
Comparisons of Videolaryngoscopes for Intubation Undergoing General Anesthesia: Systematic Review and Network Meta-Analysis of Randomized Controlled Trials

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Methods
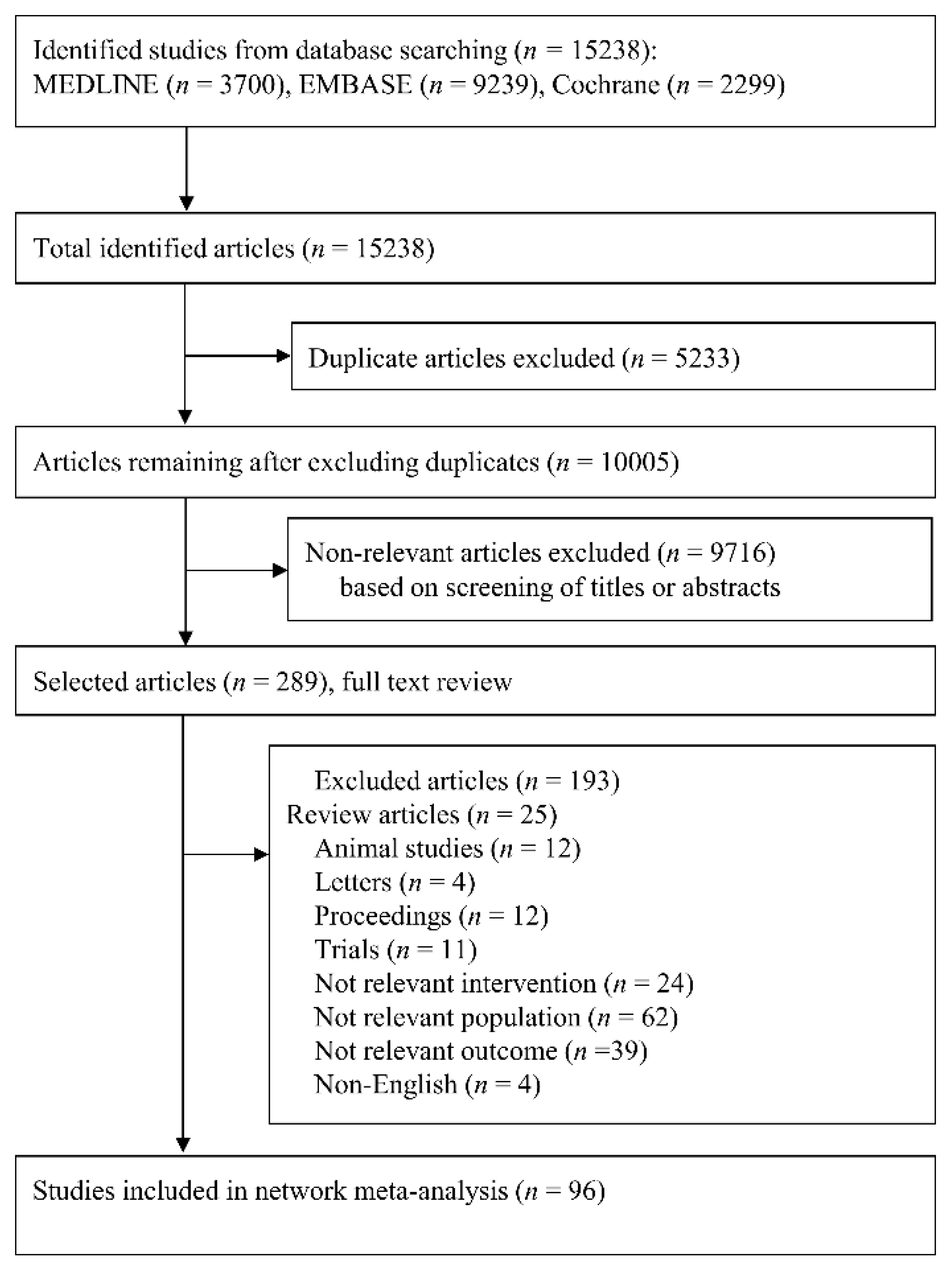
2.1. Literature Search
2.2. Data Selection
2.3. Data Identification and Extraction
2.4. Outcome Measures
2.5. Quality Assessment
2.6. Reporting Guidelines and Certainty of Evidence
2.7. Statistical Analysis
3. Results
3.1. Study and Patient Characteristics
3.2. Quality Assessment of the Included Studies
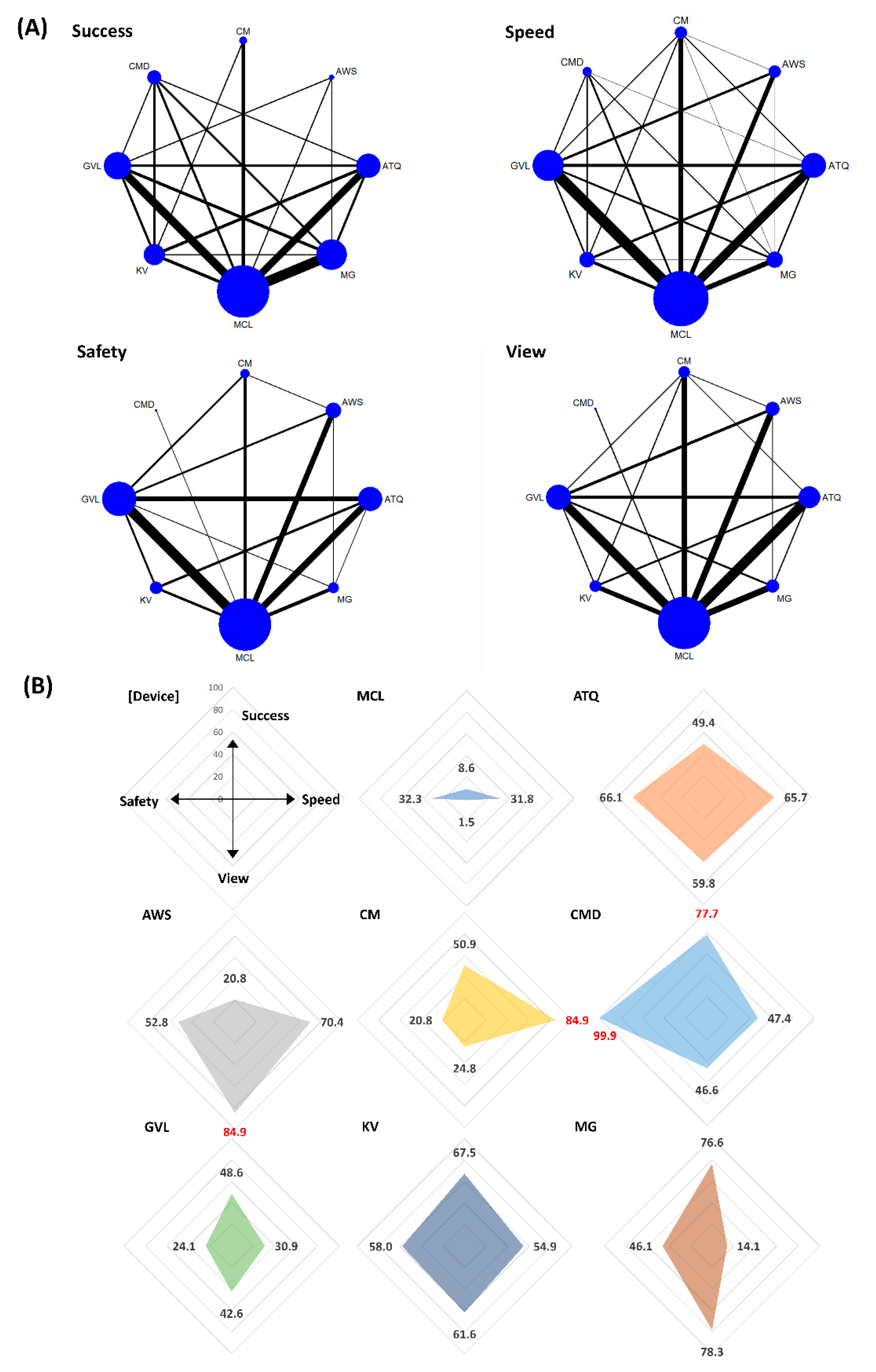
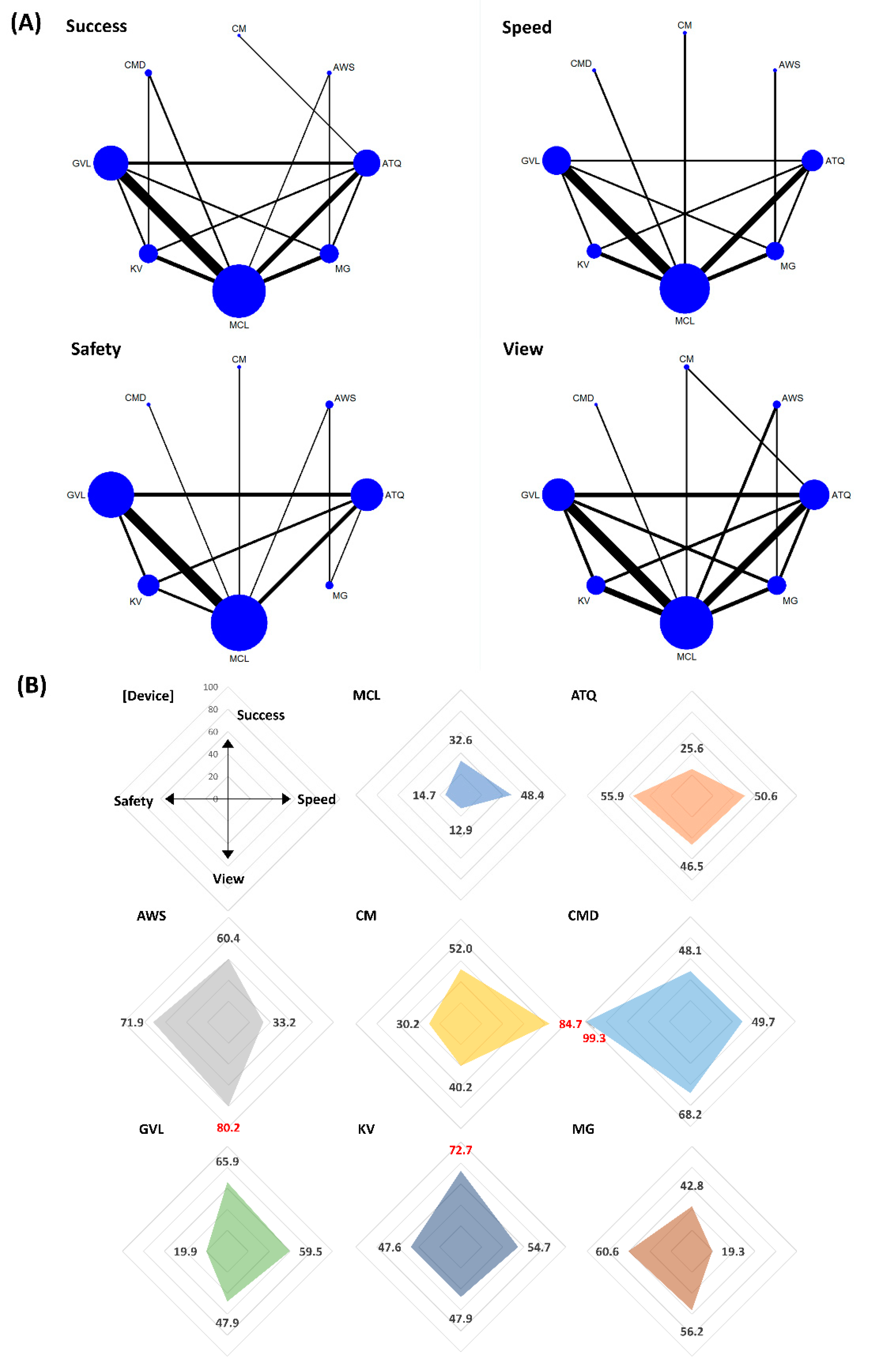
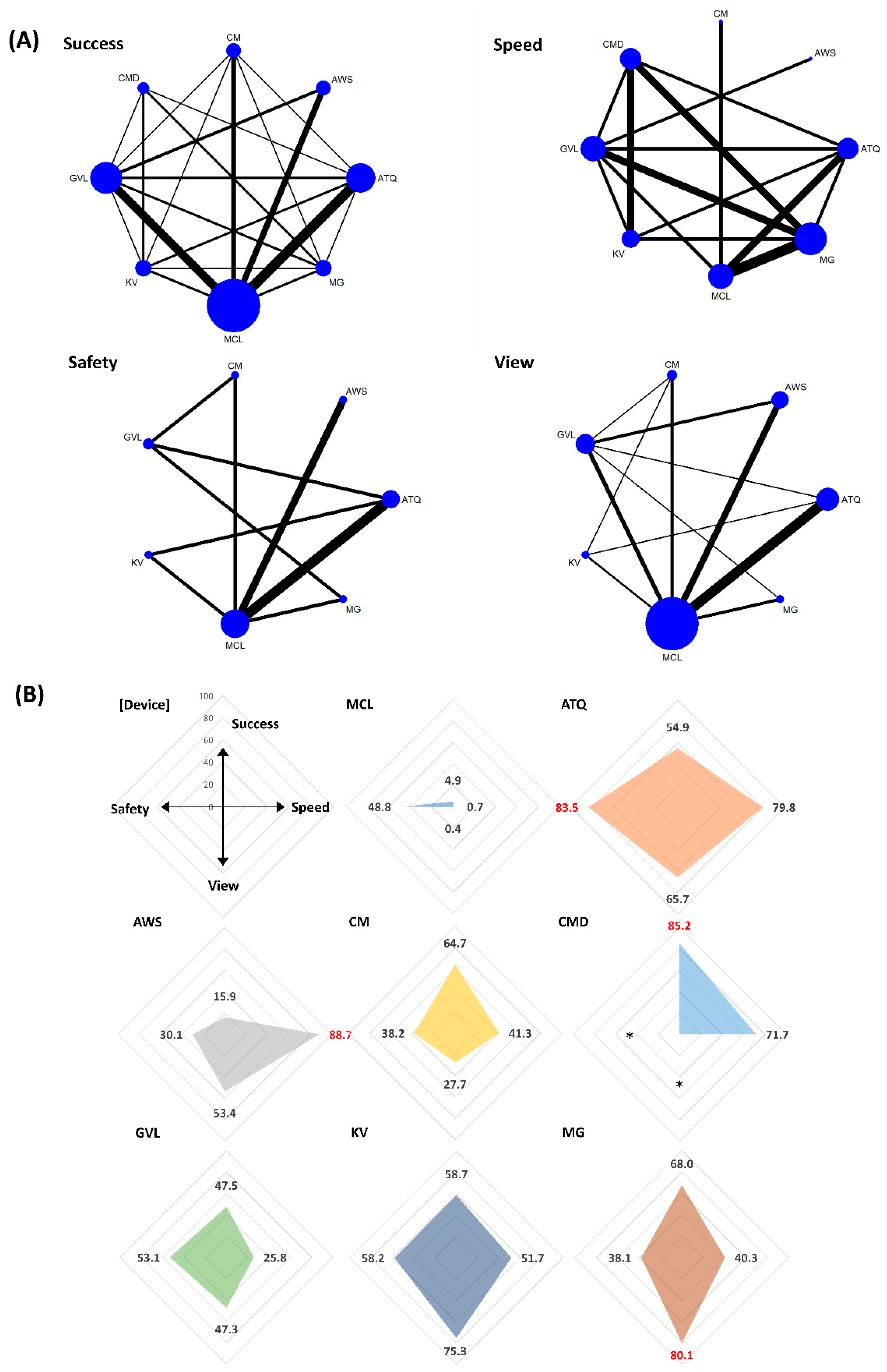
3.3. Quantitative Data Synthesis
3.3.1. Intubation Success Rate at First Attempt (Success)
3.3.2. Intubation Time to Confirmation by Capnometry (Speed)
3.3.3. Glottic View (View)
3.3.4. Sore Throat within 24 h after Extubation (Safety)
3.4. Quality Evidence in GRADE Assessment
3.5. Publication Bias
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Caplan, R.A.; Posner, K.L.; Ward, R.J.; Cheney, F.W. Adverse respiratory events in anesthesia: A closed claims analysis. Anesthesiology 1990, 72, 828–833. [Google Scholar] [CrossRef] [PubMed]
- Rose, D.K.; Cohen, M.M. The airway: Problems and predictions in 18,500 patients. Can. J. Anaesth. 1994, 41, 372–383. [Google Scholar] [CrossRef] [Green Version]
- Crosby, E.T.; Cooper, R.M.; Douglas, M.J.; Doyle, D.J.; Hung, O.R.; Labrecque, P.; Muir, H.; Murphy, M.F.; Preston, R.P.; Rose, D.K.; et al. The unanticipated difficult airway with recommendations for management. Can. J. Anaesth. 1998, 45, 757–776. [Google Scholar] [CrossRef] [Green Version]
- Karkouti, K.; Rose, D.K.; Wigglesworth, D.; Cohen, M.M. Predicting difficult intubation: A multivariable analysis. Can. J. Anaesth. 2000, 47, 730–739. [Google Scholar] [CrossRef] [Green Version]
- Juvin, P.; Lavaut, E.; Dupont, H.; Lefevre, P.; Demetriou, M.; Dumoulin, J.L.; Desmonts, J.M. Difficult tracheal intubation is more common in obese than in lean patients. Anesth. Analg. 2003, 97, 595–600. [Google Scholar] [CrossRef] [PubMed]
- Lundstrom, L.H.; Moller, A.M.; Rosenstock, C.; Astrup, G.; Wetterslev, J. High body mass index is a weak predictor for difficult and failed tracheal intubation: A cohort study of 91,332 consecutive patients scheduled for direct laryngoscopy registered in the Danish Anesthesia Database. Anesthesiology 2009, 110, 266–274. [Google Scholar] [CrossRef]
- Langeron, O.; Cuvillon, P.; Ibanez-Esteve, C.; Lenfant, F.; Riou, B.; Le Manach, Y. Prediction of difficult tracheal intubation: Time for a paradigm change. Anesthesiology 2012, 117, 1223–1233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bilehjani, E.; Fakhari, S. Hemodynamic response to laryngoscopy in ischemic heart disease: Macintosh blade versus glidescope videolaryngoscope. Rawal Med. J. 2009, 34, 151–154. [Google Scholar]
- Abdallah, R.; Galway, U.; You, J.; Kurz, A.; Sessler, D.I.; Doyle, D.J. A randomized comparison between the Pentax AWS video laryngoscope and the Macintosh laryngoscope in morbidly obese patients. Anesth. Analg. 2011, 113, 1082–1087. [Google Scholar] [CrossRef] [PubMed]
- Russell, T.; Slinger, P.; Roscoe, A.; McRae, K.; Van Rensburg, A. A randomised controlled trial comparing the GlideScope(®) and the Macintosh laryngoscope for double-lumen endobronchial intubation. Anaesthesia 2013, 68, 1253–1258. [Google Scholar] [CrossRef]
- Arici, S.; Karaman, S.; Dogru, S.; Karaman, T.; Tapar, H.; Ozsoy, A.Z.; Kaya, Z.; Suren, M. The McGrath Series 5 video laryngoscope versus the Macintosh laryngoscope: A randomized trial in obstetric patients. Turk. J. Med. Sci. 2014, 44, 387–392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruck, S.; Trautner, H.; Wolff, A.; Hain, J.; Mols, G.; Pakos, P.; Roewer, N.; Lange, M. Comparison of the C-MAC() and GlideScope() videolaryngoscopes in patients with cervical spine disorders and immobilisation. Anaesthesia 2015, 70, 160–165. [Google Scholar] [CrossRef]
- Pazur, I.; Maldini, B.; Hostic, V.; Ozegic, O.; Obraz, M. Comparison of Cormack Lehane Grading System and Intubation Difficulty Score in Patients Intubated by D-Blade Video and Direct Macintosh Laryngoscope: A Randomized Controlled Study. Acta Clin. Croat. 2016, 55, 560–564. [Google Scholar] [CrossRef] [Green Version]
- Ander, F.; Magnuson, A.; Berggren, L.; Ahlstrand, R.; de Leon, A. Time-to-intubation in obese patients. A randomized study comparing direct laryngoscopy and videolaryngoscopy in experienced anesthetists. Minerva Anestesiol. 2017, 83, 906–913. [Google Scholar] [CrossRef]
- Lu, Y.; Jiang, H.; Zhu, Y.S. Airtraq laryngoscope versus conventional Macintosh laryngoscope: A systematic review and meta-analysis. Anaesthesia 2011, 66, 1160–1167. [Google Scholar] [CrossRef] [PubMed]
- Griesdale, D.E.; Liu, D.; McKinney, J.; Choi, P.T. Glidescope(R) video-laryngoscopy versus direct laryngoscopy for endotracheal intubation: A systematic review and meta-analysis. Can. J. Anaesth. 2012, 59, 41–52. [Google Scholar] [CrossRef] [PubMed]
- Hoshijima, H.; Kuratani, N.; Hirabayashi, Y.; Takeuchi, R.; Shiga, T.; Masaki, E. Pentax Airway Scope(R) vs Macintosh laryngoscope for tracheal intubation in adult patients: A systematic review and meta-analysis. Anaesthesia 2014, 69, 911–918. [Google Scholar] [CrossRef] [PubMed]
- Lewis, S.R.; Butler, A.R.; Parker, J.; Cook, T.M.; Smith, A.F. Videolaryngoscopy versus direct laryngoscopy for adult patients requiring tracheal intubation. Cochrane Database Syst. Rev. 2016, 11, CD011136. [Google Scholar] [CrossRef] [PubMed]
- Jain, D. Scoring system for videolaryngoscopes: CL grade or POGO? Acta Anaesthesiol. Scand. 2018, 62, 1483. [Google Scholar] [CrossRef]
- Tripathi, M.; Pandey, M. Short thyromental distance: A predictor of difficult intubation or an indicator for small blade selection? Anesthesiology 2006, 104, 1131–1136. [Google Scholar] [CrossRef]
- Arne, J.; Descoins, P.; Fusciardi, J.; Ingrand, P.; Ferrier, B.; Boudigues, D.; Aries, J. Preoperative assessment for difficult intubation in general and ENT surgery: Predictive value of a clinical multivariate risk index. Br. J. Anaesth. 1998, 80, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Suppan, L.; Tramer, M.R.; Niquille, M.; Grosgurin, O.; Marti, C. Alternative intubation techniques vs Macintosh laryngoscopy in patients with cervical spine immobilization: Systematic review and meta-analysis of randomized controlled trials. Br. J. Anaesth. 2016, 116, 27–36. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2008. [Google Scholar]
