
Oral Health among Elderly, Impact on Life Quality, Access of Elderly Patients to Oral Health Services and Methods to Improve Oral Health: A Narrative Review



 ,
,
Abstract
:1. Introduction
2. Materials and Methods
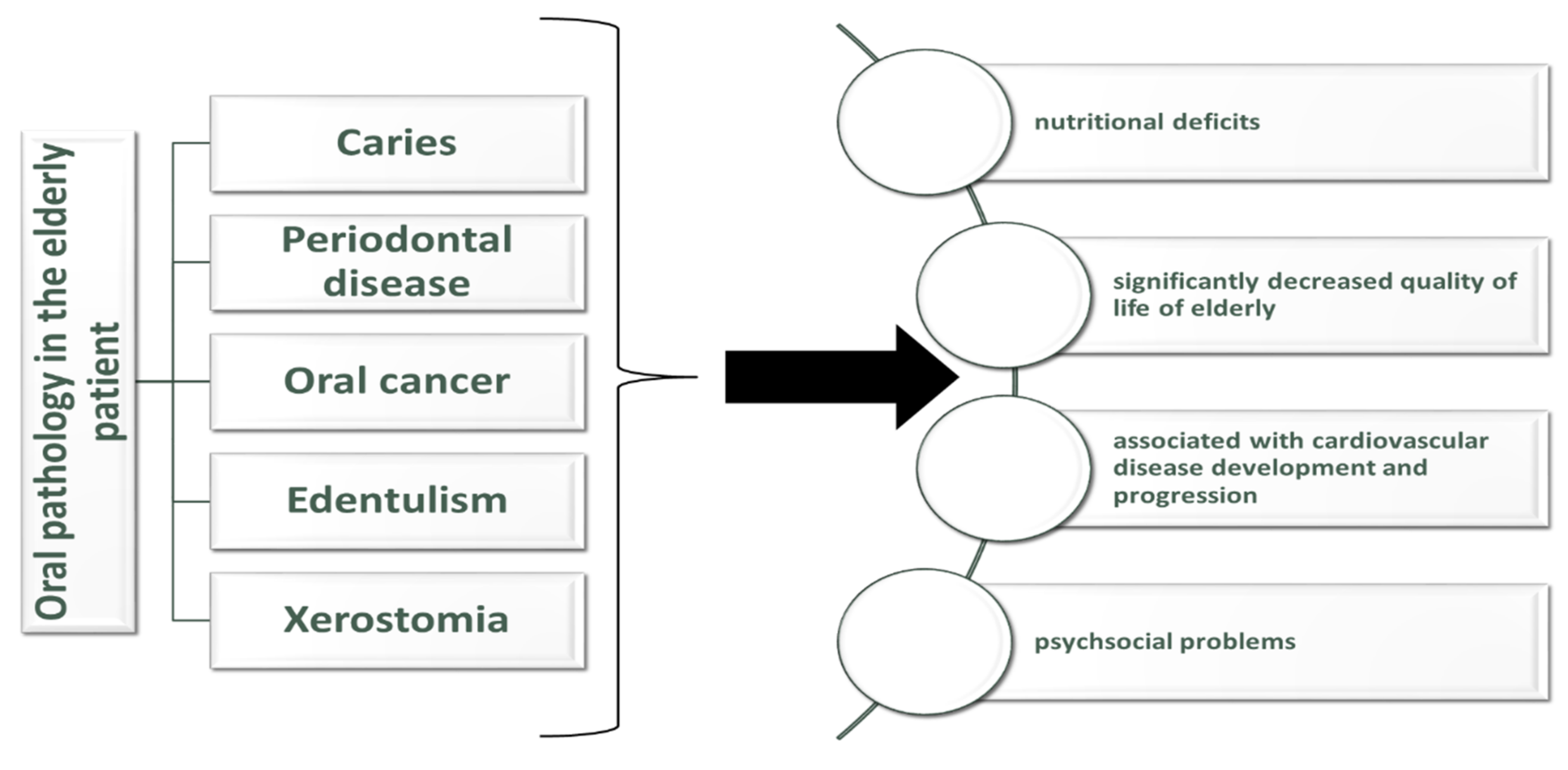
3. Oral Pathology in the Elderly Patient
3.1. Caries
3.2. Periodontal Disease
3.3. Oral Cancer in the Elderly
3.4. Edentulism
4. Impact of Oral Health among Elderly on Health and Nutrition
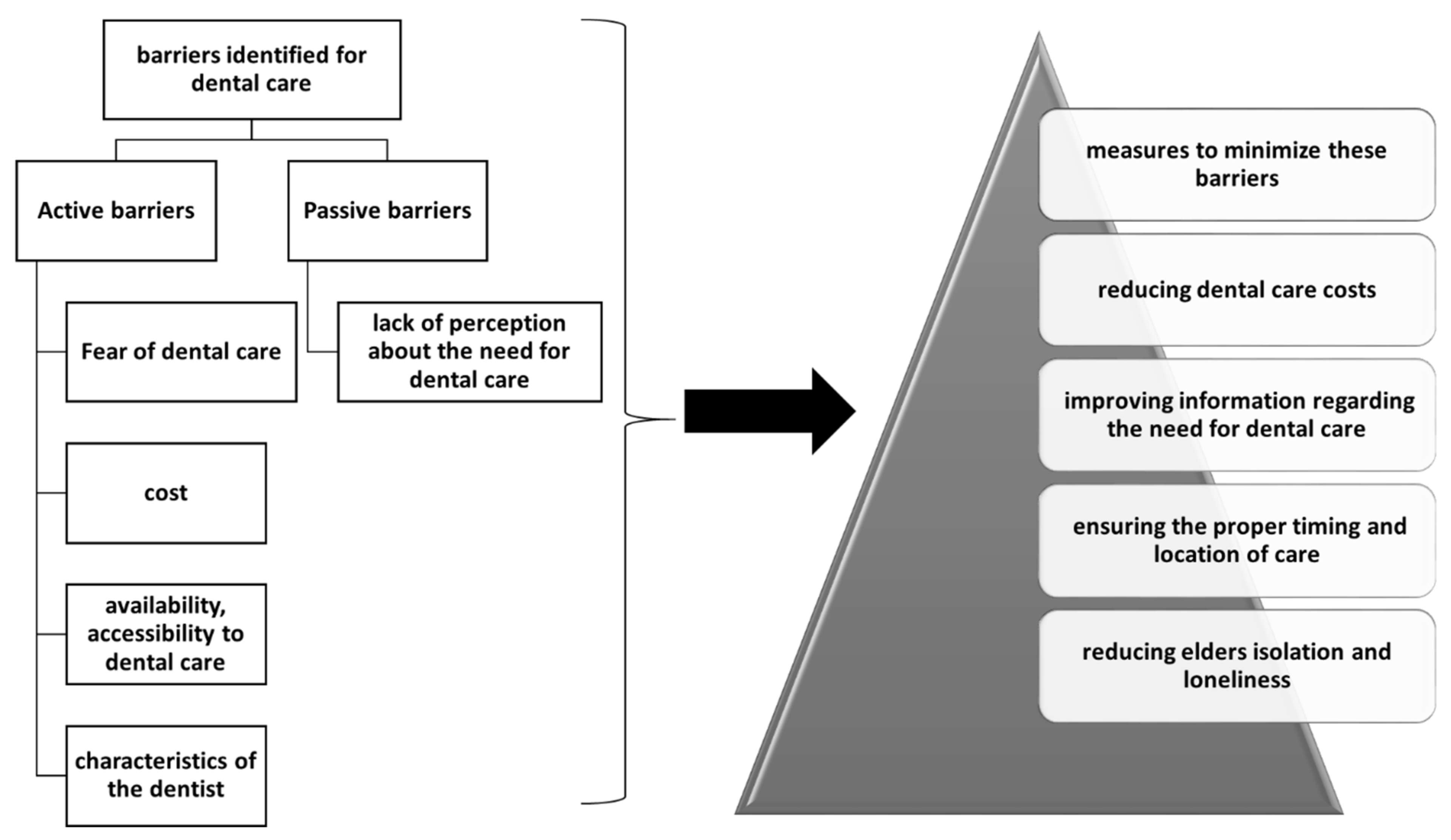
5. Access of Elderly Patients to Oral Health Services
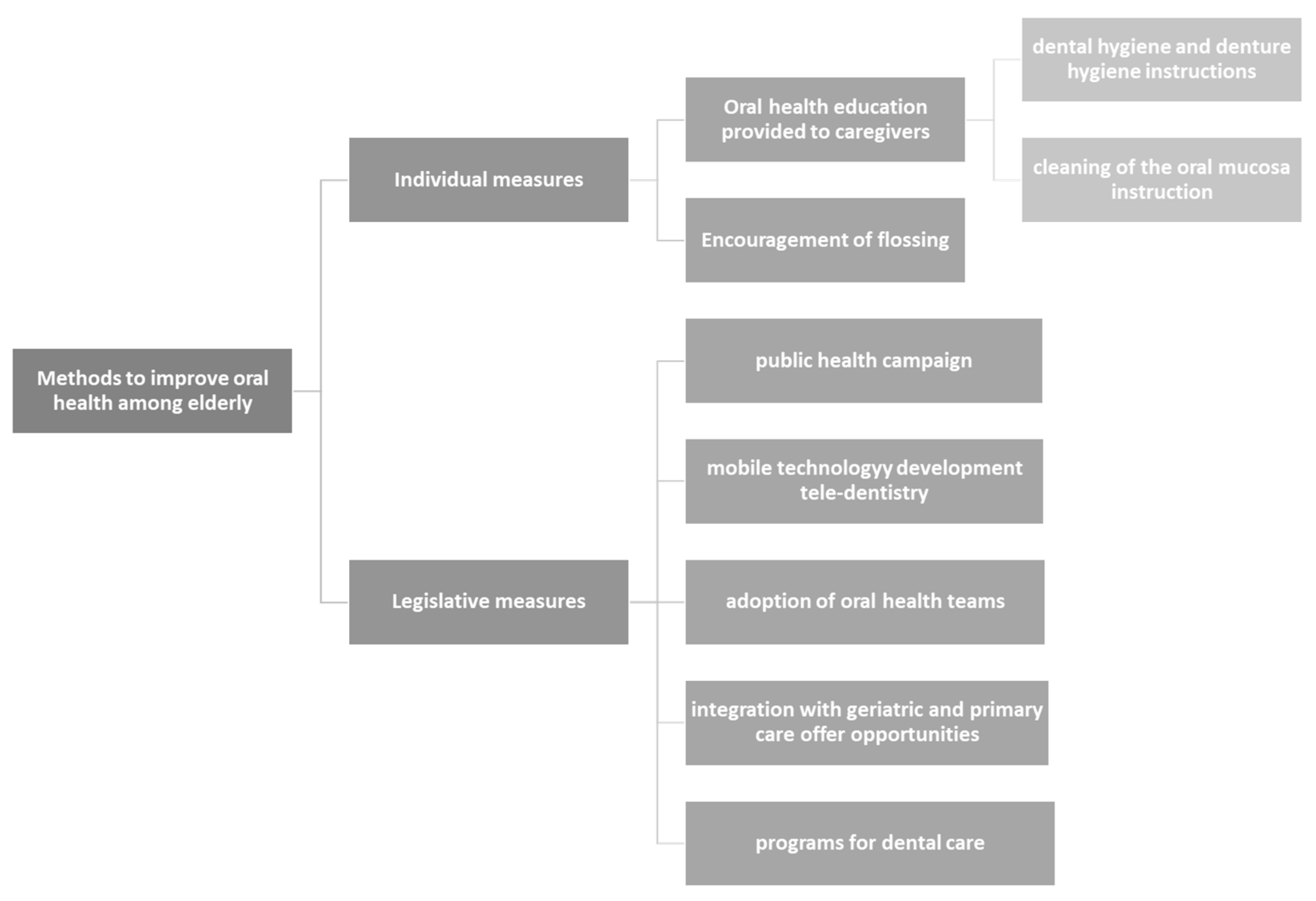
6. Methods to Improve Oral Health among Elderly
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Cho, E.-P.; Hwang, S.-J.; Clovis, J.B.; Lee, T.-Y.; Paik, D.-I.; Hwang, Y.-S. Enhancing the Quality of Life in Elderly Women through a Programme to Improve the Condition of Salivary Hypofunction: Oral Health Promotion Programme and Quality of Life. Gerodontology 2012, 29, e972–e980. [Google Scholar] [CrossRef]
- Glazar, I.; Urek, M.M.; Brumini, G.; Pezelj-Ribaric, S. Oral Sensorial Complaints, Salivary Flow Rate and Mucosal Lesions in the Institutionalized Elderly. J. Oral. Rehabil. 2010, 37, 93–99. [Google Scholar] [CrossRef]
- Sischo, L.; Broder, H.L. Oral Health-Related Quality of Life: What, Why, How, and Future Implications. J. Dent. Res. 2011, 90, 1264–1270. [Google Scholar] [CrossRef] [Green Version]
- Cosola, S.; Marconcini, S.; Giammarinaro, E.; Poli, G.L.; Covani, U.; Barone, A. Oral Health-Related Quality of Life and Clinical Outcomes of Immediately or Delayed Loaded Implants in the Rehabilitation of Edentulous Jaws: A Retrospective Comparative Study. Minerva Dent. Oral Sc. 2018, 67, 185–195. [Google Scholar] [CrossRef]
- De Lima Saintrain, M.V.; Gonçalves, R.D. Salivary Tests Associated with Elderly People’s Oral Health: Salivary Test in Elderly People. Gerodontology 2013, 30, 91–97. [Google Scholar] [CrossRef]
- Kossioni, A.E.; Dontas, A.S. The Stomatognathic System in the Elderly. Useful Information for the Medical Practitioner. Clin. Interv. Aging 2007, 2, 591–597. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). Oral Health. Available online: https://www.euro.who.int/en/health-topics/disease-prevention/oral-health# (accessed on 11 November 2021).
