
Association between Glasgow Coma Scale in Early Carbon Monoxide Poisoning and Development of Delayed Neurological Sequelae: A Meta-Analysis

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Reporting Guidelines and Protocol Registration
2.2. Search Strategy
2.3. Study Selection
2.4. Data Extraction
2.5. Risk of Bias Individual Studies
2.6. Statistical Analysis
3. Results
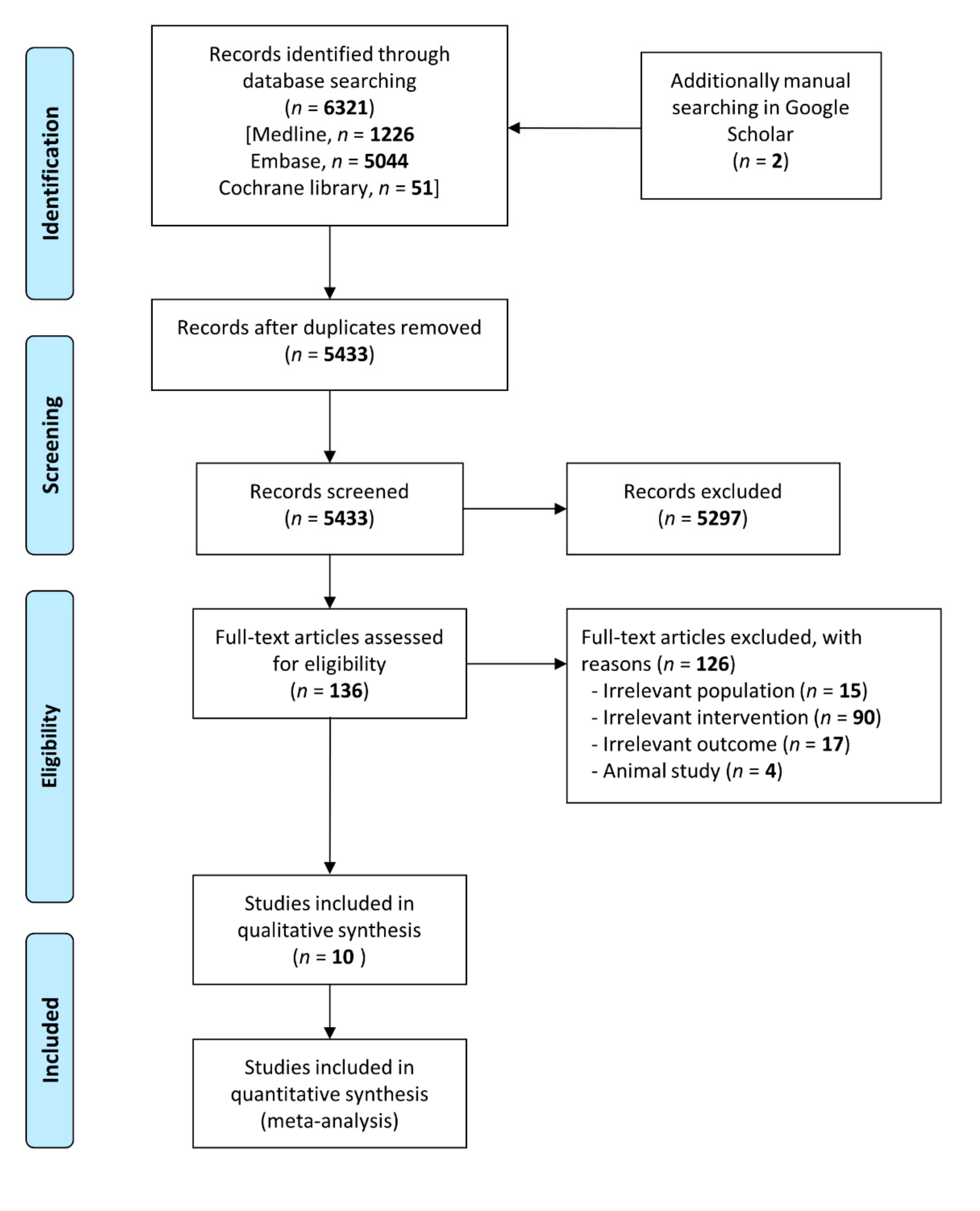
3.1. Study Selection
3.2. Study Characteristics
3.3. Risk of Bias and Quality Assessment
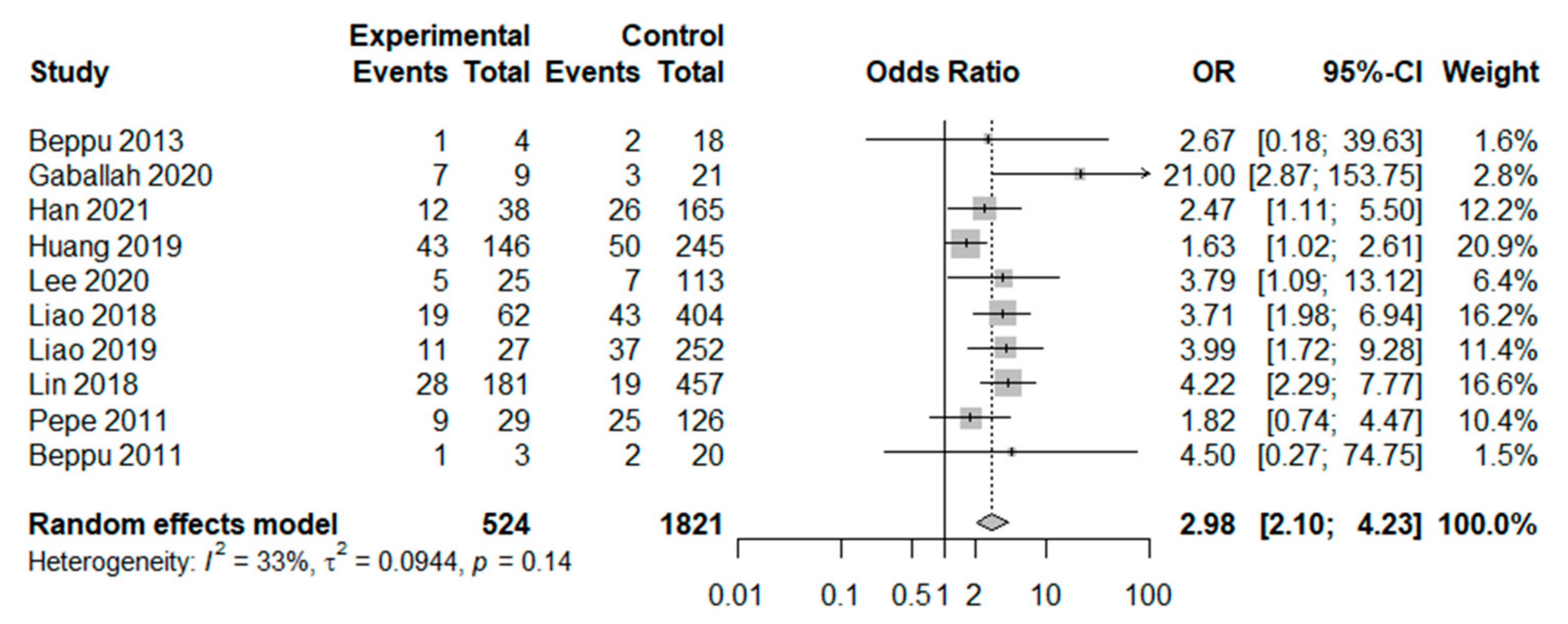
3.4. Main Analysis and Subgroup Analysis
3.5. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Liao, S.C.; Mao, Y.C.; Yang, K.J.; Wang, K.C.; Wu, L.Y.; Yang, C.C. Targeting optimal time for hyperbaric oxygen therapy following carbon monoxide poisoning for prevention of delayed neuropsychiatric sequelae: A retrospective study. J. Neurol. Sci. 2019, 396, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Sircar, K.; Clower, J.; Shin, M.K.; Bailey, C.; King, M.; Yip, F. Carbon monoxide poisoning deaths in the United States, 1999 to 2012. Am. J. Emerg. Med. 2015, 33, 1140–1145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mattiuzzi, C.; Lippi, G. Worldwide epidemiology of carbon monoxide poisoning. Hum. Exp. Toxicol. 2020, 39, 387–392. [Google Scholar] [CrossRef] [PubMed]
- Sekiya, K.; Nishihara, T.; Abe, N.; Konishi, A.; Nandate, H.; Hamada, T.; Ikemune, K.; Takasaki, Y.; Tanaka, J.; Asano, M.; et al. Carbon monoxide poisoning-induced delayed encephalopathy accompanies decreased microglial cell numbers: Distinctive pathophysiological features from hypoxemia-induced brain damage. Brain Res. 2019, 1710, 22–32. [Google Scholar] [CrossRef]
- Weaver, L.K. Carbon monoxide poisoning. Undersea Hyperb. Med. 2020, 47, 151–169. [Google Scholar] [CrossRef]
- Lin, C.H.; Su, W.H.; Chen, Y.C.; Feng, P.H.; Shen, W.C.; Ong, J.R.; Wu, M.Y.; Wong, C.S. Treatment with normobaric or hyperbaric oxygen and its effect on neuropsychometric dysfunction after carbon monoxide poisoning: A systematic review and meta-analysis of randomized controlled trials. Medicine 2018, 97, e12456. [Google Scholar] [CrossRef]
- Zhang, Y.; Wang, T.; Lei, J.; Guo, S.; Wang, S.; Gu, Y.; Dou, Y.; Zhuang, X. Cerebral Damage after Carbon Monoxide Poisoning: A Longitudinal Diffusional Kurtosis Imaging Study. AJNR Am. J. Neuroradiol. 2019, 40, 1630–1637. [Google Scholar] [CrossRef]
