
Analysis of the Efficacy of Universal Screening of Coronavirus Disease with Antigen-Detecting Rapid Diagnostic Tests at Point-or-Care Settings and Sharing the Experience of Admission Protocol—A Pilot Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocols for Admission to Our Hospital
- (1)
- Emergency department
- (2)
- Out-patient department
- (3)
- Operation room
2.2. Radiologic Evaluations
2.3. Statistical Analysis
3. Results
3.1. Demographics and Diagnostic Values of Ag-RDT and LDCT for High Risk of Screening Patients
3.2. Results of Laboratory Test including Ct Values of RT-PCR
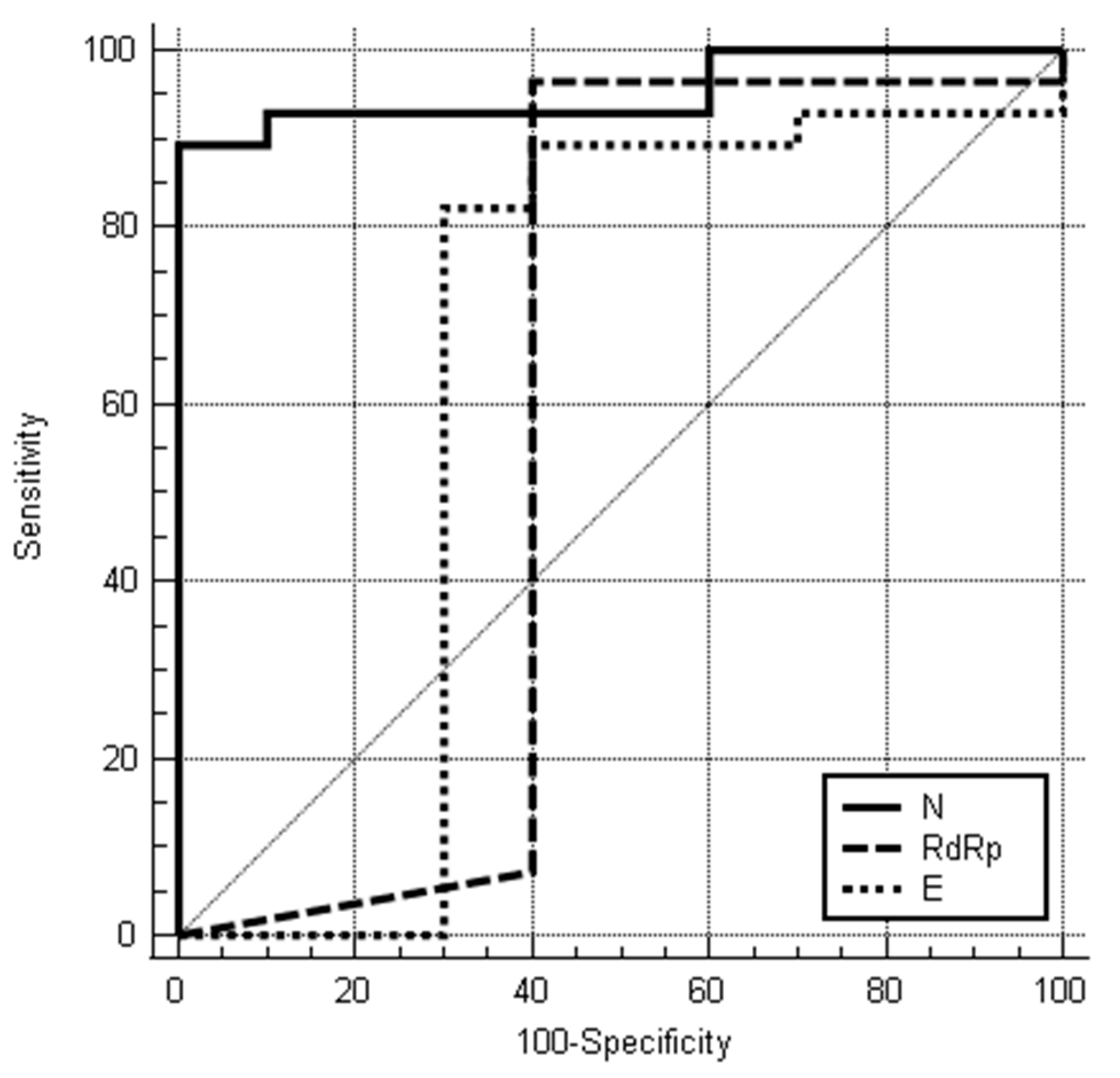
3.3. Results of Ag-RDT Compared to Ct Values of Each Gene through RT-PCR
3.4. Radiologic Findings on LDCT
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- The, L. Facing up to long COVID. Lancet 2020, 396, 1861. [Google Scholar] [CrossRef]
- Kim, J.Y.; Choe, P.G.; Oh, Y.; Oh, K.J.; Kim, J.; Park, S.J.; Park, J.H.; Na, H.K.; Oh, M.-D. The First Case of 2019 Novel Coronavirus Pneumonia Imported into Korea from Wuhan, China: Implication for Infection Prevention and Control Measures. J. Korean Med. Sci. 2020, 35, e61. [Google Scholar] [CrossRef] [PubMed]
- Ji, W.; Huh, K.; Ko, K.-P.; Im, J.-S.; Jung, J.; Kang, M.; Hong, J.; Bae, G.H.; Lee, R.; Na, Y.; et al. Effect of Underlying Comorbidities on the Infection and Severity of COVID-19 in Korea: A Nationwide Case-Control Study. J. Korean Med. Sci. 2020, 35, e237. [Google Scholar] [CrossRef] [PubMed]
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Pan, J.; Pang, J.; Zhong, Z.; Li, H.; He, C.; Zhang, J.; Zhao, C. Clinical characteristics of 3062 COVID-19 patients: A meta-analysis. J. Med. Virol. 2020, 92, 1902–1914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cui, X.; Zhao, Z.; Zhang, T.; Guo, W.; Guo, W.; Zheng, J.; Zhang, J.; Dong, C.; Na, R.; Zheng, L.; et al. A systematic review and meta-analysis of children with coronavirus disease 2019 (COVID-19). J. Med. Virol. 2020, 93, 1057–1069. [Google Scholar] [CrossRef]
- Bullard, J.; Dust, K.; Funk, D.; Strong, J.E.; Alexander, D.; Garnett, L.; Boodman, C.; Bello, A.; Hedley, A.; Schiffman, Z.; et al. Predicting Infectious Severe Acute Respiratory Syndrome Coronavirus 2 From Diagnostic Samples. Clin. Infect. Dis. 2020, 71, 2663–2666. [Google Scholar] [CrossRef]