- De Oliveira, T.C.; da Silva, D.A.; Leite de Freitas, Y.N.; da Silva, R.L.; Pegado, C.P.d.C.; de Lima, K.C. Socio-Demographic Factors and Oral Health Conditions in the Elderly: A Population-Based Study. Arch. Gerontol. Geriatr. 2013, 57, 389–397. [Google Scholar] [CrossRef]
- Tsakos, G. Inequalities in Oral Health of the Elderly: Rising to the Public Health Challenge? J. Dent. Res. 2011, 90, 689–690. [Google Scholar] [CrossRef]
- Chalmers, J.; Pearson, A. Oral Hygiene Care for Residents with Dementia: A Literature Review. J. Adv. Nurs. 2005, 52, 410–419. [Google Scholar] [CrossRef]
- Jokanovic, N.; Tan, E.C.K.; Dooley, M.J.; Kirkpatrick, C.M.; Bell, J.S. Prevalence and Factors Associated with Polypharmacy in Long-Term Care Facilities: A Systematic Review. J. Am. Med. Dir. Assoc. 2015, 16, e1–e12. [Google Scholar] [CrossRef]
- Goldstein, G.; Goodacre, C.; MacGregor, K. Occlusal Vertical Dimension: Best Evidence Consensus Statement. J. Prosthodont. 2021, 30, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Morita, K.; Kimura, H.; Tsuka, H.; Nishio, F.; Yoshida, M.; Tsuga, K. Association between Salivary Alpha-Amylase and Subjective and Objective Oral Parafunctions in Community-Dwelling Elderly Individuals. J. Dent. Sci. 2020, 15, 310–314. [Google Scholar] [CrossRef] [PubMed]
- Bondar, A.; Popa, A.R.; Papanas, N.; Popoviciu, M.; Vesa, C.M.; Sabau, M.; Daina, C.; Stoica, R.A.; Katsiki, N.; Stoian, A.P. Diabetic Neuropathy: A Narrative Review of Risk Factors, Classification, Screening and Current Pathogenic Treatment Options (Review). Exp. Ther. Med. 2021, 22, 690. [Google Scholar] [CrossRef] [PubMed]
- Bekiroglu, N.; Çiftçi, A.; Bayraktar, K.; Yavuz, A.; Kargul, B. Oral Complaints of Denture-Wearing Elderly People Living in Two Nursing Homes in Istanbul, Turkey. Oral. Health Dent. Manag. 2012, 11, 107–115. [Google Scholar]
- Razak, P.A.; Richard, K.M.J.; Thankachan, R.P.; Hafiz, K.A.A.; Kumar, K.N.; Sameer, K.M. Geriatric Oral Health: A Review Article. J. Int. Oral. Health 2014, 6, 110–116. [Google Scholar]
- Wyatt, C.C.L.; Wang, D.; Aleksejuniene, J. Incidence of Dental Caries among Susceptible Community-Dwelling Older Adults Using Fluoride Toothpaste: 2-Year Follow-up Study. J. Can. Dent. Assoc. 2014, 80, e44. [Google Scholar]
- Hayes, M.; Allen, E.; da Mata, C.; McKenna, G.; Burke, F. Minimal Intervention Dentistry and Older Patients Part 2: Minimally Invasive Operative Interventions. Dent. Update 2014, 41, 500–505. [Google Scholar] [CrossRef]
- Thomson, W.M. Dental Caries Experience in Older People over Time: What Can the Large Cohort Studies Tell Us? Br. Dent. J. 2004, 196, 89–92. [Google Scholar] [CrossRef] [Green Version]
- Dye, B.A.; Tan, S.; Smith, V.; Lewis, B.G.; Barker, L.K.; Thornton-Evans, G.; Eke, P.I.; Beltrán-Aguilar, E.D.; Horowitz, A.M.; Li, C.-H. Trends in Oral Health Status: United States, 1988–1994 and 1999–2004; U.S. Department of Health and Human Services: Washington, DC, USA, 2007. [Google Scholar]
- Dye, B.; Thornton-Evans, G.; Li, X.; Iafolla, T. Dental Caries and Tooth Loss in Adults in the United States, 2011–2012. NCHS Data Brief. 2015, 197, 197. [Google Scholar]
- Jordan, R.A.; Micheelis, W. Krankheitsund Versorgungspravalenzen Bei Alteren Senioeren Mit Pflegebedarf; Funfte Deutsche: Koln, Germany, 2015. [Google Scholar]
- Schiffner, U. Krankheits- Und Versorgungspravalenzen Bei Jungeren Senioeren (65–74-Jahrige): Karies Und Erosionen; Institut der Deutschen Zahnärzte: Koln, Germany, 2015. [Google Scholar]
- Chan, A.K.Y.; Tamrakar, M.; Jiang, C.M.; Lo, E.C.M.; Leung, K.C.M.; Chu, C.H. A Systematic Review on Caries Status of Older Adults. Int. J. Environ. Res. Public Health 2021, 18, 10662. [Google Scholar] [CrossRef]
- Newman, M.G. Carranza’s Clinical Periodontology; Elsevier Health Sciences: Amsterdam, The Netherlands, 2011. [Google Scholar]
- World Health Organization. Oral Health; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Vos, T.; Abajobir, A.A.; Abate, K.H.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abdulkader, R.S.; Abdulle, A.M.; Abebo, T.A.; Abera, S.F.; et al. Global, Regional, and National Incidence, Prevalence, and Years Lived with Disability for 328 Diseases and Injuries for 195 Countries, 1990–2016: A Systematic Analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1211–1259. [Google Scholar] [CrossRef] [Green Version]
- Hirotomi, T.; Yoshihara, A.; Yano, M.; Ando, Y.; Miyazaki, H. Longitudinal Study on Periodontal Conditions in Healthy Elderly People in Japan. Community Dent. Oral Epidemiol. 2002, 30, 409–417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kassebaum, N.J.; Bernabé, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.L.; Marcenes, W. Global Burden of Severe Periodontitis in 1990-2010: A Systematic Review and Meta-Regression. J. Dent. Res. 2014, 93, 1045–1053. [Google Scholar] [CrossRef] [PubMed]
- Albandar, J.M. Epidemiology and risk factors of periodontal diseases. Dent. Clin. N. Am. 2005, 49, 517–532. [Google Scholar] [CrossRef]
