
Artificial Intelligence in Cardiovascular Atherosclerosis Imaging


Abstract
:1. Introduction
2. Application of AI in Coronary Atherosclerotic Plaque
2.1. Overview of Artificial Intelligence
2.2. Coronary Atherosclerotic Plaque
2.3. Characterization of Coronary Atherosclerotic Plaques
2.4. Detection of Coronary Atherosclerotic Plaque
3. Application of AI in Coronary Atherosclerotic Plaque Analysis
3.1. Identification of Vulnerable Plaques
3.2. Assessment of Myocardium
3.3. Risk Prediction
4. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| AI | Artificial intelligence |
| MACEs | Major adverse cardiac events |
| CVDs | Cardiovascular disease |
| CAD | Coronary artery disease |
| OCT | Optical coherence tomography |
| CT | Computed tomography |
| MRI | Magnetic resonance imaging |
| IVUS | Intravascular ultrasound |
| AS | Atherosclerosis |
| ACS | Acute coronary syndrome |
| ML | Machine learning |
| DL | Deep learning |
| ROI | Region of interest |
References
- Mattiuzzi, C.; Lippi, G. Cancer statistics: A comparison between World Health Organization (WHO) and Global Burden of Disease (GBD). Eur. J. Public Health 2020, 30, 1026–1027. [Google Scholar] [CrossRef] [PubMed]
- Walli-Attaei, M.; Joseph, P.; Rosengren, A.; Chow, C.K.; Rangarajan, S.; Lear, S.A.; AlHabib, K.F.; Davletov, K.; Dans, A.; Lanas, F.; et al. Variations between women and men in risk factors, treatments, cardiovascular disease incidence, and death in 27 high-income, middle-income, and low-income countries (PURE): A prospective cohort study. Lancet 2020, 396, 97–109. [Google Scholar] [CrossRef]
- Plana, J.C.; Thavendiranathan, P.; Bucciarelli-Ducci, C.; Lancellotti, P. Multi-Modality Imaging in the Assessment of Cardiovascular Toxicity in the Cancer Patient. JACC Cardiovasc. Imaging 2018, 11, 1173–1186. [Google Scholar] [CrossRef] [PubMed]
- Williams, A.M.; Liu, Y.; Regner, K.R.; Jotterand, F.; Liu, P.; Liang, M. Artificial intelligence, physiological genomics, and precision medicine. Physiol. Genom. 2018, 50, 237–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henglin, M.; Stein, G.; Hushcha, P.V.; Snoek, J.; Wiltschko, A.B.; Cheng, S. Machine Learning Approaches in Cardiovascular Imaging. Circ. Cardiovasc. Imaging 2017, 10, e005614. [Google Scholar] [CrossRef]
- Jordan, M.I.; Mitchell, T.M. Machine learning: Trends, perspectives, and prospects. Science 2015, 349, 255–260. [Google Scholar] [CrossRef]
- Nicol, E.D.; Norgaard, B.L.; Blanke, P.; Ahmadi, A.; Weir-McCall, J.; Horvat, P.M.; Han, K.; Bax, J.J.; Leipsic, J. The Future of Cardiovascular Computed Tomography: Advanced Analytics and Clinical Insights. JACC Cardiovasc. Imaging 2019, 12, 1058–1072. [Google Scholar] [CrossRef]
- Dey, D.; Slomka, P.J.; Leeson, P.; Comaniciu, D.; Shrestha, S.; Sengupta, P.P.; Marwick, T.H. Artificial Intelligence in Cardiovascular Imaging: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2019, 73, 1317–1335. [Google Scholar] [CrossRef]
- Al’Aref, S.J.; Anchouche, K.; Singh, G.; Slomka, P.J.; Kolli, K.K.; Kumar, A.; Pandey, M.; Maliakal, G.; Van Rosendael, A.R.; Beecy, A.N.; et al. Clinical applications of machine learning in cardiovascular disease and its relevance to cardiac imaging. Eur. Heart J. 2019, 40, 1975–1986. [Google Scholar] [CrossRef]
- Johnson, K.; Soto, J.T.; Glicksberg, B.; Shameer, K.; Miotto, R.; Ali, M.; Ashley, E.; Dudley, J.T. Artificial Intelligence in Cardiology. J. Am. Coll. Cardiol. 2018, 71, 2668–2679. [Google Scholar] [CrossRef]
- Ching, T.; Himmelstein, D.S.; Beaulieu-Jones, B.K.; Kalinin, A.A.; Do, B.T.; Way, G.P.; Ferrero, E.; Agapow, P.M.; Zietz, M.; Hoffman, M.M.; et al. Opportunities and obstacles for deep learning in biology and medicine. J. R. Soc. Interface 2018, 15, 20170387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lancet, T. Artificial intelligence in health care: Within touching distance. Lancet 2017, 390, 2739. [Google Scholar] [CrossRef]
