
Traceable Features of Static Plantar Pressure Characteristics and Foot Postures in College Students with Hemiplegic Cerebral Palsy


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instruments and Equipment
2.3. Plantar Pressure Distribution Assessment Processes
- Assist the subject to roll both trouser legs above the knee in order to prevent the trouser legs from restricting the natural stance of the foot;
- Guide the subject to stand barefoot on the sensing pads with specific marks and the pressure sensing range platform of the JC Mat;
- Ask the subject to relax, control and balance their centers of gravity in a natural static posture. Stand still with feet shoulder-width apart and distribute body weight evenly on the feet;
- Ask the subject to stampede easily in place for six to eight steps, then stand still naturally with arms hanging down;
- Guide the subject to face the experimental instructor standing in front of the subject. Face the instructor directly in the eyes. Keep the body posture steady and balanced until there is no noticeable change in the measurement of foot pressure on the JC Mat.
2.4. Plantar Pressure Distribution Measurement
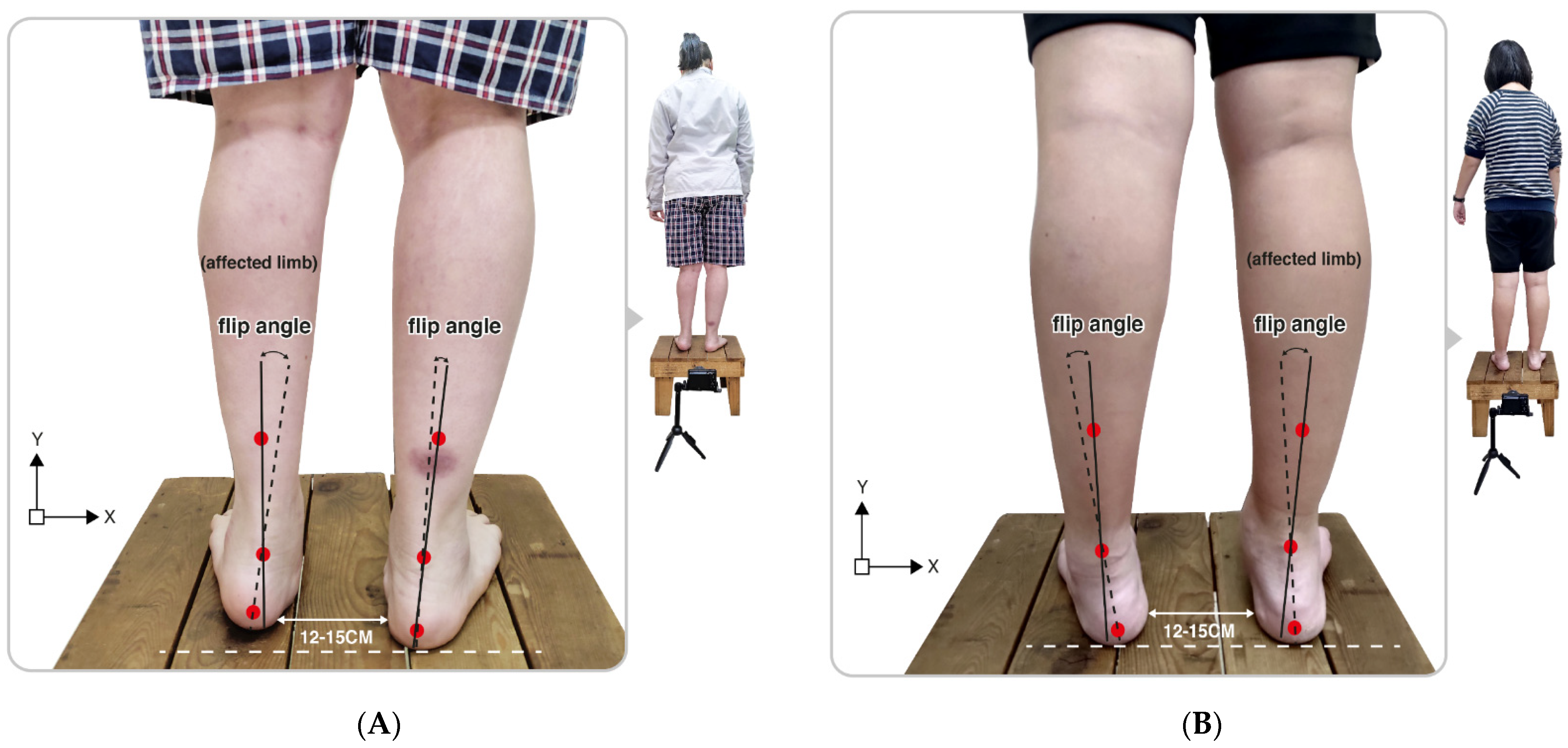
2.5. Rearfoot Postural Assessment Processes
2.6. Statistical Analysis
3. Results
3.1. Arch Index
3.2. Plantar Pressure Distribution of the Three Regions
3.3. Balance of the Centers of Gravity
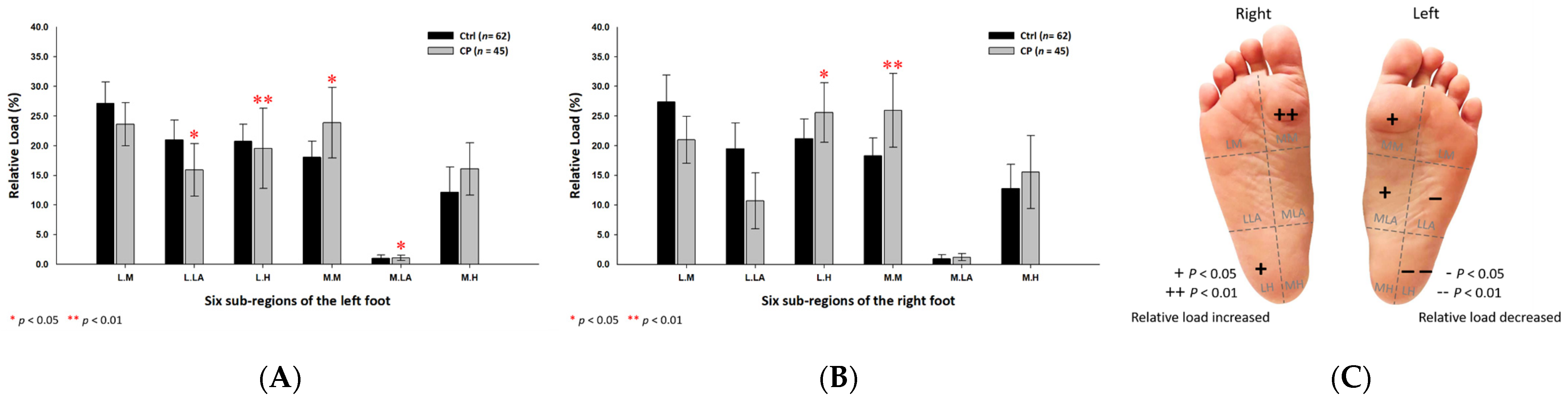
3.4. Plantar Pressure Distribution of the Six Subregions
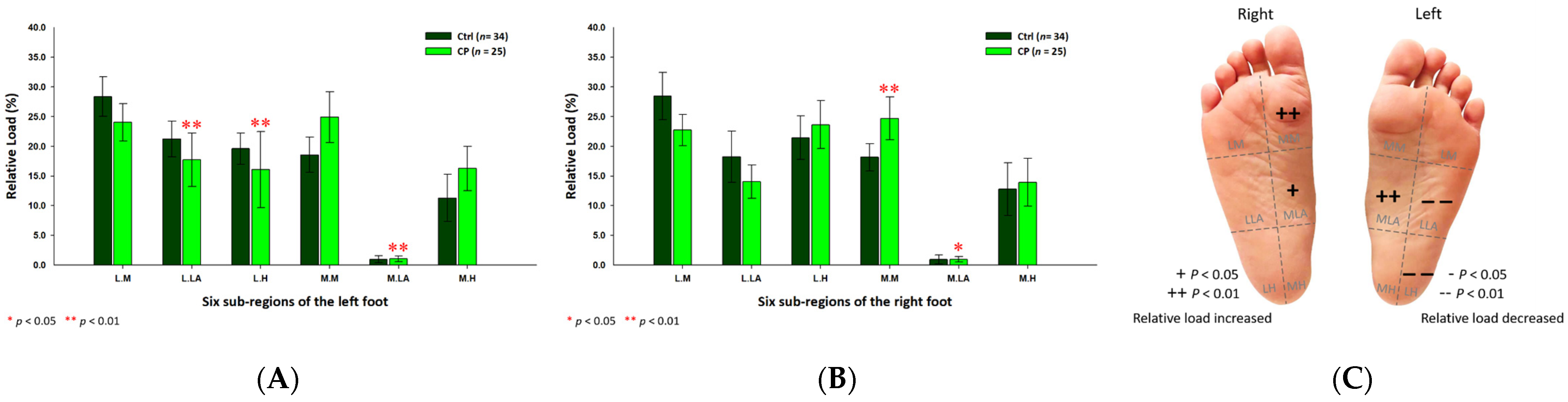
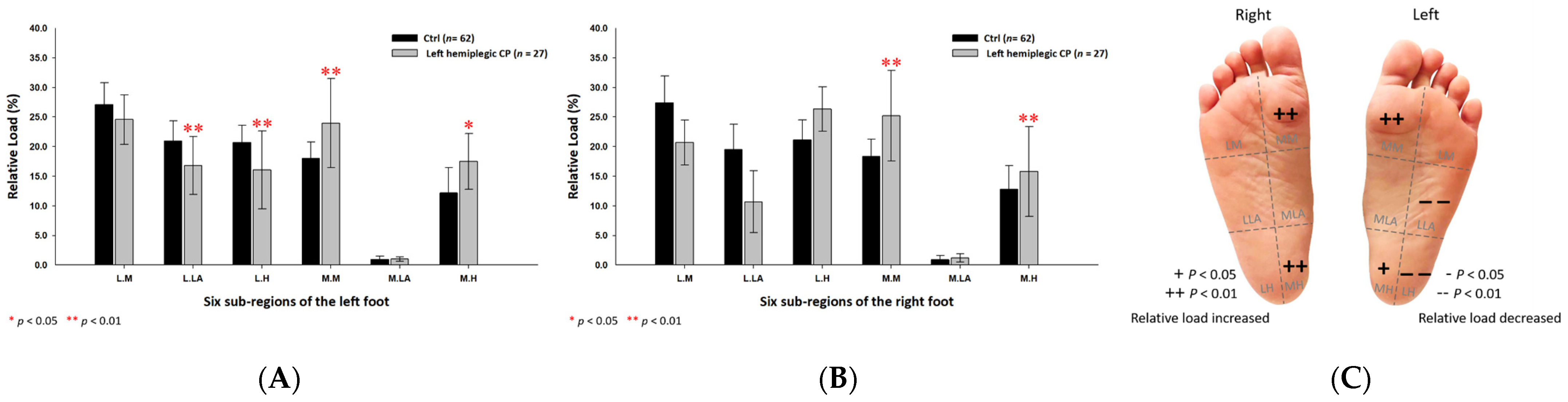
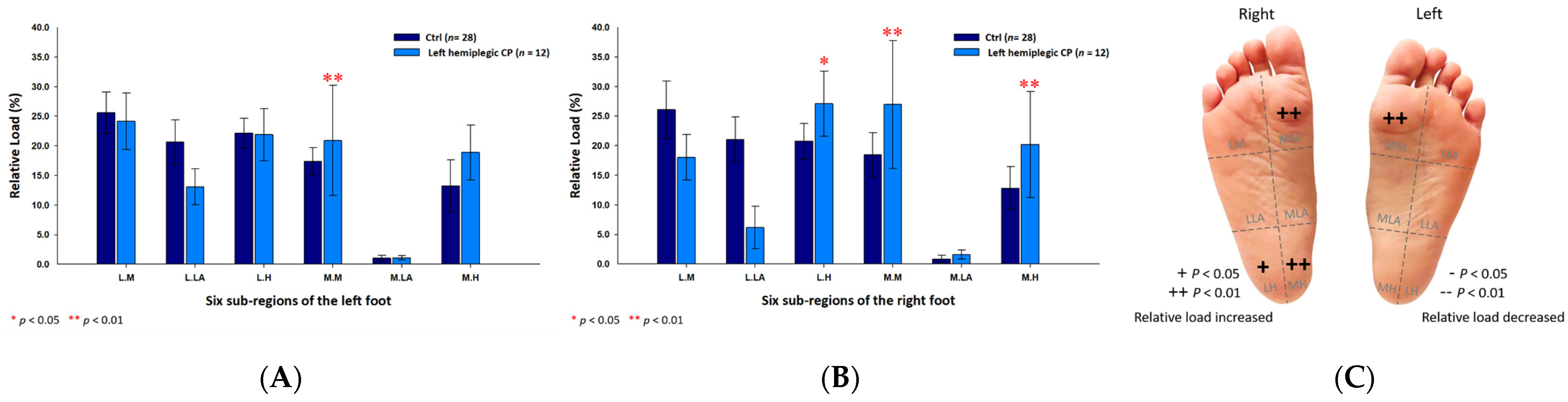
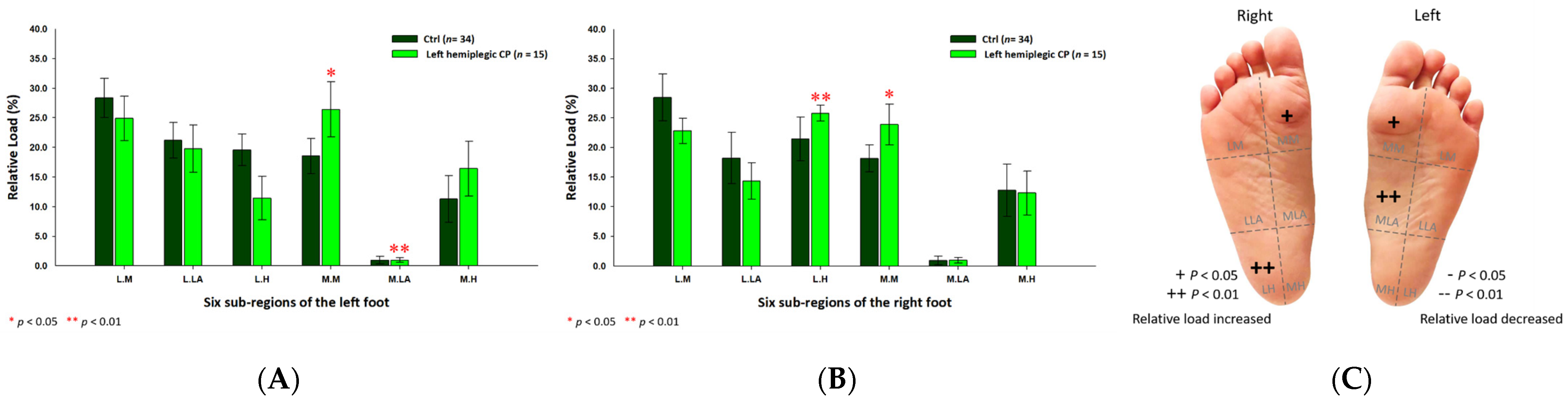
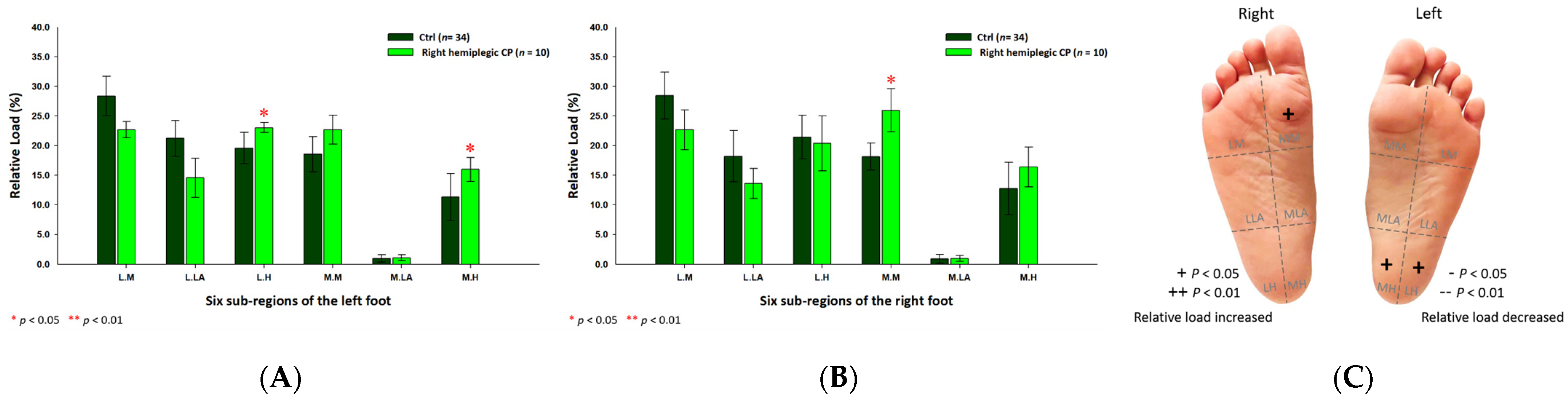
3.5. Plantar Pressure Distribution of the Six Subregions in the Left Hemiplegic CP Students
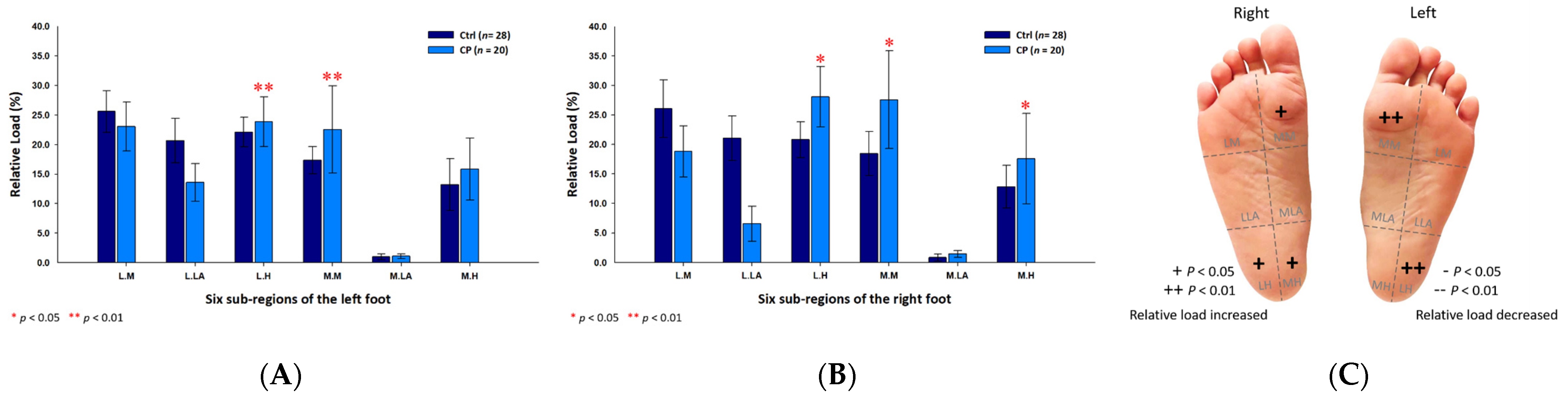
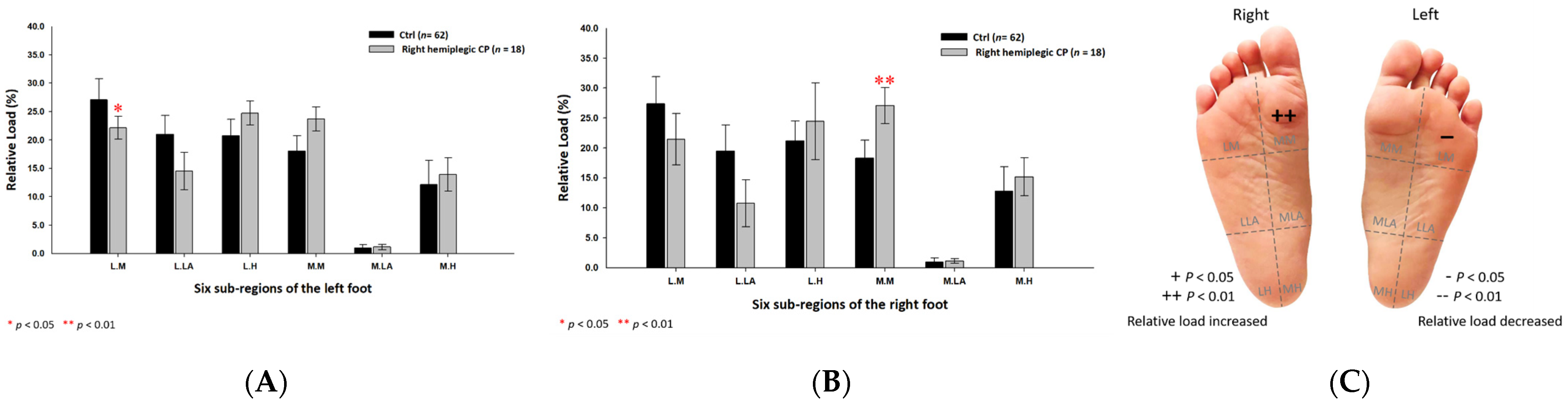
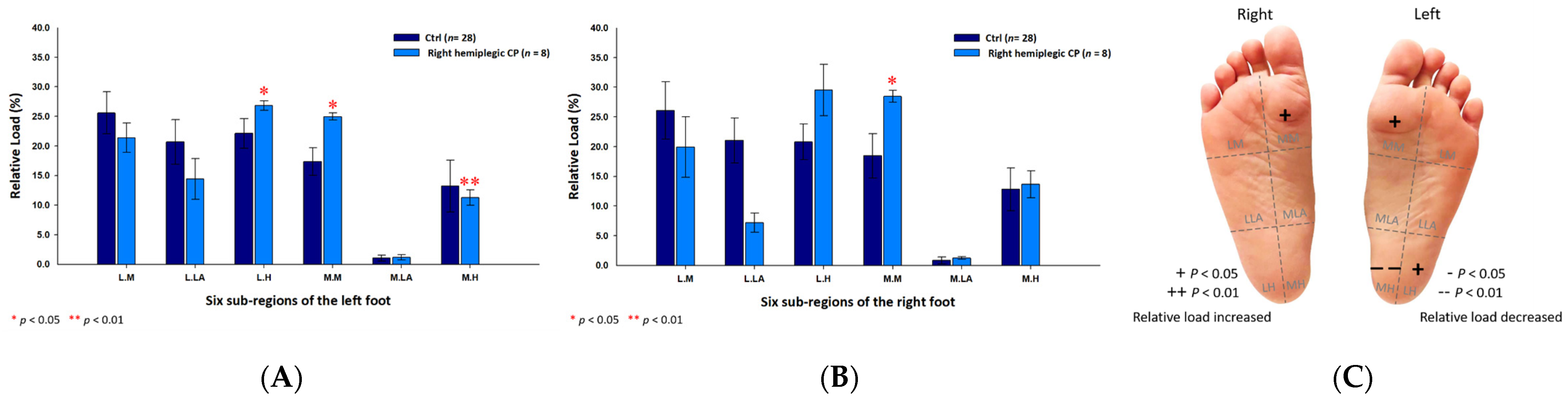
3.6. Plantar Pressure Distribution of the Six Subregions in the Right Hemiplegic CP Students
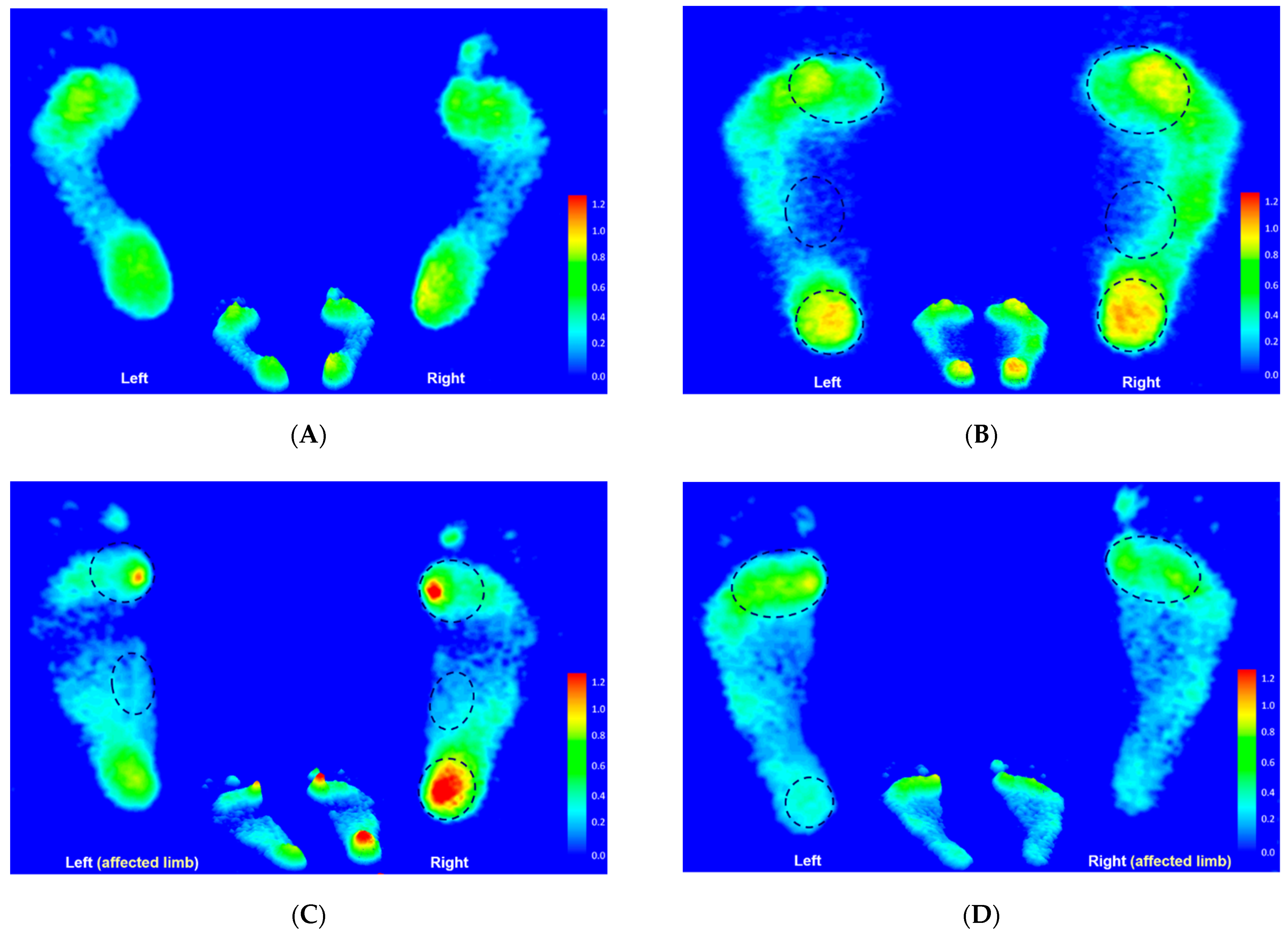
3.7. Footprint Image Characteristics
3.8. Rearfoot Postural Alignment
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Matusiak-Wieczorek, E.; Dziankowska-Zaborszczyk, E.; Synder, M.; Borowski, A. The influence of hippotherapy on the body posture in a sitting position among children with cerebral palsy. Int. J. Environ. Res. Public Health 2020, 17, 6846. [Google Scholar] [CrossRef]