- Socransky, S.S.; Haffajee, A.D.; Cugini, M.A.; Smith, C.; Kent, R.L., Jr. Microbial complexes in subgingival plaque. J. Clin. Microbiol. 1998, 25, 134–144. [Google Scholar] [CrossRef]
- Abusleme, L.; Dupuy, A.K.; Dutzan, N.; Silva, N.; Burleson, J.A.; Strausbaugh, L.D.; Gamonal, J.; Diaz, P.I. The subgingival microbiome in health and periodontitis and its relationship with community biomass and inflammation. ISME J. 2013, 7, 1016–1025. [Google Scholar] [CrossRef] [Green Version]
- Park, O.J.; Yi, H.; Jeon, J.H.; Kang, S.S.; Koo, K.; Kum, K.Y.; Chun, J.; Yun, C.H.; Han, S.H. Pyrosequencing Analysis of Subgingival Microbiota in Distinct Periodontal Conditions. J. Dent. Res. 2015, 94, 921–927. [Google Scholar] [CrossRef]
- Huang, S.; Yang, F.; Zeng, X.; Chen, J.; Li, R.; Wen, T.; Li, C.; Wei, W.; Liu, J.; Chen, L.; et al. Preliminary characterization of the oral microbiota of Chinese adults with and without gingivitis. BMC Oral Health 2011, 11, 33. [Google Scholar] [CrossRef] [Green Version]
- Griffen, A.L.; Beall, C.J.; Campbell, J.H.; Firestone, N.D.; Kumar, P.S.; Yang, Z.K.; Podar, M.; Leys, E.J. Distinct and complex bacterial profiles in human periodontitis and health revealed by 16S pyrosequencing. ISME J. 2012, 6, 1176–1185. [Google Scholar] [CrossRef] [Green Version]
- Shaddox, L.M.; Walker, C.B. Treating chronic periodontitis: Current status, challenges, and future directions. Clin. Cosmet. Investig. Dent. 2010, 2, 79–91. [Google Scholar] [CrossRef] [Green Version]
- Darveau, R.P. Periodontitis: A polymicrobial disruption of host homeostasis. Nat. Rev. Microbiol. 2010, 8, 481–490. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Wang, X.; Li, H.; Ni, C.; Du, Z.; Yan, F. Human oral microbiota and its modulation for oral health. Biomed. Pharmacother. 2018, 99, 883–893. [Google Scholar] [CrossRef] [PubMed]
- Kotronia, E.; Brown, H.; Papacosta, A.O.; Lennon, L.T.; Weyant, R.J.; Whincup, P.H.; Wannamethee, S.G.; Ramsay, S.E. Oral Health and All-Cause, Cardiovascular Disease, and Respiratory Mortality in Older People in the UK and USA. Sci. Rep. 2021, 11, 16452. [Google Scholar] [CrossRef] [PubMed]
- Brown, D.W. Complete Edentulism Prior to the Age of 65 Years Is Associated with All-Cause Mortality. J. Public Health Dent. 2009, 69, 260–266. [Google Scholar] [CrossRef]
- Emami, E.; de Souza, R.F.; Kabawat, M.; Feine, J.S. The Impact of Edentulism on Oral and General Health. Int. J. Dent. 2013, 2013, 498305. [Google Scholar] [CrossRef]
- Ministry of Health. Our Oral Health: Key Findings of the 2009 New Zealand Oral Health Survey; Ministry of Health: Wellington, New Zealand, 2010. [Google Scholar]
- Gerritsen, A.E.; Allen, P.F.; Witter, D.J.; Bronkhorst, E.M.; Creugers, N.H.J. Tooth Loss and Oral Health-Related Quality of Life: A Systematic Review and Meta-Analysis. Health Qual. Life Outcomes 2010, 8, 126. [Google Scholar] [CrossRef] [Green Version]
- Kassebaum, N.J.; Bernabé, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.L.; Marcenes, W. Global Burden of Severe Tooth Loss: A Systematic Review and Meta-Analysis: A Systematic Review and Meta-Analysis. J. Dent. Res. 2014, 93, 20S–28S. [Google Scholar] [CrossRef] [Green Version]
- Somsak, K.; Kaewplung, O. The Effects of the Number of Natural Teeth and Posterior Occluding Pairs on the Oral Healthrelated Quality of Life in Elderly Dental Patients. Gerodontology 2015, 33, 52–60. [Google Scholar] [CrossRef]
- Roohafza, H.; Afghari, P.; Keshteli, A.H.; Vali, A.; Shirani, M.; Adibi, P.; Afshar, H. The Relationship between Tooth Loss and Psychological Factors. Community Dent. Health 2015, 32, 16–19. [Google Scholar]
- Liljestrand, J.M.; Havulinna, A.S.; Paju, S.; Männistö, S.; Salomaa, V.; Pussinen, P.J. Missing Teeth Predict Incident Cardiovascular Events, Diabetes, and Death. J. Dent. Res. 2015, 94, 1055–1062. [Google Scholar] [CrossRef] [Green Version]
- Padilha, D.M.P.; Hilgert, J.B.; Hugo, F.N.; Bós, A.J.G.; Ferrucci, L. Number of Teeth and Mortality Risk in the Baltimore Longitudinal Study of Aging. J. Gerontol. A Biol. Sci. Med. Sci. 2008, 63, 739–744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ehizele, A.; Ojehanon, P. Periodontal Conditions Seen in a Group of Nigerian Older Adult Patients. J. Interdiscip. Dent. 2016, 6, 121. [Google Scholar] [CrossRef]
- Renvert, S.; Persson, G.R. Treatment of Periodontal Disease in Older Adults. Periodontology 2000 2016, 72, 108–119. [Google Scholar] [CrossRef] [PubMed]
- Eltas, A.; Uslu, M.O.; Eltas, S.D. Association of Oral Health-Related Quality of Life with Periodontal Status and Treatment Needs. Oral Health Prev. Dent. 2016, 14, 339–347. [Google Scholar]
- Sarini, J.; Fournier, C.; Lefebvre, J.L.; Bonafos, G.; Van, J.T.; Coche-Dequéant, B. Head and Neck Squamous Cell Carcinoma in Elderly Patients: A Long-Term Retrospective Review of 273 Cases. Arch. Otolaryngol. Head Neck Surg. 2001, 127, 1089–1092. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanabria, A.; Carvalho, A.L.; Vartanian, J.G.; Magrin, J.; Ikeda, M.K.; Kowalski, L.P. Comorbidity Is a Prognostic Factor in Elderly Patients with Head and Neck Cancer. Ann. Surg. Oncol. 2007, 14, 1449–1457. [Google Scholar] [CrossRef]
