
4-Hydroxyphenyllactic Acid in Cerebrospinal Fluid as a Possible Marker of Post-Neurosurgical Meningitis: Retrospective Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Biological Samples
2.2. Patients
- -
- Information on proved or suspected bacterial meningitis in the medical records according to the clinical signs;
- -
- Positive bacterial CSF culture;
- -
- CSF leukocyte count more than 300 cells/mm3 with the relative number of neutrophils more than 80%.
- -
- Glucose level less than 2.7 mmol/L;
- -
- Lactate level more than 4 mmol/L;
- -
- Protein level more than 1 g/L.
- -
- Hyperthermia/hypothermia;
- -
- The presence of the draining devices.
2.3. Statistical Analysis
3. Results
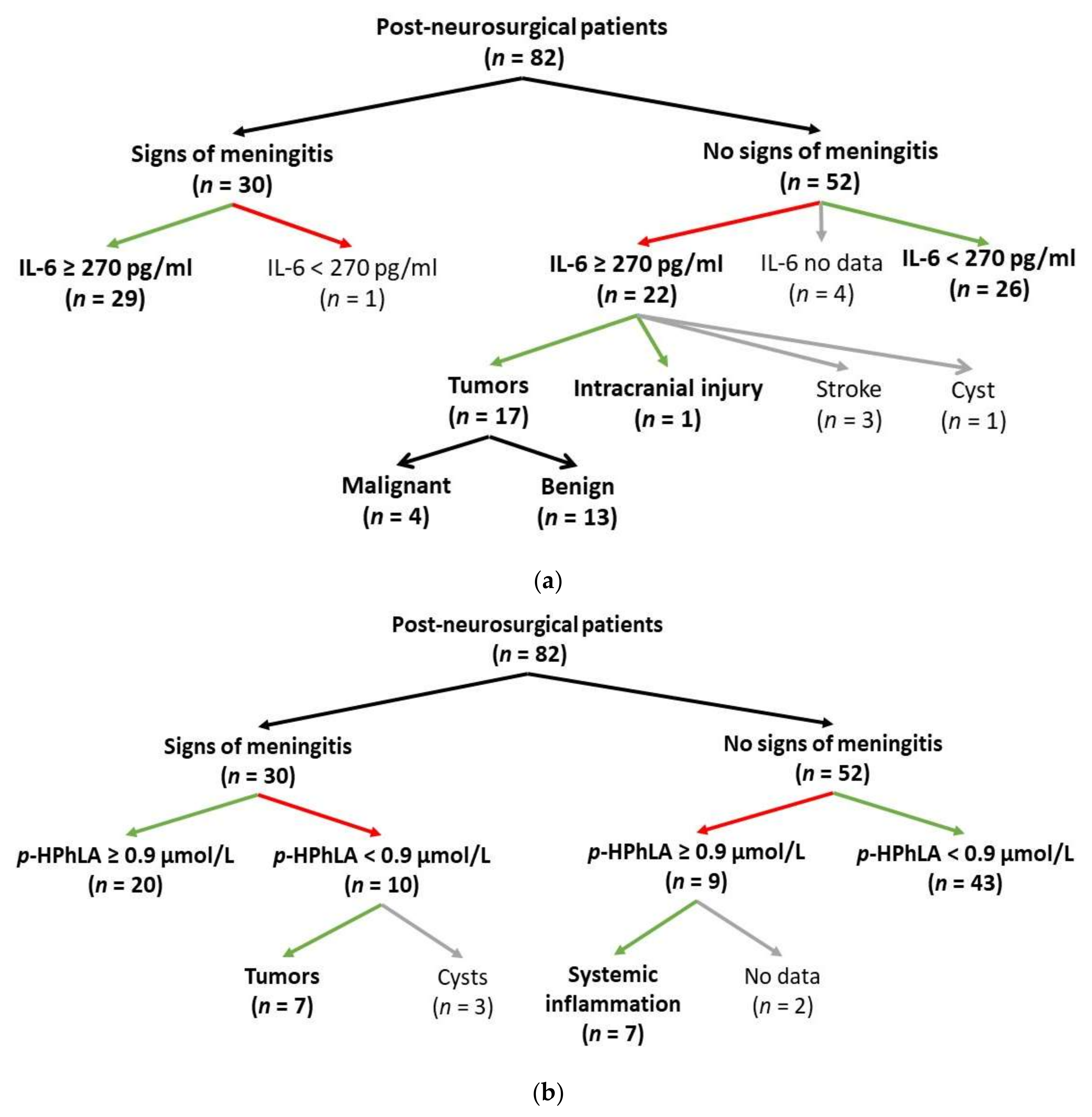
3.1. Characteristics of the Patients with Signs of Post-Neurosurgical Meningitis
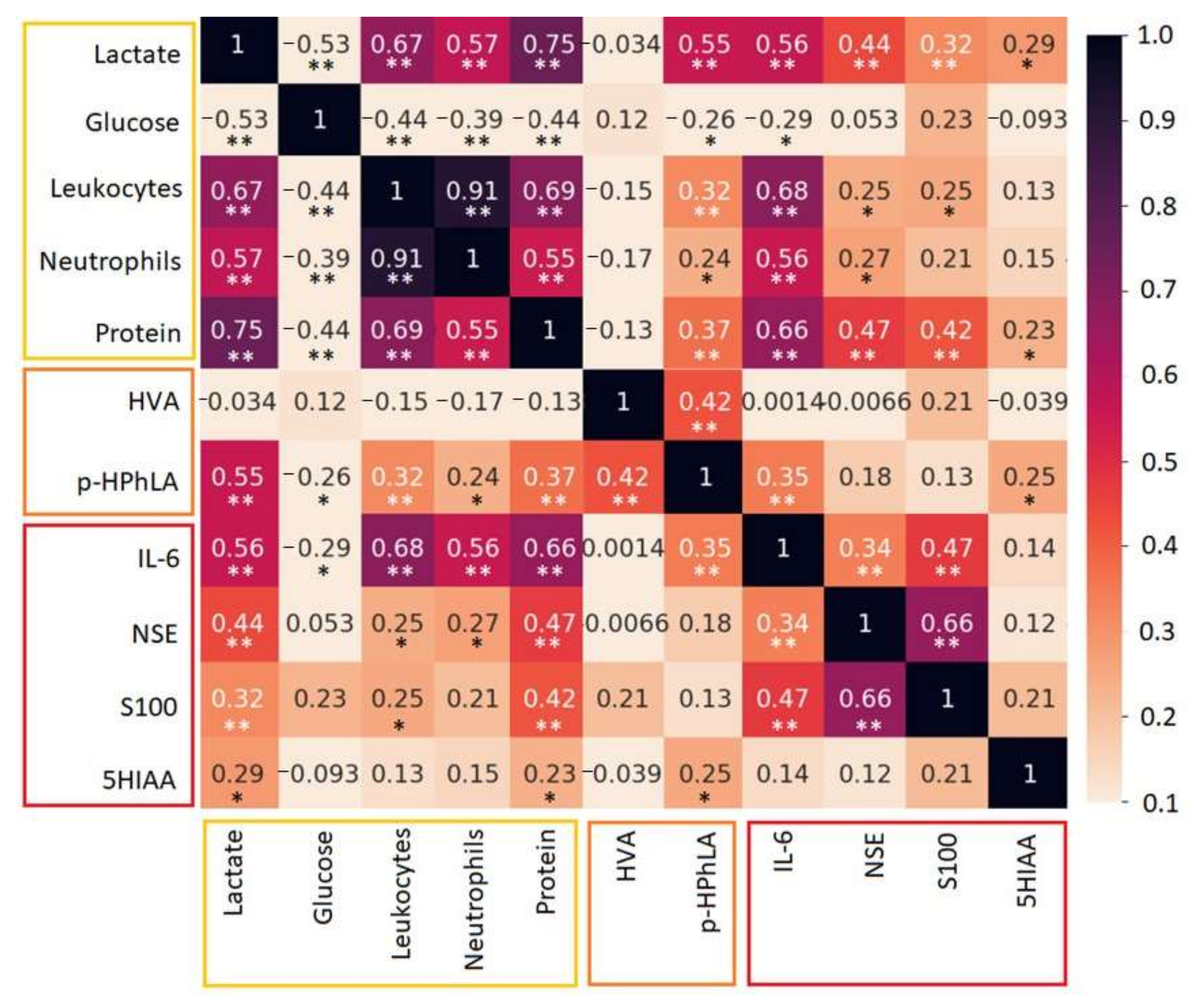
3.2. Aromatic Metabolites and Biomarkers in the CSF
4. Discussion
4.1. Biomarkers
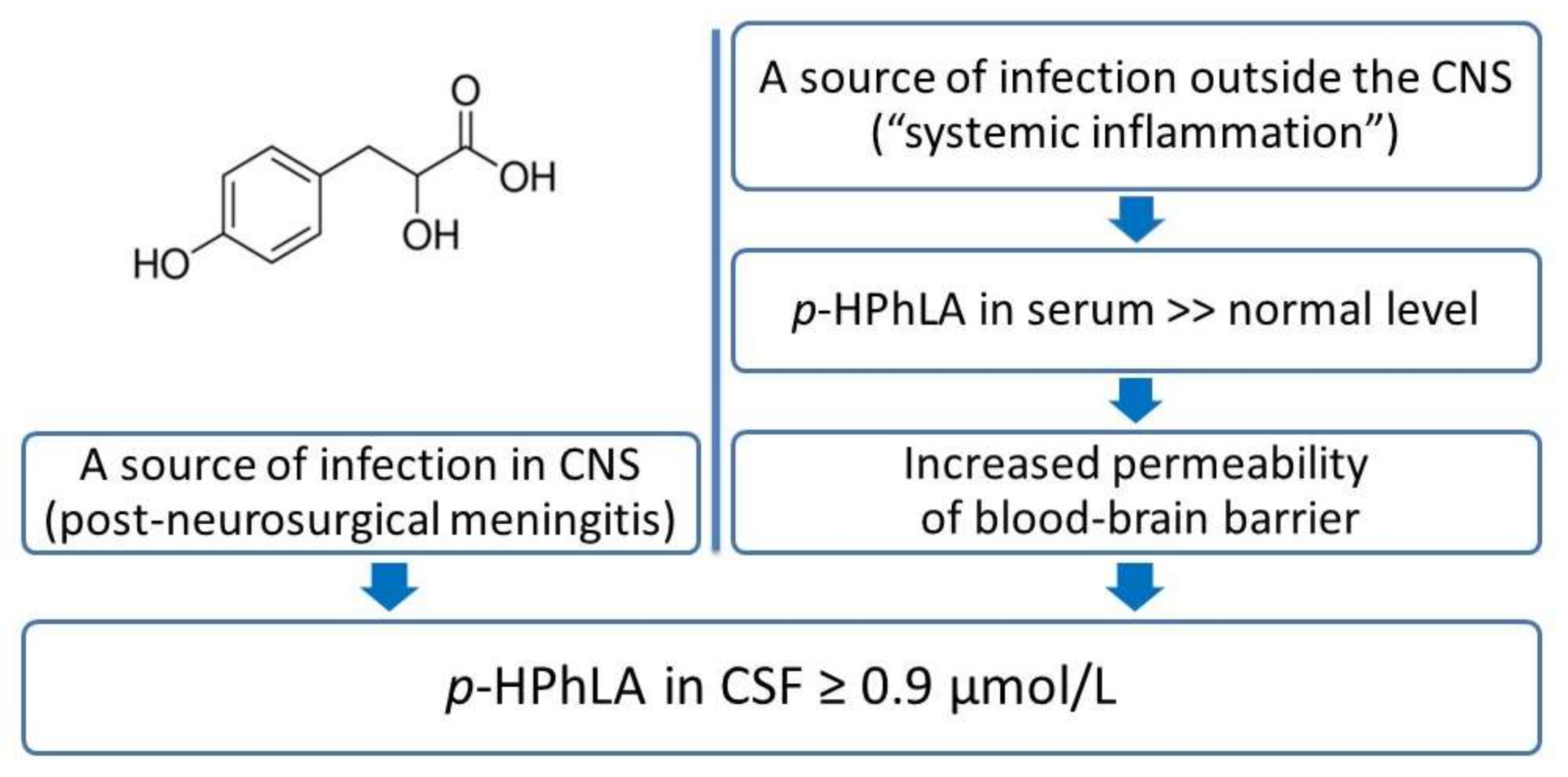
4.2. Aromatic Metabolites
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Van de Beek, D.; Drake, J.M.; Tunkel, A.R. Nosocomial Bacterial Meningitis. N. Engl. J. Med. 2010, 362, 146–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hussein, K.; Bitterman, R.; Shofty, B.; Paul, M.; Neuberger, A. Management of post-neurosurgical meningitis: Narrative review. Clin. Microbiol. Infect. 2017, 23, 621–628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tunkel, A.R.; Hartman, B.J.; Kaplan, S.L.; Kaufman, B.A.; Roos, K.L.; Scheld, W.M.; Whitley, R.J. Practice Guidelines for the Management of Bacterial Meningitis. Clin. Infect. Dis. 2004, 39, 1267–1284. [Google Scholar] [CrossRef] [PubMed]
- Tunkel, A.R.; Hasbun, R.; Bhimraj, A.; Byers, K.; Kaplan, S.L.; Scheld, W.M.; van de Beek, D.; Bleck, T.P.; Garton, H.J.; Zunt, J.R. 2017 Infectious Diseases Society of America’s Clinical Practice Guidelines for Healthcare-Associated Ventriculitis and Meningitis. Clin. Infect. Dis. 2017, 64, e34–e65. [Google Scholar] [CrossRef] [PubMed]
