
The Morphology of a Kinematically Aligned Distal Femoral Osteotomy Is Different from That Obtained with Mechanical Alignment and Could Have Implications for the Design of Total Knee Arthroplasty


Abstract
:1. Introduction
2. Materials and Methods
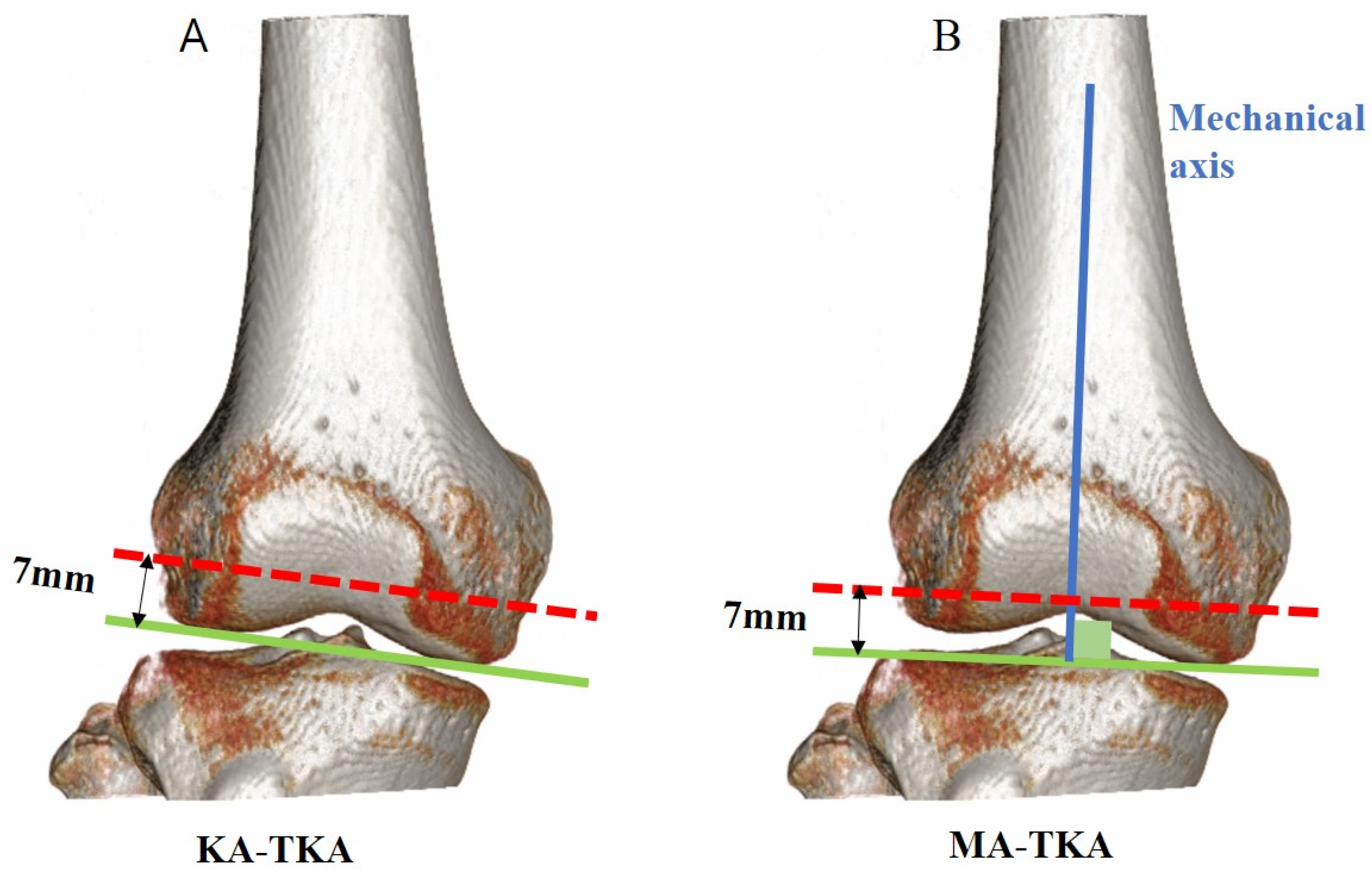
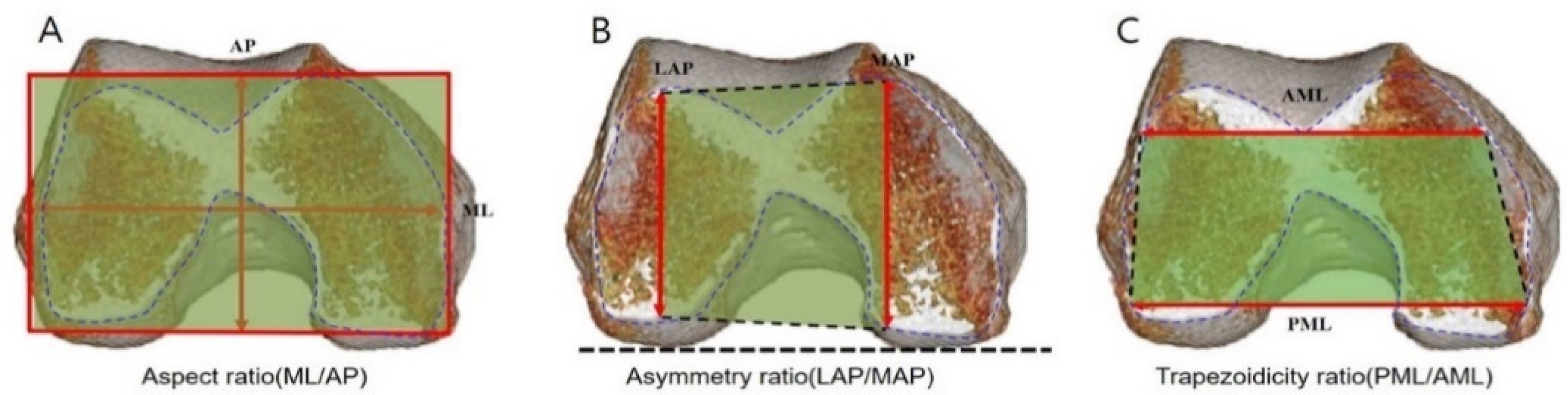
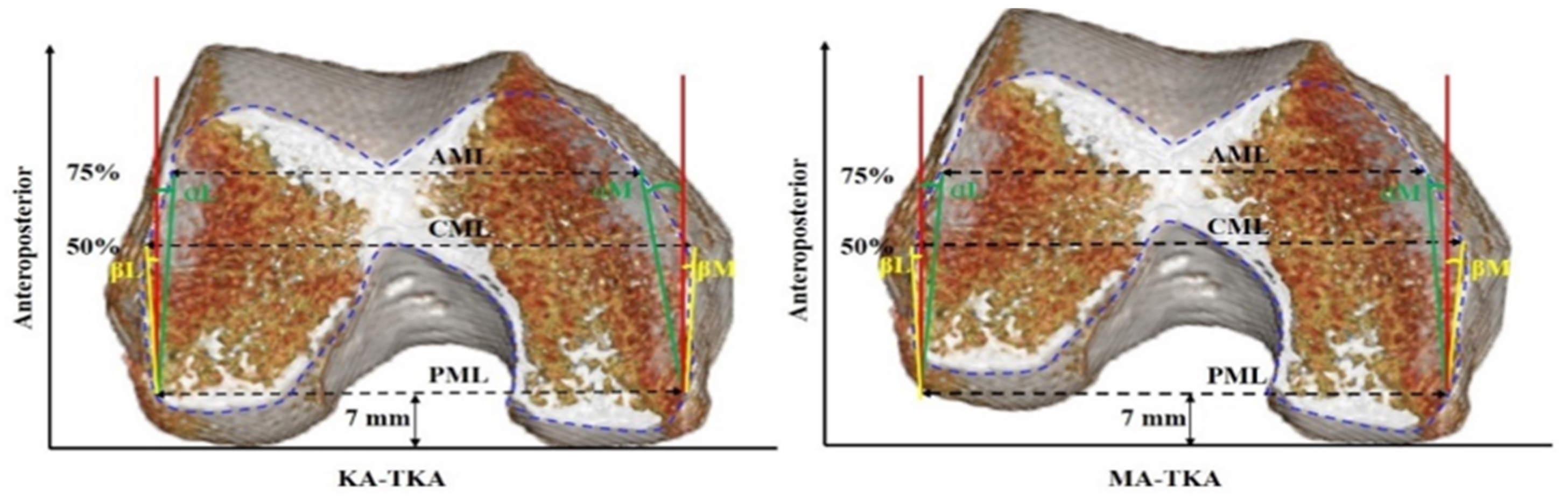
2.1. Virtual Surgery
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Choi, Y.J.; Ra, H.J. Patient Satisfaction after Total Knee Arthroplasty. Knee Surg. Relat. Res. 2016, 28, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahoney, O.M.; Kinsey, T. Overhang of the femoral component in total knee arthroplasty: Risk factors and clinical consequences. J. Bone Jt. Surg. Am. 2010, 92, 1115–1121. [Google Scholar] [CrossRef] [PubMed]
- Bonnin, M.P.; Schmidt, A.; Basiglini, L.; Bossard, N.; Dantony, E. Mediolateral oversizing influences pain, function, and flexion after TKA. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 2314–2324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beckers, L.; Müller, J.H.; Daxhelet, J.; Ratano, S.; Saffarini, M.; Aït-Si-Selmi, T.; Bonnin, M.P. Considerable inter-individual variability of tibial geometric ratios renders bone-implant mismatch unavoidable using off-the-shelf total knee arthroplasty: A systematic review and meta-analysis. Knee Surg. Sports Traumatol. Arthrosc. 2021. [Google Scholar] [CrossRef] [PubMed]
- Marmor, S.; Renault, E.; Valluy, J.; Saffarini, M. Over-voluming predicted by pre-operative planning in 24% of total knee arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 1544–1551. [Google Scholar] [CrossRef] [PubMed]