- Pool, D.; Blackmore, A.M.; Bear, N.; Valentine, J. Effects of short-term daily community walk aide use on children with unilateral spastic cerebral palsy. Pediatric Phys. Ther. 2014, 26, 308–317. [Google Scholar] [CrossRef]
- Ricardo, D.; Raposo, M.R.; Cruz, E.B.; Oliveira, R.; Carnide, F.; Veloso, A.P.; João, F. Effects of ankle foot orthoses on the gait patterns in children with spastic bilateral cerebral palsy: A scoping review. Children 2021, 8, 903. [Google Scholar] [CrossRef]
- Chang, W.D.; Chang, N.J.; Lin, H.Y.; Lai, P.T. Changes of plantar pressure and gait parameters in children with mild cerebral palsy who used a customized external strap orthosis: A crossover study. BioMed Res. Int. 2015, 2015, 813942. [Google Scholar] [CrossRef] [Green Version]
- Bloom, T.; Sabharwal, S. Surgical management of foot and ankle deformities in cerebral palsy. Clin. Podiatr. Med. Surg. 2022, 39, 37–55. [Google Scholar] [CrossRef]
- Galli, M.; Cimolin, V.; Pau, M.; Leban, B.; Brunner, R.; Albertini, G. Foot pressure distribution in children with cerebral palsy while standing. Res. Dev. Disabil. 2015, 41, 52–57. [Google Scholar] [CrossRef]
- Otjen, J.; Menashe, S.J.; Maloney, E.; Iyer, R.S.; Ngo, A.V.; Sousa, T.C.; Thapa, M. Foot and ankle musculoskeletal imaging of pediatric patients with cerebral palsy. Am. J. Roentgenol. 2020, 214, 1389–1397. [Google Scholar] [CrossRef]
- Ferreira, L.A.; Cimolin, V.; Costici, P.F.; Albertini, G.; Oliveira, C.S.; Galli, M. Effects of gastrocnemius fascia lengthening on gait pattern in children with cerebral palsy using the gait profile score. Res. Dev. Disabil. 2014, 35, 1137–1143. [Google Scholar] [CrossRef]
- Saxena, S.; Rao, B.K.; Kumaran, S. Analysis of postural stability in children with cerebral palsy and children with typical development: An observational study. Pediatric Phys. Ther. 2014, 26, 325–330. [Google Scholar] [CrossRef]
- Zhang, C.; Pan, S.; Qi, Y.; Yang, Y. A Footprint extraction and recognition algorithm based on plantar pressure. Traitement Du Signal 2019, 36, 419–424. [Google Scholar] [CrossRef]
- Truong, P.H.; You, S.; Ji, S.H.; Jeong, G.M. Adaptive accumulation of plantar pressure for ambulatory activity recognition and pedestrian identification. Sensors 2021, 21, 3842. [Google Scholar] [CrossRef]
- Monteiro, R.L.; Sartor, C.D.; Ferreira, J.S.S.P.; Dantas, M.G.B.; Bus, S.A.; Sacco, I.C.N. Protocol for evaluating the effects of a foot-ankle therapeutic exercise program on daily activity, foot-ankle functionality, and biomechanics in people with diabetic polyneuropathy: A randomized controlled trial. BMC Musculoskelet. Disord. 2018, 19, 400. [Google Scholar] [CrossRef] [Green Version]