- Brignardello-Petersen, R.; Bonner, A.; Alexander, P.E.; Siemieniuk, R.A.; Furukawa, T.A.; Rochwerg, B.; Hazlewood, G.S.; Alhazzani, W.; Mustafa, R.A.; Murad, M.H.; et al. Advances in the GRADE approach to rate the certainty in estimates from a network meta-analysis. J. Clin. Epidemiol. 2018, 93, 36–44. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Jackson, D.; Barrett, J.K.; Lu, G.; Ades, A.E.; White, I.R. Consistency and inconsistency in network meta-analysis: Concepts and models for multi-arm studies. Res. Synth. Methods 2012, 3, 98–110. [Google Scholar] [CrossRef] [Green Version]
- Chaimani, A.; Higgins, J.P.; Mavridis, D.; Spyridonos, P.; Salanti, G. Graphical tools for network meta-analysis in STATA. PLoS ONE 2013, 8, e76654. [Google Scholar] [CrossRef]
- Ahmed, S.M.; Doley, K.; Athar, M.; Raza, N.; Siddiqi, O.A.; Ali, S. Comparison of endotracheal intubation time in neutral position between C-Mac and Airtraq laryngoscopes: A prospective randomised study. Indian J. Anaesth. 2017, 61, 338–343. [Google Scholar] [CrossRef] [PubMed]
- Akbar, S.H.M.; Ooi, J.S.M. Comparison between C-MAC video-laryngoscope and macintosh direct laryngoscope during cervical spine immobilization. Middle East J. Anaesthesiol. 2015, 23, 43–50. [Google Scholar] [PubMed]
- Akbas, S.; Ozkan, A.S.; Karaaslan, E. A Comparison of McGrath MAC Versus C-MAC Videolaryngoscopes in Morbidly Obese Patients Undergoing Bariatric Surgery: A Randomized, Controlled Clinical Trial. Bariatr. Surg. Pract. Patient Care 2019, 14, 25–33. [Google Scholar] [CrossRef]
- Al-Ghamdi, A.A.; El Tahan, M.R.; Khidr, A.M. Comparison of the Macintosh, GlideScope, Airtraq, and King VisionTM laryngoscopes in routine airway management. Minerva Anestesiol. 2016, 82, 1278–1287. [Google Scholar] [PubMed]
- Ali, Q.E.; Amir, S.H.; Ahmad, S. A comparative evaluation of King Vision video laryngoscope (Channelled blade), McCoy, and Macintosh laryngoscopes for tracheal intubation in patients with immobilized cervical spine. Sri Lankan J. Anaesthesiol. 2017, 25, 70–75. [Google Scholar] [CrossRef]
- Ali, Q.E.; Amir, S.H.; Jamil, S.; Ahmad, S. A comparative evaluation of the Airtraq and King Vision video laryngoscope as an intubating aid in adult patients. Acta Anaesthesiol. Belg. 2015, 66, 81–85. [Google Scholar] [PubMed]
- Ali, Q.E.; Amir, S.H.; Siddiqui, O.A.; Mahopatra, P.S. A comparative evaluation of conventional Macintosh laryngoscope and the Airtraq in different intubation scenarios. Sri Lankan J. Anaesthesiol. 2012, 20, 3–6. [Google Scholar] [CrossRef]
- Amini, S.; Shakib, M. Hemodynamic changes following endotracheal intubation in patients undergoing cesarean section with general anesthesia: Application of glidescope videolaryngoscope versus direct laryngoscope. Anesthesiol. Pain Med. 2015, 5, e21836. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aoi, Y.; Inagawa, G.; Nakamura, K.; Sato, H.; Kariya, T.; Goto, T. Airway scope versus macintosh laryngoscope in patients with simulated limitation of neck movements. J. Trauma 2010, 69, 838–842. [Google Scholar] [CrossRef] [PubMed]
- Aqil, M.; Khan, M.U.; Hussain, A.; Khokhar, R.S.; Mansoor, S.; Alzahrani, T. Routine Use of Glidescope and Macintosh Laryngoscope by Trainee Anesthetists. J. Coll. Physicians Surg. Pak. JCPSP 2016, 26, 245–249. [Google Scholar] [PubMed]
- Aqil, M.; Khan, M.U.; Mansoor, S.; Mansoor, S.; Khokhar, R.S.; Narejo, A.S. Incidence and severity of postoperative sore throat: A randomized comparison of Glidescope with Macintosh laryngoscope. BMC Anesthesiol. 2017, 17, 127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bakshi, S.G.; Gawri, A.; Divatia, J.V. McGrath MAC video laryngoscope versus direct laryngoscopy for the placement of double-lumen tubes: A randomised control trial. Indian J. Anaesth. 2019, 63, 456–461. [Google Scholar] [CrossRef] [PubMed]
- Belze, O.; Lepage, E.; Bazin, Y.; Kerourin, P.; Fusciardi, J.; Remerand, F.; Espitalier, F. Glidescope versus Airtraq DL for double-lumen tracheal tube insertion in patients with a predicted or known difficult airway: A randomised study. Eur. J. Anaesthesiol. 2017, 34, 456–463. [Google Scholar] [CrossRef] [PubMed]
- Bhandari, G.; Shahi, K.S.; Asad, M.; Bhakuni, R. Airtraq() versus Macintosh laryngoscope: A comparative study in tracheal intubation. Anesth. Essays Res. 2013, 7, 232–236. [Google Scholar] [CrossRef] [Green Version]
- Blajic, I.; Hodzovic, I.; Lucovnik, M.; Mekis, D.; Novak-Jankovic, V.; Stopar Pintaric, T. A randomised comparison of C-MAC and King Vision(R) videolaryngoscopes with direct laryngoscopy in 180 obstetric patients. Int. J. Obs. Anesth. 2019, 39, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Çaparlar, C.Ö.; Aydın, G.B.; Sezer, E.; Ergil, J.; Doğan, A.Ş. A comparison of C-MAC videolaryngoscope and Macintosh laryngoscope in intraocular pressure changes, throat pain, intubation time and hemodynamic variables. Eur. Res. J. 2019, 5, 745–750. [Google Scholar] [CrossRef]
- Cavus, E.; Thee, C.; Moeller, T.; Kieckhaefer, J.; Doerges, V.; Wagner, K. A randomised, controlled crossover comparison of the C-MAC videolaryngoscope with direct laryngoscopy in 150 patients during routine induction of anaesthesia. BMC Anesthesiol. 2011, 11, 6. [Google Scholar] [CrossRef] [Green Version]
- Chalkeidis, O.; Kotsovolis, G.; Kalakonas, A.; Filippidou, M.; Triantafyllou, C.; Vaikos, D.; Koutsioumpas, E. A comparison between the Airtraq and Macintosh laryngoscopes for routine airway management by experienced anesthesiologists: A randomized clinical trial. Acta Anaesthesiol. Taiwanica Off. J. Taiwan Soc. Anesthesiol. 2010, 48, 15–20. [Google Scholar] [CrossRef]
- Chandrashekaraiah, M.M.; Shah, V.H.; Pandey, V.C.; Adeel, S. Evaluation of ease of intubation using C-MAC vs Macintosh laryngoscope in patients with the application of manual inline axial stabilization—A randomized comparative study. Sri Lankan J. Anaesthesiol. 2017, 25, 8–12. [Google Scholar] [CrossRef] [Green Version]
- Dhonneur, G.; Abdi, W.; Ndoko, S.K.; Amathieu, R.; Risk, N.; El Housseini, L.; Polliand, C.; Champault, G.; Combes, X.; Tual, L. Video-assisted versus conventional tracheal intubation in morbidly obese patients. Obes. Surg. 2009, 19, 1096–1101. [Google Scholar] [CrossRef]