- Conen, A.; Walti, L.N.; Merlo, A.; Fluckiger, U.; Battegay, M.; Trampuz, A. Characteristics and Treatment Outcome of Cerebrospinal Fluid Shunt–Associated Infections in Adults: A Retrospective Analysis over an 11-Year Period. Clin. Infect. Dis. 2008, 47, 73–82. [Google Scholar] [CrossRef]
- Maskin, L.P.; Capparelli, F.; Mora, A.; Hlavnicka, A.; Orellana, N.; Díaz, M.F.; Wainsztein, N.; del Castillo, M. Cerebrospinal fluid lactate in post-neurosurgical bacterial meningitis diagnosis. Clin. Neurol. Neurosurg. 2013, 115, 1820–1825. [Google Scholar] [CrossRef]
- Alons, I.M.E.; Verheul, R.J.; Kuipers, I.; Jellema, K.; Wermer, M.J.H.; Algra, A.; Ponjee, G. Procalcitonin in cerebrospinal fluid in meningitis: A prospective diagnostic study. Brain Behav. 2016, 6, e00545. [Google Scholar] [CrossRef] [Green Version]
- Hirano, T. IL-6 in inflammation, autoimmunity and cancer. Int. Immunol. 2021, 33, 127–148. [Google Scholar] [CrossRef]
- Lee, D.; Cho, Y.; Ko, Y.; Heo, N.H.; Kang, H.G.; Han, S. Neuron-specific enolase level as a predictor of neurological outcome in near-hanging patients: A retrospective multicenter study. PLoS ONE 2021, 16, e0246898. [Google Scholar] [CrossRef]
- Janigro, D.; Bailey, D.M.; Lehmann, S.; Badaut, J.; O’Flynn, R.; Hirtz, C.; Marchi, N. Peripheral Blood and Salivary Biomarkers of Blood–Brain Barrier Permeability and Neuronal Damage: Clinical and Applied Concepts. Front. Neurol. 2021, 11, 577312. [Google Scholar] [CrossRef]
- Al-Mekhlafi, A.; Sühs, K.-W.; Schuchardt, S.; Kuhn, M.; Müller-Vahl, K.; Trebst, C.; Skripuletz, T.; Klawonn, F.; Stangel, M.; Pessler, F. Elevated Free Phosphatidylcholine Levels in Cerebrospinal Fluid Distinguish Bacterial from Viral CNS Infections. Cells 2021, 10, 1115. [Google Scholar] [CrossRef] [PubMed]
- Kozar, M.P.; Krahmer, M.T.; Fox, A.; Gray, B.M. Failure to Detect Muramic Acid in Normal Rat Tissues but Detection in Cerebrospinal Fluids from Patients with Pneumococcal Meningitis. Infect. Immun. 2000, 68, 4688–4698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beloborodova, N.; Pautova, A.; Sergeev, A.; Fedotcheva, N. Serum Levels of Mitochondrial and Microbial Metabolites Reflect Mitochondrial Dysfunction in Different Stages of Sepsis. Metabolites 2019, 9, 196. [Google Scholar] [CrossRef] [Green Version]
