
Effects of Pain Neuroscience Education Combined with Lumbar Stabilization Exercise on Strength and Pain in Patients with Chronic Low Back Pain: Randomized Controlled Trial



Abstract
:1. Introduction
2. Materials and Methods
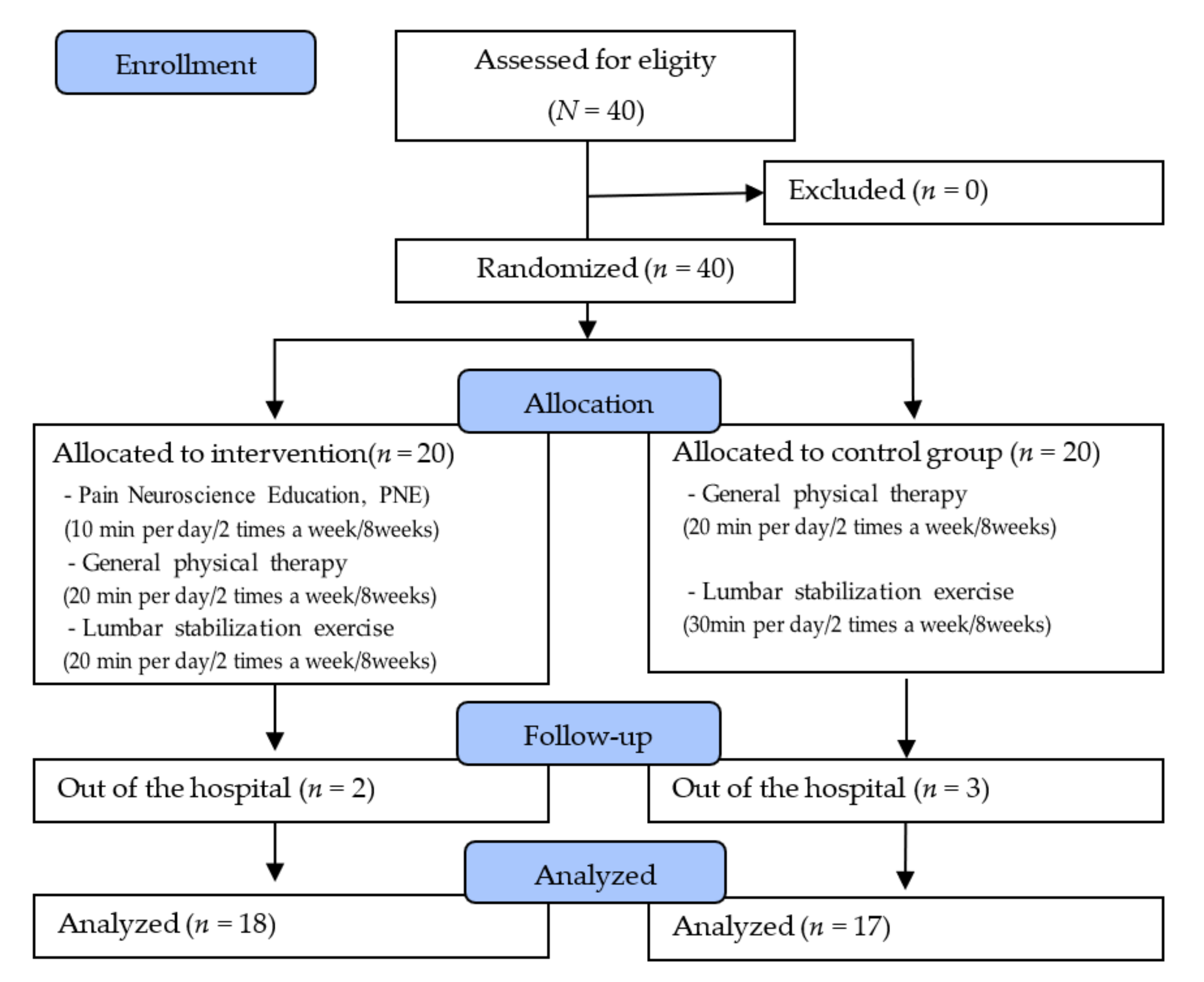
2.1. Participants
2.2. Experimental Procedures
2.2.1. Pain Neuroscience Education
2.2.2. LSE Training
2.3. Outcome Measurements
2.3.1. Primary Outcome: Muscle Strength
2.3.2. Primary Outcome: Pain
2.3.3. Secondary Outcome: Flexibility
2.3.4. Secondary Outcome: Activity Disorder Index
2.4. Statistical Analysis
3. Results
3.1. Muscle Strength
3.2. Pain
3.3. Flexibility
3.4. Activity Disorder
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- U.S. Department of Health and Human Services-National Institutes of Health. Low Back Pain Fact Sheet. Available online: https://www.ninds.nih.gov/Disorders/Patient-Caregiver-Education/Fact-Sheets/Low-Back-Pain-Fact-Sheet. (accessed on 11 November 2020).