- Tearney, G.J.; Regar, E.; Akasaka, T.; Adriaenssens, T.; Barlis, P.; Bezerra, H.G.; Bouma, B.; Bruining, N.; Cho, J.M.; Chowdhary, S.; et al. Consensus standards for acquisition, measurement, and reporting of intravascular optical coherence tomography studies: A report from the International Working Group for Intravascular Optical Coherence Tomography Standardization and Validation. J. Am. Coll. Cardiol. 2012, 59, 1058–1072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camacho, D.; Collins, K.M.; Powers, R.K.; Costello, J.C.; Collins, J.J. Next-Generation Machine Learning for Biological Networks. Cell 2018, 173, 1581–1592. [Google Scholar] [CrossRef] [Green Version]
- Sohail, A.; Arif, F. Supervised and unsupervised algorithms for bioinformatics and data science. Prog. Biophys. Mol. Biol. 2020, 151, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Ross, R. The pathogenesis of atherosclerosis: A perspective for the 1990s. Nature 1993, 362, 801–809. [Google Scholar] [CrossRef]
- Weissberg, P.L.; Bennett, M.R. Atherosclerosis—An inflammatory disease. N. Engl. J. Med. 1999, 340, 1928–1929. [Google Scholar]
- Libby, P.; Ridker, P.M.; Hansson, G.K. Progress and challenges in translating the biology of atherosclerosis. Nature 2011, 473, 317–325. [Google Scholar] [CrossRef]
- Bentzon, J.F.; Otsuka, F.; Virmani, R.; Falk, E. Mechanisms of plaque formation and rupture. Circ. Res. 2014, 114, 1852–1866. [Google Scholar] [CrossRef]
- Otsuka, F.; Yasuda, S.; Noguchi, T.; Ishibashi-Ueda, H. Pathology of coronary atherosclerosis and thrombosis. Cardiovasc. Diagn. Ther. 2016, 6, 396–408. [Google Scholar] [CrossRef] [Green Version]
- Kriszbacher, I.; Koppan, M.; Bodis, J. Inflammation, atherosclerosis, and coronary artery disease. N. Engl. J. Med. 2005, 353, 429–430. [Google Scholar] [PubMed]
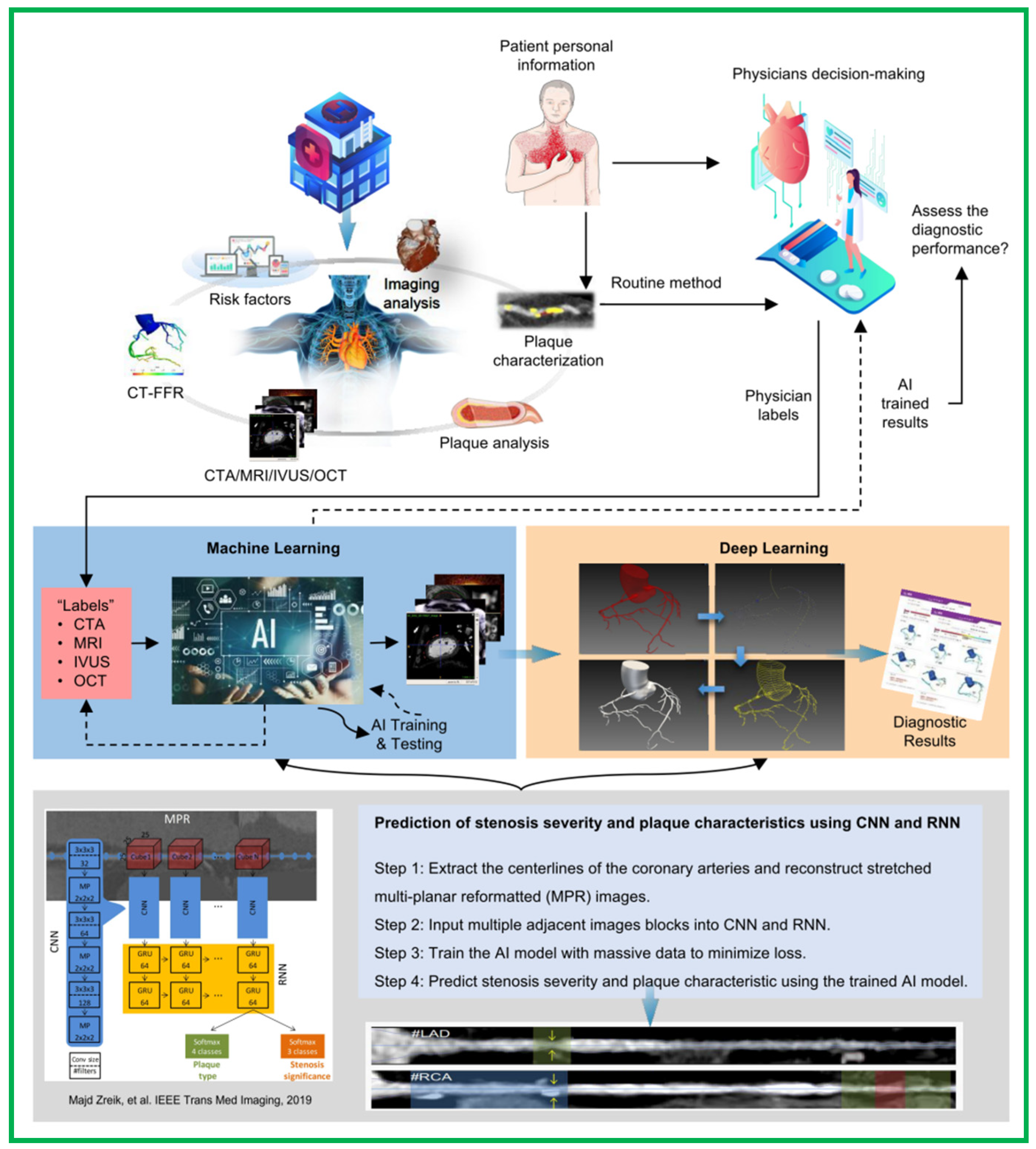
- Zreik, M.; Van Hamersvelt, R.W.; Wolterink, J.M.; Leiner, T.; Viergever, M.A.; Isgum, I. AA Recurrent CNN for Automatic Detection and Classification of Coronary Artery Plaque and Stenosis in Coronary CT Angiography. IEEE Trans. Med. Imaging 2019, 38, 1588–1598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Acharya, U.R.; Meiburger, K.M.; Koh, J.E.W.; Vicnesh, J.; Ciaccio, E.J.; Lih, O.S.; Tan, S.K.; Aman, R.R.A.R.; Molinari, F.; Ng, K.H. Automated plaque classification using computed tomography angiography and Gabor transformations. Artif. Intell. Med. 2019, 100, 101724. [Google Scholar] [CrossRef] [PubMed]
- Kolluru, C.; Prabhu, D.; Gharaibeh, Y.; Bezerra, H.; Guagliumi, G.; Wilson, D. Deep neural networks for A-line-based plaque classification in coronary intravascular optical coherence tomography images. J. Med. Imaging 2018, 5, 044504. [Google Scholar] [CrossRef]
- Yamak, D.; Panse, P.; Pavlicek, W.; Boltz, T.; Akay, M. Non-calcified coronary atherosclerotic plaque characterization by dual energy computed tomography. IEEE J. Biomed. Health Inform. 2014, 18, 939–945. [Google Scholar] [CrossRef]
- Kim, G.Y.; Lee, J.H.; Na Hwang, Y.; Kim, S.M. A novel intensity-based multi-level classification approach for coronary plaque characterization in intravascular ultrasound images. Biomed. Eng. Online 2018, 17, 151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheet, D.; Karamalis, A.; Eslami, A.; Noël, P.; Chatterjee, J.; Ray, A.K.; Laine, A.F.; Carlier, S.G.; Navab, N.; Katouzian, A. Joint learning of ultrasonic backscattering statistical physics and signal confidence primal for characterizing atherosclerotic plaques using intravascular ultrasound. Med. Image Anal. 2014, 18, 103–117. [Google Scholar] [CrossRef] [PubMed]
- Shalev, R.; Bezerra, H.G.; Ray, S.; Prabhu, D.; Wilson, D.L. Classification of calcium in intravascular OCT images for the purpose of intervention planning. In Proceedings of the Medical Imaging 2016: Image-Guided Procedures, Robotic Interventions, and Modeling, San Diego, CA, USA, 27 February–3 March 2016; Volume 9786, p. 978605. [Google Scholar] [CrossRef] [Green Version]
- Xu, M.; Cheng, J.; Wong, D.W.K.; Taruya, A.; Tanaka, A.; Liu, J. Automatic atherosclerotic heart disease detection in intracoronary optical coherence tomography images. In Proceedings of the 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 26 February–30 August 2014; pp. 174–177. [Google Scholar] [CrossRef]