- El-Tahan, M.R.; El Kenany, S.; Khidr, A.M.; Al Ghamdi, A.A.; Tawfik, A.M.; Al Mulhim, A.S. Cervical spine motion during tracheal intubation with King VisionTM video laryngoscopy and conventional laryngoscopy: A crossover randomized study. Minerva Anestesiol. 2017, 83, 1152–1160. [Google Scholar] [CrossRef]
- El-Tahan, M.R.; Khidr, A.M.; Gaarour, I.S.; Alshadwi, S.A.; Alghamdi, T.M.; Al’ghamdi, A. A Comparison of 3 Videolaryngoscopes for Double-Lumen Tube Intubation in Humans by Users With Mixed Experience: A Randomized Controlled Study. J. Cardiothorac. Vasc. Anesth. 2018, 32, 277–286. [Google Scholar] [CrossRef]
- Enomoto, Y.; Asai, T.; Arai, T.; Kamishima, K.; Okuda, Y. Pentax-AWS, a new videolaryngoscope, is more effective than the Macintosh laryngoscope for tracheal intubation in patients with restricted neck movements: A randomized comparative study. Br. J. Anaesth. 2008, 100, 544–548. [Google Scholar] [CrossRef] [Green Version]
- Foulds, L.T.; McGuire, B.E.; Shippey, B.J. A randomised cross-over trial comparing the McGrath® Series 5 videolaryngoscope with the Macintosh laryngoscope in patients with cervical spine immobilisation. Anaesthesia 2016, 71, 437–442. [Google Scholar] [CrossRef]
- Gupta, N.; Rath, G.P.; Prabhakar, H. Clinical evaluation of C-MAC videolaryngoscope with or without use of stylet for endotracheal intubation in patients with cervical spine immobilization. J. Anesth. 2013, 27, 663–670. [Google Scholar] [CrossRef] [PubMed]
- Hosalli, V.; Arjun, B.K.; Ambi, U.; Hulakund, S. Comparison of AirtraqTM, McCoyTM and Macintosh laryngoscopes for endotracheal intubation in patients with cervical spine immobilisation: A randomised clinical trial. Indian J. Anaesth. 2017, 61, 332–337. [Google Scholar] [CrossRef] [PubMed]
- Hsu, H.T.; Chou, S.H.; Wu, P.J.; Tseng, K.Y.; Kuo, Y.W.; Chou, C.Y.; Cheng, K.I. Comparison of the GlideScope® videolaryngoscope and the Macintosh laryngoscope for double-lumen tube intubation. Anaesthesia 2012, 67, 411–415. [Google Scholar] [CrossRef] [PubMed]
- Hu, B.; Zhou, H.; Wang, J.; Li, Y.; Luo, J. Glidescope video laryngoscope vs. Macintosh direct laryngoscope for the intubation of laryngeal neoplasm patients: A randomized controlled study. Int. J. Clin. Exp. Med. 2017, 10, 13639–13645. [Google Scholar]
- Ilyas, S.; Symons, J.; Bradley, W.P.L.; Segal, R.; Taylor, H.; Lee, K.; Balkin, M.; Bain, C.; Ng, I. A prospective randomised controlled trial comparing tracheal intubation plus manual in-line stabilisation of the cervical spine using the Macintosh laryngoscope vs the McGrath() Series 5 videolaryngoscope. Anaesthesia 2014, 69, 1345–1350. [Google Scholar] [CrossRef]
- Jafra, A.; Gombar, S.; Kapoor, D.; Sandhu, H.S.; Kumari, K. A prospective randomized controlled study to evaluate and compare GlideScope with Macintosh laryngoscope for ease of endotracheal intubation in adult patients undergoing elective surgery under general anesthesia. Saudi J. Anaesth. 2018, 12, 272–278. [Google Scholar] [CrossRef] [PubMed]
- Jeon, W.J.; Kim, K.H.; Yeom, J.H.; Bang, M.R.; Hong, J.B.; Cho, S.Y. A comparison of the glidescopespi to the mcgrath videolaryngoscope in patients. Korean J. Anesthesiol. 2011, 61, 19–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kido, H.; Komasawa, N.; Matsunami, S.; Kusaka, Y.; Minami, T. Comparison of McGRATH MAC and Macintosh laryngoscopes for double-lumen endotracheal tube intubation by anesthesia residents: A prospective randomized clinical trial. J. Clin. Anesth. 2015, 27, 476–480. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.K.; Park, S.W.; Lee, J.W. Randomized comparison of the Pentax AirWay Scope and Macintosh laryngoscope for tracheal intubation in patients with obstructive sleep apnoea. Br. J. Anaesth. 2013, 111, 662–666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kleine-Brueggeney, M.; Buttenberg, M.; Greif, R.; Nabecker, S.; Theiler, L. Evaluation of three unchannelled videolaryngoscopes and the Macintosh laryngoscope in patients with a simulated difficult airway: A randomised, controlled trial. Anaesthesia 2017, 72, 370–378. [Google Scholar] [CrossRef]
- Kleine-Brueggeney, M.; Greif, R.; Schoettker, P.; Savoldelli, G.L.; Nabecker, S.; Theiler, L.G. Evaluation of six videolaryngoscopes in 720 patients with a simulated difficult airway: A multicentre randomized controlled trial. Br. J. Anaesth. 2016, 116, 670–679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lange, M.; Frommer, M.; Redel, A.; Trautner, H.; Hampel, J.; Kranke, P.; Kehl, F.; Scholtz, L.U.; Roewer, N. Comparison of the Glidescope and Airtraq optical laryngoscopes in patients undergoing direct microlaryngoscopy. Anaesthesia 2009, 64, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Lee, H. The Pentax airway scope versus the Macintosh laryngoscope: Comparison of hemodynamic responses and concentrations of plasma norepinephrine to tracheal intubation. Korean J. Anesthesiol. 2013, 64, 315–320. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Kwak, H.J.; Lee, J.Y.; Chang, M.Y.; Lee, S.Y.; Kim, J.Y. Comparison of the Pentax AirwayScope and McGrath MAC videolaryngoscope for endotracheal intubation in patients with a normal airway. Medicine 2017, 96, e8713. [Google Scholar] [CrossRef] [PubMed]
- Lee, R.A.; van Zundert, A.A.J.; Maassen, R.L.J.G.; Wieringa, P.A. Forces applied to the maxillary incisors by video laryngoscopes and the Macintosh laryngoscope. Acta Anaesthesiol. Scand. 2012, 56, 224–229. [Google Scholar] [CrossRef]
- Lim, Y.; Yeo, S.W. A comparison of the GlideScope with the Macintosh laryngoscope for tracheal intubation in patients with simulated difficult airway. Anaesth. Intensive Care 2005, 33, 243–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, E.H.C.; Goy, R.W.L.; Tan, B.H.; Asai, T. Tracheal intubation with videolaryngoscopes in patients with cervical spine immobilization: A randomized trial of the Airway Scope and the GlideScope. Br. J. Anaesth. 2009, 103, 446–451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maharaj, C.H.; Buckley, E.; Harte, B.H.; Laffey, J.G. Endotracheal intubation in patients with cervical spine immobilization: A comparison of macintosh and airtraq laryngoscopes. Anesthesiology 2007, 107, 53–59. [Google Scholar] [CrossRef]
- Maharaj, C.H.; Costello, J.F.; Harte, B.H.; Laffey, J.G. Evaluation of the Airtraq and Macintosh laryngoscopes in patients at increased risk for difficult tracheal intubation. Anaesthesia 2008, 63, 182–188. [Google Scholar] [CrossRef]