- Meucci, R.D.; Fassa, A.G.; Faria, N.M.X. Prevalence of chronic low back pain: Systematic review. Rev. Saude Publica 2015, 49, 1. [Google Scholar] [CrossRef] [PubMed]
- Hicks, G.E.; Fritz, J.M.; Delitto, A.; McGill, S.M. Preliminary Development of a Clinical Prediction Rule for Determining Which Patients With Low Back Pain Will Respond to a Stabilization Exercise Program. Arch. Phys. Med. Rehabil. 2005, 86, 1753–1762. [Google Scholar] [CrossRef] [PubMed]
- Rozenberg, S. Chronic low back pain: Definition and treatment. Rev. Prat. 2008, 58, 265–272. [Google Scholar]
- Marshall, P.W.; Mannion, J.; Murphy, B.A. The eccentric, concentric strength relationship of the hamstring muscles in chronic low back pain. J. Electromyogr. Kinesiol. 2010, 20, 39–45. [Google Scholar] [CrossRef]
- Panjabi, M.M. Clinical spinal instability and low back pain. J. Electromyogr. Kinesiol. 2003, 13, 371–379. [Google Scholar] [CrossRef]
- Kofotolis, N.; Kellis, E. Effects of Two 4-Week Proprioceptive Neuromuscular Facilitation Programs on Muscle Endurance, Flexibility, and Functional Performance in Women With Chronic Low Back Pain. Phys. Ther. 2006, 86, 1001–1012. [Google Scholar] [CrossRef] [Green Version]
- Fritz, J.M.; Cleland, J.A.; Speckman, M.; Brennan, G.P.; Hunter, S.J. Physical therapy for acute low back pain: Associations with subsequent healthcare costs. Spine 2008, 33, 1800–1805. [Google Scholar] [CrossRef] [Green Version]
- Goubert, L.; Crombez, G.; Van Damme, S.; Vlaeyen, J.W.S.; Bijttebier, P.; Roelofs, J. Confirmatory factor analysis of the Tampa Scale for Kinesiophobia: Invariant two-factor model across low back pain patients and fibromyalgia patients. Clin. J. Pain. 2004, 20, 103–110. [Google Scholar] [CrossRef]
- Kader, D.; Wardlaw, D.; Smith, F. Correlation Between the MRI Changes in the Lumbar Multifidus Muscles and Leg Pain. Clin. Radiol. 2000, 55, 145–149. [Google Scholar] [CrossRef] [Green Version]
- Mulligan, B. The painful dysfunctional shoulder. A new treatment approach using ‘Mobilisation with Movement’. N. Z. J. Physiother. 2003, 31, 140–142. [Google Scholar]
- Troyanovich, S.J.; Harrison, N.D.; Harrison, D.E. Low back pain and the lumbar intervertebral disk: Clinical considerations for the doctor of chiropractic. J. Manip. Physiol. Ther. 1999, 22, 96–104. [Google Scholar] [CrossRef]
- Bender, T.; Németh, A.; Szekeres, L. Effect of thermal water and adjunctive electrotherapy on chronic low back pain: A double-blind, randomized, follow-up study. J. Rehabil. Med. 2009, 41, 73–79. [Google Scholar] [CrossRef] [Green Version]
- Kofotolis, N.; Sambanis, M. The influence of exercise on musculoskeletal disorders of the lumbar spine. J. Sports Med. Phys. Fit. 2005, 45, 84–92. [Google Scholar]
- Searle, A.; Spink, M.; Ho, A.; Chuter, V. Exercise interventions for the treatment of chronic low back pain: A systematic review and meta-analysis of randomised controlled trials. Clin. Rehabil. 2015, 29, 1155–1167. [Google Scholar] [CrossRef] [PubMed]
- Shnayderman, I.; Katz-Leurer, M. An aerobic walking programme versus muscle strengthening programme for chronic low back pain: A randomized controlled trial. Clin. Rehabil. 2013, 27, 207–214. [Google Scholar] [CrossRef]
