
Is the TOAST Classification Suitable for Use in Personalized Medicine in Ischemic Stroke?

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Examinations
2.3. Magnetic Resonance Imaging
2.4. Carotid Ultrasound
2.5. Ankle–Brachial Index
2.6. Reactive Hyperemia Index
2.7. Statistical Analyses
3. Results
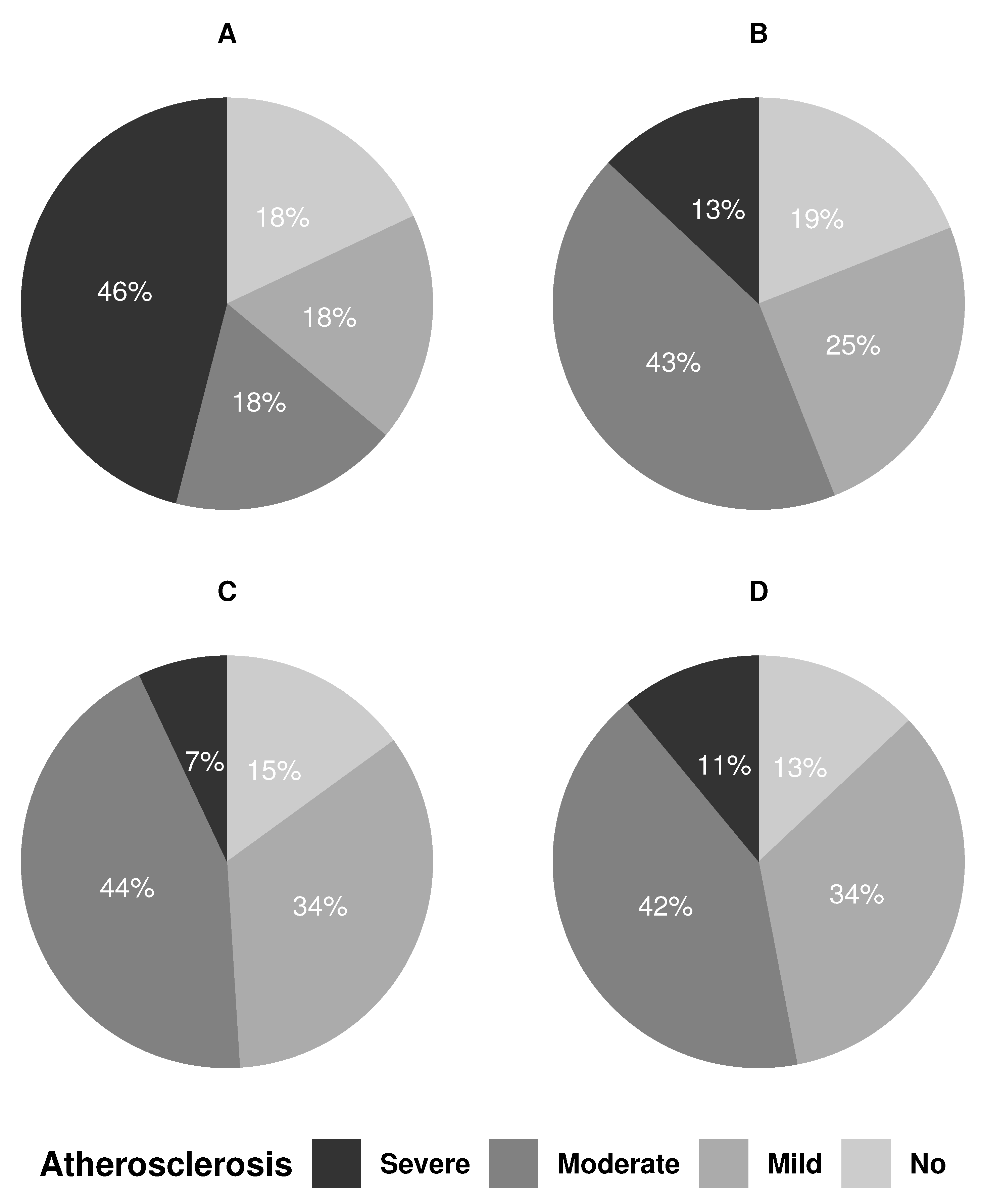
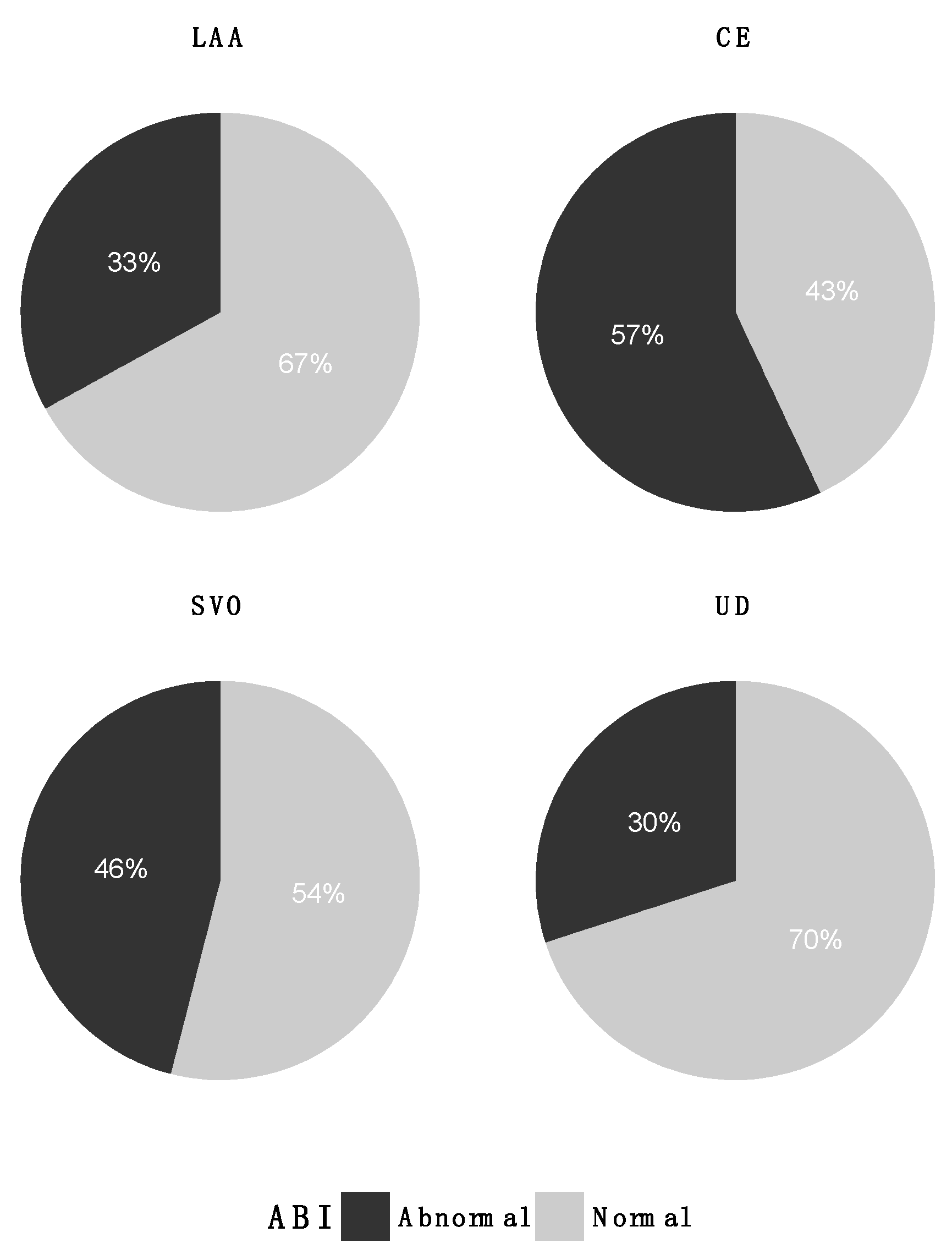
Vascular Parameters Related to TOAST Groups
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rostanski, S.K.; Marshall, R.S. Precision Medicine for Ischemic Stroke. JAMA Neurol. 2016, 73, 773–774. [Google Scholar] [CrossRef]
- Markus, H. Personalising secondary prevention: Different treatments for different strokes. Pract. Neurol. 2020, 20, 34–38. [Google Scholar] [CrossRef]
- Adams, H.P.; Bendixen, B.H.; Kappelle, L.J.; Biller, J.; Love, B.B.; Gordon, D.L.; Marsh, E.E. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke 1993, 24, 35–41. [Google Scholar] [CrossRef] [Green Version]
- Schulz, U.G.R. Differences in Vascular Risk Factors Between Etiological Subtypes of Ischemic Stroke: Importance of Population-Based Studies. Stroke 2003, 34, 2050–2059. [Google Scholar] [CrossRef] [Green Version]
- Weimar, C.; Goertler, M.; Röther, J.; Ringelstein, E.B.; Darius, H.; Nabavi, D.G.; Kim, I.-H.; Theobald, K.; Diener, H.-C. SCALA Study Group Systemic risk score evaluation in ischemic stroke patients (SCALA): A prospective cross sectional study in 85 German stroke units. J. Neurol. 2007, 254, 1562–1568. [Google Scholar] [CrossRef]
- Hong, J.B.; Leonards, C.O.; Endres, M.; Siegerink, B.; Liman, T.G. Ankle-Brachial Index and Recurrent Stroke Risk: Meta-Analysis. Stroke 2016, 47, 317–322. [Google Scholar] [CrossRef] [Green Version]
- Barreto-Neto, N.; Barros, A.D.; Jesus, P.A.P.; Reis, C.C.; Jesus, M.L.; Ferreira, I.L.O.; Fernandes, R.D.; Resende, L.L.; Andrade, A.L.; Gonçalves, B.M.; et al. Low Ankle-Brachial Index is a Simple Physical Exam Sign Predicting Intracranial Atherosclerotic Stenosis in Ischemic Stroke Patients. J. Stroke Cerebrovasc. Dis. 2016, 25, 1417–1420. [Google Scholar] [CrossRef]