- Gniazdowski, V.; Morris, C.P.; Wohl, S.; Mehoke, T.; Ramakrishnan, S.; Thielen, P.; Powellet, H.; Smith, B.; Armstrong, D.; Herrera, M.; et al. Repeat COVID-19 Molecular Testing: Correlation of SARS-CoV-2 Culture with Molecular Assays and Cycle Thresholds. Clin. Infect. Dis. 2020, 73, e860–e869. [Google Scholar] [CrossRef]
- Jefferson, T.; Spencer, E.A.; Brassey, J.; Heneghan, C. Viral cultures for COVID-19 infectious potential assessment—A systematic review. Clin. Infect. Dis. 2020, 73, e3884–e3899. [Google Scholar] [CrossRef]
- Young, B.E.; Ong, S.W.X.; Ng, L.F.P.; Anderson, D.E.; Chia, W.N.; Chia, P.Y.; Ang, L.W.; Mak, T.-M.; Kalimuddin, S.; Chai, L.Y.A.; et al. Viral dynamics and immune correlates of COVID-19 disease severity. Clin. Infect. Dis. 2020, 73, e2932–e2942. [Google Scholar] [CrossRef] [PubMed]
- La Scola, B.; Le Bideau, M.; Andreani, J.; Hoang, V.T.; Grimaldier, C.; Colson, P.; Gautret, P.; Raoult, D. Viral RNA load as determined by cell culture as a management tool for discharge of SARS-CoV-2 patients from infectious disease wards. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 1059–1061. [Google Scholar] [CrossRef]
- Young, S.; Taylor, S.N.; Cammarata, C.L.; Varnado, K.G.; Roger-Dalbert, C.; Montano, A.; Griego-Fullbright, C.; Burgard, C.; Fernandez, C.; Eckert, K.; et al. Clinical Evaluation of BD Veritor SARS-CoV-2 Point-of-Care Test Performance Compared to PCR-Based Testing and versus the Sofia 2 SARS Antigen Point-of-Care Test. J. Clin. Microbiol. 2020, 59, e02338-20. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Kim, S.Y.; Huh, H.J.; Kim, N.; Sung, H.; Lee, H.; Roh, K.H.; Kim, T.S.; Hong, A.K.H. Clinical Performance of the Standard Q COVID-19 Rapid Antigen Test and Simulation of its Real-World Application in Korea. Ann. Lab. Med. 2021, 41, 588–592. [Google Scholar] [CrossRef] [PubMed]
- Prince-Guerra, J.L.; Almendares, O.; Nolen, L.D.; Gunn, J.K.L.; Dale, A.P.; Buono, S.A.; Deutsch-Feldman, M.; Suppiah, S.; Hao, L.; Zeng, Y.; et al. Evaluation of Abbott BinaxNOW Rapid Antigen Test for SARS-CoV-2 Infection at Two Community-Based Testing Sites—Pima County, Arizona, 3–17 November 2020. MMWR. Morb. Mortal. Wkly. Rep. 2021, 70, 100–105. [Google Scholar] [CrossRef] [PubMed]
- Larke, F.J.; Kruger, R.L.; Cagnon, C.H.; Flynn, M.J.; McNitt-Gray, M.M.; Wu, X.; Judy, P.F.; Cody, D.D. Estimated Radiation Dose Associated with Low-Dose Chest CT of Average-Size Participants in the National Lung Screening Trial. Am. J. Roentgenol. 2011, 197, 1165–1169. [Google Scholar] [CrossRef] [PubMed]