- Kovacs, F.M.; Abraira, V.; Zamora, J.; Gil del Real, M.T.; Llobera, J.; Fernández, C. Correlation Between Pain, Disability, and Quality of Life in Patients With Common Low Back Pain. Spine 2004, 29, 206–210. [Google Scholar] [CrossRef] [PubMed]
- Luoto, S.; Aalto, H.; Taimela, S.; Hurri, H.; Pyykkö, I.; Alaranta, H. One-Footed and Externally Disturbed Two-Footed Postural Control in Patients With Chronic Low Back Pain and Healthy Control Subjects. Spine 1998, 23, 2081–2089. [Google Scholar] [CrossRef]
- Thomas, E.-N.; Pers, Y.-M.; Mercier, G.; Cambiere, J.-P.; Frasson, N.; Ster, F.; Hérisson, C.; Blotman, F. The importance of fear, beliefs, catastrophizing and kinesiophobia in chronic low back pain rehabilitation. Ann. Phys. Rehabil. Med. 2010, 53, 3–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Louw, A.; Puentedura, E.J.; Diener, I.; Zimney, K.J.; Cox, T. Pain neuroscience education: Which pain neuroscience education metaphor worked best? S. Afr. J. Physiother. 2019, 75, 1329. [Google Scholar] [CrossRef] [Green Version]
- Watson, J.A.; Ryan, C.G.; Cooper, L.; Ellington, D.; Whittle, R.; Lavender, M.; Dixon, J.; Atkinson, G.; Cooper, K.; Martin, D.J. Pain Neuroscience Education for Adults With Chronic Musculoskeletal Pain: A Mixed-Methods Systematic Review and Meta-Analysis. J. Pain. 2019, 20, 1140-e1. [Google Scholar] [CrossRef]
- Moseley, G.L. Widespread brain activity during an abdominal task markedly reduced after pain physiology education: fMRI evaluation of a single patient with chronic low back pain. Aust. J. Physiother. 2005, 51, 49–52. [Google Scholar] [CrossRef] [Green Version]
- Moseley, G.L. Evidence for a direct relationship between cognitive and physical change during an education intervention in people with chronic low back pain. Eur. J. Pain. 2004, 8, 39–45. [Google Scholar] [CrossRef]
- Van Oosterwijck, J.; Nijs, J.; Meeus, M.; Truijen, S.; Craps, J.; van den Keybus, N.; Paul, L. Pain neurophysiology education improves cognitions, pain thresholds and movement performance in people with chronic whiplash: A pilot study. J. Rehabil. Res. Dev. 2011, 48, 43–58. [Google Scholar] [CrossRef] [Green Version]
- Louw, A.; Farrell, K.; Choffin, B.; Foster, B.; Lunde, G.; Snodgrass, M.; Sweet, R.; Weitzel, M.; Wilder, R.; Puentedura, E.J. Immediate effect of pain neuroscience education for recent onset low back pain: An exploratory single arm trial. J. Man. Manip. Ther. 2019, 27, 267–276. [Google Scholar] [CrossRef] [Green Version]
- Marris, D.; Theophanous, K.; Cabezon, P.; Dunlap, Z.; Donaldson, M. The impact of combining pain education strategies with physical therapy interventions for patients with chronic pain: A systematic review and meta-analysis of randomized controlled trials. Physiother. Theory Pract. 2019, 37, 461–472. [Google Scholar] [CrossRef]
- Siddall, B.; Ram, A.; Jones, M.D.; Booth, J.; Perriman, D.; Summers, S.J. Short-term impact of combining pain neuroscience education with exercise for chronic musculoskeletal pain: A systematic review and meta-analysis. Pain 2021, 163, e20–e30. [Google Scholar] [CrossRef]
