 4, ‘l2_leaf_reg’: 1, ‘learning_rate’: 0.2 |
| Target | Best Classifier | ROC AUC | F-Score | Recall | Precision |
|---|---|---|---|---|---|
| In-hospital mortality | CC * + SMOTE (all feat.) | 0.965 | 0.966 | 0.992 | 0.942 |
| Temporary neurological deficit (TND) | CC + SMOTE (all feat.) | 0.960 | 0.959 | 0.936 | 0.983 |
| Permanent neurological deficit (PND) | CC + SMOTE (all feat.) | 0.946 | 0.947 | 0.969 | 0.926 |
| Prolonged lung ventilation (>7 days) | CC + SMOTE (all feat.) | 0.957 | 0.958 | 0.984 | 0.934 |
| Renal replacement therapy (RRT) | CC + SMOTE (all feat.) | 0.985 | 0.984 | 0.992 | 0.978 |
| Myocardial infarction (MI) | CC + SMOTE (imp. feat.) | 0.986 | 0.984 | 0.993 | 0.979 |
| Multiple organ failure (MOF) | CC + SMOTE (all feat.) | 0.952 | 0.950 | 0.964 | 0.958 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lenivtceva, I.; Panfilov, D.; Kopanitsa, G.; Kozlov, B. Aortic Risks Prediction Models after Cardiac Surgeries Using Integrated Data. J. Pers. Med. 2022, 12, 637. https://doi.org/10.3390/jpm12040637
Lenivtceva I, Panfilov D, Kopanitsa G, Kozlov B. Aortic Risks Prediction Models after Cardiac Surgeries Using Integrated Data. Journal of Personalized Medicine. 2022; 12(4):637. https://doi.org/10.3390/jpm12040637
Chicago/Turabian StyleLenivtceva, Iuliia, Dmitri Panfilov, Georgy Kopanitsa, and Boris Kozlov. 2022. "Aortic Risks Prediction Models after Cardiac Surgeries Using Integrated Data" Journal of Personalized Medicine 12, no. 4: 637. https://doi.org/10.3390/jpm12040637