- Petersen, P.E.; Bourgeois, D.; Ogawa, H.; Estupinan-Day, S.; Ndiaye, C. The global burden of oral diseases and risk to oral health. Bull. World Health Organ. 2005, 83, 661–669. [Google Scholar]
- Gugić, J.; Strojan, P. Squamous Cell Carcinoma of the Head and Neck in the Elderly. Rep. Pract. Oncol. Radiother. 2012, 18, 16–25. [Google Scholar] [CrossRef] [Green Version]
- Paleri, V.; Wight, R.G.; Silver, C.E.; Haigentz, M., Jr.; Takes, R.P.; Bradley, P.J.; Rinaldo, A.; Sanabria, A.; Bień, S.; Ferlito, A. Comorbidity in Head and Neck Cancer: A Critical Appraisal and Recommendations for Practice. Oral Oncol. 2010, 46, 712–719. [Google Scholar] [CrossRef]
- Malik, A.; Mishra, A.; Chopda, P.; Singhvi, H.; Nair, S.; Nair, D.; Laskar, S.G.; Prabhash, K.; Agarwal, J.P.; Chaturvedi, P. Impact of Age on Elderly Patients with Oral Cancer. Eur. Arch. Otorhinolaryngol. 2019, 276, 223–231. [Google Scholar] [CrossRef]
- Polzer, I.; Schwahn, C.; Völzke, H.; Mundt, T.; Biffar, R. The Association of Tooth Loss with All-Cause and Circulatory Mortality. Is There a Benefit of Replaced Teeth? A Systematic Review and Meta-Analysis. Clin. Oral. Investig. 2012, 16, 333–351. [Google Scholar] [CrossRef] [PubMed]
- Dye, B.A.; Li, X.; Thorton-Evans, G. Oral Health Disparities as Determined by Selected Healthy People 2020 Oral Health Objectives for the United States, 2009–2010; US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics: Hyattsville, MD, USA, 2012. [Google Scholar]
- Osterberg, T.; Carlsson, G.E. Dental State, Prosthodontic Treatment and Chewing Ability - a Study of Five Cohorts of 70-Year-Old Subjects. J. Oral Rehabil. 2007, 34, 553–559. [Google Scholar] [CrossRef]
- Fantin, R.; Delpierre, C.; Kelly-Irving, M.; Barboza Solís, C. Early socioeconomic conditions and severe tooth loss in middle-aged Costa Ricans. Community Dent Oral Epidemiol. 2018, 46, 178–184. [Google Scholar] [CrossRef] [PubMed]
- Slade, G.D.; Akinkugbe, A.A.; Sanders, A.E. Projections of US Edentulism Prevalence Following 5 Decades of Decline. J. Dent. Res. 2014, 93, 959–965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peltzer, K.; Hewlett, S.; Yawson, A.E.; Moynihan, P.; Preet, R.; Wu, F.; Guo, G.; Arokiasamy, P.; Snodgrass, J.J.; Chatterji, S.; et al. Prevalence of Loss of All Teeth (Edentulism) and Associated Factors in Older Adults in China, Ghana, India, Mexico, Russia and South Africa. Int. J. Environ. Res. Public Health 2014, 11, 11308–11324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osterberg, T.; Carlsson, G.E.; Sundh, V. Trends and Prognoses of Dental Status in the Swedish Population: Analysis Based on Interviews in 1975 to 1997 by Statistics Sweden. Acta Odontol. Scand. 2000, 58, 177–182. [Google Scholar] [CrossRef]
- Cooper, L.F. The Current and Future Treatment of Edentulism. J. Prosthodont. 2009, 18, 116–122. [Google Scholar] [CrossRef]
- Müller, F.; Naharro, M.; Carlsson, G.E. What Are the Prevalence and Incidence of Tooth Loss in the Adult and Elderly Population in Europe? Clin. Oral. Implants Res. 2007, 18, 2–14. [Google Scholar] [CrossRef] [Green Version]
- Beltrán-Aguilar, E.D.; Barker, L.K.; Canto, M.T. Surveillance for Dental Caries, Dental Sealants, Tooth Retention, Edentulism, and Enamel Fluorosis—United States, 1988–1994 and 1999–2002; Department of Health and Human Services, Centers for Disease Control and Prevention: Hyattsville, MD, USA, 2005. [Google Scholar]
- Seerig, L.M.; Nascimento, G.G.; Peres, M.A.; Horta, B.L.; Demarco, F.F. Tooth loss in adults and income: Systematic review and meta-analysis. J Dent. 2015, 43, 1051–1059. [Google Scholar] [CrossRef]
- Hugo, F.N.; Hilgert, J.B.; da Luz Rosário de Sousa, M.; Cury, J.A. Oral Status and Its Association with General Quality of Life in Older Independent-Living South-Brazilians. Community Dent. Oral Epidemiol. 2009, 37, 231–240. [Google Scholar] [CrossRef]
- Nitschke, I.; Müller, F. The Impact of Oral Health on the Quality of Life in the Elderly. Oral Health Prev. Dent. 2004, 2, 271–275. [Google Scholar]
- Heydecke, G.; Thomason, J.M.; Lund, J.P.; Feine, J.S. The Impact of Conventional and Implant Supported Prostheses on Social and Sexual Activities in Edentulous Adults: Results from a Randomized Trial 2 Months after Treatment. J. Prosthet. Dent. 2006, 95, 396. [Google Scholar] [CrossRef]
- Rodrigues, S.M.; Oliveira, A.C.; Vargas, A.M.D.; Moreira, A.N.; E Ferreira, E.F. Implications of Edentulism on Quality of Life among Elderly. Int. J. Environ. Res. Public Health 2012, 9, 100–109. [Google Scholar] [CrossRef]
- National Center for Health Statistics National Health and Nutrition Examination Survey Data [2003–2008]; US Department of Health and Human Services, Centers for Disease Control and Prevention: Hyattsville, MD, USA, 2008.