- Malfliet, A.; Kregel, J.; Meeus, M.; Roussel, N.; Danneels, L.; Cagnie, B.; Dolphens, M.; Nijs, J. Blended-Learning Pain Neuroscience Education for People With Chronic Spinal Pain: Randomized Controlled Multicenter Trial. Phys. Ther. 2017, 98, 357–368. [Google Scholar] [CrossRef]
- Butler, D.S.; Moseley, G.L. Explain Pain, 2nd ed.; NOI Group: Adelaide, Australia, 2013. [Google Scholar]
- Moseley, G.L. A pain neuromatrix approach to patients with chronic pain. Man. Ther. 2003, 8, 130–140. [Google Scholar] [CrossRef]
- Moseley, L. Combined physiotherapy and education is efficacious for chronic low back pain. Aust. J. Physiother. 2002, 48, 297–302. [Google Scholar] [CrossRef] [Green Version]
- Pardo, G.B.; Girbés, E.L.; Roussel, N.; Izquierdo, T.G.; Penick, V.J.; Pecos-Martin, D. Pain Neurophysiology Education and Therapeutic Exercise for Patients With Chronic Low Back Pain: A Single-Blind Randomized Controlled Trial. Arch. Phys. Med. Rehabilitation 2018, 99, 338–347. [Google Scholar] [CrossRef]
- Moon, H.J.; Choi, K.H.; Kim, D.H.; Kim, H.J.; Cho, Y.K.; Lee, K.H.; Kim, J.H.; Choi, Y.J. Effect of lumbar stabilization and dynamic lumbar strengthening exercises in patients with chronic low back pain. Ann. Rehabil. Med. 2013, 37, 110–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finch, E. Physical Rehabilitation Outcome Measures: A Guide to Enhanced Clinical Decision Making; BC Decker: Hamilton ON, Canada, 2002; p. 64. [Google Scholar]
- Mintken, P.E.; Glynn, P.; Cleland, J.A. Psychometric properties of the shortened disabilities of the Arm, Shoulder, and Hand Questionnaire (QuickDASH) and Numeric Pain Rating Scale in patients with shoulder pain. J. Shoulder Elb. Surg. 2009, 18, 920–926. [Google Scholar] [CrossRef] [PubMed]
- De Williams, A.C.; Davies, H.T.O.; Chadury, Y. Simple pain rating scales hide complex idiosyncratic meanings. Pain 2000, 85, 457–463. [Google Scholar] [CrossRef]
- Farrar, J.T.; Young, J.P., Jr.; LaMoreaux, L.; Werth, J.L.; Poole, R.M. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain 2001, 94, 149–158. [Google Scholar] [CrossRef]
- Ferraz, M.B.; Quaresma, M.R.; Aquino, L.R.; Atra, E.; Tugwell, P.; Goldsmith, C.H. Reliability of pain scales in the assessment of literate and illiterate patients with rheumatoid arthritis. J. Rheumatol. 1990, 17, 1022–1024. [Google Scholar]
- Sullivan, M.J.L.; Bishop, S.R.; Pivik, J. The Pain Catastrophizing Scale: Development and validation. Psychol. Assess. 1995, 7, 524. [Google Scholar] [CrossRef]
- Cho, S.; Kim, H.-Y.; Lee, J.-H. Validation of the Korean version of the Pain Catastrophizing Scale in patients with chronic non-cancer pain. Qual. Life Res. 2012, 22, 1767–1772. [Google Scholar] [CrossRef] [PubMed]
- Miller, R.P.; Kori, S.H.; Todd, D.D. The Tampa Scale: A Measure of Kinisophobia. Clin. J. Pain. 1991, 7, 51. [Google Scholar] [CrossRef]
- Tkachuk, G.A.; Harris, C.A. Psychometric Properties of the Tampa Scale for Kinesiophobia-11 (TSK-11). J. Pain 2012, 13, 970–977. [Google Scholar] [CrossRef]