- Chambers, C.A.; Hopkins, R.O.; Weaver, L.K.; Key, C. Cognitive and affective outcomes of more severe compared to less severe carbon monoxide poisoning. Brain Inj. 2008, 22, 387–395. [Google Scholar] [CrossRef]
- Han, S.; Choi, S.; Nah, S.; Lee, S.U.; Cho, Y.S.; Kim, G.W.; Lee, Y.H. Cox regression model of prognostic factors for delayed neuropsychiatric sequelae in patients with acute. carbon monoxide poisoning: A prospective observational study. Neurotoxicology 2021, 82, 63–68. [Google Scholar] [CrossRef]
- Rose, J.J.; Wang, L.; Xu, Q.; McTiernan, C.F.; Shiva, S.; Tejero, J.; Gladwin, M.T. Carbon Monoxide Poisoning: Pathogenesis, Management, and Future Directions of Therapy. Am. J. Respir. Crit. Care Med. 2017, 195, 596–606. [Google Scholar] [CrossRef]
- Choi, I.S. Delayed neurologic sequelae in carbon monoxide intoxication. Arch. Neurol. 1983, 40, 433–435. [Google Scholar] [CrossRef]
- Bleecker, M.L. Carbon monoxide intoxication. Handb. Clin. Neurol. 2015, 131, 191–203. [Google Scholar] [CrossRef]
- Chan, M.Y.; Au, T.T.; Leung, K.S.; Yan, W.W. Acute carbon monoxide poisoning in a regional hospital in Hong Kong: Historical cohort study. Hong Kong Med. J. 2016, 22, 46–55. [Google Scholar] [CrossRef]
- Hafez, A.S.; El-Sarnagawy, G.N. S-100beta in predicting the need of hyperbaric oxygen in CO-induced delayed neurological sequels. Hum. Exp. Toxicol. 2020, 39, 614–623. [Google Scholar] [CrossRef]
- Park, E.; Ahn, J.; Min, Y.G.; Jung, Y.S.; Kim, K.; Lee, J.; Choi, S.C. The usefulness of the serum s100b protein for predicting delayed neurological sequelae in acute carbon monoxide poisoning. Clin. Toxicol. 2012, 50, 183–188. [Google Scholar] [CrossRef]
- Kudo, K.; Otsuka, K.; Yagi, J.; Sanjo, K.; Koizumi, N.; Koeda, A.; Umetsu, M.Y.; Yoshioka, Y.; Mizugai, A.; Shiga, Y.; et al. Predictors for delayed encephalopathy following acute carbon monoxide poisoning. BMC Emerg. Med. 2014, 14, 3. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.; Kang, H.; Ko, B.S.; Oh, J.; Lim, T.H.; Cho, Y. Initial creatine kinase level as predictor for delayed neuropsychiatric sequelae associated with acute carbon monoxide poisoning. Am. J. Emerg. Med. 2021, 43, 195–199. [Google Scholar] [CrossRef]
- Kitamoto, T.; Tsuda, M.; Kate, M.; Saito, F.; Kamijo, Y.; Kinoshita, T. Risk factors for the delayed onset of neuropsychologic sequelae following carbon monoxide poisoning. Acute Med. Surg. 2016, 3, 315–319. [Google Scholar] [CrossRef]