- Morley, J.E. Anorexia of Ageing: A Key Component in the Pathogenesis of Both Sarcopenia and Cachexia: Editorial. J. Cachexia Sarcopenia Muscle 2017, 8, 523–526. [Google Scholar] [CrossRef] [Green Version]
- Agarwal, E.; Miller, M.; Yaxley, A.; Isenring, E. Malnutrition in the Elderly: A Narrative Review. Maturitas 2013, 76, 296–302. [Google Scholar] [CrossRef] [Green Version]
- Touger-Decker, R. Diet, Cardiovascular Disease and Oral Health. J. Am. Dent. Assoc. 2010, 141, 167–170. [Google Scholar] [CrossRef]
- Naka, O.; Anastassiadou, V.; Pissiotis, A. Association between Functional Tooth Units and Chewing Ability in Older Adults: A Systematic Review. Gerodontology 2014, 31, 166–177. [Google Scholar] [CrossRef]
- Greksa, L.P.; Parraga, I.M.; Clark, C.A. The Dietary Adequacy of Edentulous Older Adults. J. Prosthet. Dent. 1995, 73, 142–145. [Google Scholar] [CrossRef]
- Hung, H.-C.; Colditz, G.; Joshipura, K.J. The Association between Tooth Loss and the Self-Reported Intake of Selected CVD-Related Nutrients and Foods among US Women. Community Dent. Oral Epidemiol. 2005, 33, 167–173. [Google Scholar] [CrossRef]
- Takahashi, M.; Maeda, K.; Wakabayashi, H. Prevalence of Sarcopenia and Association with Oral Health-Related Quality of Life and Oral Health Status in Older Dental Clinic Outpatients. Geriatr. Gerontol. Int. 2018, 18, 915–921. [Google Scholar] [CrossRef]
- Friedlander, A.H.; Weinreb, J.; Friedlander, I.; Yagiela, J.A. Metabolic Syndrome: Pathogenesis, Medical Care and Dental Implications. J. Am. Dent. Assoc. 2007, 138, 179–187. [Google Scholar] [CrossRef]
- Gil-Montoya, J.A.; Sánchez-Lara, I.; Carnero-Pardo, C.; Fornieles-Rubio, F.; Montes, J.; Barrios, R.; Gonzalez-Moles, M.A.; Bravo, M. Oral Hygiene in the Elderly with Different Degrees of Cognitive Impairment and Dementia. J. Am. Geriatr. Soc. 2017, 65, 642–647. [Google Scholar] [CrossRef]
- Almirall, J.; Serra-Prat, M.; Bolíbar, I.; Balasso, V. Risk Factors for Community-Acquired Pneumonia in Adults: A Systematic Review of Observational Studies. Respiration 2017, 94, 299–311. [Google Scholar] [CrossRef]
- Lee, J.-H.; Oh, J.-Y.; Youk, T.-M.; Jeong, S.-N.; Kim, Y.-T.; Choi, S.-H. Association between Periodontal Disease and Non-Communicable Diseases: A 12-Year Longitudinal Health-Examinee Cohort Study in South Korea. Medicine 2017, 96, e7398. [Google Scholar] [CrossRef]
- Jansson, L.; Kalkali, H.; Mulk Niazi, F. Mortality Rate and Oral Health—A Cohort Study over 44 Years in the County of Stockholm. Acta Odontol. Scand. 2018, 76, 299–304. [Google Scholar] [CrossRef]
- Sjögren, P.; Wårdh, I.; Zimmerman, M.; Almståhl, A.; Wikström, M. Oral Care and Mortality in Older Adults with Pneumonia in Hospitals or Nursing Homes: Systematic Review and Meta-Analysis. J. Am. Geriatr. Soc. 2016, 64, 2109–2115. [Google Scholar] [CrossRef]
- Nakashima, T.; Maeda, K.; Tahira, K.; Taniguchi, K.; Mori, K.; Kiyomiya, H.; Akagi, J. Silent Aspiration Predicts Mortality in Older Adults with Aspiration Pneumonia Admitted to Acute Hospitals: Silent Aspiration in Pneumonia. Geriatr. Gerontol. Int. 2018, 18, 828–832. [Google Scholar] [CrossRef]
- Chalmers, J.M.; King, P.L.; Spencer, A.J.; Wright, F.A.C.; Carter, K.D. The Oral Health Assessment Tool—Validity and Reliability. Aust. Dent. J. 2005, 50, 191–199. [Google Scholar] [CrossRef] [Green Version]
- Maeda, K.; Mori, N. Poor Oral Health and Mortality in Geriatric Patients Admitted to an Acute Hospital: An Observational Study. BMC Geriatr. 2020, 20, 26. [Google Scholar] [CrossRef]
- Bianco, A.; Mazzea, S.; Fortunato, L.; Giudice, A.; Papadopoli, R.; Nobile, C.G.A.; Pavia, M. Oral Health Status and the Impact on Oral Health-Related Quality of Life among the Institutionalized Elderly Population: A Cross-Sectional Study in an Area of Southern Italy. Int. J. Environ. Res. Public Health 2021, 18, 2175. [Google Scholar] [CrossRef]
- Ide, K.; Seto, K.; Usui, T.; Tanaka, S.; Kawakami, K. Correlation between Dental Conditions and Comorbidities in an Elderly Japanese Population: A Cross-Sectional Study. Medicine 2018, 97, e11075. [Google Scholar] [CrossRef] [PubMed]
- Andersson, P.; Kragh Ekstam, A. Impaired Oral Health in Older Orthopaedic In-Care Patients: The Influence of Medication and Morbidity. Clin. Interv. Aging 2021, 16, 1691–1702. [Google Scholar] [CrossRef]
- Petersen, P.E.; Yamamoto, T. Improving the Oral Health of Older People: The Approach of the WHO Global Oral Health Programme. Community Dent. Oral Epidemiol. 2005, 33, 81–92. [Google Scholar] [CrossRef] [PubMed]
- Liddell, A.; Locker, D. Dental Anxiety in the Elderly. Psychol. Health 1993, 8, 175–183. [Google Scholar] [CrossRef]
- Slack-Smith, L.; Lange, A.; Paley, G.; O’Grady, M.; French, D.; Short, L. Oral Health and Access to Dental Care: A Qualitative Investigation among Older People in the Community: Oral Health and Access to Dental Care. Gerodontology 2009, 27, 104–113. [Google Scholar] [CrossRef] [Green Version]