- Tousignant, M.; Poulin, L.; Marchand, S.; Viau, A.; Place, C. The Modified-Modified Schober Test for range of motion assessment of lumbar flexion in patients with low back pain: A study of criterion validity, intra- and inter-rater reliability and minimum metrically detectable change. Disabil. Rehabil. 2005, 27, 553–559. [Google Scholar] [CrossRef]
- Perret, C.; Poiraudeau, S.; Fermanian, J.; Colau, M.M.L.; Benhamou, M.A.M.; Revel, M. Validity, reliability, and responsiveness of the fingertip-to-floor test. Arch. Phys. Med. Rehabil. 2001, 82, 1566–1570. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Lee, D.H.; Suh, K.T.; Kim, J.I.; Lim, J.M.; Goh, T.S. Validation of the Korean version of the Roland–Morris Disability Questionnaire. Eur. Spine J. 2011, 20, 2115–2119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andias, R.; Neto, M.; Silva, A.G. The effects of pain neuroscience education and exercise on pain, muscle endurance, catastrophizing and anxiety in adolescents with chronic idiopathic neck pain: A school-based pilot, randomized and controlled study. Physiother. Theory Pract. 2018, 34, 682–691. [Google Scholar] [CrossRef]
- Larsen, J.B.; Skou, S.T.; Arendt-Nielsen, L.; Simonsen, O.; Madeleine, P. Neuromuscular exercise and pain neuroscience education compared with pain neuroscience education alone in patients with chronic pain after primary total knee arthroplasty: Study protocol for the NEPNEP randomized controlled trial. Trials 2020, 21, 218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Childs, J.D.; Piva, S.R.; Fritz, J.M. Responsiveness of the Numeric Pain Rating Scale in Patients with Low Back Pain. Spine 2005, 30, 1331–1334. [Google Scholar] [CrossRef] [PubMed]
- George, S.Z.; Valencia, C.; Beneciuk, J.M. A Psychometric Investigation of Fear-Avoidance Model Measures in Patients With Chronic Low Back Pain. J. Orthop. Sports Phys. Ther. 2010, 2010. 40, 197–205. [Google Scholar] [CrossRef] [Green Version]
- Pires, D.; Cruz, E.; Caeiro, C. Aquatic exercise and pain neurophysiology education versus aquatic exercise alone for patients with chronic low back pain: A randomized controlled trial. Clin. Rehabil. 2014, 29, 538–547. [Google Scholar] [CrossRef]
- Nijs, J.; van Wilgen, C.P.; Van Oosterwijck, J.; van Ittersum, M.; Meeus, M. How to explain central sensitization to patients with ‘unexplained’ chronic musculoskeletal pain: Practice guidelines. Man. Ther. 2011, 16, 413–418. [Google Scholar] [CrossRef] [Green Version]
- Woby, S.R.; Watson, P.J.; Roach, N.K.; Urmston, M. Are changes in fear-avoidance beliefs, catastrophizing, and appraisals of control, predictive of changes in chronic low back pain and disability? Eur. J. Pain. 2004, 8, 201–210. [Google Scholar] [CrossRef]
- Roland, M.; Fairbank, J. The Roland–Morris Disability Questionnaire and the Oswestry Disability Questionnaire. Spine 2000, 25, 3115–3124. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Weekly Training Topics (Training Time: 10 min Each) | |
|---|---|
| 1. Neurophysiology of pain | Explain the basic theory of the structure of the brain and nerves, the peripheral nervous system, and the central nervous system by comparing to a mobile phone or computer. |