- Hansell, D.M.; Bankier, A.A.; MacMahon, H.; McLoud, T.C.; Müller, N.L.; Remy, J. Fleischner Society: Glossary of Terms for Thoracic Imaging. Radiology 2008, 246, 697–722. [Google Scholar] [CrossRef] [Green Version]
- Simpson, S.; Kay, F.U.; Abbara, S.; Bhalla, S.; Chung, J.H.; Chung, M.; Henry, T.S.; Kanne, J.P.; Kligerman, S.; Ko, J.P.; et al. Radiological Society of North America Expert Consensus Document on Reporting Chest CT Findings Related to COVID-19: Endorsed by the Society of Thoracic Radiology, the American College of Radiology, and RSNA. Radiol. Cardiothorac. Imaging 2020, 2, e200152. [Google Scholar] [CrossRef] [Green Version]
- Pekosz, A.; Parvu, V.; Li, M.; Andrews, J.C.; Manabe, Y.C.; Kodsi, S.; Gary, D.S.; Roger-Dalbert, C.; Leitch, J.; Cooper, C.K. Antigen-Based Testing but Not Real-Time Polymerase Chain Reaction Correlates with Severe Acute Respiratory Syndrome Coronavirus 2 Viral Culture. Clin. Infect. Dis. 2021, 73, e2861–e2866. [Google Scholar] [CrossRef]
- Porte, L.; Legarraga, P.; Vollrath, V.; Aguilera, X.; Munita, J.M.; Araos, R.; Pizarro, G.; Vial, P.; Iruretagoyena, M.; Dittrich, S.; et al. Evaluation of a novel antigen-based rapid detection test for the diagnosis of SARS-CoV-2 in respiratory samples. Int. J. Infect. Dis. 2020, 99, 328–333. [Google Scholar] [CrossRef]
- Waller, J.V.; Kaur, P.; Tucker, A.; Lin, K.K.; Diaz, M.; Henry, T.S.; Hope, M. Diagnostic Tools for Coronavirus Disease (COVID-19): Comparing CT and RT-PCR Viral Nucleic Acid Testing. Am. J. Roentgenol. 2020, 215, 834–838. [Google Scholar] [CrossRef]
- Kucharik, M.P.; Rudisill, S.S.; Meek, W.M.; Martin, S.D. Elective Orthopaedic Surgery in the Era of COVID-19: Summary of Current Guidelines and Road Map to Resuming and Sustaining Safe Practice. JBJS Rev. 2021, 9, e20.00193. [Google Scholar] [CrossRef] [PubMed]
- Parvizi, J.; Gehrke, T.; Krueger, C.; Chisari, E.; Citak, M.; Van Onsem, S.; Walter, W. Resuming Elective Orthopaedic Surgery During the COVID-19 Pandemic. J. Bone Jt. Surg. Am. Vol. 2020, 102, 1205–1212. [Google Scholar] [CrossRef] [PubMed]
- Mouton, C.; Hirschmann, M.T.; Ollivier, M.; Seil, R.; Menetrey, J. COVID-19—ESSKA guidelines and recommendations for resuming elective surgery. J. Exp. Orthop. 2020, 7, 28. [Google Scholar] [CrossRef]