- Maharaj, C.H.; O’Croinin, D.; Curley, G.; Harte, B.H.; Laffey, J.G. A comparison of tracheal intubation using the Airtraq or the Macintosh laryngoscope in routine airway management: A randomised, controlled clinical trial. Anaesthesia 2006, 61, 1093–1099. [Google Scholar] [CrossRef] [PubMed]
- Malik, M.A.; Maharaj, C.H.; Harte, B.H.; Laffey, J.G. Comparison of Macintosh, Truview EVO2, Glidescope, and Airwayscope laryngoscope use in patients with cervical spine immobilization. Br. J. Anaesth. 2008, 101, 723–730. [Google Scholar] [CrossRef] [Green Version]
- Malik, M.A.; Subramaniam, R.; Churasia, S.; Maharaj, C.H.; Harte, B.H.; Laffey, J.G. Tracheal intubation in patients with cervical spine immobilization: A comparison of the Airwayscope®, LMA CTrach®, and the Macintosh laryngoscopes. Br. J. Anaesth. 2009, 102, 654–661. [Google Scholar] [CrossRef] [Green Version]
- Malik, M.A.; Subramaniam, R.; Maharaj, C.H.; Harte, B.H.; Laffey, J.G. Randomized controlled trial of the Pentax AWS, Glidescope, and Macintosh laryngoscopes in predicted difficult intubation. Br. J. Anaesth. 2009, 103, 761–768. [Google Scholar] [CrossRef] [Green Version]
- Maruyama, K.; Nakagawa, H.; Imanishi, H.; Kitamura, A.; Hayashida, M. Comparison of postoperative pharyngeal morbidity using the Macintosh laryngoscope or AirWay Scope after mastectomy. J. Anesth. 2011, 25, 773–776. [Google Scholar] [CrossRef]
- Maruyama, K.; Yamada, T.; Kawakami, R.; Hara, K. Randomized cross-over comparison of cervical-spine motion with the AirWay Scope or Macintosh laryngoscope with in-line stabilization: A video-fluoroscopic study. Br. J. Anaesth. 2008, 101, 563–567. [Google Scholar] [CrossRef] [Green Version]
- Mathew, N.; Gaude, Y.K.; Joseph, T.T.; Kini, K.G. Comparison of haemodynamic responses to tracheal intubation using macintosh and airtraq laryngoscope in patients with simulated cervical spine injury. Sri Lankan J. Anaesthesiol. 2018, 26, 124–130. [Google Scholar] [CrossRef]
- McElwain, J.; Laffey, J.G. Comparison of the C-MAC, Airtraq, and Macintosh laryngoscopes in patients undergoing tracheal intubation with cervical spine immobilization. Br. J. Anaesth. 2011, 107, 258–264. [Google Scholar] [CrossRef] [Green Version]
- Mendonca, C.; Ungureanu, N.; Nowicka, A.; Kumar, P. A randomised clinical trial comparing the ‘sniffing’ and neutral position using channelled (KingVision) and non-channelled (C-MAC) videolaryngoscopes. Anaesthesia 2018, 73, 847–855. [Google Scholar] [CrossRef] [Green Version]
- Najafi, A.; Imani, F.; Makarem, J.; Khajavi, M.R.; Etezadi, F.; Habibi, S.; Shariat Moharari, R. Postoperative sore throat after laryngoscopy with macintosh or glide scope video laryngoscope blade in normal airway patients. Anesthesiol. Pain Med. 2014, 4, e15136. [Google Scholar] [CrossRef] [Green Version]
- Nandakumar, K.P.; Bhalla, A.P.; Pandey, R.K.; Baidya, D.K.; Subramaniam, R.; Kashyap, L. Comparison of Macintosh, McCoy, and Glidescope video laryngoscope for intubation in morbidly obese patients: Randomized controlled trial. Saudi J. Anaesth. 2018, 12, 433–439. [Google Scholar] [CrossRef]
- Ndoko, S.K.; Amathieu, R.; Tual, L.; Polliand, C.; Kamoun, W.; El Housseini, L.; Champault, G.; Dhonneur, G. Tracheal intubation of morbidly obese patients: A randomized trial comparing performance of Macintosh and Airtraq laryngoscopes. Br. J. Anaesth. 2008, 100, 263–268. [Google Scholar] [CrossRef] [Green Version]
- Ng, I.; Hill, A.L.; Williams, D.L.; Lee, K.; Segal, R. Randomized controlled trial comparing the McGrath videolaryngoscope with the C-MAC videolaryngoscope in intubating adult patients with potential difficult airways. Br. J. Anaesth. 2012, 109, 439–443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ninan, J.E.; Ranjan, R.V.; Ramachandran, T.R.; George, S.K. C-MAC videolaryngoscope improves the laryngoscopy view in Mallampati class 2 and 3 patients. Anaesth. Pain Intensive Care 2016, 20, 261–265. [Google Scholar]
- Nishikawa, K.; Matsuoka, H.; Saito, S. Tracheal intubation with the PENTAX-AWS (airway scope) reduces changes of hemodynamic responses and bispectral index scores compared with the Macintosh laryngoscope. J. Neurosurg. Anesthesiol. 2009, 21, 292–296. [Google Scholar] [CrossRef]
- Parasa, M.; Yallapragada, S.V.; Vemuri, N.N.; Shaik, M.S. Comparison of GlideScope video laryngoscope with Macintosh laryngoscope in adult patients undergoing elective surgical procedures. Anesth. Essays Res. 2016, 10, 245–249. [Google Scholar] [CrossRef] [Green Version]
- Ranieri, D.; Filho, S.M.; Batista, S.; do Nascimento, P. Comparison of Macintosh and Airtraq™ laryngoscopes in obese patients placed in the ramped position. Anaesthesia 2012, 67, 980–985. [Google Scholar] [CrossRef] [Green Version]
- Raza, N.; Hasan, M.; Ahmed, S.M.; Bano, S.; Athar, M. A comparative study of McGrath and Airtraq videolaryngoscopes for tracheal intubation. J. Anaesthesiol. Clin. Pharmacol. 2017, 33, 221–225. [Google Scholar] [CrossRef]
- Reena. Comparison of King Vision video laryngoscope (channeled blade) with Macintosh laryngoscope for tracheal intubation using armored endotracheal tubes. J. Anaesthesiol. Clin. Pharm. 2019, 35, 359–362. [Google Scholar] [CrossRef]
- Sahajanandan, R.; Dhanyee, A.S.; Gautam, A.K. A comparison of King vision video laryngoscope with CMAC D-blade in obese patients with anticipated difficult airway in tertiary hospital in India—Randomized control study. J. Anaesthesiol. Clin. Pharm. 2019, 35, 363–367. [Google Scholar] [CrossRef]
- Sargin, M.; Uluer, M.S. Comparison of McGrath() Series 5 video laryngoscope with Macintosh laryngoscope: A prospective, randomised trial in patients with normal airways. Pak. J. Med. Sci. 2016, 32, 869–874. [Google Scholar] [CrossRef] [PubMed]
- Sarkilar, G.; Sargin, M.; Saritas, T.B.; Borazan, H.; Gok, F.; Kilicaslan, A.; Otelcioglu, S. Hemodynamic responses to endotracheal intubation performed with video and direct laryngoscopy in patients scheduled for major cardiac surgery. Int. J. Clin. Exp. Med. 2015, 8, 11477–11483. [Google Scholar] [PubMed]
- Serocki, G.; Neumann, T.; Scharf, E.; Dorges, V.; Cavus, E. Indirect videolaryngoscopy with C-MAC D-Blade and GlideScope: A randomized, controlled comparison in patients with suspected difficult airways. Minerva Anestesiol. 2013, 79, 121–129. [Google Scholar] [PubMed]