- Beloborodova, N.; Sarshor, Y.N.; Bedova, A.Y.; Chernevskaya, E.; Pautova, A.K. Involvement of Aromatic Metabolites in the Pathogenesis of Septic Shock. Shock 2018, 50, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Moroz, V.V.; Beloborodova, N.V.; Osipov, A.A.; Vlasenko, A.V.; Bedova, A.Y.; Pautova, A.K. Phenylcarboxylic acids in the assessment of the severity of patient condition and the efficiency of intensive treatment in critical care medicine. Obs. Reanimatol. 2016, 12, 37–48. [Google Scholar] [CrossRef] [Green Version]
- Chernevskaya, E.; Beloborodova, N.; Klimenko, N.; Pautova, A.; Shilkin, D.; Gusarov, V.; Tyakht, A. Serum and fecal profiles of aromatic microbial metabolites reflect gut microbiota disruption in critically ill patients: A prospective observational pilot study. Crit. Care 2020, 24, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Chernevskaya, E.; Klimenko, N.; Pautova, A.; Buyakova, I.; Tyakht, A.; Beloborodova, N. Host-Microbiome Interactions Mediated by Phenolic Metabolites in Chronically Critically Ill Patients. Metabolites 2021, 11, 122. [Google Scholar] [CrossRef]
- Beloborodov, N.V.; Khodakova, A.S.; Bairamov, I.T.; Olenin, A.Y. Microbial origin of phenylcarboxylic acids in the human body. Biochemistry 2009, 74, 1350–1355. [Google Scholar] [CrossRef]
- Pautova, A.K.; Khesina, Z.B.; Litvinova, T.N.; Revelsky, A.I.; Beloborodova, N.V. Metabolic profiling of aromatic compounds in cerebrospinal fluid of neurosurgical patients using microextraction by packed sorbent and liquid–liquid extraction with gas chromatography–mass spectrometry analysis. Biomed. Chromatogr. 2021, 35, 1–11. [Google Scholar] [CrossRef]
- Obrenovich, M.E.; Donskey, C.J.; Schiefer, I.T.; Bongiovanni, R.; Li, L.; Jaskiw, G.E. Quantification of phenolic acid metabolites in humans by LC–MS: A structural and targeted metabolomics approach. Bioanalysis 2018, 10, 1591–1608. [Google Scholar] [CrossRef]