- Zhou, P.; Zhu, T.; He, C.; Li, Z.-Y. Automatic classification of atherosclerotic tissue in intravascular optical coherence tomography images. J. Opt. Soc. Am. A Opt. Image Sci. Vis. 2017, 34, 1152–1159. [Google Scholar] [CrossRef]
- Kolluru, C.; Prabhu, D.; Gharaibeh, Y.; Wu, H.; Wilson, D.L. Voxel-based plaque classification in coronary intravascular optical coherence tomography images using decision trees. In Proceedings of the Medical Imaging 2018: Computer-Aided Diagnosis, Houston, TX, USA, 10–15 February 2018; Volume 10575, p. 105752Y. [Google Scholar] [CrossRef] [Green Version]
- Rico-Jimenez, J.J.; Campos-Delgado, D.U.; Villiger, M.; Otsuka, K.; Bouma, B.E.; Jo, J.A. Automatic classification of atherosclerotic plaques imaged with intravascular OCT. Biomed. Opt. Express 2016, 7, 4069–4085. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.; Prabhu, D.; Kolluru, C.; Gharaibeh, Y.; Zimin, V.N.; Bezerra, H.G.; Wilson, D.L. Automated plaque characterization using deep learning on coronary intravascular optical coherence tomographic images. Biomed. Opt. Express 2019, 10, 6497–6515. [Google Scholar] [CrossRef] [PubMed]
- Stocker, T.J.; Deseive, S.; Leipsic, J.; Hadamitzky, M.; Chen, M.Y.; Rubinshtein, R.; Heckner, M.; Bax, J.J.; Fang, X.M.; Grove, E.L.; et al. Reduction in radiation exposure in cardiovascular computed tomography imaging: Results from the PROspective multicenter registry on radiaTion dose Estimates of cardiac CT angIOgraphy iN daily practice in 2017 (PROTECTION VI). Eur. Heart J. 2018, 39, 3715–3723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Athanasiou, L.S.; Exarchos, T.P.; Naka, K.K.; Michalis, L.K.; Prati, F.; Fotiadis, D.I. Atherosclerotic plaque characterization in Optical Coherence Tomography images. In Proceedings of the 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Boston, MA, USA, 30 August–3 September 2011; pp. 4485–4488. [Google Scholar] [CrossRef] [PubMed]
- Kolossváry, M.; Karády, J.; Szilveszter, B.; Kitslaar, P.; Hoffmann, U.; Merkely, B.; Maurovich-Horvat, P. Radiomic Features Are Superior to Conventional Quantitative Computed Tomographic Metrics to Identify Coronary Plaques with Napkin-Ring Sign. Circ. Cardiovasc. Imaging 2017, 10, e006843. [Google Scholar] [CrossRef]
- Tarkin, J.; Dweck, M.; Evans, N.R.; Takx, R.A.; Brown, A.J.; Tawakol, A.; Fayad, Z.A.; Rudd, J.H. Imaging Atherosclerosis. Circ. Res. 2016, 118, 750–769. [Google Scholar] [CrossRef] [Green Version]
- Puchner, S.B.; Liu, T.; Mayrhofer, T.; Truong, Q.A.; Lee, H.; Fleg, J.L.; Nagurney, J.T.; Udelson, J.E.; Hoffmann, U.; Ferencik, M. High-risk plaque detected on coronary CT angiography predicts acute coronary syndromes independent of significant stenosis in acute chest pain: Results from the ROMICAT-II trial. J. Am. Coll. Cardiol. 2014, 64, 684–692. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Fleischmann, D. Improving Spatial Resolution at CT: Development, Benefits, and Pitfalls. Radiology 2018, 289, 261–262. [Google Scholar] [CrossRef] [Green Version]
- Nordbeck, P.; Ertl, G.; Ritter, O. Magnetic resonance imaging safety in pacemaker and implantable cardioverter defibrillator patients: How far have we come? Eur. Heart J. 2015, 36, 1505–1511. [Google Scholar] [CrossRef] [Green Version]
- Peters, R.J.; Kok, W.E.; Havenith, M.G.; Rijsterborgh, H.; van der Wal, A.; Visser, C.A. Histopathologic validation of intracoronary ultrasound imaging. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 1994, 7, 230–241. [Google Scholar] [CrossRef]
- Pighi, M.; Gratta, A.; Marin, F.; Bellamoli, M.; Lunardi, M.; Fezzi, S.; Zivelonghi, C.; Pesarini, G.; Tomai, F.; Ribichini, F. Cardiac allograft vasculopathy: Pathogenesis, diagnosis and therapy. Transplant Rev. (Orlando) 2020, 34, 100569. [Google Scholar] [CrossRef] [PubMed]
- Schaar, J.A.; Muller, J.E.; Falk, E.; Virmani, R.; Fuster, V.; Serruys, P.W.; Colombo, A.; Stefanadis, C.; Casscells, S.W.; Moreno, P.R.; et al. Terminology for high-risk and vulnerable coronary artery plaques. Report of a meeting on the vulnerable plaque, 17–18 June 2003, Santorini, Greece. Eur. Heart J. 2004, 25, 1077–1082. [Google Scholar] [CrossRef] [PubMed]