- Gaballah, S.Z.; Elkhishin, I.A.R.; Hashim, N.A.; Hamid, O.I.A. Predictors of Delayed Neurological Sequelae after Acute Carbon Monoxide Poisoning at Zagazig University Hospitals. Zagazig J. Forensic Med. 2020, 18, 105–121. [Google Scholar] [CrossRef]
- Cha, Y.S.; Kim, H.; Do, H.H.; Kim, H.I.; Kim, O.H.; Cha, K.C.; Le, K.H.; Hwang, S.O. Serum neuron-specific enolase as an early predictor of delayed neuropsychiatric sequelae in patients with acute carbon monoxide poisoning. Hum. Exp. Toxicol. 2018, 37, 240–246. [Google Scholar] [CrossRef]
- Jeon, S.B.; Sohn, C.H.; Seo, D.W.; Oh, B.J.; Lim, K.S.; Kang, D.W.; Kim, W.Y. Acute Brain Lesions on Magnetic Resonance Imaging and Delayed Neurological Sequelae in Carbon Monoxide Poisoning. JAMA Neurol. 2018, 75, 436–443. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.S.; Cha, Y.S.; Kim, M.S.; Kim, H.J.; Lee, Y.S.; Youk, H.; Kim, H.I.; Kim, O.H.; Cha, K.C.; Kim, H.; et al. The usefulness of diffusion-weighted magnetic resonance imaging performed in the acute phase as an early predictor of delayed neuropsychiatric sequelae in acute carbon monoxide poisoning. Hum. Exp. Toxicol. 2018, 37, 587–595. [Google Scholar] [CrossRef] [PubMed]
- Nah, S.; Choi, S.; Kim, H.B.; Lee, J.; Lee, S.U.; Lee, Y.H.; Kim, K.W.; Han, S. Cerebral White Matter Lesions on Diffusion-Weighted Images and Delayed Neurological Sequelae after Carbon Monoxide Poisoning: A Prospective Observational Study. Diagnostics 2020, 10, 698. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.S.; Lin, C.C.; Yang, C.C.; Weng, S.C.; Wang, S.M.; Chen, C.Y.; Huang, N.; Chou, Y.H. Myocardial injury was associated with neurological sequelae of acute carbon monoxide poisoning in Taiwan. J. Chin. Med. Assoc. 2018, 81, 682–690. [Google Scholar] [CrossRef]
- Pepe, G.; Castelli, M.; Nazerian, P.; Vanni, S.; Panta, M.D.; Gambassi, F.; Botti, P.; Missanelli, A.; Grifoni, S. Delayed neuropsychological sequelae after carbon monoxide poisoning: Predictive risk factors in the Emergency Department. A retrospective study. Scand. J. Trauma Resusc. Emerg. Med. 2011, 19, 16. [Google Scholar] [CrossRef] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Murlow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef]