- Mandrekar, J.N. Receiver Operating Characteristic Curve in Diagnostic Test Assessment. J. Thorac. Oncol. 2010, 5, 1315–1316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mukaka, M.M. Statistics corner: A guide to appropriate use of correlation coefficient in medical research. Malawi Med. J. 2012, 24, 69–71. [Google Scholar] [PubMed]
- Nguyen, D.P.; Li, J.; Tewari, A.K. Inflammation and prostate cancer: The role of interleukin 6 (IL-6). Br. J. Urol. 2014, 113, 986–992. [Google Scholar] [CrossRef] [PubMed]
- Tyrrell, D.J.; Goldstein, D.R. Ageing and atherosclerosis: Vascular intrinsic and extrinsic factors and potential role of IL-6. Nat. Rev. Cardiol. 2021, 18, 58–68. [Google Scholar] [CrossRef]
- Smok, B.; Domagalski, K.; Pawłowska, M. Diagnostic and Prognostic Value of IL-6 and sTREM-1 in SIRS and Sepsis in Children. Mediat. Inflamm. 2020, 2020, 1–8. [Google Scholar] [CrossRef]
- Gruol, D.L.; Nelson, T.E. Physiological and pathological roles of interleukin-6 in the central nervous system. Mol. Neurobiol. 1997, 15, 307–339. [Google Scholar] [CrossRef]
- Baker, D.G.; Ekhator, N.N.; Kasckow, J.W.; Hill, K.K.; Zoumakis, E.; Dashevsky, B.A.; Chrousos, G.P.; Geracioti, T.D., Jr. Plasma and Cerebrospinal Fluid Interleukin-6 Concentrations in Posttraumatic Stress Disorder. Neuroimmunomodulation 2001, 9, 209–217. [Google Scholar] [CrossRef]
- Hopkins, S.J.; McMahon, C.J.; Singh, N.; Galea, J.; Hoadley, M.; Scarth, S.; Patel, H.; Vail, A.; Hulme, S.; Rothwell, N.J.; et al. Cerebrospinal fluid and plasma cytokines after subarachnoid haemorrhage: CSF interleukin-6 may be an early marker of infection. J. Neuroinflammation 2012, 9, 255. [Google Scholar] [CrossRef]
- Kestner, M.; Rosler, A.E.; Baumgärtner, M.; Lindner, A.; Orth, M. CSF interleukin 6—A useful biomarker of meningitis in adults? LaboratoriumsMedizin 2011, 35, 107–113. [Google Scholar] [CrossRef]