- Metcalf, S.S.; Northridge, M.E.; Lamster, I.B. A Systems Perspective for Dental Health in Older Adults; American Public Health Association: Washington, DC, USA, 2011. [Google Scholar]
- Ornstein, K.A.; DeCherrie, L.; Gluzman, R.; Scott, E.S.; Kansal, J.; Shah, T.; Katz, R.; Soriano, T.A. Significant Unmet Oral Health Needs of Homebound Elderly Adults. J. Am. Geriatr. Soc. 2015, 63, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Nitschke, I.; Stillhart, A.; Kunze, J. Utilization of Dental Services in Old Age. Swiss Dent. J. 2015, 125, 433–447. [Google Scholar] [PubMed]
- Borreani, E.; Wright, D.; Scambler, S.; Gallagher, J.E. Minimising Barriers to Dental Care in Older People. BMC Oral Health 2008, 8, 7. [Google Scholar] [CrossRef] [Green Version]
- Gallagher, J.E.; Fiske, J. Special Care Dentistry: A Professional Challenge. Br. Dent. J. 2007, 202, 619–629. [Google Scholar] [CrossRef]
- Rocha, J.S.; Arima, L.; Chibinski, A.C.; Werneck, R.I.; Moysés, S.J.; Baldani, M.H. Barriers and facilitators to dental care during pregnancy: A systematic review and meta-synthesis of qualitative studies. Cad Saude Publ. 2018, 34, e00130817. [Google Scholar] [CrossRef] [Green Version]
- American Geriatrics Society. American Geriatrics Society Policy Brief: COVID-19 and Nursing Homes: Ags Policy Brief: COVID-19 & Nursing Homes. J. Am. Geriatr. Soc. 2020, 68, 908–911. [Google Scholar]
- Centers for Medicare & Medicaid Services. CMS Releases Recommendations on Adult Elective Surgeries, Non-Essential Medical, Surgical, And Dental Procedures during COVID-19 Response. Available online: https://www.cms.gov/newsroom/press-releases/cms-releases-recommendations-adult-elective-surgeries-non-essential-medical-surgical-and-dental (accessed on 21 November 2021).
- Ren, Y.F.; Rasubala, L.; Malmstrom, H.; Eliav, E. Dental Care and Oral Health under the Clouds of COVID-19. JDR Clin. Trans. Res. 2020, 5, 202–210. [Google Scholar] [CrossRef]
- Meng, L.; Hua, F.; Bian, Z. Coronavirus Disease 2019 (COVID-19): Emerging and Future Challenges for Dental and Oral Medicine. J. Dent. Res. 2020, 99, 481–487. [Google Scholar] [CrossRef] [Green Version]
- Hamasha, A.-H.; Aldosari, M.; Alturki, A.; Aljohani, S.; Aljabali, I.; Alotibi, R. Barrier to Access and Dental Care Utilization Behavior with Related Independent Variables in the Elderly Population of Saudi Arabia. J. Int. Soc. Prev. Community Dent. 2019, 9, 349. [Google Scholar] [CrossRef]
- Bomberg, T.J.; Ernst, N.S. Improving Utilization of Dental Care Services by the Elderly. Gerodontics 1986, 2, 57–60. [Google Scholar]
- Conrad, D.A. Dental Care Demand: Age-Specific Estimates for the Population 65 Years of Age and Over. Health Care Financ. Rev. 1983, 4, 47–57. [Google Scholar]
- Manski, R.; Moeller, J.; Chen, H.; Widström, E.; Lee, J.; Listl, S. Disparity in Dental Coverage among Older Adult Populations: A Comparative Analysis across Selected European Countries and the USA. Int. Dent. J. 2015, 65, 77–88. [Google Scholar] [CrossRef] [Green Version]
- Spinler, K.; Aarabi, G.; Valdez, R.; Kofahl, C.; Heydecke, G.; König, H.-H.; Hajek, A. Prevalence and Determinants of Dental Visits among Older Adults: Findings of a Nationally Representative Longitudinal Study. BMC Health Serv. Res. 2019, 19, 590. [Google Scholar] [CrossRef]
- Fleming, E.; Afful, J.; Griffin, S.O. Prevalence of tooth loss among older adults: United States, 2015-2018. NCHS Data Brief. 2020, 2020, 368. [Google Scholar]
- Kramarow, E.A. Dental Care among Adults Aged 65 and over, 2017. NCHS Data Brief. 2019, 2019, 337. [Google Scholar]
- Marshall, S.; Northridge, M.E.; De La Cruz, L.D.; Vaughan, R.D.; O’Neil-Dunne, J.; Lamster, I.B. ElderSmile: A Comprehensive Approach to Improving Oral Health for Seniors. Am. J. Public Health 2009, 99, 595–599. [Google Scholar] [CrossRef]
- Lewis, A.; Wallace, J.; Deutsch, A.; King, P. Improving the Oral Health of Frail and Functionally Dependent Elderly. Aust. Dent. J. 2015, 60, 95–105. [Google Scholar] [CrossRef] [Green Version]
- Marchesan, J.T.; Byrd, K.M.; Moss, K. Flossing Is Associated with Improved Oral Health in Older Adults. J. Dent. Res. 2020, 5, 072001. [Google Scholar] [CrossRef]
- Raphael, C. Oral Health and Aging. Am. J. Public Health 2017, 107, S44–S45. [Google Scholar] [CrossRef]
- Gomez-Rossi, J.; Hertrampf, K.; Abraham, J.; Gaßmann, G.; Meyer, G.; Schlattmann, P.; Göstemeyer, G.; Schwendicke, F. Interventions to Improve Oral Health of Older People: A Scoping Review. J. Dent. 2020, 101, 103451. [Google Scholar] [CrossRef]