- Helili, M.; Geng, X.; Ma, X.; Chen, W.; Zhang, C.; Huang, J.; Wang, X. An investigation of regional plantar soft tissue hard-ness and its potential correlation with plantar pressure distribution in healthy adults. Appl. Bionics Biomech. 2021, 2021, 5566036. [Google Scholar] [CrossRef]
- Chuter, V.H.; Spink, M.J.; David, M.; Lanting, S.; Searle, A. Clinical foot measurements as a proxy for plantar pressure testing in people with diabetes. J. Foot Ankle Res. 2021, 14, 56. [Google Scholar] [CrossRef]
- Zhang, B.; Lu, Q. A current review of foot disorder and plantar pressure alternation in the elderly. Phys. Act. Health 2020, 4, 95–106. [Google Scholar] [CrossRef]
- Hollander, K.; Zech, A.; Rahlf, A.L.; Orendurff, M.S.; Stebbins, J.; Heidt, C. The relationship between static and dynamic foot posture and running biomechanics: A systematic review and meta-analysis. Gait Posture 2019, 72, 109–122. [Google Scholar] [CrossRef]
- Yoon, H.K.; Park, K.B.; Roh, J.Y.; Park, H.W.; Chi, H.J.; Kim, H.W. Extraarticular subtalar arthrodesis for pes planovalgus: An interim result of 50 feet in patients with spastic diplegia. Clin. Orthop. Surg. 2010, 2, 13–21. [Google Scholar] [CrossRef] [Green Version]
- Femery, V.; Moretto, P.; Renaut, H.; Lensel, G.; Thevenon, A. Asymmetries in dynamic plantar pressure distribution measurement in able-bodied gait: Application to the study of the gait asymmetries in children with hemiplegic cerebral palsy. Ann. Readapt Med. Phys. 2002, 45, 114–122. [Google Scholar] [CrossRef]
- Leunkeu, A.N.; Lelard, T.; Shephard, R.J.; Doutrellot, P.L.; Ahmaidi, S. Gait cycle and plantar pressure distribution in children with cerebral palsy: Clinically useful outcome measures for a management and rehabilitation. NeuroRehabilitation 2014, 35, 657–663. [Google Scholar] [CrossRef]
- Jiménez-Cebrián, A.M.; Roman-Bravo, P.D.; Morente-Bernal, M.F.; Alonso-Ríos, J.A.; De-la-Cruz-Torres, B.; Romero-Morales, C.; Navarro-Flores, E.; Montiel-Luque, A. Influence of childhood overweight and obesity on foot and lower limb pain in a population of primary school children. Arch. Med. Sci. 2020. [Google Scholar] [CrossRef]