- Ridwan, S.; Grote, A.; Simon, M. Interleukin 6 in cerebrospinal fluid is a biomarker for delayed cerebral ischemia (DCI) related infarctions after aneurysmal subarachnoid hemorrhage. Sci. Rep. 2021, 11, 1–10. [Google Scholar] [CrossRef]
- Schoch, B.; Regel, J.P.; Nierhaus, A.; Wichert, M.; Mueller, O.M.; Sandalcioglu, I.E.; Mann, K.; Stolke, D. Predictive Value of Intrathecal Interleukin-6 for Ventriculostomy-related Infection. Zent. Neurochir. 2008, 69, 80–86. [Google Scholar] [CrossRef]
- Kępa, L.; Oczko-Grzesik, B.; Stolarz, W.; Boroń-Kaczmarska, A. Cerebrospinal fluid ferritin concentration in patients with purulent, bacterial meningitis—Own observations. Przegl. Epidemiol. 2016, 70, 593–603. [Google Scholar] [PubMed]
- Lenski, M.; Biczok, A.; Neufischer, K.; Tonn, J.-C.; Briegel, J.; Thon, N. Significance of cerebrospinal fluid inflammatory markers for diagnosing external ventricular drain–associated ventriculitis in patients with severe traumatic brain injury. Neurosurg. Focus 2019, 47, E15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García-Hernández, P.; Prieto, B.; Martínez-Morillo, E.; Rodríguez, V.; Alvarez, F.V. Interleukin-6 in cerebrospinal fluid as a biomarker of acute meningitis. Ann. Clin. Biochem. 2016, 53, 155–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaplin, A.I.; Deshpande, D.M.; Scott, E.; Krishnan, C.; Carmen, J.S.; Shats, I.; Martinez, T.; Drummond, J.; Dike, S.; Pletnikov, M.; et al. IL-6 induces regionally selective spinal cord injury in patients with the neuroinflammatory disorder transverse myelitis. J. Clin. Investig. 2005, 115, 2731–2741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uzawa, A.; Mori, M.; Ito, M.; Uchida, T.; Hayakawa, S.; Masuda, S.; Kuwabara, S. Markedly increased CSF interleukin-6 levels in neuromyelitis optica, but not in multiple sclerosis. J. Neurol. 2009, 256, 2082–2084. [Google Scholar] [CrossRef] [PubMed]
- Shen, F.; Zhang, Y.; Yao, Y.; Hua, W.; Zhang, H.-S.; Wu, J.-S.; Zhong, P.; Zhou, L.-F. Proteomic analysis of cerebrospinal fluid: Toward the identification of biomarkers for gliomas. Neurosurg. Rev. 2014, 37, 367–380. [Google Scholar] [CrossRef]