- Hitt, K.; Shurman, J.R., 2nd; Greene, K.; McCarthy, J.; Moskal, J.; Hoeman, T.; Mont, M.A. Anthropometric measurements of the human knee: Correlation to the sizing of current knee arthroplasty systems. J. Bone Jt. Surg. Am. 2003, 85 (Suppl. 4), 115–122. [Google Scholar] [CrossRef] [Green Version]
- Bellemans, J.; Carpentier, K.; Vandenneucker, H.; Vanlauwe, J.; Victor, J. The John Insall Award: Both morphotype and gender influence the shape of the knee in patients undergoing TKA. Clin. Orthop. Relat. Res. 2010, 468, 29–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishikawa, M.; Owaki, H.; Kaneshiro, S.; Fuji, T. Preoperative morphometric differences in the distal femur are based on skeletal size in Japanese patients undergoing total knee arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 2962–2968. [Google Scholar] [CrossRef] [PubMed]
- Hafez, M.A.; Sheikhedrees, S.M.; Saweeres, E.S. Anthropometry of Arabian Arthritic Knees: Comparison to Other Ethnic Groups and Implant Dimensions. J. Arthroplast. 2016, 31, 1109–1116. [Google Scholar] [CrossRef] [PubMed]
- Yin, X.; Yang, D.; Zhou, Y.; Shao, H.; Huang, Y.; Huang, X. Different femoral origins of valgus deformity affect aspect ratios of resected distal femurs in total knee arthroplasty. Knee 2019, 26, 1073–1079. [Google Scholar] [CrossRef] [PubMed]
- Bonnin, M.P.; Saffarini, M.; Bossard, N.; Dantony, E.; Victor, J. Morphometric analysis of the distal femur in total knee arthroplasty and native knees. Bone Jt. J. 2016, 98, 49–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, K.; Saffarini, M.; Valluy, J.; Desseroit, M.C.; Morvan, Y.; Telmon, N.; Cavaignac, E. Sexual and ethnic polymorphism render prosthetic overhang and under-coverage inevitable using off-the shelf TKA implants. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 2130–2139. [Google Scholar] [CrossRef] [PubMed]