- Brzeziński, M.; Czubek, Z.; Niedzielska, A.; Jankowski, M.; Kobus, T.; Ossowski, Z. Relationship between lower-extremity defects and body mass among polish children: A cross-sectional study. BMC Musculoskelet. Disord. 2019, 20, 84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yan, S.H.; Zhang, K.; Tan, G.Q.; Yang, J.; Liu, Z.C. Effects of obesity on dynamic plantar pressure distribution in Chinese prepubescent children during walking. Gait Posture 2013, 37, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Gijon-Nogueron, G.; Martinez-Nova, A.; Alfageme-Garcia, P.; Montes-Alguacil, J.; Evans, A.M. International normative data for paediatric foot posture assessment: A cross-sectional investigation. BMJ Open 2019, 9, e023341. [Google Scholar] [CrossRef] [Green Version]
- Rojas, V.G.; Rebolledo, G.M.; Muñoz, E.G.; Cortés, N.I.; Gaete, C.B.; Delgado, C.M. Differences in standing balance between patients with diplegic and hemiplegic cerebral palsy. Neural Regen. Res. 2013, 8, 2478–2483. [Google Scholar]
- Galli, M.; Cimolin, V.; Rigoldi, C.; Tenore, N.; Albertini, G. Gait patterns in hemiplegic children with cerebral palsy: Comparison of right and left hemiplegia. Res. Dev. Disabil. 2010, 31, 1340–1345. [Google Scholar] [CrossRef] [PubMed]
- Jankowicz-Szymanska, A.; Mikolajczyk, E. Genu Valgum and Flat Feet in Children with Healthy and Excessive Body Weight. Pediatric Phys. Ther. 2016, 28, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Yan, S.; Li, R.; Shi, B.; Wang, R.; Yang, L. Mixed factors affecting plantar pressures and center of pressure in obese children: Obesity and flatfoot. Gait Posture 2020, 80, 7–13. [Google Scholar] [CrossRef]
- Park, S.Y.; Park, D.J. Comparison of Foot Structure, Function, Plantar Pressure and Balance Ability According to the Body Mass Index of Young Adults. Osong Public Health Res. Perspect. 2019, 10, 102–107. [Google Scholar] [CrossRef]
- Lim, J.U.; Lee, J.H.; Kim, J.S.; Hwang, Y.I.; Kim, T.H.; Lim, S.Y.; Yoo, K.H.; Jung, K.S.; Kim, Y.K.; Rhee, C.K. Comparison of World Health Organization and Asia-Pacific body mass index classifications in COPD patients. Int. J. Chronic Obstr. Pulm. Dis. 2017, 21, 2465–2475. [Google Scholar] [CrossRef] [Green Version]
- Chow, T.H.; Chen, Y.S.; Wang, J.C. Characteristics of plantar pressures and related pain profiles in elite sprinters and recreational runners. J. Am. Podiatr. Med. Assoc. 2018, 108, 33–44. [Google Scholar] [CrossRef]
- Chow, T.H.; Chen, Y.S.; Tsai, W.C.; Lin, M.H. Plantar pressure profiles and possible foot syndromes of Taiwanese college elite basketball players. J. Am. Podiatr. Med. Assoc. 2021, 111, Article_5. [Google Scholar] [CrossRef] [PubMed]