- Shah, S.B.; Bhargava, A.K.; Hariharan, U.; Mittal, A.K.; Goel, N.; Choudhary, M. A Randomized Clinical Trial Comparing the Standard Mcintosh Laryngoscope and the C-Mac D blade Video laryngoscopeTM for Double Lumen Tube Insertion for One Lung Ventilation in Onco surgical Patients. Indian J. Anaesth. 2016, 60, 312–318. [Google Scholar] [CrossRef] [PubMed]
- Shravanalakshmi, D.; Bidkar, P.U.; Narmadalakshmi, K.; Lata, S.; Mishra, S.K.; Adinarayanan, S. Comparison of intubation success and glottic visualization using King Vision and C-MAC videolaryngoscopes in patients with cervical spine injuries with cervical immobilization: A randomized clinical trial. Surg. Neurol. Int. 2017, 8, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siddiqui, N.; Katznelson, R.; Friedman, Z. Heart rate/blood pressure response and airway morbidity following tracheal intubation with direct laryngoscopy, GlideScope and Trachlight: A randomized control trial. Eur. J. Anaesthesiol. 2009, 26, 740–745. [Google Scholar] [CrossRef] [PubMed]
- Sun, D.A.; Warriner, C.B.; Parsons, D.G.; Klein, R.; Umedaly, H.S.; Moult, M. The GlideScope Video Laryngoscope: Randomized clinical trial in 200 patients. Br. J. Anaesth. 2005, 94, 381–384. [Google Scholar] [CrossRef] [Green Version]
- Taylor, A.M.; Peck, M.; Launcelott, S.; Hung, O.R.; Law, J.A.; MacQuarrie, K.; McKeen, D.; George, R.B.; Ngan, J. The McGrath® Series 5 videolaryngoscope vs the Macintosh laryngoscope: A randomised, controlled trial in patients with a simulated difficult airway. Anaesthesia 2013, 68, 142–147. [Google Scholar] [CrossRef]
- Tempe, D.K.; Chaudhary, K.; Diwakar, A.; Datt, V.; Virmani, S.; Tomar, A.S.; Mohandas, A.; Mohire, V.B. Comparison of hemodynamic responses to laryngoscopy and intubation with Truview PCD™, McGrath® and Macintosh laryngoscope in patients undergoing coronary artery bypass grafting: A randomized prospective study. Ann. Card. Anaesth. 2016, 19, 68–75. [Google Scholar] [CrossRef]
- Teoh, W.H.L.; Saxena, S.; Shah, M.K.; Sia, A.T.H. Comparison of three videolaryngoscopes: Pentax Airway Scope, C-MAC, Glidescope vs the Macintosh laryngoscope for tracheal intubation. Anaesthesia 2010, 65, 1126–1132. [Google Scholar] [CrossRef]
- Teoh, W.H.L.; Shah, M.K.; Sia, A.T.H. Randomised comparison of Pentax AirwayScope and Glidescope for tracheal intubation in patients with normal airway anatomy. Anaesthesia 2009, 64, 1125–1129. [Google Scholar] [CrossRef]
- Toker, M.K.; Altiparmak, B.; Karabay, A.G. Comparison of the McGrath video laryngoscope and macintosh direct laryngoscope in obstetric patients: A randomized controlled trial. Pak. J. Med. Sci 2019, 35, 342–347. [Google Scholar] [CrossRef] [Green Version]
- Tolon, M.A.; Zanaty, O.M.; Shafshak, W.; Arida, E.E. Comparative study between the use of Macintosh Laryngoscope and Airtraq in patients with cervical spine immobilization. Alex. J. Med. 2012, 48, 179–185. [Google Scholar] [CrossRef]
- Tosh, P.; Kadapamannil, D.; Rajan, S.; Narayani, N.; Kumar, L. Effect of C-MAC Video Laryngoscope-aided intubations Using D-Blade on Incidence and Severity of Postoperative Sore Throat. Anesth. Essays Res. 2018, 12, 140–144. [Google Scholar] [CrossRef] [PubMed]
- Turkstra, T.P.; Cusano, F.; Fridfinnson, J.A.; Batohi, P.; Rachinsky, M. Early Endotracheal Tube Insertion with the GlideScope: A Randomized Controlled Trial. Anesth. Analg. 2016, 122, 753–757. [Google Scholar] [CrossRef] [PubMed]
- Varsha, A.V.; George, G.; Pillai, R.; Sahajanandan, R. Comparative evaluation of hemodynamic responses and ease of intubation with airtraq video laryngoscope versus macintosh laryngoscope in patients with ischemic heart disease. Ann. Card Anaesth. 2019, 22, 365–371. [Google Scholar] [CrossRef]
- Vijayakumar, V.; Rao, S.; Shetty, N. A Comparison of Macintosh and Airtraq Laryngoscopes for Endotracheal Intubation in Adult Patients With Cervical Spine Immobilization Using Manual In Line Axial Stabilization: A Prospective Randomized Study. J. Neurosurg. Anesthesiol. 2016, 28, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Wan, L.; Liao, M.; Li, L.; Qian, W.; Hu, R.; Chen, K.; Zhang, C.; Yao, W. McGrath Series 5 videolaryngoscope vs Airtraq DL videolaryngoscope for double-lumen tube intubation: A randomized trial. Medicine 2016, 95, e5739. [Google Scholar] [CrossRef] [PubMed]
- Wasem, S.; Lazarus, M.; Hain, J.; Festl, J.; Kranke, P.; Roewer, N.; Lange, M.; Smul, T.M. Comparison of the Airtraq and the Macintosh laryngoscope for double-lumen tube intubation: A randomised clinical trial. Eur. J. Anaesthesiol. 2013, 30, 180–186. [Google Scholar] [CrossRef] [PubMed]
- Wasinwong, W.; Pukdeetanakul, V.; Kanchanawanitkul, O.; Sriyannaluk, B. Comparison of Intubation Time with GlideScope and McIntosh Laryngoscope in Obese Patients. J. Med. Assoc. Thail. Chotmaihet Thangphaet 2017, 100, 306–312. [Google Scholar]
- Woo, C.-H.; Kim, S.H.; Park, J.-Y.; Bae, J.Y.; Kwak, I.-S.; Mun, S.H.; Kim, K.-M. Macintosh laryngoscope vs. Pentax-AWS video laryngoscope: Comparison of efficacy and cardiovascular responses to tracheal intubation in major burn patients. Korean J. Anesthesiol. 2012, 62, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Xue, F.S.; Zhang, G.H.; Li, X.Y.; Sun, H.T.; Li, P.; Li, C.W.; Liu, K.P. Comparison of hemodynamic responses to orotracheal intubation with the GlideScope videolaryngoscope and the Macintosh direct laryngoscope. J. Clin. Anesth. 2007, 19, 245–250. [Google Scholar] [CrossRef]
- Yao, W.L.; Wan, L.; Xu, H.; Qian, W.; Wang, X.R.; Tian, Y.K.; Zhang, C.H. A comparison of the McGrath Series 5 videolaryngoscope and Macintosh laryngoscope for double-lumen tracheal tube placement in patients with a good glottic view at direct laryngoscopy. Anaesthesia 2015, 70, 810–817. [Google Scholar] [CrossRef] [PubMed]
- Yi, J.; Gong, Y.; Quan, X.; Huang, Y. Comparison of the Airtraq laryngoscope and the GlideScope for double-lumen tube intubation in patients with predicted normal airways: A prospective randomized trial. BMC Anesthesiol. 2015, 15, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoo, J.Y.; Park, S.Y.; Kim, J.Y.; Kim, M.; Haam, S.J.; Kim, D.H. Comparison of the McGrath videolaryngoscope and the Macintosh laryngoscope for double lumen endobronchial tube intubation in patients with manual in-line stabilization: A randomized controlled trial. Medicine 2018, 97, e0081. [Google Scholar] [CrossRef] [PubMed]