- Hayden, J.A.; Van der Windt, D.A.; Cartwright, J.L.; Côté, P.; Bombardier, C. Assessing bias in studies of prognostic factors. Ann. Intern Med. 2013, 158, 280–286. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Liao, S.C.; Mao, Y.C.; Hung, Y.M.; Lee, C.H.; Yang, C.C. Predictive Role of QTc Prolongation in Carbon Monoxide Poisoning-Related Delayed Neuropsychiatric Sequelae. Biomed. Res. Int. 2018, 2018, 2543018. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.C.; Lee, J.C.; Lin, K.C.; Lin, H.J.; Su, S.B.; Hsu, C.C.; Guo, H.R. Exposure Duration and History of Hypertension Predicted Neurological Sequelae in Patients with Carbon Monoxide Poisoning. Epidemiology 2019, 30, S76–S81. [Google Scholar] [CrossRef]
- Beppu, T.; Nishimoto, H.; Fujiwara, S.; Kudo, K.; Sanjo, K.; Narumi, S.; Oikawa, H.; Onodera, M.; Ogasawara, K.; Sasaki, M. 1H-magnetic resonance spectroscopy indicates damage to cerebral white matter in the subacute phase after CO poisoning. J. Neurol. Neurosurg. Psychiatry 2011, 82, 869–875. [Google Scholar] [CrossRef]
- Beppu, T.; Fujiwara, S.; Nishimoto, H.; Koeda, A.; Narumi, S.; Mori, K.; Ogasawara, K.; Sasaki, M. Fractional anisotropy in the centrum semiovale as a quantitative indicator of cerebral white matter damage in the subacute phase in patients with carbon monoxide poisoning: Correlation with the concentration of myelin basic protein in cerebrospinal fluid. J. Neurol. 2012, 259, 1698–1705. [Google Scholar] [CrossRef] [Green Version]
- Zou, J.F.; Guo, Q.; Shao, H.; Li, B.; Du, Y.; Liu, M.; Liu, F.; Dai, L.; Lin, H.J.; Su, S.B.; et al. Lack of pupil reflex and loss of consciousness predict 30-day neurological sequelae in patients with carbon monoxide poisoning. PLoS ONE 2015, 10, e0119126. [Google Scholar] [CrossRef]
- Pang, L.; Wang, H.L.; Wang, Z.H.; Wu, Y.; Dong, N.; Xu, D.H.; Wang, D.W.; Xu, H.; Zhang, N. Plasma copeptin as a predictor of intoxication severity and delayed neurological sequelae in acute carbon monoxide poisoning. Peptides 2014, 59, 89–93. [Google Scholar] [CrossRef]
- Sönmez, F.T.; Güneş, H.; Saritaş, A.; Kandiş, H. Carbon Monoxide Poisoning: Clinical Manifestations, Consequences, Monitoring, Diagnosis and Treatment of Toxicity. Konuralp Med. J. 2015, 7, 192–198. [Google Scholar]
- Thom, S.R. Dehydrogenase conversion to oxidase and lipid peroxidation in brain after carbon monoxide poisoning. J. Appl. Physiol. 1992, 73, 1584–1589. [Google Scholar] [CrossRef]
- Thom, S.R. Leukocytes in carbon monoxide-mediated brain oxidative injury. Toxicol. Appl. Pharmacol. 1993, 123, 234–247. [Google Scholar] [CrossRef]