- Chow, T.H.; Chen, Y.S.; Hsu, C.C. Relationships between plantar pressure distribution and rearfoot alignment in the Taiwanese college athletes with plantar fasciopathy during static standing and walking. Int. J. Environ. Res. Public Health 2021, 18, 12942. [Google Scholar] [CrossRef] [PubMed]
- Chow, T.H.; Chen, Y.S.; Hsu, C.C.; Hsu, C.H. Characteristics of plantar pressure with foot postures and lower limb pain profiles in Taiwanese college elite rugby league athletes. Int. J. Environ. Res. Public Health 2022, 19, 1158. [Google Scholar] [CrossRef]
- Cavanagh, P.R.; Rodgers, M.M. The arch index: A useful measure from footprints. J. Biomech. 1987, 20, 547–551. [Google Scholar] [CrossRef]
- Ribeiro, A.P.; Sacco, I.C.; Dinato, R.C.; João, S.M.A. Relationships between static foot alignment and dynamic plantar loads in runners with acute and chronic stages of plantar fasciitis: A cross-sectional study. Braz. J. Phys. Ther. 2016, 20, 87–95. [Google Scholar] [CrossRef] [Green Version]
- Cornwall, M.W.; McPoil, T.G. Influence of rearfoot postural alignment on rearfoot motion during walking. Foot 2004, 14, 133–138. [Google Scholar] [CrossRef]
- Price, C.; Parker, D.; Nester, C. Validity and repeatability of three in-shoe pressure measurement systems. Gait Posture 2016, 46, 69–74. [Google Scholar] [CrossRef] [Green Version]
- Righi, N.C.; Martins, F.K.; Souza, J.A.; Trevisan, C.M. Plantar pressure distribution and foot morphology of children with cerebral palsy and typical development. Fisioter. E Pesqui. 2017, 24, 321–326. [Google Scholar] [CrossRef] [Green Version]
- Look, N.; Autruong, P.; Pan, Z.; Chang, F.M.; Carollo, J.J. Radiographic and plantar pressure assessment of pes planovalgus severity in children with cerebral palsy. Clin. Biomech. 2021, 85, 105364. [Google Scholar] [CrossRef]
- Dias, C.P.; Onzi, E.S.; Goulart, N.B.A.; Vaz, M.A. Muscular morphological adaptations of spasticity: Literature review. Sci. Med. 2013, 23, 102–107. [Google Scholar]
- Domagalska-Szopa, M.; Szopa, A. Postural pattern recognition in children with unilateral cerebral palsy. Ther. Clin. Risk Manag. 2014, 10, 113–120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maturana, C.S.; Silva, L.S.T.; Gaetan, E.S.M.; Ribeiro, D.C.L. Plantar pressure distribution in children with hemiparetic and diparetic cerebral palsy: Case control study. Ter Man 2013, 11, 481–487. [Google Scholar]