| 2. Nociception | Explain and compare concepts and differences between acute and chronic pain with real-world experiences and emphasize the importance of exercise. |
| 3. Nociceptive pathways | Explains the paths of pain sensation and noxious/innoxious pain sensations, and highlights how psychological aspects and thoughts affect pain. |
| 4. Neurons and synapses | Explain the structure and function of neurons and synapses, the processes of electrical signals, and how the patient’s thoughts can influence these signaling processes. |
| 5. Action potential | Describe action potentials and thresholds, and differences in sensations felt by each person by comparing them to signals and alarms generated by the body. |
| 6. Spinal inhibition and facilitation | Explain the process of inhibition and promotion of the spine by comparing the process of electrical signal transmission and homeostasis and emphasize the change in sensation according to the state of the body. |
| 7. Sensitization | Explain the types of sensations, the process of transmitting each sensation, and the differences, and emphasize the understanding of pain through the gate control theory. |
| 8. Plasticity of the nervous system | Explain the basic concept of neuroplasticity in relation to changes in the brain caused by experience and learning and emphasize positive changes through exercise. |
| Item | Training Method |
|---|---|
| Hamstring stretching | In the supine position, place a towel under the sole of the foot, hold the ends of the towel with both hands, extend the knee, lift the leg, and repeat the stretching five times. |
| Abdominal stretching | In the prone position, place both hands on the floor, stretch the elbows and lift the upper body, and repeat the abdominal muscle stretching five times. |
| Quadriceps stretching | In the lying position, bend one knee, pull back the lower leg with the arm of the same side, and repeat the stretching five times. |
| Cat–camel | In the crawling position, contract the abdominal muscles and bend and open the back five times. |
| Neutral position | In the knee-bent and lying position, pull the abdominal muscles to contract the transverse abdominal muscles and the pelvic floor muscles isometrically, and maintain for 5 s. Repeat five times. |
| Curl up | In the knee-bent and lying position, up the trunk to contract the transverse abdominal muscles and maintain for 5 s. (arm position: knee-chest-head) Repeat five times. |
| Dead bug | In the supine position, bend hip and knee 90 degree and lift from floor, flex the opposite shoulder and maintain for 5 s. Repeat five times. |
| Side bridge | In the side lying position with knee flexion, left the pelvic off from the floor and maintain for 5 s. Repeat five times. |
| Superman | In the prone position with arms straight overhead and legs fully extended, simultaneously lift arms and legs off the floor and maintain for 5 s. Repeat five times. |
| Bridge | In the supine position with knee flexion, left the hips off from the floor and maintain for 5 s. Repeat five times. |
| Quadruped position with lifting arm and leg | In the quadruped position, left the arm and leg off from the floor and maintain for 5 s. Repeat five times. |