- Virmani, R.; Kolodgie, F.D.; Burke, A.P.; Farb, A.; Schwartz, S.M. Lessons from sudden coronary death: A comprehensive morphological classification scheme for atherosclerotic lesions. Arterioscler. Thromb. Vasc. Biol. 2000, 20, 1262–1275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jia, H.; Abtahian, F.; Aguirre, A.D.; Lee, S.; Chia, S.; Lowe, H.; Kato, K.; Yonetsu, T.; Vergallo, R.; Hu, S.; et al. In vivo diagnosis of plaque erosion and calcified nodule in patients with acute coronary syndrome by intravascular optical coherence tomography. J. Am. Coll. Cardiol. 2013, 62, 1748–1758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolossváry, M.; Karády, J.; Kikuchi, Y.; Ivanov, A.; Schlett, C.L.; Lu, M.T.; Foldyna, B.; Merkely, B.; Aerts, H.J.; Hoffmann, U.; et al. Radiomics versus Visual and Histogram-based Assessment to Identify Atheromatous Lesions at Coronary CT Angiography: An ex Vivo Study. Radiology 2019, 293, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Kolossváry, M.; Park, J.; Bang, J.-I.; Zhang, J.; Lee, J.M.; Paeng, J.C.; Merkely, B.; Narula, J.; Kubo, T.; Akasaka, T.; et al. Identification of invasive and radionuclide imaging markers of coronary plaque vulnerability using radiomic analysis of coronary computed tomography angiography. Eur. Heart J. Cardiovasc. Imaging 2019, 20, 1250–1258. [Google Scholar] [CrossRef] [PubMed]
- Sheet, D.; Karamalis, A.; Eslami, A.; Noël, P.; Virmani, R.; Nakano, M.; Chatterjee, J.; Ray, A.K.; Laine, A.F.; Carlier, S.; et al. Hunting for necrosis in the shadows of intravascular ultrasound. Comput. Med. Imaging Graph. Off. J. Comput. Med. Imaging Soc. 2014, 38, 104–112. [Google Scholar] [CrossRef]
- Wang, Z.; Chamié, D.; Bezerra, H.G.; Yamamoto, H.; Kanovsky, J.; Wilson, D.L.; Costa, M.A.; Rollins, A.M. Volumetric quantification of fibrous caps using intravascular optical coherence tomography. Biomed. Opt. Express 2012, 3, 1413–1426. [Google Scholar] [CrossRef]
- Liu, R.; Zhang, Y.; Zheng, Y.; Liu, Y.; Zhao, Y.; Yi, L. Automated Detection of Vulnerable Plaque for Intravascular Optical Coherence Tomography Images. Cardiovasc. Eng. Technol. 2019, 10, 590–603. [Google Scholar] [CrossRef]
- Lee, J.M.; Choi, G.; Koo, B.-K.; Hwang, D.; Park, J.; Zhang, J.; Kim, K.-J.; Tong, Y.; Kim, H.J.; Grady, L.; et al. Identification of High-Risk Plaques Destined to Cause Acute Coronary Syndrome Using Coronary Computed Tomographic Angiography and Computational Fluid Dynamics. JACC Cardiovasc. Imaging 2019, 12, 1032–1043. [Google Scholar] [CrossRef]
- Park, J.B.; Choi, G.; Chun, E.J.; Kim, H.J.; Park, J.; Jung, J.H.; Lee, M.-H.; Otake, H.; Doh, J.H.; Nam, C.W.; et al. Computational fluid dynamic measures of wall shear stress are related to coronary lesion characteristics. Heart 2016, 102, 1655–1661. [Google Scholar] [CrossRef] [PubMed]
- Samady, H.; Eshtehardi, P.; McDaniel, M.C.; Suo, J.; Dhawan, S.S.; Maynard, C.; Timmins, L.H.; Quyyumi, A.A.; Giddens, D.P. Coronary artery wall shear stress is associated with progression and transformation of atherosclerotic plaque and arterial remodeling in patients with coronary artery disease. Circulation 2011, 124, 779–788. [Google Scholar] [CrossRef] [Green Version]
- Choi, G.; Lee, J.M.; Kim, H.J.; Park, J.B.; Sankaran, S.; Otake, H.; Doh, J.H.; Nam, C.W.; Shin, E.S.; Taylor, C.A.; et al. Coronary Artery Axial Plaque Stress and its Relationship with Lesion Geometry: Application of Computational Fluid Dynamics to Coronary CT Angiography. JACC Cardiovasc. Imaging 2015, 8, 1156–1166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tonino, P.A.; De Bruyne, B.; Pijls, N.H.; Siebert, U.; Ikeno, F.; van’t Veer, M.; Klauss, V.; Manoharan, G.; Engstrøm, T.; Oldroyd, K.G.; et al. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. N. Engl. J. Med. 2009, 360, 213–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Nunen, L.X.; Zimmermann, F.M.; Tonino, P.A.L.; Barbato, E.; Baumbach, A.; Engstrøm, T.; Klauss, V.; MacCarthy, P.A.; Manoharan, G.; Oldroyd, K.G.; et al. Fractional flow reserve versus angiography for guidance of PCI in patients with multivessel coronary artery disease (FAME): 5-year follow-up of a randomised controlled trial. Lancet 2015, 386, 1853–1860. [Google Scholar] [CrossRef]