- Tomita, H.; Fukaya, Y.; Takagi, Y.; Yokozawa, A. Effects of severity of gross motor disability on anticipatory postural adjustments while standing in individuals with bilateral spastic cerebral palsy. Res. Dev. Disabil. 2016, 57, 92–101. [Google Scholar] [CrossRef]
- Shiratori, T.; Girolami, G.L.; Aruin, A.S. Anticipatory postural adjustments associated with a loading perturbation in children with hemiplegic and diplegic cerebral palsy. Exp. Brain Res. 2016, 234, 2967–2978. [Google Scholar] [CrossRef] [PubMed]
- Pereiro-Buceta, H.; Becerro-de-Bengoa-Vallejo, R.; Losa-Iglesias, M.E.; López-López, D.; Navarro-Flores, E.; Martínez-Jiménez, E.M.; Martiniano, J.; Calvo-Lobo, C. The Effect of Simulated Leg-Length Discrepancy on the Dynamic Parameters of the Feet during Gait-Cross-Sectional Research. Healthcare 2021, 9, 932. [Google Scholar] [CrossRef]
- Khamis, S.; Carmeli, E. Relationship and significance of gait deviations associated with limb length discrepancy: A systematic review. Gait Posture 2017, 57, 115–123. [Google Scholar] [CrossRef]
- Chang, W.D.; Chang, W.Y.; Lee, C.L.; Feng, C.Y. Validity and reliability of wii fit balance board for the assessment of balance of healthy young adults and the elderly. J. Phys. Ther. Sci. 2013, 25, 1251–1253. [Google Scholar] [CrossRef] [Green Version]
- Kruger, K.M.; Konop, K.A.; Krzak, J.J.; Graf, A.; Altiok, H.; Smith, P.A.; Harris, G.F. Segmental kinematic analysis of planovalgus feet during walking in children with cerebral palsy. Gait Posture 2017, 54, 277–283. [Google Scholar] [CrossRef] [Green Version]
- Ehlert, R.; Manfio, E.F.; Heidrich, R.D.O.; Goldani, R. Cerebral palsy: Influence of TheraTogs® on gait, posture and in functional performance. Fisioter. Em Mov. 2017, 30, 307–317. [Google Scholar] [CrossRef]
- Lee, S.Y.; Hertel, J. Effect of static foot alignment on plantar-pressure measures during running. J. Sport Rehabil. 2012, 21, 137–143. [Google Scholar] [CrossRef]
- Rodrigues, P.; Chang, R.; TenBroek, T.; van Emmerik, R.; Hamill, J. Evaluating the coupling between foot pronation and tibial internal rotation continuously using vector coding. J. Appl. Biomech. 2015, 31, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Menz, H.B.; Dufour, A.B.; Riskowski, J.L.; Hillstrom, H.J.; Hannan, M.T. Association of planus foot posture and pronated foot function are associated with foot pain: The Framingham foot study. Arthritis Care Res. 2013, 65, 1991–1999. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stovitz, S.D.; Coetzee, J.C. Hyperpronation and foot pain: Steps toward pain-free feet. Physician Sportsmed. 