- Beckers, L.; Muller, J.H.; Daxhelet, J.; Saffarini, M.; Ait-Si-Selmi, T.; Bonnin, M.P. Sexual dimorphism and racial diversity render bone-implant mismatch inevitable after off-the-shelf total knee arthroplasty: A systematic review and meta-analysis. Knee Surg. Sports Traumatol. Arthrosc. 2022, 30, 809–821. [Google Scholar] [CrossRef] [PubMed]
- Ji, H.M.; Han, J.; Jin, D.S.; Seo, H.; Won, Y.Y. Kinematically aligned TKA can align knee joint line to horizontal. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 2436–2441. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.S.; Howell, S.M.; Won, Y.Y.; Lee, O.S.; Lee, S.H.; Vahedi, H.; Teo, S.H. Kinematic alignment is a possible alternative to mechanical alignment in total knee arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 3467–3479. [Google Scholar] [CrossRef] [PubMed]
- Howell, S.M.; Shelton, T.J.; Hull, M.L. Implant Survival and Function Ten Years After Kinematically Aligned Total Knee Arthroplasty. J. Arthroplast. 2018, 33, 3678–3684. [Google Scholar] [CrossRef] [PubMed]
- Roussot, M.A.; Vles, G.F.; Oussedik, S. Clinical outcomes of kinematic alignment versus mechanical alignment in total knee arthroplasty: A systematic review. EFORT Open Rev. 2020, 5, 486–497. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.T.; Han, J.; Shen, Q.H.; Moon, S.W.; Won, Y.Y. Morphological Patterns of Anterior Femoral Condylar Resection in Kinematically and Mechanically Aligned Total Knee Arthroplasty. J. Arthroplast. 2018, 33, 2506–2511. [Google Scholar] [CrossRef] [PubMed]
- Pinskerova, V.; Nemec, K.; Landor, I. Gender differences in the morphology of the trochlea and the distal femur. Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 2342–2349. [Google Scholar] [CrossRef] [PubMed]