- Du, X.; Gu, H.; Hao, F.; Gao, L.; Wang, J.; Sun, C.; Zhang, H.; Ma, P.; Zhang, X.; Hu, W. Utility of brain CT for predicting delayed encephalopathy after acute carbon monoxide poisoning. Exp. Ther. Med. 2019, 17, 2682–2688. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.H.; Chang, K.H.; Song, I.C.; Kim, K.H.; Kwon, B.J.; Kim, H.C.; Kim, J.H.; Han, M.H. Delayed encephalopathy of acute carbon monoxide intoxication: Diffusivity of cerebral white matter lesions. AJNR Am. J. Neuroradiol. 2003, 24, 1592–1597. [Google Scholar]
- Hampson, N.B.; Bodwin, D. Toxic CO-ingestions in intentional carbon monoxide poisoning. J. Emerg. Med. 2013, 44, 625–630. [Google Scholar] [CrossRef] [PubMed]
- Targosz, D.; Sancewicz-Pach, K.; Szkolnicka, B.; Mitrus, M.; Kłys, M. Frequency and pattern of poisoning in adult and adolescent Kraków population in 2003 and 1983. Przegl. Lek. 2005, 62, 446–452. [Google Scholar] [PubMed]
- Lo, C.P.; Chen, S.Y.; Chou, M.C.; Wang, C.Y.; Lee, K.W.; Hsueh, C.J.; Chen, C.Y.; Huang, K.L.; Huang, G.S. Diffusion-tensor MR imaging for evaluation of the efficacy of hyperbaric oxygen therapy in patients with delayed neuropsychiatric syndrome caused by carbon monoxide inhalation. Eur. J. Neurol. 2007, 14, 777–782. [Google Scholar] [CrossRef] [PubMed]
- Murata, M.; Suzuki, M.; Hasegawa, Y.; Nohara, S.; Kurachi, M. Improvement of occipital alpha activity by repetitive hyperbaric oxygen therapy in patients with carbon monoxide poisoning: A possible indicator for treatment efficacy. J. Neurol. Sci. 2005, 235, 69–74. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study | Region | Period | Design | Cutoff Point of GCS (Low GCS Score) | No. of Patients (DNS/No DNS) | Age (DNS/No DNS) | Male(n) (DNS/No DNS) | HBOT (DNS/No DNS) | Maximum Time of Assessment of DNS |
|---|---|---|---|---|---|---|---|---|---|
| Liao et al., 2018 [30] | Taiwan | January 2009–December 2015 | retrospective, single | <9 | 62/404 | 41.0 (26.0–52.0)/ 32.0 (21.0–43.0) | 35/195 | 47/232 | 6 mon |
| Huang et al., 2019 [31] | Taiwan | January 2005–December 2014 | retrospective, single | <9 | 93/298 | 41.4 ± 14.7/ 39.7 ± 14.2 | 55/163 | 73/214 | 6 wks |
| Liao et al., 2019 [1] | Taiwan | January 2009–December 2015 | retrospective, single | <9 | 48/231 | 38.4 ± 16.1/33.3 ± 17.1 | 29/100 | 48/231 | 6 mon |
| Lin et al., 2018 [6] | Taiwan | January 1990–December 2011 | retrospective, multicenter | <9 | 47/591 | 44.2 ± 12.6/34.3 ± 16.3 | 27/284 | 38/505 | 2 yrs |