2004, 32, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Gómez, R.; Becerro-de-Bengoa-Vallejo, R.; Losa-Iglesias, M.; Calvo-Lobo, C.; Navarro-Flores, E.; Palomo-López, P.; Romero-Morales, C.; López-López, D. Reliability Study of Diagnostic Tests for Functional Hallux Limitus. Foot Ankle Int. 2020, 41, 457–462. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Healthy | Hemiplegic Cerebral Palsy | |||||
|---|---|---|---|---|---|---|
| Total | Male | Female | Total | Male | Female | |
| Number | 62 | 28 | 34 | 45 | 20 | 25 |
| Age (years) | 20.2 ± 0.8 | 20.1 ± 0.9 | 20.2 ± 0.7 | 19.4 ± 0.9 | 18.8 ± 0.5 | 20.0 ± 0.7 |
| Height (cm) | 165.5 ± 5.5 | 168.2 ± 5.1 | 163.3 ± 4.8 | 158.4 ± 4.8 | 161.4 ± 4.3 | 156.0 ± 3.8 |
| Mass (kg) | 60.8 ± 4.1 | 63.6 ± 3.8 | 58.5 ± 2.5 | 53.5 ± 4.7 | 57.0 ± 3.8 | 50.8 ± 3.5 |
| BMI (kg/m2) | 22.2 ± 1.2 | 22.5 ± 1.1 | 22.0 ± 1.3 | 21.4 ± 1.8 | 21.9 ± 1.6 | 20.9 ± 1.8 |
| Left Foot | Right Foot | |||||
|---|---|---|---|---|---|---|
| Total | Male | Female | Total | Male | Female | |
| Healthy | 0.22 ± 0.04 | 0.24 ± 0.02 | 0.20 ± 0.05 | 0.22 ± 0.05 | 0.23 ± 0.03 | 0.21 ± 0.06 |
| CP group | 0.26 ± 0.03 | 0.27 ± 0.03 1 | 0.24 ± 0.03 1 | 0.26 ± 0.04 | 0.27 ± 0.05 1 | 0.25 ± 0.03 1 |
| Left hemiplegic CP | 0.26 ± 0.03 | 0.27 ± 0.03 1 | 0.25 ± 0.02 1 | 0.26 ± 0.04 | 0.26 ± 0.04 | 0.26 ± 0.03 |
| Right hemiplegic CP | 0.25 ± 0.04 | 0.26 ± 0.05 | 0.24 ± 0.03 | 0.26 ± 0.04 | 0.27 ± 0.06 2 | 0.24 ± 0.02 1 |
| Left Foot (%) | Right Foot (%) | |||||
|---|---|---|---|---|---|---|
| Total | Male | Female | Total | Male | Female | |
| Forefoot | ||||||
| Healthy | 17.74 ± 11.40 | 21.48 ± 5.10 | 14.65 ± 14.00 | 22.84 ± 5.95 | 22.27 ± 5.76 | 23.30 ± 6.11 |
| CP group | 23.73 ± 4.89 2 | 22.79 ± 5.93 | 24.47 ± 3.77 2 | 23.48 ± 5.77 1 | 23.18 ± 7.90 1 | 23.72 ± 3.27 2 |
| Left hemiplegic CP | 24.28 ± 6.02 2 | 22.54 ± 7.43 | 25.67 ± 4.23 2 | 22.95 ± 6.40 | 22.49 ± 9.14 1 | 23.32 ± 2.87 2 |
| Right hemiplegic CP | 22.90 ± 2.20 2 | 23.18 ± 2.55 2 | 22.68 ± 1.92 2 | 24.27 ± 4.64 1 | 24.21 ± 5.66 | 24.31 ± 3.80 2 |
| Midfoot | ||||||
| Healthy | 10.98 ± 10.31 | 10.85 ± 10.26 | 11.10 ± 10.43 | 10.19 ± 9.84 | 10.93 ± 10.55 | 9.58 ± 9.24 |
| CP group | 8.48 ± 8.08 2 | 7.36 ± 6.72 2 | 9.38 ± 8.99 2 | 5.95 ± 5.85 2 | 4.01 ± 3.34 2 | 7.51 ± 6.90 2 |
| Left hemiplegic CP | 8.92 ± 8.69 2 | 7.08 ± 6.50 2 | 10.40 ± 9.97 | 5.97 ± 6.05 2 | 3.87 ± 3.45 2 | 7.64 ± 7.14 2 |