- Inui, H.; Taketomi, S.; Yamagami, R.; Shirakawa, N.; Kawaguchi, K.; Tanaka, S. The Relationship between Soft-Tissue Balance and Intraoperative Kinematics of Guided Motion Total Knee Arthroplasty. J. Knee Surg. 2019, 32, 91–96. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Total (n = 80) | Females (n = 50) | Males (n = 30) | |
|---|---|---|---|
| Mean ± SD (range) | Mean ± SD (range) | Mean ± SD (range) | |
| Age (year) | 72 ± 2.6 (52–77) | 73 ± 3.7 (61–80) | 70 ± 2.5 (52–79) |
| BMI (kg/m2) | 26.8 ± 3.5 (19.3–33.5) | 30.2 ± 5.6 (19.3–33.5) | 25.5 ± 3.2 (20.4–28.4) |
| KA-TKA (n = 80) | MA -TKA (n = 80) | ||
|---|---|---|---|
| Mean ± SD (range) | Mean ± SD (range) | p value | |
| MAP (mm) | 49.5 ± 2.5 (43.1–54.8) | 48.8 ± 3.9 (38.8–59.0) | 0.141 |
| LAP (mm) | 51.9 ± 3.0 (45.5–60.5) | 46.2 ± 4.2 (37.6–55.9) | 0.000 |
| AML (mm) | 59.3 ± 4.5 (50.4–70.7) | 59.1 ± 4.8 (49.8–70.4) | 0.802 |
| CML (mm) | 65.5 ± 4.8 (56.8–77.6) | 66.3 ± 5.5 (57.3–77.3) | 0.319 |
| PML (mm) | 67.8 ± 5.7 (57.1–79.9) | 69.7 ± 6.3 (58.4–82.4) | 0.042 |
| ML/AP | 1.3 ± 0.1 (1.2–1.5) | 1.4 ± 0.1 (1.3–1.6) | 0.000 |
| PML/AML | 1.1 ± 0.1(1.0–1.3) | 1.2 ± 0.1 (1.1–1.3) | 0.000 |
| LAP/MAP | 1.0 ± 0.0 (1.0–1.2) | 0.9 ± 0.0 (0.8–1.1) | 0.000 |
| αL (°) | 4.0 ± 3.1 (−5.2–10.3) | 8.8 ± 4.1 (−2.9–20.2) | 0.000 |
| βL (°) | 1.4 ± 5.8 (−14.5–11.1) | 4.2 ± 5.5 (−9.1–16.1) | 0.002 |
| αM (°) | 11.5 ± 4.3 (2.2–23.0) | 12.3 ± 5.0 (4.0–21.7) | 0.189 |
| βM (°) | 4.2 ± 5.3 (−10.6–14.9) | 11.6 ± 5.0 (−7.4–23.9) | 0.000 |
| KA-TKA (n = 30) | MA-TKA (n = 30) | ||
|---|---|---|---|
| Mean ± SD (range) | Mean ± SD (range) | p value | |
| MAP (mm) | 50.6 ± 2.5 (45.0–54.8) | 51.6 ± 3.5 (43.8–59.0) | 0.190 |
| LAP (mm) | 53.9 ± 3.0 (48.7–60.5) | 48.5 ± 4.2 (41.5–55.9) | 0.000 |
| AML (mm) | 63.2 ± 3.8 (56.8–70.7) | 63.6 ± 3.6 (56.8–70.4) | 0.666 |