- Del Brutto, O.H.; Sedler, M.J.; Mera, R.M.; Lama, J.; Gruen, J.A.; Phelan, K.J.; Cusick, E.H.; Zambrano, M.; Brown, D.L. The association of ankle-brachial index with silent cerebral small vessel disease: Results of the Atahualpa Project. Int. J. Stroke 2015, 10, 589–593. [Google Scholar] [CrossRef] [PubMed]
- Scherbakov, N.; Sandek, A.; Martens-Lobenhoffer, J.; Kung, T.; Turhan, G.; Liman, T.; Ebinger, M.; von Haehling, S.; Bode-Böger, S.M.; Endres, M.; et al. Endothelial Dysfunction of the Peripheral Vascular Bed in the Acute Phase after Ischemic Stroke. Cerebrovasc. Dis. 2012, 33, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Toyoda, K.; Ninomiya, T. Stroke and cerebrovascular diseases in patients with chronic kidney disease. Lancet Neurol. 2014, 13, 823–833. [Google Scholar] [CrossRef]
- Wardlaw, J.M.; Smith, E.E.; Biessels, G.J.; Cordonnier, C.; Fazekas, F.; Frayne, R.; Lindley, R.I.; O’Brien, J.T.; Barkhof, F.; Benavente, O.R.; et al. STandards for ReportIng Vascular changes on nEuroimaging (STRIVE v1) Neuroimaging standards for research into small vessel disease and its contribution to ageing and neurodegeneration. Lancet Neurol. 2013, 12, 822–838. [Google Scholar] [CrossRef] [Green Version]
- Staals, J.; Makin, S.D.J.; Doubal, F.N.; Dennis, M.S.; Wardlaw, J.M. Stroke subtype, vascular risk factors, and total MRI brain small-vessel disease burden. Neurology 2014, 83, 1228–1234. [Google Scholar] [CrossRef]
- Radu, R.A.; Terecoasă, E.O.; Băjenaru, O.A.; Tiu, C. Etiologic classification of ischemic stroke: Where do we stand? Clin. Neurol. Neurosurg. 2017, 159, 93–106. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Grant, E.G.; Benson, C.B.; Moneta, G.L.; Alexandrov, A.V.; Baker, J.D.; Bluth, E.I.; Carroll, B.A.; Eliasziw, M.; Gocke, J.; Hertzberg, B.S.; et al. Carotid artery stenosis: Grayscale and Doppler ultrasound diagnosis—Society of Radiologists in Ultrasound consensus conference. Ultrasound Q. 2003, 19, 190–198. [Google Scholar] [CrossRef]