- Nakazato, R.; Shalev, A.; Doh, J.H.; Koo, B.K.; Gransar, H.; Gomez, M.J.; Leipsic, J.; Park, H.B.; Berman, D.S.; Min, J.K. Aggregate plaque volume by coronary computed tomography angiography is superior and incremental to luminal narrowing for diagnosis of ischemic lesions of intermediate stenosis severity. J. Am. Coll. Cardiol. 2013, 62, 460–467. [Google Scholar] [CrossRef] [Green Version]
- Dey, D.; Zamudio, M.D.; Schuhbaeck, A.; Orozco, L.E.J.; Otaki, Y.; Gransar, H.; Li, D.; Germano, G.; Achenbach, S.; Berman, D.S.; et al. Relationship Between Quantitative Adverse Plaque Features from Coronary Computed Tomography Angiography and Downstream Impaired Myocardial Flow Reserve by 13N-Ammonia Positron Emission Tomography: A Pilot Study. Circ. Cardiovasc. Imaging 2015, 8, e003255. [Google Scholar] [CrossRef] [Green Version]
- Dey, D.; Gaur, S.; Ovrehus, K.A.; Slomka, P.J.; Betancur, J.; Goeller, M.; Hell, M.M.; Gransar, H.; Berman, D.S.; Achenbach, S.; et al. Integrated prediction of lesion-specific ischaemia from quantitative coronary CT angiography using machine learning: A multicentre study. Eur. Radiol. 2018, 28, 2655–2664. [Google Scholar] [CrossRef]
- Gaur, S.; Øvrehus, K.A.; Dey, D.; Leipsic, J.; Bøtker, H.E.; Jensen, J.M.; Narula, J.; Ahmadi, A.; Achenbach, S.; Ko, B.S.; et al. Coronary plaque quantification and fractional flow reserve by coronary computed tomography angiography identify ischaemia-causing lesions. Eur. Heart J. 2016, 37, 1220–1227. [Google Scholar] [CrossRef]
- von Knebel Doeberitz, P.L.; De Cecco, C.N.; Schoepf, U.J.; Duguay, T.M.; Albrecht, M.H.; Van Assen, M.; Bauer, M.J.; Savage, R.H.; Pannell, J.T.; De Santis, D.; et al. Coronary CT angiography-derived plaque quantification with artificial intelligence CT fractional flow reserve for the identification of lesion-specific ischemia. Eur. Radiol. 2019, 29, 2378–2387. [Google Scholar] [CrossRef]
- Kawasaki, T.; Kidoh, M.; Kido, T.; Sueta, D.; Fujimoto, S.; Kumamaru, K.K.; Uetani, T.; Tanabe, Y.; Ueda, T.; Sakabe, D.; et al. Evaluation of Significant Coronary Artery Disease Based on CT Fractional Flow Reserve and Plaque Characteristics Using Random Forest Analysis in Machine Learning. Acad. Radiol. 2020, 27, 1700–1708. [Google Scholar] [CrossRef] [PubMed]
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics-2020 Update: A Report from the American Heart Association. Circulation 2020, 141, e139–e596. [Google Scholar] [CrossRef] [PubMed]
- Sarwar, N.; Gao, P.; Seshasai, S.R.; Gobin, R.; Kaptoge, S.; Di Angelantonio, E.; Ingelsson, E.; Lawlor, D.A.; Selvin, E.; Stampfer, M.; et al. Diabetes mellitus, fasting blood glucose concentration, and risk of vascular disease: A collaborative meta-analysis of 102 prospective studies. Lancet 2010, 375, 2215–2222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, I.; Al’Aref, S.J.; Berger, A.; Hartaigh, B.Ó.; Gransar, H.; Valenti, V.; Lin, F.Y.; Achenbach, S.; Berman, D.S.; Budoff, M.J.; et al. Prognostic value of coronary computed tomographic angiography findings in asymptomatic individuals: A 6-year follow-up from the prospective multicentre international CONFIRM study. Eur. Heart J. 2018, 39, 934–941. [Google Scholar] [CrossRef] [PubMed]
- Williams, M.C.; Hunter, A.; Shah, A.S.V.; Assi, V.; Lewis, S.; Smith, J.; Berry, C.; Boon, N.A.; Clark, E.; Flather, M.; et al. Use of Coronary Computed Tomographic Angiography to Guide Management of Patients with Coronary Disease. J. Am. Coll. Cardiol. 2016, 67, 1759–1768. [Google Scholar] [CrossRef] [Green Version]
- Araki, T.; Ikeda, N.; Shukla, D.; Londhe, N.D.; Shrivastava, V.; Banchhor, S.K.; Saba, L.; Nicolaides, A.; Shafique, S.; Laird, J.R.; et al. A new method for IVUS-based coronary artery disease risk stratification: A link between coronary & carotid ultrasound plaque burdens. Comput. Methods Programs Biomed. 2016, 124, 161–179. [Google Scholar] [CrossRef]