| CML (mm) | 70.2 ± 3.3 (63.9–77.6) | 72.1 ± 3.4 (65.8–77.3) | 0.028 |
| PML (mm) | 73.7 ± 3.6 (63.3–79.9) | 76.3 ± 4.0 (69.3–82.4) | 0.011 |
| ML/AP | 1.4 ± 0.1 (1.2–1.5) | 1.5 ± 0.1 (1.3–1.6) | 0.000 |
| PML/AML | 1.2 ± 0.6 (1.1–1.3) | 1.2 ± 0.5 (1.1–1.3) | 0.010 |
| LAP/MAP | 1.1 ± 0.0 (1.0–1.2) | 0.9 ± 0.1 (0.8–1.0) | 0.000 |
| αL (°) | 5.4 ± 2.8 (−0.6–10.3) | 11.0 ± 3.7 (3.4–20.2) | 0.000 |
| βL (°) | 3.3 ± 5.1 (−7.1–11.1) | 5.9 ± 5.2 (−4.6–16.1) | 0.054 |
| αM (°) | 13.2 ± 4.5 (2.2–23.0) | 13.4 ± 3.9 (4.0–21.7) | 0.807 |
| βM (°) | 6.3 ± 4.7 (−3.6–14.9) | 11.6 ± 5.8 (−7.4–23.9) | 0.000 |
| KA-TKA (n = 50) | MA-TKA (n = 50) | ||
|---|---|---|---|
| Mean ± SD (range) | Mean ± SD (range) | p value | |
| MAP (mm) | 48.9 ± 2.4 (43.1–54.6) | 47.1 ± 3.0 (38.8–53.7) | 0.001 |
| LAP (mm) | 50.7 ± 2.3 (45.5–57.9) | 44.8 ± 3.6 (37.6–54.1) | 0.000 |
| AML (mm) | 56.9 ± 3.1 (50.4–64.9) | 56.4 ± 3.2 (49.8–65.9) | 0.380 |
| CML (mm) | 62.6 ± 3.1 (56.8–69.2) | 62.8 ± 3.1 (57.3–69.3) | 0.808 |
| PML (mm) | 64.2 ± 3.3 (57.1–72.2) | 65.8 ± 3.5 (58.4–75.0) | 0.024 |
| ML/AP | 1.3 ± 0.1 (1.2–1.4) | 1.4 ± 0.1 (1.3–1.6) | 0.000 |
| PML/AML | 1.1 ± 0.0 (1.0–1.3) | 1.2 ± 0.1 (1.1–1.3) | 0.000 |
| LAP/MAP | 1.0 ± 0.0 (1.0–1.1) | 0.9 ± 0.0 (0.8–1.1) | 0.000 |
| αL (°) | 3.2 ± 3.0 (−5.2–9.5) | 7.6 ± 4.0 (−2.9–16.6) | 0.000 |
| βL (°) | 0.2 ± 5.9 (−14.5–10.9) | 3.2 ± 5.4 (−9.1–13.5) | 0.010 |
| αM (°) | 10.5 ± 3.9 (2.8–17.9) | 11.7 ± 3.3 (4.3–18.7) | 0.109 |
| βM (°) | 2.9 ± 5.3 (−10.6–12.2) | 11.5 ± 4.5 (−2.7–20.9) | 0.000 |
| KA-TKA (Mean ± SD) | MA-TKA (Mean ± SD) | |||||
|---|---|---|---|---|---|---|
| Females | Males | p Value | Females | Males | p Value | |
| MAP (mm) | 48.9 ± 2.4 | 50.6 ± 2.5 | 0.004 | 47.1 ± 3.0 | 51.6 ± 3.5 | 0.000 |
| LAP (mm) | 50.7 ± 2.3 | 53.9 ± 3.0 | 0.000 | 44.8 ± 3.6 | 48.5 ± 4.2 | 0.000 |