- Hori, T.; Sasayama, T.; Tanaka, K.; Koma, Y.-I.; Nishihara, M.; Tanaka, H.; Nakamizo, S.; Nagashima, H.; Maeyama, M.; Fujita, Y.; et al. Tumor-associated macrophage related interleukin-6 in cerebrospinal fluid as a prognostic marker for glioblastoma. J. Clin. Neurosci. 2019, 68, 281–289. [Google Scholar] [CrossRef]
- El-Batata, M. Cytology of Cerebrospinal Fluid in the Diagnosis of Malignancy. J. Neurosurg. 1968, 28, 317–326. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.; Jia, H.; Yang, Y.; Dai, W.; Su, X.; Zhao, G. Cerebrospinal Fluid Cytology and Clinical Analysis of 34 Cases with Leptomeningeal Carcinomatosis. J. Int. Med Res. 2009, 37, 1913–1920. [Google Scholar] [CrossRef]
- Bönig, L.; Möhn, N.; Ahlbrecht, J.; Wurster, U.; Raab, P.; Puppe, W.; Sühs, K.-W.; Stangel, M.; Skripuletz, T.; Schwenkenbecher, P. Leptomeningeal Metastasis: The Role of Cerebrospinal Fluid Diagnostics. Front. Neurol. 2019, 10, 839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bi, X.; Zhao, D.; He, Q.; Liu, F.; Gong, L.; Li, H. Diagnosis of intracranial embryonal carcinoma by cerebrospinal fluid cytology: A case report. Int. J. Clin. Exp. Pathol. 2020, 13, 1216–1219. [Google Scholar] [PubMed]
- Pautova, A.K.; Bedova, A.Y.; Sarshor, Y.N.; Beloborodova, N. Determination of Aromatic Microbial Metabolites in Blood Serum by Gas Chromatography–Mass Spectrometry. J. Anal. Chem. 2018, 73, 160–166. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Patients with Signs of the Post-Neurosurgical Meningitis (n = 30) | Patients without Sufficient Signs of the Bacterial Meningitis (n = 52) |
|---|---|---|
| Sex, male/female | n = 18/n = 12 | n = 22/n = 30 |
| Primary diagnosis | benign tumor (n = 10) | benign tumor (n = 32) |
| malignant tumor (n = 10) | malignant tumor (n = 8) | |
| stroke (n = 1) | stroke (n = 7) | |
| intracranial injury (n = 3) | intracranial injury (n = 2) | |
| cyst (n = 3) | cyst (n = 1) | |
| hydrocephalus (n = 2) | hydrocephalus (n = 1) | |