- Espinola-Klein, C.; Rupprecht, H.J.; Bickel, C.; Lackner, K.; Savvidis, S.; Messow, C.M.; Münzel, T.; Blankenberg, S. AtheroGene Investigators Different calculations of ankle-brachial index and their impact on cardiovascular risk prediction. Circulation 2008, 118, 961–967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Resnick, H.E.; Lindsay, R.S.; McDermott, M.M.; Devereux, R.B.; Jones, K.L.; Fabsitz, R.R.; Howard, B.V. Relationship of high and low ankle brachial index to all-cause and cardiovascular disease mortality: The Strong Heart Study. Circulation 2004, 109, 733–739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuvin, J.T.; Patel, A.R.; Sliney, K.A.; Pandian, N.G.; Sheffy, J.; Schnall, R.P.; Karas, R.H.; Udelson, J.E. Assessment of peripheral vascular endothelial function with finger arterial pulse wave amplitude. Am. Heart J. 2003, 146, 168–174. [Google Scholar] [CrossRef]
- Hedetoft, M.; Olsen, N.V. Evaluation of endothelial function by peripheral arterial tonometry and relation with the nitric oxide pathway. Nitric Oxide 2014, 42, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Lau, K.K.; Li, L.; Schulz, U.; Simoni, M.; Chan, K.H.; Ho, S.L.; Cheung, R.T.F.; Küker, W.; Mak, H.K.F.; Rothwell, P.M. Total small vessel disease score and risk of recurrent stroke. Am. Acad. Neurol. 2017, 88, 2260–2267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, T.-J.; Kim, J.; Song, D.; Yoo, J.; Lee, H.S.; Kim, Y.-J.; Nam, H.S.; Heo, J.H.; Kim, Y.D. Total Cerebral Small-Vessel Disease Score is Associated with Mortality during Follow-Up after Acute Ischemic Stroke. J. Clin. Neurol. 2017, 13, 187–189. [Google Scholar] [CrossRef] [Green Version]
- Tuttolomondo, A.; Casuccio, A.; Della Corte, V.; Maida, C.; Pecoraro, R.; Di Raimondo, D.; Vassallo, V.; Simonetta, I.; Arnao, V.; Pinto, A. Endothelial function and arterial stiffness indexes in subjects with acute ischemic stroke: Relationship with TOAST subtype. Atherosclerosis 2017, 256, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Ratanakorn, D.; Keandoungchun, J.; Tegeler, C.H. Prevalence and Association between Risk Factors, Stroke Subtypes, and Abnormal Ankle Brachial Index in Acute Ischemic Stroke. J. Stroke Cerebrovasc. Dis. 2012, 21, 498–503. [Google Scholar] [CrossRef] [PubMed]