- Araki, T.; Ikeda, N.; Shukla, D.; Jain, P.K.; Londhe, N.D.; Shrivastava, V.K.; Banchhor, S.K.; Saba, L.; Nicolaides, A.; Shafique, S.; et al. PCA-based polling strategy in machine learning framework for coronary artery disease risk assessment in intravascular ultrasound: A link between carotid and coronary grayscale plaque morphology. Comput. Methods Programs Biomed. 2016, 128, 137–158. [Google Scholar] [CrossRef]
- Banchhor, S.K.; Londhe, N.D.; Araki, T.; Saba, L.; Radeva, P.; Laird, J.R.; Suri, J.S. Wall-based measurement features provides an improved IVUS coronary artery risk assessment when fused with plaque texture-based features during machine learning paradigm. Comput. Biol. Med. 2017, 91, 198–212. [Google Scholar] [CrossRef]
- Cao, Y.; Xiao, X.; Liu, Z.; Yang, M.; Sun, D.; Guo, W.; Cui, L.; Zhang, P. Detecting vulnerable plaque with vulnerability index based on convolutional neural networks. Comput. Med. Imaging Graph. Off. J. Comput. Med. Imaging Soc. 2020, 81, 101711. [Google Scholar] [CrossRef]
- Zhang, L.; Wahle, A.; Chen, Z.; Lopez, J.J.; Kovarnik, T.; Sonka, M. Predicting Locations of High-Risk Plaques in Coronary Arteries in Patients Receiving Statin Therapy. IEEE Trans. Med. Imaging 2018, 37, 151–161. [Google Scholar] [CrossRef]
- van Assen, M.; Varga-Szemes, A.; Schoepf, U.J.; Duguay, T.M.; Hudson, H.T.; Egorova, S.; Johnson, K.; Pierre, S.S.; Zaki, B.; Oudkerk, M.; et al. Automated plaque analysis for the prognostication of major adverse cardiac events. Eur. J. Radiol. 2019, 116, 76–83. [Google Scholar] [CrossRef]
- van Rosendael, A.R.; Maliakal, G.; Kolli, K.K.; Beecy, A.; Al’Aref, S.J.; Dwivedi, A.; Singh, G.; Panday, M.; Kumar, A.; Ma, X.; et al. Maximization of the usage of coronary CTA derived plaque information using a machine learning based algorithm to improve risk stratification; insights from the CONFIRM registry. J. Cardiovasc. Comput. Tomogr. 2018, 12, 204–209. [Google Scholar] [CrossRef] [PubMed]
- Johnson, K.M.; Johnson, H.E.; Zhao, Y.; Dowe, D.A.; Staib, L.H. Scoring of Coronary Artery Disease Characteristics on Coronary CT Angiograms by Using Machine Learning. Radiology 2019, 292, 354–362. [Google Scholar] [CrossRef] [PubMed]
- Motwani, M.; Dey, D.; Berman, D.S.; Germano, G.; Achenbach, S.; Al-Mallah, M.; Andreini, D.; Budoff, M.J.; Cademartiri, F.; Callister, T.Q.; et al. Machine learning for prediction of all-cause mortality in patients with suspected coronary artery disease: A 5-year multicentre prospective registry analysis. Eur. Heart J. 2017, 38, 500–507. [Google Scholar] [CrossRef] [PubMed]
- Han, D.; Kolli, K.K.; Al’Aref, S.J.; Baskaran, L.; van Rosendael, A.R.; Gransar, H.; Andreini, D.; Budoff, M.J.; Cademartiri, F.; Chinnaiyan, K.; et al. Machine Learning Framework to Identify Individuals at Risk of Rapid Progression of Coronary Atherosclerosis: From the PARADIGM Registry. J. Am. Heart Assoc. 2020, 9, e013958. [Google Scholar] [CrossRef]
- Kigka, V.I.; Sakellarios, A.I.; Tsompou, P.; Kyriakidis, S.; Siogkas, P.; Andrikos, I.; Michalis, L.K.; Fotiadis, D.I. Site specific prediction of atherosclerotic plaque progression using computational biomechanics and machine learning. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 6998–7001. [Google Scholar] [CrossRef]
- Falk, E.; Nakano, M.; Bentzon, J.F.; Finn, A.V.; Virmani, R. Update on acute coronary syndromes: The pathologists’ view. Eur. Heart J. 2013, 34, 719–728. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Authors | Vascular Segments | Year | The Method Applied | Outcomes | Advantages | Disadvantages |
|---|---|---|---|---|---|---|
| Athanasiou | Plaques | 2011 | OCT | Random forest (RF), accuracy of 80.41% | Random forest (RF) classifier to classify atherosclerotic plaques (calcium, lipid pools, fibrous tissue, and mixed plaques) | Invasive |
| Wang | Vulnerable plaques | 2012 | Fibrous cap (FC) | Proposed a computer-aided method for quantification of fibrous cap (FC) thickness to indicate vulnerable plaques | A method for quantification of fibrous cap (FC) thickness | Invasive |