| bacterial meningitis (n = 1) | bacterial meningitis (n = 1) 1 | |
| Non-survived patients | n = 2 | n = 1 |
| Proved/suspected bacterial meningitis as an infectious complication | n = 6/n = 2 | 0 |
| Positive bacterial CSF culture | n = 6 | 0 |
| CSF leukocyte count more/less/no data than 300 cells/mm3 | n = 25/n = 5/n = 0 | n = 4/n = 44/n = 4 |
| CSF relative number of the neutrophils more/less/no data than 80% | n = 26/n = 2/n = 2 | n = 9/n = 33/n = 10 |
| CSF glucose level more/less/no data than 2.7 mmol/L | n = 12/n = 17/n = 1 | n = 46/n = 4/n = 2 |
| CSF lactate level more/less/no data than 4 mmol/L | n = 18/n = 10/n = 2 | n = 5/n = 40/n = 7 |
| CSF protein level more/less/no data than 1.0 g/L | n = 25/n = 4/n = 1 | n = 18/n = 33/n = 1 |
| Draining devices | n = 12 | n = 13 |
| Hyperthermia | n = 9 | n = 3 |
| Parameter | Patients with Signs of Post-Neurosurgical Meningitis (n = 30) | Patients without Sufficient Signs of the Bacterial Meningitis (n = 52) | The Mann–Whitney U-Test, p-Value |
|---|---|---|---|
| Age, years | 34 [14.5–53], 0.7–67 | 33 [10–54], 2–91 | 0.365 |
| Leukocyte count, cells/mm3 | 936 [504–2688], 38–20488 | 17 [7–72], 1–672 | <0.0001 *** |
| Neutrophils, % | 96 [88–98], 33–100 | 23 [7–66], 1–100 | <0.0001 *** |
| Glucose, mmol/L | 2.2 [0.8–3.2], 0.2–5.2 | 3.3 [2.9–4.1], 1.7–7.9 | <0.0001 *** |
| Lactate, mmol/L | 4.9 [3.6–6.2], 2.9–9.4 | 2.0 [1.7–3.2], 1.4–6.5 | <0.0001 *** |
| Protein, g/L | 3.2 [1.2–3.9], 0.4–22.8 | 0.6 [0.3–1.5], 0.1–3.4 | <0.0001 *** |
| BA, µmol/L | 0.7 [0 *–0.8], 0 *–1.0 | 0.8 [0.7–1.0], 0 *–2.4 | 0.127 |
| HVA, µmol/L | 0 * [0 *–0 *], 0 *–1.5 | 0 * [0 *–0.5], 0 *–3.3 | 0.311 |
| p-HPhLA, µmol/L | 1.1 [0.5–1.6], 0 *–6.6 | 0.4 [0 *–0.7], 0 *–5 | 0.00019 *** |
| 5HIAA, ng/mL | 5 [3–7], 2–400 ** | 5 [3–6], 2–400 ** | 0.631 |
| IL-6, pg/mL | 2678 [600–5000 **], 163–5000 ** | 227 [33–1825], 7–5000 ** | 0.00002 *** |
| S100, µg/L | 2.9 [0.6–13.2], 0.1–39 ** | 3.5 [0.4–22.0], 0.2–39 ** | 0.788 |
| NSE, ng/mL | 5.9 [1.6–32.6], 0.2–2496 | 2.4 [1.4–8.8], 0.5–370 | 0.122 |