- Kanamaru, T.; Suda, S.; Muraga, K.; Okubo, S.; Watanabe, Y.; Tsuruoka, S.; Kimura, K. Albuminuria predicts early neurological deterioration in patients with acute ischemic stroke. J. Neurol. Sci. 2017, 372, 417–420. [Google Scholar] [CrossRef] [PubMed]
- Chwojnicki, K.; Król, E.; Wierucki, Ł.; Kozera, G.; Sobolewski, P.; Nyka, W.M.; Zdrojewski, T. Renal Dysfunction in Post-Stroke Patients. PLoS ONE 2016, 11, e0159775. [Google Scholar] [CrossRef] [PubMed]
- Buon, R.; Guidolin, B.; Jaffre, A.; Lafuma, M.; Barbieux, M.; Nasr, N.; Larrue, V. Carotid Ultrasound for Assessment of Nonobstructive Carotid Atherosclerosis in Young Adults with Cryptogenic Stroke. J. Stroke Cerebrovasc. Dis. 2018, 27, 1212–1216. [Google Scholar] [CrossRef] [PubMed]
- Becattini, C.; Dentali, F.; Camporese, G.; Sembolini, A.; Rancan, E.; Tonello, C.; Manina, G.; Padayattil, S.; Agnelli, G. Carotid atherosclerosis and risk for ischemic stroke in patients with atrial fibrillation on oral anticoagulant treatment. Atherosclerosis 2018, 271, 177–181. [Google Scholar] [CrossRef] [PubMed]
- Amarenco, P.; Albers, G.W.; Denison, H.; Easton, J.D.; Evans, S.R.; Held, P.; Hill, M.D.; Jonasson, J.; Kasner, S.E.; Ladenvall, P.; et al. Efficacy and safety of ticagrelor versus aspirin in acute stroke or transient ischaemic attack of atherosclerotic origin: A subgroup analysis of SOCRATES, a randomised, double-blind, controlled trial. Lancet Neurol. 2017, 16, 301–310. [Google Scholar] [CrossRef]
- Ay, H.; Furie, K.L.; Singhal, A.; Smith, W.S.; Sorensen, A.G.; Koroshetz, W.J. An evidence-based causative classification system for acute ischemic stroke. Ann. Neurol. 2005, 58, 688–697. [Google Scholar] [CrossRef] [PubMed]
- Ay, H.; Benner, T.; Murat Arsava, E.; Furie, K.L.; Singhal, A.B.; Jensen, M.B.; Ayata, C.; Towfighi, A.; Smith, E.E.; Chong, J.Y.; et al. A Computerized Algorithm for Etiologic Classification of Ischemic Stroke: The Causative Classification of Stroke System. Stroke 2007, 38, 2979–2984. [Google Scholar] [CrossRef] [Green Version]