| Sheet D | Coronary plaque | 2013 | IVUS | Validation analysis revealed that SDH is highly consistent with traditional histology in characterizing calcification, fibrotic tissues, and lipids, with 99%, 97%, 99% accuracy, respectively | Developed a novel machine-learning-based technique called Stochastic Driven Histology (SDH), which can automatically characterize image components in IVUS images | Invasive, the small number of observation |
| Ughi | Plaques | 2013 | OCT | Random forest (RF), accuracy of 81.5%% | Random forest (RF) classifier to classify atherosclerotic plaques (calcium, lipid pools, fibrous tissue, and mixed plaques) | Invasive |
| Yamak D | Coronary plaque | 2014 | Non-calcified coronary atherosclerotic plaque. Characterization by Dual Energy Computed Tomography | Learning approaches were explored as a more advanced mathematical analysis to use additional information provided by DECT | Three models (ANN, RF and SVM) | The small number of observations is the other limitation of this study |
| Xu M | Atherosclerotic heart disease | 2014 | OCT | A linear SVM classifier to detect unhealthy objects | The system classifies the image from healthy and unhealthy subjects automatically by utilizing texture features | Invasive |
| Gaur | Coronary | 2016 | Coronary CTA stenosis, plaque volumes, FFRCT, and FFR were assessed | Redictive ability of local ischemia was 0.90 | Coronary atherosclerotic plaque and FFRCT assessment improve the discrimination of ischaemia | Did not confirm plaque findings by intravascular ultrasound |
| Shalev R | Coronary plaque | 2016 | OCT | Rained and validated the model using frozen microscopic data, and the accuracy of calcified plaque recognition achieved 0.97 | Regions for extraction of sub-images (SI’s) were selected by experts to include calcium, fibrous, or lipid tissues | Invasive |
| Rico-Jimenez | Aining plaques | 2016 | OCT | An A-line modeling method to characterize plaques in OCT, which can automatically identify fibrotic plaques and lipid-containing plaques with 85% accuracy | Automatically identify fibrotic plaques and lipid-containing plaques | Invasive |
| Kolossváry M | Coronary vulnerable plaques | 2017 | Features are superior to conventional quantitative computed tomographic metrics to identify coronary plaques with napkin-ring sign | Radiomics and found that 916 features (20.6%) were associated with napkin-ring sign (NRS), of which 440 (9.9%) multiple radiographic features (short-run low-gray-level emphasis, long-run low-gray-level emphasis | High-risk plaques, napkin-ring sign | The true prevalence of the NRS is considerably smaller compared with non-NRS plaques in a real population |
| Kim G | Coronary plaque | 2018 | Plaque components were classifed into FT, FFT, NC, or DC using an intensity-based multi-level classifcation model | The classifers had classifcation accuracies of 85.1%, 71.9%, and 77.2%, respectively | Three diferent nets. Net 1 diferentiated low-intensity components into FT/FFT and NC/DC groups. Then, net 2 subsequently divided FT/FFT into FT or FFT, NC or DC via net 3 | Invasive, it did not acquire signifcant classifcation results compared with VH |
| Kolluru | Classify plaques in OCT | 2018 | OCT | The model achieved an accuracy value that exceeded 90% in all categories. | Model also trained on frozen images to classify plaques in OCT into four categories, fiber, lipid, calcium, and others | Invasive |
| Wilson | Plaques | 2018 | OCT | Convolutional neural network (CNN) in identifying plaque properties in OCT images using line-based modeling methods, learning that CNN can significantly outperform in this task | A method based on the SegNet deep learning network | Invasive |
| Zreik M | Coronary artery plaque | 2019 | A recurrent CNN for automatic detection and classification of coronary crtery plaque and stenosis in coronary CT angiography | For detection and characterization of coronary plaque, the method was achieved an accuracy of 0.77 | Three-dimensional convolutional neural network and neural networkautomatic detection and classification of coronary artery plaque and stenosis are feasible | Coronary artery bifurcations were not manually annotated and the network was not trained to detect these as a separate class |