| Parameter | CSF Level of IL-6 | CSF Level of p-HPhLA | ||
|---|---|---|---|---|
| CNS Inflammation | Systemic Inflammation | |||
| Area | 0.785 | 0.734 | 0.698 | |
| Standard Error | 0.051 | 0.064 | 0.070 | |
| p-Value | 0.001 | 0.001 | 0.011 | |
| Asymptotic 95% CI | Lower Bound | 0.685 | 0.608 | 0.560 |
| Upper Bound | 0.886 | 0.860 | 0.836 | |
| Cut-Off Value | 270 pg/mL | 0.9 µmol/L | 0.9 µmol/L | |
| Sensitivity [95% CI], % | 96.30 [81.03–99.91] | 66.67 [47.19–82.71] | 48.39 [30.15–66.94] | |
| Specificity [95% CI], % | 54.17 [39.17–68.63] | 82.69 [69.67–91.77] | 76.00 [54.87–90.64] | |
| Positive Predictive Value [95% CI], % | 54.17 [46.28–61.85] | 68.97 [53.81–80.91] | 71.43 [53.24–84.59] | |
| Negative Predictive Value [95% CI], % | 96.30 [78.87–99.45] | 81.13 [71.83–87.88] | 54.29 [44.18–64.05] | |
| Accuracy [95% CI], % | 69.33 [57.62–79.47] | 76.83 [66.20–85.44] | 60.71 [46.75–73.50] | |
| Odds Ratio [95% CI] | 30.7 [3.9–245.1] | 9.6 [3.4–27.2] | 3.0 [0.9–9.4] | |
| Cut-Off Value | 270 pg/mL | 0.9 µmol/L | 0.9 µmol/L | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pautova, A.K.; Meglei, A.Y.; Chernevskaya, E.A.; Alexandrova, I.A.; Beloborodova, N.V. 4-Hydroxyphenyllactic Acid in Cerebrospinal Fluid as a Possible Marker of Post-Neurosurgical Meningitis: Retrospective Study. J. Pers. Med. 2022, 12, 399. https://doi.org/10.3390/jpm12030399
Pautova AK, Meglei AY, Chernevskaya EA, Alexandrova IA, Beloborodova NV. 4-Hydroxyphenyllactic Acid in Cerebrospinal Fluid as a Possible Marker of Post-Neurosurgical Meningitis: Retrospective Study. Journal of Personalized Medicine. 2022; 12(3):399. https://doi.org/10.3390/jpm12030399
Chicago/Turabian StylePautova, Alisa K., Anastasiia Yu. Meglei, Ekaterina A. Chernevskaya, Irina A. Alexandrova, and Natalia V. Beloborodova. 2022. "4-Hydroxyphenyllactic Acid in Cerebrospinal Fluid as a Possible Marker of Post-Neurosurgical Meningitis: Retrospective Study" Journal of Personalized Medicine 12, no. 3: 399. https://doi.org/10.3390/jpm12030399