| Right hemiplegic CP | 7.82 ± 7.16 2 | 7.78 ± 7.24 2 | 7.85 ± 7.28 2 | 5.93 ± 5.61 2 | 4.21 ± 3.27 2 | 7.30 ± 6.72 2 |
| Rearfoot | ||||||
| Healthy | 16.46 ± 5.61 | 17.68 ± 5.72 | 15.45 ± 5.35 | 16.97 ± 5.60 | 16.80 ± 5.20 | 17.12 ± 5.95 |
| CP group | 17.80 ± 5.95 | 19.85 ± 6.22 | 16.17 ± 5.22 | 20.57 ± 7.52 2 | 22.82 ± 8.35 2 | 18.77 ± 6.32 |
| Left hemiplegic CP | 16.80 ± 5.72 | 20.39 ± 4.68 | 13.94 ± 4.82 | 21.08 ± 7.97 2 | 23.63 ± 8.09 2 | 19.03 ± 7.38 2 |
| Right hemiplegic CP | 19.30 ± 6.04 | 19.04 ± 8.11 | 19.52 ± 3.90 | 19.81 ± 6.84 | 21.59 ± 8.84 | 18.38 ± 4.43 |
| Left Foot (%) | Right Foot (%) | |||||
|---|---|---|---|---|---|---|
| Total | Male | Female | Total | Male | Female | |
| Control group | 48.85 ± 3.70 | 49.39 ± 3.21 | 48.41 ± 4.05 | 51.16 ± 3.69 | 50.61 ± 3.21 | 51.62 ± 4.03 |
| CP group | 48.60 ± 7.96 2 | 48.55 ± 8.08 2 | 48.64 ± 8.04 | 51.40 ± 7.96 2 | 51.45 ± 8.08 2 | 51.36 ± 8.04 2 |
| Left hemiplegic CP | 43.41 ± 5.22 1 | 42.83 ± 3.90 2 | 43.87 ± 6.17 1 | 56.59 ± 5.22 2 | 57.17 ± 3.90 2 | 56.13 ± 6.17 2 |
| Right hemiplegic CP | 56.39 ± 3.93 2 | 57.13 ± 3.60 2 | 55.80 ± 4.26 2 | 43.61 ± 3.93 2 | 42.88 ± 3.60 2 | 44.20 ± 4.26 1 |
| Left Foot | Right Foot | |||||
|---|---|---|---|---|---|---|
| Total | Male | Female | Total | Male | Female | |
| Healthy | 4.10 ± 2.41 | 4.04 ± 2.38 | 4.15 ± 2.47 | 4.68 ± 1.81 | 4.76 ± 1.55 | 4.61 ± 2.01 |
| CP group | 5.18 ± 1.59 | 5.12 ± 1.42 | 5.23 ± 1.74 | 4.48 ± 1.46 | 4.30 ± 1.09 | 4.62 ± 1.71 |
| Left hemiplegic CP | 6.11 ± 1.25 1 | 6.15 ± 0.67 1 | 6.07 ± 1.60 | 3.69 ± 1.32 1 | 3.51 ± 0.52 1 | 3.84 ± 1.72 |
| Right hemiplegic CP | 3.80 ± 0.87 2 | 3.57 ± 0.47 1 | 3.98 ± 1.09 1 | 5.65 ± 0.66 2 | 5.48 ± 0.36 1 | 5.79 ± 0.82 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chow, T.-H. Traceable Features of Static Plantar Pressure Characteristics and Foot Postures in College Students with Hemiplegic Cerebral Palsy. J. Pers. Med. 2022, 12, 394. https://doi.org/10.3390/jpm12030394
Chow T-H. Traceable Features of Static Plantar Pressure Characteristics and Foot Postures in College Students with Hemiplegic Cerebral Palsy. Journal of Personalized Medicine. 2022; 12(3):394. https://doi.org/10.3390/jpm12030394
Chicago/Turabian StyleChow, Tong-Hsien. 2022. "Traceable Features of Static Plantar Pressure Characteristics and Foot Postures in College Students with Hemiplegic Cerebral Palsy" Journal of Personalized Medicine 12, no. 3: 394. https://doi.org/10.3390/jpm12030394