- Yumul, R.; Elvir-Lazo, O.L.; White, P.F.; Sloninsky, A.; Kaplan, M.; Kariger, R.; Naruse, R.; Parker, N.; Pham, C.; Zhang, X.; et al. Comparison of three video laryngoscopy devices to direct laryngoscopy for intubating obese patients: A randomized controlled trial. J. Clin. Anesth. 2016, 31, 71–77. [Google Scholar] [CrossRef] [Green Version]
- Maruyama, K.; Yamada, T.; Kawakami, R.; Kamata, T.; Yokochi, M.; Hara, K. Upper cervical spine movement during intubation: Fluoroscopic comparison of the AirWay Scope, McCoy laryngoscope, and Macintosh laryngoscope. Br. J. Anaesth. 2008, 100, 120–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Jong, A.; Molinari, N.; Conseil, M.; Coisel, Y.; Pouzeratte, Y.; Belafia, F.; Jung, B.; Chanques, G.; Jaber, S. Video laryngoscopy versus direct laryngoscopy for orotracheal intubation in the intensive care unit: A systematic review and meta-analysis. Intensive Care Med. 2014, 40, 629–639. [Google Scholar] [CrossRef] [PubMed]
- Rombey, T.; Schieren, M.; Pieper, D. Video Versus Direct Laryngoscopy for Inpatient Emergency Intubation in Adults. Dtsch. Arztebl. Int. 2018, 115, 437–444. [Google Scholar] [CrossRef]
- Seo, K.H.; Kim, K.M.; John, H.; Jun, J.H.; Han, M.; Kim, S. Comparison of C-MAC D-blade videolaryngoscope and McCoy laryngoscope efficacy for nasotracheal intubation in simulated cervical spinal injury: A prospective randomized comparative study. BMC Anesth. 2020, 20, 114. [Google Scholar] [CrossRef]
- Kim, Y.S.; Song, J.; Lim, B.G.; Lee, I.O.; Won, Y.J. Different classes of videoscopes and direct laryngoscopes for double-lumen tube intubation in thoracic surgery: A systematic review and network meta-analysis. PLoS ONE 2020, 15, e0238060. [Google Scholar] [CrossRef]
- Kim, W.; Choi, H.J.; Lim, T.; Kang, B.S. Can the new McGrath laryngoscope rival the GlideScope Ranger portable video laryngoscope? A randomized manikin study. Am. J. Emerg. Med. 2014, 32, 1225–1229. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study, Year | Country | Patients Number | Airway Status | Devices | Tracheal Tube (Size; mm or Fr) | Success Rate (n) | Intubation Time (s) | Good Glottic View (n) | Sore Throat (n) |
|---|---|---|---|---|---|---|---|---|---|
| Abdallah, 2011 | USA | 99 | Difficult | MCL AWS | ETT (7/7.5 mm) | 45/49 43/50 | N/A | 38/49 43/50 | 16/50 16/49 |
| Abdulmohsen, 2016 | Saudi Arabia | 86 | Normal | MCL ATQ GVL KV | ETT (7/8 mm) | 16/22 9/21 15/21 15/22 | 35.1 ± 8.61 56.4 ± 6.02 41 ± 6.41 47.5 ± 8.94 | 19/22 19/21/ 19/21 22/22 | 19/22 6/21 16/21 11/22 |
| Ahmed, 2017 | India | 60 | Normal | ATQ CM | ETT | 27/30 28/30 | N/A | 28/30 28/30 | N/A |
| Akbar, 2015 | Malaysia | 90 | Difficult | MCL CM | ETT (7/7.5/8 mm) | 39/45 44/45 | 38.8 ± 8.9 32.7 ± 6.8 | 42/45 43/45 | N/A |
| Akbas, 2019 | Turkey | 80 | Difficult | CMD MG | ETT (7/7.5 mm) | 37/40 37/40 | 38.65 ± 17.57 55.2 ± 6.32 | N/A | N/A |
| Ali, 2012 | India | 50 | All | MCL ATQ | ETT | 16/25 22/25 | 36 ± 16 48 ± 18 | N/A | N/A |
| Ali, 2015 | India | 50 | All | ATQ KV | ETT | 21/25 24/25 | 38 ± 18 26 ± 11 | N/A | N/A |
| Ali, 2017 | India | 60 | Difficult | MCL KV | ETT (7/8 mm) | 27/30 29/30 | N/A | 24/30 28/30 | N/A |
| Amini, 2015 | Iran | 70 | Normal | MCL GVL | ETT | N/A | 9.3 ± 1.4 10.6 ± 1.7 | N/A | 15/35 13/35 |
| Ander, 2017 | Sweden | 78 | Difficult | MCL CM | ETT (6/7/8 mm) | 34/39 39/39 | N/A | N/A | 4/36 8/39 |
| Aoi, 2010 | Japan | 36 | Difficult | MCL AWS | ETT | 14/18 14/18 | N/A | 11/18 18/18 | 4/18 8/18 |
| Aqil, 2016 | Saudi Arabia | 80 | Normal | MCL GVL | ETT (7/8 mm) | 33/40 34/40 | 41.3 ± 15.2 32.9 ± 8.6 | 36/40 39/40 | N/A |
| Aqil, 2017 | Saudi Arabia | 140 | Normal | MCL GVL | ETT (7/8 mm) | 55/70 64/70 | N/A | 56/70 67/70 | 15/70 7/70 |
| Arici, 2014 | Turkey | 80 | All | MCL MG | ETT | 40/40 40/40 | 32.2 ± 6.58 47.25 ± 14.92 | 40/40 38/40 | N/A |
| Bakshi, 2019 | India | 74 | Normal | MCL MG | ETT* (35/37/39 Fr) | 35/3736/37 | 56.6 ± 14 64.4 ± 24 | 36/37 37/37 | N/A |
| Belze, 2017 | France | 72 | Difficult | ATQ GVL | ETT* (35/37/39/41 Fr) | 28/36 29/36 | N/A | 36/36 33/36 | 34/36 33/36 |
| Bhandari, 2013 | India | 80 | Normal | MCL ATQ | ETT | 38/40 40/40 | 29 ± 5.4 18 ± 2.6 | 34/36 36/36 | 36/36 34/36 |
| Bilehjani, 2009 | Iran | 80 | Normal | MCL GVL | ETT | 29/40 35/40 | N/A | N/A | N/A |
| Blajic, 2019 | Slovenia | 178 | All | MCL CM KV | ETT (6.5 mm) | 56/59 59/60 56/59 | 29 ± 14 25 ± 7 29 ± 9 | 52/59 55/60 57/59 | N/A |
| Bruck, 2015 | Germany | 56 | Difficult | CM GVL | ETT (7.5/8 mm) | 15/26 28/30 | N/A | 26/26 30/30 | 9/26 12/30 |
| Caparlar, 2019 | Turkey | 78 | Normal | MCL CM | ETT | N/A | 41.49 ± 10.3 27.74 ± 7.2 | 39/39 39/39 | 0/39 0/39 |
| Cavus, 2011 | Germany | 87 | All | MCL CM | ETT | 48/50 27/37 | N/A | N/A | N/A |
| Chalkeidis, 2010 | Greece | 63 | All | MCL ATQ | ETT | 27/28 31/35 | N/A | N/A | N/A |
| Chandrashek-araiah, 2017 | Bahrain | 60 | Difficult | MCL CM | ETT | N/A | N/A | 26/30 28/30 | N/A |
| Dhonneur, 2009 | France | 212 | Difficult | MCL ATQ | ETT | N/A | N/A | 90/106 106/106 | N/A |
| ElTahan, 2017 | Saudi Arabia | 29 | Normal | MCL KV | ETT | 29/29 29/29 | N/A | N/A | N/A |
| ElTahan, 2018 | Saudi Arabia | 133 | Normal | MCL ATQ GVL KV | ETT* (35/37/39 Fr) | 32/32 33/35 34/34 32/32 | N/A | 28/32 30/35 29/34 25/32 | 2/32 1/35 29/34 2/32 |
| Enomoto, 2008 | Japan | 203 | Difficult | MCL AWS | ETT (7/8 mm) | N/A | N/A | 181/203 203/203 | N/A |
| Foulds, 2016 | England | 49 | Difficult | MCL MG | ETT | 18/25 24/24 | 95.3 ± 55.2 55 ± 18.5 | 28/49 0/49 | N/A |
| Gupta, 2013 | India | 60 | Difficult | MCL CM | ETT (7.5/8.5 mm) | 28/30 30/30 | N/A | 12/30 26/30 | N/A |
| Hosalli, 2017 | India | 60 | Difficult | MCL ATQ | ETT | 23/30 27/30 | N/A | 27/30 30/30 | N/A |
| Hsu, 2012 | Taiwan | 60 | Normal | MCL GVL | ETT* (35/37 Fr) | 26/30 30/30 | 62.5 ± 29.7 45.6 ± 10.7 | N/A | 12/30 6/30 |
| Hu, 2017 | China | 196 | Difficult | MCL GVL | ETT (6/6.5/7 mm) | 95/96 100/100 | N/A | 46/96 88/100 | N/A |
| Ilyas, 2014 | Australia | 128 | Difficult | MCL MG | ETT (7/7.5/8/8.5 mm) | N/A | N/A | N/A | 39/64 40/64 |
| Jafra, 2018 | India | 200 | Normal | MCL GVL | ETT | 100/100 100/100 | N/A | 86/100 77/100 | 0/100 1/100 |
| Jeon, 2011 | South Korea | 56 | Normal | GVL MG | ETT (7/7.5 mm) | 25/28 27/28 | 41.6 ± 10.7 56.5 ± 23.2 | 28/28 28/28 | N/A |
| Kido, 2015 | Japan | 50 | All | MCL MG | ETT* (32/35/37 Fr) | 16/25 24/25 | 20.8 ± 5.9 17.1 ± 4.6 | 20/25 25/25 | 14/25 7/25 |