- Moverman, M.A.; Puzzitiello, R.N.; Pagani, N.R.; Barnes, C.L.; Jawa, A.; Menendez, M.E. Public Perceptions of Resuming Elective Surgery During the COVID-19 Pandemic. J. Arthroplast. 2020, 36, 397–402.e2. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-H.; Jang, J.-S.; Chung, J.-W.; Kwon, J.-T.; Park, Y.-S. Clinical Pathway for Emergency Brain Surgery during COVID-19 Pandemic and Its Impact on Clinical Outcomes. J. Korean Med. Sci. 2021, 36, e16. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| RT-PCR Positive, n = 41 | RT-PCR Negative, n = 605 | p-Value | |
|---|---|---|---|
| Ag-RDT | <0.001 | ||
| Positive | 28 | 3 | |
| Negative | 13 | 602 | |
| Sex | 0.868 | ||
| Male | 21 | 318 | |
| Female | 20 | 287 | |
| Age (mean±SD) | 70.1 ± 13.1 | 63.4 ± 19.9 | 0.033 |
| Body mass index | 22.4 ± 3.1 | 23.4 ± 4.0 | 0.122 |
| Symptoms | |||
| Fever | 37.7 ± 0.8 | 36.8 ± 0.7 | <0.001 |
| Cough | 17 | 13 | <0.001 |
| Sputum | 10 | 29 | <0.001 |
| Myalgia | 11 | 9 | <0.001 |
| Rhinorrhea | 0 | 4 | 1.000 |
| Dyspnea | 17 | 91 | <0.001 |
| Nausea/Vomiting | 3 | 57 | 0.206 |
| Headache | 25 | 174 | <0.001 |
| Comorbidities | |||
| Diabetes mellitus | 11 | 148 | 0.734 |
| Hypertension | 24 | 262 | 0.057 |
| Ischemic heart disease | 3 | 32 | 0.579 |
| Renal insufficiency | 1 | 20 | 0.762 |
| Neurological disease | 3 | 32 | 0.579 |
| Asthma | 1 | 15 | 1.000 |
| Ag-RDT | LDCT | Ag-RDT + LDCT | ||
|---|---|---|---|---|
| All Patients | Symptomatic Patients | Symptomatic Patients | Symptomatic Patients | |
| Sensitivity, % | 68.3 | 73.0 | 48.6 | 91.8 |
| Specificity, % | 99.5 | 98.8 | 98.7 | 98.7 |
| Positive Predictive value, % | 90.3 | 87.1 | 81.8 | 89.5 |
| Negative Predictive value, % | 97.9 | 96.9 | 94.3 | 99.1 |
| RT-PCR Positive, n = 41 (%) | RT-PCR Negative, n = 605 (%) | p-Value | |
|---|---|---|---|
| WBC, 109/L | 7.83 ± 5.84 | 9.84 ± 4.74 | 0.010 |
| Neutrophil (%) | 71.2 ± 15.1 | 73.4 ± 14.4 | 0.344 |
| Lymphocyte (%) | 19.1 ± 11.9 | 18.3 ± 12.2 | 0.670 |
| Platelet, 109/L | 217.2 ± 84.4 | 237.4 ± 82.7 | 0.131 |
| CRP, mg/L | 5.78 ± 7.52 | 3.76 ± 6.64 | 0.061 |
| Ct values of RT-PCR, (mean±standard deviations(SD)) | |||
| RdRp gene | 17.95 ± 10.66 | ||
| E gene | 20.17 ± 9.87 | ||
| N gene | 20.54 ± 10.47 | ||
| Ct values of RT-PCR according to the Ag-RDT results, (mean±SD) | |||
| RdRp gene | 0.668 | ||
| Positive Ag-RDT, n = 28 | 17.30 ± 7.23 | ||
| Negative Ag-RDT, n = 13 | 19.35 ± 16.08 | ||
| E gene | 0.263 | ||
| Positive Ag-RDT, n= 28 | 18.68 ± 7.31 | ||
| Negative Ag-RDT, n= 13 | 23.39 ± 13.71 | ||
| N gene | <0.001 | ||
| Positive Ag-RDT, n = 28 | 16.29 ± 8.60 | ||
| Negative Ag-RDT, n = 13 | 32.43 ± 4.01 | ||