| Pepe et al., 2011 [25] | Italy | 1992–2007 | retrospective, single | <9 | 34/107 | 40.4 ± 15.5/41.7 ± 21.7 | 11/53 | 11/44 | 12 mon |
| Beppu 2011 [32] | Japan | April 2008–March 2010 | prospective, single | <9 | 3/20 | 55.0 ± 26.0/54.8 ± 19.2 | Not reported | 3/20 | 6 wks |
| Han et al., 2021 [9] | South Korea | July 2017–February 2020 | prospective, single | <10 | 38/165 | 44.0 (34.3–57.0)/43.0 (32.0–54.0) | 23/113 | 38/165 | 6 wks |
| Lee et al., 2020 [17] | South Korea | January 2018–July 2018 | retrospective, single | <10 | 12/126 | 47.0 (33.0–50.0)/36.0 (26.0–53.0) | 6/69 | 12/117 | 6 wks |
| Beppu 2013 [33] | Japan | April 2008–February 2011 | prospective, single | <9 | 3/19 | 44.3 ± 13.8/38.4 ± 10.9 | Not reported | 3/19 | 6 wks |
| Gaballah et al., 2020 [19] | Egypt | January 2018–December 2018 | prospective, single | <11 | 10/20 | 37.0 (18.0–55.0)/23.0 (15.0–40.0) | 7/12 | 2/2 | 6 mon |
| Characteristics | Development of DNS | |||
|---|---|---|---|---|
| n | OR (95%CI) | p-Value for Heterogeneity | I2 (%) | |
| All studies | ||||
| All | 10 | 2.98 (2.10–4.23) | 0.14 | 33 |
| Sample size | ||||
| ≥100 | 7 | 2.79 (1.98–3.93) | 0.16 | 36 |
| <100 | 3 | 8.31 (2.07–33.43) | 0.43 | 0 |
| Cutoff point (low GCS score group) | ||||
| <9 | 7 | 2.80 (1.91–4.12) | 0.17 | 34 |
| <10 or <11 | 3 | 4.24 (1.55–11.56) | 0.15 | 48 |
| Study quality | ||||
| High | 6 | 2.66 (1.83–3.88) | 0.14 | 40 |
| Low | 4 | 4.86 (2.36–10.00) | 0.48 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Namgung, M.; Oh, J.; Ahn, C.; Kim, C.W.; Lee, H.; Kang, H. Association between Glasgow Coma Scale in Early Carbon Monoxide Poisoning and Development of Delayed Neurological Sequelae: A Meta-Analysis. J. Pers. Med. 2022, 12, 635. https://doi.org/10.3390/jpm12040635
Namgung M, Oh J, Ahn C, Kim CW, Lee H, Kang H. Association between Glasgow Coma Scale in Early Carbon Monoxide Poisoning and Development of Delayed Neurological Sequelae: A Meta-Analysis. Journal of Personalized Medicine. 2022; 12(4):635. https://doi.org/10.3390/jpm12040635
Chicago/Turabian StyleNamgung, Myeong, Jaehoon Oh, Chiwon Ahn, Chan Woong Kim, Heekyung Lee, and Hyunggoo Kang. 2022. "Association between Glasgow Coma Scale in Early Carbon Monoxide Poisoning and Development of Delayed Neurological Sequelae: A Meta-Analysis" Journal of Personalized Medicine 12, no. 4: 635. https://doi.org/10.3390/jpm12040635