| Kim, 2013 | South Korea | 45 | All | MCL AWS | ETT (7/7.5/8 mm) | 19/23 22/22 | 24.3 ± 16.6 12.9 ± 6 | 8/23 22/22 | N/A |
| Kleine-Brueg-geney, 2016 | Switzerland | 600 | Difficult | ATQ CMD GVL KV MG | ETT (6.5/7.5 mm) | 102/120 114/120 102/120 104/120 117/120 | 47.7 ± 18 62 ± 30 68.7 ± 37.5 61 ± 24 57.3 ± 26.2 | N/A | N/A |
| Kleine-Brueg-geney, 2017 | Switzerland | 360 | Difficult | MCL ATQ KV | ETT (6.5/7.5 mm) | 53/120 98/120 108/120 | N/A | 7/120 107/120 116/120 | 28/120 21/120 26/120 |
| Lange, 2009 | Germany | 60 | All | ATQ GVL | ETT | 28/30 29/30 | N/A | 28/30 30/30 | 15/30 12/30 |
| Lee, 2012 | Netherlands | 75 | Normal | MCL GVL MG | ETT | 21/25 25/25 25/25 | N/A | 21/25 25/25 25/25 | N/A |
| Lee, 2013 | South Korea | 40 | Normal | MCL AWS | ETT (6.5/7.5 mm) | N/A | N/A | N/A | 0/20 0/20 |
| Lee, 2017 | South Korea | 140 | Normal | AWS MG | ETT (7 mm) | 70/70 70/70 | 30.3 ± 5.3 31.3 ± 6.1 | 70/70 67/70 | 10/70 17/70 |
| Lim, 2005 | Singapore | 60 | Difficult | MCL GVL | ETT (7 mm) | 26/30 28/30 | 56.2 ± 27 41.8 ± 20 | 12/30 28/30 | N/A |
| Liu 2009 | Japan | 70 | Difficult | AWS GVL | ETT | 34/35 29/35 | 34.2 ± 25.1 71.9 ± 47.9 | 35/35 35/35 | N/A |
| Maharaj, 2006 | Ireland | 60 | Normal | MCL ATQ | ETT | 29/30 30/30 | N/A | 29/30 30/30 | N/A |
| Maharaj, 2007 | Ireland | 40 | Difficult | MCL ATQ | ETT | 19/20 20/20 | N/A | 13/20 20/20 | N/A |
| Maharaj, 2008 | Ireland | 40 | Difficult | MCL ATQ | ETT | 13/20 19/20 | N/A | 3/20 20/20 | N/A |
| Malik, 2008 | Ireland | 90 | Difficult | MCL AWS GVL | ETT (7.5/8.5 mm) | 26/30 27/30 28/30 | N/A | 25/30 30/30 30/30 | N/A |
| Malik1, 2009 | Ireland | 75 | Difficult | MCL AWS GVL | ETT (7.5/8.5 mm) | 17/25 18/25 22/25 | N/A | 17/25 25/25 25/25 | N/A |
| Malik2, 2009 | Ireland | 60 | Difficult | MCL AWS | ETT (7.5/8 mm) | 29/30 28/30 | N/A | 25/30 30/30 | N/A |
| Maruyama, 2008 | Japan | 24 | Normal | MCL AWS | ETT | N/A | N/A | 12/12 12/12 | N/A |
| Maruyama, 2011 | Japan | 68 | Normal | MCL AWS | ETT (7 mm) | 32/34 33/34 | N/A | 31/34 34/34 | N/A |
| Mathew, 2018 | India | 60 | Difficult | MCL ATQ | ETT (7/7.5/8/8.5 mm) | 29/30 27/30 | N/A | 25/30 21/30 | 26/30 27/30 |
| McElwain, 2011 | Ireland | 90 | Difficult | MCL ATQ CM | ETT | 25/31 28/29 26/30 | N/A | N/A | N/A |
| Mendonca, 2018 | England | 100 | Normal | KV CMD | ETT | 47/50 48/50 | N/A | N/A | N/A |
| Najafi, 2014 | Iran | 300 | All | MCL GVL | ETT (7.5/8 mm) | N/A | N/A | N/A | 81/150 34/150 |
| Nandakumar, 2018 | India | 30 | Difficult | MCL GVL | ETT (7/7.5/8/8.5 mm) | 13/15 11/15 | N/A | N/A | N/A |
| Ndoko, 2008 | France | 106 | Difficult | MCL ATQ | ETT | 49/53 53/53 | N/A | 42/53 53/53 | N/A |
| Ng, 2012 | Australia | 130 | Difficult | MG CM | ETT (7/7.5/8/8.5 mm) | 45/65 58/65 | N/A | N/A | N/A |
| Ninan, 2016 | India | 60 | All | MCL CM | ETT | 30/30 30/30 | N/A | 20/30 21/30 | N/A |
| Nishikawa, 2009 | Japan | 40 | All | MCL AWS | ETT (7/8 mm) | N/A | N/A | N/A | 6/20 2/20 |
| Parasa, 2016 | India | 60 | All | MCL GVL | ETT (7/8 mm) | 30/30 24/30 | 27.77 ± 5.12 45.70 ± 11.65 | 26/30 29/30 | 8/30 10/30 |
| Pazur, 2016 | Croatia | 52 | Normal | MCL CMD | ETT (7.5/8.5 mm) | 26/26 26/26 | 34.3 ± 15.1 33.6 ± 16.7 | 24/26 26/26 | N/A |
| Ranieri, 2012 | Brazil | 132 | Difficult | MCL ATQ | ETT (7.5/8.5 mm) | 54/64 68/68 | 37 ± 23 14 ± 3 | 57/64 68/68 | N/A |
| Raza, 2017 | India | 60 | Normal | MG ATQ | ETT | 25/30 27/30 | N/A | 30/30 30/30 | N/A |
| Reena, 2019 | India | 100 | Normal | MCL KV | ETT (7/8 mm) | 37/50 46/50 | 40.3 ± 14.4 28.7 ± 10.6 | 41/50 48/50 | N/A |
| Russell, 2013 | Canada | 70 | Normal | MCL GVL | ETT* | 32/35 29/35 | N/A | N/A | 2/35 5/35 |
| Sahajanandan, 2019 | India | 63 | Difficult | KV CMD | ETT | 23/31 27/32 | 50.04 ± 24.17 46.93 ± 26.54 | N/A | N/A |
| Sargin, 2016 | Turkey | 100 | Normal | MCL MG | ETT (7/7.5 mm) | 50/50 50/50 | N/A | N/A | N/A |
| Sarkilar, 2015 | Turkey | 110 | All | MCL CM | ETT (8/9 mm) | 55/55 55/55 | N/A | 49/55 53/55 | N/A |
| Serocki, 2013 | Germany | 96 | All | MCL CMD GVL | ETT (7/8 mm) | 27/32 27/32 29/32 | N/A | N/A | N/A |
| Shah, 2016 | India | 60 | All | MCL CMD | ETT* (35/37/39 Fr) | 16/30 26/30 | 81.41 ± 19.7 88.75 ± 14.33 | 19/30 26/30 | N/A |
| Shravanalakshmi, 2017 | India | 90 | Difficult | CM KV | ETT (7/8 mm) | 45/45 42/45 | N/A | 45/45 45/45 | N/A |
| Siddiqui, 2009 | Canada | 40 | Normal | MCL GVL | ETT (7/8 mm) | N/A | N/A | N/A | 2/20 4/20 |
| Sun, 2005 | Canada | 200 | All | MCL GVL | ETT | 97/100 94/100 | N/A | 82/100 85/100 | N/A |
| Taylor, 2013 | Canada | 88 | All | MCL MG | ETT (7/7.5 mm) | 26/44 44/44 | 21.7 ± 9.4 35.8 ± 20.4 | 1/44 44/44 | 8/44 5/44 |
| Tempe, 2016 | India | 39 | Normal | MCL MG | ETT | 17/19 14/20 | 24.53 ± 10.9 52.3 ± 28.1 | 18/19 20/20 | N/A |
| Teoh, 2009 | Singapore | 140 | All | AWS GVL | ETT (7 mm) | 61/70 64/70 | N/A | 70/70 70/70 | 0/70 13/70 |
| Teoh, 2010 | Singapore | 400 | All | MCL AWS CM GVL | ETT (7 mm) | 98/100 95/100 93/100 91/100 | N/A | 95/100 100/100 98/100 99/100 | 3/100 1/100 8/100 15/100 |
| Toker, 2019 | Turkey | 100 | Difficult | MCL MG | ETT | N/A | 40.1 ± 5.4 34.7 ± 5.2 | 37/50 48/50 | N/A |
| Tolon, 2012 | Egypt | 40 | Difficult | MCL ATQ | ETT | 20/20 20/20 | 48.75 ± 21.57 34.3 ± 12.27 | 17/20 20/20 | 1/20 0/20 |
| Tosh, 2018 | India | 130 | Normal | MCL CMD | ETT (7/8 mm) | 54/65 53/65 | N/A | N/A | 44/65 0/65 |
| Turkstra, 2016 | Canada | 160 | Normal | MCL GVL | ETT (7/7.5/8/8.5 mm) | 76/80 74/80 | 48.2 ± 17.1 51.5 ± 21.8 | 79/80 78/80 | N/A |
| Varsha, 2019 | India | 70 | Normal | MCL ATQ | ETT (7/7.5/8/8.5 mm) | 33/35 35/35 | 31 ± 37.1 27 ± 29.37 | 24/35 35/35 | N/A |
| Vijayakumar, 2016 | India | 90 | Difficult | MCL ATQ | ETT (7/8 mm) | N/A | N/A | 33/45 45/45 | N/A |
| Wan, 2016 | China | 87 | Normal | ATQ MG | ETT* (35/37/39 Fr) | 40/43 42/44 | 28.6 ± 13.6 39.9 ± 9.1 | 43/43 44/44 | 8/43 5/44 |
| Wasem, 2013 | Germany | 60 | All | MCL ATQ | ETT* (35/37/39/41 Fr) | 26/30 28/30 | N/A | 30/30 30/30 | 6/30 7/30 |
| Wasinwong, 2017 | Thailand | 46 | Difficult | MCL GVL | ETT (7.5/8 mm) | 21/23 23/23 | N/A | N/A | N/A |
| Woo, 2012 | South Korea | 159 | All | MCL AWS | ETT (7/8 mm) | 50/109 50/50 | N/A | N/A | 26/109 29/50 |
| Xue, 2007 | China | 57 | Difficult | MCL GVL | ETT (7/7.5 mm) | 27/27 28/30 | N/A | N/A | N/A |
| Yao, 2015 | China | 96 | All | MCL MG | ETT* (35/37/39 Fr) | 48/48 48/48 | 24.3 ± 7.1 29.7 ± 10.5 | 48/48 48/48 | 6/48 8/48 |