| Chest CT findings, n = 355 | n = 37 | n = 318 | |
| No pneumonia | 15 (40.5) | 248 (78.0) | <0.001 |
| Any type of pneumonia | 22 (59.5) | 70 (22.0) | |
| Any COVID-19 typical findings | 18 | 4 | <0.001 |
| Involvement of the lesion | 0.299 | ||
| Single lobe | 4 | 11 | |
| Multilobular | 18 | 59 | |
| Numbers of involved lobe | 3.77 ± 1.72 | 3.43 ± 1.47 | 0.370 |
| Laterality | 0.952 | ||
| Rt | 4 | 13 | |
| Lt | 2 | 5 | |
| Both | 16 | 52 | |
| Cephalocaudal distribution | 0.407 | ||
| Upper | 1 | 1 | |
| Middle | 1 | 0 | |
| Lower | 5 | 20 | |
| Diffuse | 15 | 49 | |
| Axial distribution† | 0.115 | ||
| Central | 1 | 3 | |
| Peripheral | 13 | 26 | |
| Diffuse | 8 | 41 | |
| Density | <0.001 | ||
| GGO | 11 (50.0) | 13 (18.6) | |
| Crazy-paving pattern | 3 (13.6) | 2 (2.9) | |
| Mixed GGO and consolidation | 7 (31.8) | 17 (24.3) | |
| Consolidation | 1 (4.5) | 38 (54.3) | |
| AUC | 95%CI of AUC | Cut-off | Sensitivity, % | Specificity, % | p-Value | |
|---|---|---|---|---|---|---|
| RdRp | 0.610 | 0.445–0.758 | ≤25.16 | 96.4 | 61.5 | 0.408 |
| E gene | 0.695 | 0.532–0.829 | ≤24.2 | 82.1 | 76.9 | 0.096 |
| N gene | 0.954 | 0.831–0.995 | ≤25.67 | 89.3 | 100 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, J.Y.; Lee, J.H.; Cha, B.K.; Kim, B.-S.; Lee, H.-J.; Kim, G.H.; Kang, K.-T.; Lee, Y.-S.; Ahn, S.K.; Kim, S.H. Analysis of the Efficacy of Universal Screening of Coronavirus Disease with Antigen-Detecting Rapid Diagnostic Tests at Point-or-Care Settings and Sharing the Experience of Admission Protocol—A Pilot Study. J. Pers. Med. 2022, 12, 319. https://doi.org/10.3390/jpm12020319
Park JY, Lee JH, Cha BK, Kim B-S, Lee H-J, Kim GH, Kang K-T, Lee Y-S, Ahn SK, Kim SH. Analysis of the Efficacy of Universal Screening of Coronavirus Disease with Antigen-Detecting Rapid Diagnostic Tests at Point-or-Care Settings and Sharing the Experience of Admission Protocol—A Pilot Study. Journal of Personalized Medicine. 2022; 12(2):319. https://doi.org/10.3390/jpm12020319
Chicago/Turabian StylePark, Ji Young, Joo Hee Lee, Bong Ki Cha, Boo-Seop Kim, Han-Jun Lee, Gi Hyeon Kim, Kyu-Tae Kang, Yong-Soon Lee, Seok Keun Ahn, and Seong Hwan Kim. 2022. "Analysis of the Efficacy of Universal Screening of Coronavirus Disease with Antigen-Detecting Rapid Diagnostic Tests at Point-or-Care Settings and Sharing the Experience of Admission Protocol—A Pilot Study" Journal of Personalized Medicine 12, no. 2: 319. https://doi.org/10.3390/jpm12020319