- Amarenco, P.; Bogousslavsky, J.; Caplan, L.R.; Donnan, G.A.; Hennerici, M.G. New Approach to Stroke Subtyping: The A-S-C-O (Phenotypic) Classification of Stroke. Cerebrovasc. Dis. 2009, 27, 502–508. [Google Scholar] [CrossRef] [PubMed]
- Amarenco, P.; Bogousslavsky, J.; Caplan, L.R.; Donnan, G.A.; Wolf, M.E.; Hennerici, M.G. The ASCOD Phenotyping of Ischemic Stroke (Updated ASCO Phenotyping). Cerebrovasc. Dis. 2013, 36, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.J.; Kim, J.S. Ischemic Stroke Subtype Classification: An Asian Viewpoint. J. Stroke 2014, 16, 8–10. [Google Scholar] [CrossRef] [PubMed]
- Sandercock, P.A.G. Does Personalized Medicine Exist and Can You Test it in a Clinical Trial? Int. J. Stroke 2015, 10, 994–999. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients | Large Artery Atherosclerosis | Cardio-Embolism | Small Vessel Occlusion | Other Determined Etiology | Undetermined Etiology | p-Value | |
|---|---|---|---|---|---|---|---|
| n = 99 | n = 14 | n = 16 | n = 28 | n = 2 | n = 39 | ||
| Age, years | 68 (36–88) | 68 (45–81) | 73 (36–83) | 71 (47–88) | 52 (51–52) | 68 (41–85) | 0.082 |
| Sex | 0.017 | ||||||
| Men | 55 (55.6) | 5 (35.7) | 9 (56.2) | 11 (39.3) | 1 (50.0) | 29 (74.4) | |
| Woman | 44 (44.4) | 9 (64.3) | 7 (43.8) | 17 (60.7) | 1 (50.0) | 10 (25.6) | |
| mRS | 2 (0–5) | 2 (0–4) | 1 (0–4) | 2 (0–4) | 2 (2–2) | 2 (0–5) | 0.52 |
| NIHSS | 2 (0–16) | 2 (0–13) | 1 (0–13) | 2 (0–9) | 2 (1–3) | 2 (0–16) | 0.39 |
| Comorbidities | |||||||
| Hyper-tension | 59 (59.6) | 6 (42.9) | 11 (68.8) | 17 (60.7) | 1 (50.0) | 24 (61.5) | 0.67 |
| Diabetes type 2 | 20 (20.2) | 2 (14.3) | 6 (37.5) | 4 (14.3) | 0 (0.0) | 8 (20.5) | 0.41 |
| Hypercholesterolemia | 60 (60.6) | 10 (71.4) | 9 (56.2) | 19 (67.9) | 1 (50.0) | 21 (53.8) | 0.68 |
| Atrial fibrillation | 18 (18.2) | 0 (0.0) | 11 (68.8) | 0 (0.0) | 0 (0.0) | 8 (20.5) | <0.001 |
| Former stroke or TIA | 25 (25.3) | 4 (28.6) | 5 (31.2) | 10 (35.7) | 0 (0.0) | 6 (15.4) | 0.32 |