| Yi, 2015 | China | 70 | Normal | ATQ GVL | ETT* (35/37/39 Fr) | 33/35 34/35 | N/A | 28/35 35/35 | 6/35 8/35 |
| Yoo, 2018 | Korea | 44 | Difficult | MCL MG | ETT* (35/37 Fr) | 17/22 21/22 | 52.7 ± 11.1 45 ± 11.1 | 12/22 21/22 | N/A |
| Yumul, 2016 | USA | 60 | Difficult | GVL MG | ETT | 28/30 21/30 | 69 ± 34 62 ± 31 | 28/30 30/30 | 7/30 11/30 |
| Participants (Studies) | Intervention | Comparison | Airway Status | Study Event Rates (%) | Relative Effect (95% CI) | Anticipated Absolute Effects | |||
|---|---|---|---|---|---|---|---|---|---|
| Comparison | Intervention | Risk with Comparison | Risk Difference with Intervention | ||||||
| Success | 778 (9 RCTs) | ATQ | MCL | Difficult | 285/388 (73.5%) | 360/390 (92.3%) | OR 3.06 (1.39 to 6.72) | 735 per 1000 | 160 more per 1000 (from 59 more to 214 more) |
| 684 (7 RCTs) | KV | MCL | All | 250/342 (73.1%) | 315/342 (92.1%) | OR 2.01 (1.01 to 4.01) | 731 per 1000 | 114 more per 1000 (from 2 more to 185 more) | |
| 300 (2 RCTs) | KV | MCL | Difficult | 80/150 (53.3%) | 137/150 (91.3%) | OR 3.31 (1.14 to 9.56) | 533 per 1000 | 258 more per 1000 (from 32 more to 383 more) | |
| 306 (4 RCTs) | CMD | MCL | All | 123/153 (80.4%) | 132/153 (86.3%) | OR 2.36 (1.06 to 5.26) | 804 per 1000 | 102 more per 1000 (from 9 more to 152 more) | |
| 93 (2 RCTs) | MCL | MG | Difficult | 45/46 (97.8%) | 35/47 (74.5%) | OR 0.25 (0.08 to 0.76) | 978 per 1000 | 60 fewer per 1000 (from 196 fewer to 7 fewer) | |
| 1972 (21 RCTs) | GVL | MCL | All | 918/990 (92.7%) | 897/982 (91.3%) | OR 1.59 (1.00 to 2.54) | 927 per 1000 | 26 more per 1000 (from 0 fewer to 43 more) | |
| 504 (7 RCTs) | GVL | MCL | Difficult | 237/251 (94.4%) | 240/253 (94.9%) | OR 2.68 (1.23 to 5.81) | 944 per 1000 | 34 more per 1000 (from 10 more to 46 more) | |
| Intubation time | 240 (1 RCT) | ATQ | CMD | All | 120 | 120 | - | - | SMD 0.58 SD lower (0.83 lower to 0.32 lower) |
| 240 (1 RCT) | ATQ | CMD | Difficult | 120 | 120 | - | - | SMD 0.58 SD lower (0.83 lower to 0.32 lower) | |
| 43 (1 RCT) | ATQ | KV | Normal | 22 | 21 | - | - | SMD 1.14 SD higher (0.49 higher to 1.79 higher) | |
| 240 (1 RCT) | ATQ | KV | Difficult | 120 | 120 | - | - | SMD 0.62 SD lower (0.88 lower to 0.37 lower) | |
| 42 (1 RCT) | ATQ | GVL | Normal | 21 | 21 | - | - | SMD 2.43 SD higher (1.62 higher to 3.24 higher) | |
| 240 (1 RCT) | ATQ | GVL | Difficult | 120 | 120 | - | - | SMD 0.71 SD lower (0.97 lower to 0.45 lower) | |
| 327 (2 RCTs) | ATQ | MG | All | 164 | 163 | - | - | SMD 0.67 SD lower (1.2 lower to 0.14 lower) | |
| 87 (1 RCT) | ATQ | MG | Normal | 44 | 43 | - | - | SMD 0.97 SD lower (1.42 lower to 0.52 lower) | |
| 240 (1 RCT) | ATQ | MG | Difficult | 120 | 120 | - | - | SMD 0.43 SD lower (0.68 lower to 0.17 lower) | |
| 45 (1 RCT) | AWS | MCL | All | 23 | 22 | - | - | SMD 0.89 SD lower (1.5 lower to 0.27 lower) | |
| 70 (1 RCT) | AWS | GVL | All | 35 | 35 | - | - | SMD 0.97 SD lower (1.47 lower to 0.48 lower) | |
| 70 (1 RCT) | AWS | GVL | Difficult | 35 | 35 | - | - | SMD 0.97 SD lower (1.47 lower to 0.48 lower) | |
| 78 (1 RCT) | CM | MCL | Normal | 39 | 39 | - | - | SMD 1.53 SD lower (2.04 lower to 1.02 lower) | |
| 90 (1 RCT) | CM | MCL | Difficult | 45 | 45 | - | - | SMD 0.76 SD lower (1.19 lower to 0.33 lower) | |
| 56 (1 RCT) | GVL | MG | Normal | 28 | 28 | - | - | SMD 0.81 SD lower (1.36 lower to 0.27 lower) | |
| 300 (2 RCTs) | GVL | MG | Difficult | 150 | 150 | - | - | SMD 0.32 SD higher (0.1 higher to 0.55 higher) | |
| 193 (3 RCTs) | MCL | MG | Difficult | 96 | 97 | - | - | SMD 0.92 SD higher (0.62 higher to 1.22 higher) | |
| 43 (1 RCT) | GVL | KV | Normal | 22 | 21 | - | - | SMD 0.82 SD lower (1.44 lower to 0.19 lower) | |
| 60 (1 RCT) | GVL | MCL | Difficult | 30 | 30 | - | - | SMD 0.6 SD lower (1.12 lower to 0.08 lower) | |
| Glottic view | 1400 (16 RCTs) | ATQ | MCL | All | 492/697 (70.6%) | 674/703 (95.9%) | OR 45.41 (2.29 to 902.16) | 706 per 1000 | 285 more per 1000 (from 140 more to 294 more) |
| 1014 (10 RCTs) | AWS | MCL | All | 441/524 (84.2%) | 483/490 (98.6%) | OR 8.60 (1.01 to 73.79) | 842 per 1000 | 137 more per 1000 (from 1 more to 156 more) | |
| 711 (6 RCTs) | AWS | MCL | Difficult | 295/355 (83.1%) | 349/356 (98.0%) | OR 49.84 (3.97 to 626.44) | 831 per 1000 | 165 more per 1000 (from 120 more to 169 more) | |
| Safety | 313 (5 RCTs) | ATQ | GVL | All | 112/156 (71.8%) | 127/157 (80.9%) | OR 7.92 (1.93 to 32.47) | 718 per 1000 | 235 more per 1000 (from 113 more to 270 more) |
| 181 (3 RCTs) | ATQ | GVL | Normal | 61/90 (67.8%) | 78/91 (85.7%) | OR 2.78 (1.13 to 6.81) | 678 per 1000 | 176 more per 1000 (from 26 more to 257 more) | |
| 190 (3 RCTs) | ATQ | MCL | Normal | 37/94 (39.4%) | 55/96 (57.3%) | OR 3.13 (1.26 to 7.80) | 394 per 1000 | 277 more per 1000 (from 56 more to 441 more) | |
| 353 (3 RCTs) | CM | MCL | All | 168/175 (96.0%) | 162/178 (91.0%) | RR 7.49 (1.62 to 34.61) | 960 per 1000 | 1000 more per 1000 (from 595 more to 1000 more) | |
| 130 (1 RCT) | CMD | MCL | Normal | 21/65 (32.3%) | 65/65 (100.0%) | OR 271.14 (13.2 to 5568.91) | 323 per 1000 | 669 more per 1000 (from 540 more to 677 more) | |
| 60 (1 RCT) | GVL | MG | All | 19/30 (63.3%) | 23/30 (76.7%) | OR 0.07 (0.01 to 0.61) | 633 per 1000 | 525 fewer per 1000 (from 616 fewer to 120 fewer) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.; Cho, Y.; Kim, W.; Choi, K.-S.; Jang, B.-H.; Shin, H.; Ahn, C.; Kim, J.G.; Na, M.K.; Lim, T.H.; et al. Comparisons of Videolaryngoscopes for Intubation Undergoing General Anesthesia: Systematic Review and Network Meta-Analysis of Randomized Controlled Trials. J. Pers. Med. 2022, 12, 363. https://doi.org/10.3390/jpm12030363
Lee J, Cho Y, Kim W, Choi K-S, Jang B-H, Shin H, Ahn C, Kim JG, Na MK, Lim TH, et al. Comparisons of Videolaryngoscopes for Intubation Undergoing General Anesthesia: Systematic Review and Network Meta-Analysis of Randomized Controlled Trials. Journal of Personalized Medicine. 2022; 12(3):363. https://doi.org/10.3390/jpm12030363
Chicago/Turabian StyleLee, Juncheol, Youngsuk Cho, Wonhee Kim, Kyu-Sun Choi, Bo-Hyoung Jang, Hyungoo Shin, Chiwon Ahn, Jae Guk Kim, Min Kyun Na, Tae Ho Lim, and et al. 2022. "Comparisons of Videolaryngoscopes for Intubation Undergoing General Anesthesia: Systematic Review and Network Meta-Analysis of Randomized Controlled Trials" Journal of Personalized Medicine 12, no. 3: 363. https://doi.org/10.3390/jpm12030363