- Khanagar, S.; Naganandini, S.; Tuteja, J.S.; Naik, S.; Satish, G.; Divya, K.T. Improving Oral Hygiene in Institutionalised Elderly by Educating Their Caretakers in Bangalore City, India: A Randomised Control Trial. Can. Geriatr. J. 2015, 18, 136–143. [Google Scholar] [CrossRef] [Green Version]
- Nihtilä, A.; Tuuliainen, E.; Komulainen, K.; Autonen-Honkonen, K.; Nykänen, I.; Hartikainen, S.; Ahonen, R.; Tiihonen, M.; Suominen, A.L. Preventive Oral Health Intervention among Old Home Care Clients. Age Ageing 2017, 46, 846–851. [Google Scholar] [CrossRef] [Green Version]
- McGrath, C.; Zhang, W.; Lo, E.C. A review of the effectiveness of oral health promotion activities among elderly people. Gerodontology 2009, 26, 85–96. [Google Scholar] [CrossRef] [PubMed]
- Manchery, N.; Subbiah, G.K.; Nagappan, N.; Premnath, P. Are oral health education for carers effective in the oral hygiene management of elderly with dementia? A systematic review. Dent. Res. J. 2020, 17, 1–9. [Google Scholar] [CrossRef]
- Nakre, P.D.; Harikiran, A.G. Effectiveness of oral health education programs: A systematic review. J. Int. Soc. Prev. Community Dent. 2013, 3, 103–115. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Identification of Studies via Databases and Registers for Realisation of the Extensive Review | ||
|---|---|---|
| Identification | Key words with OR operator | “dental pathology elderly”, “dental care elderly”, “caries in older individuals”, “dental care access elderly” |
| Consulted Databases | Web of Science, PubMed, Cochrane, Scopus | |
| Criteria for inclusion | Review or Original Article, cited at least 20 times, relevant for the topic and thematic, articles that focus on elderly people pathology | |
| Criteria for exclusion | Abstract paper, articles cited less than 20 times, not relevant for the topic and thematic, articles that did not focus on elderly pathology, misleading title related to content | |
| Records identified | Web of Science | 145 papers: 116 original papers + 29 review papers |
| Pubmed | 126 papers: 110 original papers + 16 review papers | |
| Cochrane | 39 papers: 32 original papers + 7 review papers | |
| Scopus | 50 papers: 38 original + 12 review papers | |
| Total records | Web of Science + Pubmed + Cochrane + Scopus | 350 papers: 296 original papers + 64 review papers |
| Duplicates removal | Web of Science + Pubmed + Cochrane + Scopus | exclusion of 83 papers |
| Full-text analysis | Appliance of inclusion and exclusion criteria | exclusion 145 papers |
| Final bibliographical source | 122 papers: 88 original papers + 2 review papers | |
| Authors | Number of Included Studies | Type of Study | Main Findings | Reference |
|---|---|---|---|---|
| McGrath C et al. | 17 | Systematic Review | Fluoride use, antimicrobial agents use and health-care provider education are important measures for oral health promotion activities for elderly people | [120] |
| Manchery N et al. | 4 | Systematic Review | Significant improvement of certain oral health measures in dementia elderly following a carer oral health education program | [121] |
| Nakre P et al. | 40 | Systematic Review | Oral health education was effective in improving the knowledge attitude and practice of oral health among elderly and in reducing bleeding on probing, plaque index and caries progression | [122] |
| Gommez-Rossi J et al. | 81 | Systematic Review | Most studies (64/81) found a statistically significant benefit of the intervention in elderly. Numerous intervention types employed (e.g., professional oral healthcare, educational interventions, restorative treatment, fluoride application and, generally, dentifrices, mouthwashes, chewing gums/food supplements) | [117] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Janto, M.; Iurcov, R.; Daina, C.M.; Neculoiu, D.C.; Venter, A.C.; Badau, D.; Cotovanu, A.; Negrau, M.; Suteu, C.L.; Sabau, M.; et al. Oral Health among Elderly, Impact on Life Quality, Access of Elderly Patients to Oral Health Services and Methods to Improve Oral Health: A Narrative Review. J. Pers. Med. 2022, 12, 372. https://doi.org/10.3390/jpm12030372
Janto M, Iurcov R, Daina CM, Neculoiu DC, Venter AC, Badau D, Cotovanu A, Negrau M, Suteu CL, Sabau M, et al. Oral Health among Elderly, Impact on Life Quality, Access of Elderly Patients to Oral Health Services and Methods to Improve Oral Health: A Narrative Review. Journal of Personalized Medicine. 2022; 12(3):372. https://doi.org/10.3390/jpm12030372
Chicago/Turabian StyleJanto, Michael, Raluca Iurcov, Cristian Marius Daina, Daniela Carmen Neculoiu, Alina Cristiana Venter, Dana Badau, Adrian Cotovanu, Marcel Negrau, Corina Lacramioara Suteu, Monica Sabau, and et al. 2022. "Oral Health among Elderly, Impact on Life Quality, Access of Elderly Patients to Oral Health Services and Methods to Improve Oral Health: A Narrative Review" Journal of Personalized Medicine 12, no. 3: 372. https://doi.org/10.3390/jpm12030372