| SVD score | n = 89 | n = 14 | n = 13 | n = 25 | n = 2 | n = 35 | 0.59 |
| 0 | 29 (32.6) | 8 (57.1) | 5 (38.5) | 5 (20.0) | 2 (100.0) | 9 (25.7) | |
| 1 | 18 (20.2) | 2 (14.3) | 4 (30.8) | 5 (20.0) | 0 (0.0) | 7 (20.0) | |
| 2 | 19 (21.3) | 3 (21.4) | 2 (15.4) | 8 (32.0) | 0 (0.0) | 6 (17.1) | |
| 3 | 18 (20.2) | 1 (7.1) | 2 (15.4) | 5 (20.0) | 0 (0.0) | 10 (28.6) | |
| 4 | 5 (5.6) | 0 (0.0) | 0 (0.0) | 2 (8.0) | 0 (0.0) | 3 (8.6) | |
| Carotid examination | n = 94 | n = 11 | n = 16 | n = 27 | n = 2 | n = 38 | |
| Carotid stenosis ≥ 50% | 17 (17.2) | 6 (54.5) | 1 (6.3) | 2 (7.4) | 1 (50.0) | 7 (18.4) | 0.023 |
| Endothelial dysfunction | n = 90 | n = 12 | n = 13 | n = 26 | n = 2 | n = 37 | |
| RHI | 1.89 (0.82–3.81) | 2.21 (1.37–3.81) | 1.85 (1.28–2.42) | 1.83 (0.92–3.80) | 2.21 (1.86–2.55) | 1.90 (0.82–3.35) | 0.37 |
| Peripheral arterial disease | n = 89 | n = 12 | n = 14 | n = 24 | n = 2 | n = 37 | |
| ABI, mean (SD) | 0.93 (0.18) | 0.99 (0.11) | 0.88 (0.17) | 0.89 (0.19) | 0.81 (0.13) | 0.97 (0.20) | 0.20 |
| Renal function | n = 99 | n = 14 | n = 16 | n = 28 | n = 2 | n = 39 | |
| eGFR, mL/min/1.73 m2 | 82 (6–116) | 81 (39–116) | 81 (43–102) | 83 (6–102) | 95 (80–109) | 78 (18–105) | 0.79 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Simonsen, S.A.; West, A.S.; Heiberg, A.V.; Wolfram, F.; Jennum, P.J.; Iversen, H.K. Is the TOAST Classification Suitable for Use in Personalized Medicine in Ischemic Stroke? J. Pers. Med. 2022, 12, 496. https://doi.org/10.3390/jpm12030496
Simonsen SA, West AS, Heiberg AV, Wolfram F, Jennum PJ, Iversen HK. Is the TOAST Classification Suitable for Use in Personalized Medicine in Ischemic Stroke? Journal of Personalized Medicine. 2022; 12(3):496. https://doi.org/10.3390/jpm12030496
Chicago/Turabian StyleSimonsen, Sofie A., Anders S. West, Adam V. Heiberg, Frauke Wolfram, Poul J. Jennum, and Helle K. Iversen. 2022. "Is the TOAST Classification Suitable for Use in Personalized Medicine in Ischemic Stroke?" Journal of Personalized Medicine 12, no. 3: 496. https://doi.org/10.3390/jpm12030496