| Rajendra | Coronary artery plaque | 2019 | Seven features are extracted from the Gabor coefficients: energy, and Kapur, Max, Rényi, Shannon, Vajda, and Yager entropies | The features acquired were also ranked according to F-value and input to several classifiers, an accuracy, positive predictive value, sensitivity, and specificity of 89.09%, 91.70%, 91.83% and 83.70% were obtained | Automated plaque classification using computed tomography angiography and Gabor transformationscan be helpful in the automated classification of plaques present in CTA images | The database was limited to only 73 patients. Furthermore, no quantitative calcium score was calculated |
| Masuda T | Coronary artery plaque | 2019 | Recorded the coronary CT number and 7 histogram parameters (minimum and mean value, standard deviation (SD), maximum value, skewness, kurtosis, and entropy) of the plaque CT number | Coronary CT number (0.19) followed by the minimum value (0.17), kurtosis (0.17), entropy (0.14), skewness (0.11), the mean value (0.11), the standard deviation (0.06), and the maximum value (0.05), and energy (0.00) | The machine learning was superior the conventional cut-off method for coronary plaque characterization using the plaque CT number on CCTA images | A small single-protocol study and only the performance of the machine learning algorithm was evaluated |
| Kolossváry M. | Coronary vulnerable plaques | 2019 | Diagnosis of advanced atherosclerotic lesions on 333 cross-sections of 95 plaques and evaluation of an additional 112 cross-sections | The results showed that the model was superior to several traditional methods. | Radiomics-based ML models outperformed expert visual assessment and histogram-based methods in the identification of advanced atheroscle radiomics-based machine learning rotic lesion | Limited spatial resolution of coronary CT angiography |
| Kolossváry M. | Coronaryvuinerable plaques | 2019 | Radiomics outperformed traditional CTA parameters in detecting IVUS low-attenuating plaques, OCT validated thin-cap fibroatheroma (TVFA) and naf18-pet | CTA, IVUS, OCT, positive lesions (AUC: 0.59 vs. 0.72, 0.66 vs. 0.80, 0.65 vs. 0.87) | Coronary CTA radiomics showed a good diagnostic accuracy to identify IVUS-attenuated plaques and excellent diagnostic accuracy to identify OCT-TCFA | Our results of the general populations are limited, multicenter longitudinal studies are warranted |
| von Knebel | Coronary | 2019 | ICA, CT-FFR | Redictive ability of local ischemia was 0.93 | CCTA-derived plaque markers and CT-FFR have discriminatory power to differentiate between hemodynamically significant and non-significant coronary lesions | Did not systematically correlate our findings on CCTA with an invasive reference standard |
| Kawasaki | Coronary | 2019 | CT-FFR | rRdictive ability of local ischemia was 0.835 | CCTA features and functional CT-FFR was helpful for detecting lesion-specific ischemia | Did not evaluate the influence of CT image quality on the CT-FFR measurements |
| Liu | Vulnerable plaques | 2019 | IVOCT images based on a deep convolutional neural network (DCNN) | Automatic detection system of vulnerable plaque for IVOCT images based on a deep convolutional neural network (DCNN). The accuracy of the system reached 88.84% | Intravascular optical coherence tomography (IVOCT) | Invasive |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, J.; Han, R.; Shao, G.; Lv, B.; Sun, K. Artificial Intelligence in Cardiovascular Atherosclerosis Imaging. J. Pers. Med. 2022, 12, 420. https://doi.org/10.3390/jpm12030420
Zhang J, Han R, Shao G, Lv B, Sun K. Artificial Intelligence in Cardiovascular Atherosclerosis Imaging. Journal of Personalized Medicine. 2022; 12(3):420. https://doi.org/10.3390/jpm12030420
Chicago/Turabian StyleZhang, Jia, Ruijuan Han, Guo Shao, Bin Lv, and Kai Sun. 2022. "Artificial Intelligence in Cardiovascular Atherosclerosis Imaging" Journal of Personalized Medicine 12, no. 3: 420. https://doi.org/10.3390/jpm12030420