| AML (mm) | 56.9 ± 3.1 | 63.2 ± 3.8 | 0.000 | 56.4 ± 3.2 | 63.6 ± 3.6 | 0.000 |
| CML (mm) | 62.6 ± 3.1 | 70.2 ± 3.3 | 0.000 | 62.8 ± 3.1 | 72.1 ± 3.4 | 0.000 |
| PML (mm) | 64.2 ± 3.3 | 73.7 ± 3.6 | 0.000 | 65.8 ± 3.5 | 76.3 ± 4.0 | 0.000 |
| ML/AP | 1.3 ± 0.1 | 1.4 ± 0.1 | 0.000 | 1.4 ± 0.1 | 1.5 ± 0.1 | 0.000 |
| PML/AML | 1.1 ± 0.0 | 1.2 ± 0.6 | 0.001 | 1.2 ± 0.1 | 1.2 ± 0.5 | 0.004 |
| LAP/MAP | 1.0 ± 0.0 | 1.1 ± 0.0 | 0.001 | 0.9 ± 0.0 | 0.9 ± 0.1 | 0.263 |
| αL (°) | 3.2 ± 3.0 | 5.4 ± 2.8 | 0.002 | 7.6 ± 4.0 | 11.0 ± 3.7 | 0.000 |
| βL (°) | 0.2 ± 5.9 | 3.3 ± 5.1 | 0.021 | 3.2 ±5.4 | 5.9 ± 5.2 | 0.029 |
| αM (°) | 10.5 ± 3.9 | 13.2 ± 4.5 | 0.007 | 11.7 ± 3.3 | 13.4 ± 3.9 | 0.031 |
| βM (°) | 2.9 ± 5.3 | 6.3 ± 4.7 | 0.004 | 11.5 ± 4.5 | 11.6 ± 5.8 | 0.942 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shen, Q.-H.; Baik, J.-W.; Won, Y.-Y. The Morphology of a Kinematically Aligned Distal Femoral Osteotomy Is Different from That Obtained with Mechanical Alignment and Could Have Implications for the Design of Total Knee Arthroplasty. J. Pers. Med. 2022, 12, 422. https://doi.org/10.3390/jpm12030422
Shen Q-H, Baik J-W, Won Y-Y. The Morphology of a Kinematically Aligned Distal Femoral Osteotomy Is Different from That Obtained with Mechanical Alignment and Could Have Implications for the Design of Total Knee Arthroplasty. Journal of Personalized Medicine. 2022; 12(3):422. https://doi.org/10.3390/jpm12030422
Chicago/Turabian StyleShen, Quan-Hu, Ji-Woong Baik, and Ye-Yeon Won. 2022. "The Morphology of a Kinematically Aligned Distal Femoral Osteotomy Is Different from That Obtained with Mechanical Alignment and Could Have Implications for the Design of Total Knee Arthroplasty" Journal of Personalized Medicine 12, no. 3: 422. https://doi.org/10.3390/jpm12030422