| Parameters | PNE + LSE (n = 18) | LSE (n = 17) | t/x2 (p) |
|---|---|---|---|
| Age (years) | 68.89 (5.08) | 71.29 (5.18) | −1.386 (0.175) |
| Height (cm) | 159.94 (3.42) | 161.94 (3.63) | −1.675 (0.103) |
| Weight (kg) | 58.22 (2.94) | 60.65 (6.09) | −1.486 (0.151) |
| Obesity rate (%) | 22.76 (0.94) | 23.10 (1.86) | −0.677 (0.505) |
| Duration of injury (months) | 18.50 (6.767) | 19.71 (5.871) | 0.562 (0.578) |
| radiating pain (Yes/No) | 3/15 | 2/15 | 0.172 (0.679) |
| Analgesic use (Yes/No) | 4/14 | 3/14 | 0.114 (0.735) |
| Hypertension (Yes/No) | 11/7 | 10/7 | 0.19 (0.890) |
| Hypercholesterolemia (Yes/No) | 6/12 | 7/12 | 0.230 (0.631) |
| Previous history of cardiovascular disease (Yes/No) | 4/14 | 4/13 | 0.008 (0.927) |
| Parameters | Pre-Test | Post-Test | Group Difference, Mean (95% CI) | SS | df | MS | Effect Size | t(p)/F(p) | |
|---|---|---|---|---|---|---|---|---|---|
| Abdominal muscle strength (sec) | PNE + LSE | 33.83 (5.29) | 41.33 (4.67) | −7.500 (−9.111 to –5.889) | −9.820 (0.000) | ||||
| LSE | 31.71 (4.78) | 36.94 (4.25) | −5.235 (−5.904 to –4.567) | −16.599 (0.000) | |||||
| Covariate | 716.596 | 12 | 59.716 | 11.626 (0.000) | |||||
| Group | 49.302 | 1 | 49.302 | 0.304 | 9.598 (0.005) | ||||
| Error | 113.004 | 22 | 5.137 | ||||||
| Back muscle strength (sec) | PNE + LSE | 16.28 (1.93) | 26.00 (2.22) | −9.722 (−10.877 to –8.568) | −17.769 (0.000) | ||||
| LSE | 15.76 (1.95) | 23.18 (3.50) | −7.412 (−9.007 to –5.816) | −9.846 (0.000) | |||||
| Covariate | 189.558 | 12 | 15.796 | 2.1642 (0.056) | |||||
| Group | 51.851 | 1 | 51.851 | 0.244 | 7.102 (0.014) | ||||
| Error | 160.614 | 22 | 7.301 | ||||||
| Parameters | Pre-Test | Post-Test | Group Difference, Mean (95% CI) | SS | df | MS | Effect Size | t(p)/F(p) | |
|---|---|---|---|---|---|---|---|---|---|
| NPRS (points) | PNE + LSE | 4.67 (1.45) | 2.78 (1.26) | 1.89 (1.65 to 2.12) | 17.000 (0.000) | ||||
| LSE | 4.59 (1.66) | 3.47 (1.37) | 1.12 (0.87 to 1.37) | 9.500 (0.000) | |||||
| Covariate | 57.700 | 12 | 4.808 | 27.524 (0.000) | |||||
| Group | 4.243 | 1 | 4.243 | 0.525 | 24.286 (0.000) | ||||
| Error | 3.843 | 22 | 0.175 | ||||||
| K-PCS (points) | PNE + LSE | 20.06 (2.53) | 12.17 (2.61) | 7.89 (7.02 to 8.76) | 19.178 (0.000) | ||||
| LSE | 18.94 (2.56) | 13.47 (2.76) | 5.47 (4.81 to 6.13) | 17.615 (0.000) | |||||
| Covariate | 197.000 | 12 | 16.417 | 6.381 (0.000) | |||||
| Group | 29.736 | 1 | 29.736 | 0.344 | 11.558 (0.003) | ||||
| Error | 56.600 | 22 | 2.573 | ||||||
| TSK-11 (%) | PNE + LSE | 54.92 (9.93) | 38.13 (7.89) | 16.79 (13.99 to 19.59) | 12.655 (0.000) | ||||
| LSE | 56.95 (6.93) | 45.72 (7.31) | 11.23 (8.70 to 13.76) | 9.414 (0.000) | |||||
| Covariate | 1949.755 | 12 | 162.480 | 7.614 (0.000) | |||||
| Group | 281.246 | 1 | 281.246 | 0.375 | 13.179 (0.001) | ||||
| Error | 469.497 | 22 | 21.341 | ||||||
| Parameters | Pre-Test | Post-Test | Group Difference, Mean (95% CI) | SS | df | MS | Effect Size | t(p)/F(p) | |
|---|---|---|---|---|---|---|---|---|---|
| FFT (cm) | PNE + LSE | −1.83 (3.73) | −1.16 (3.91) | −0.66 (−0.99 to −0.33) | −4.225 (0.001) | ||||
| LSE | 0.17 (3.52) | 0.58 (3.51) | −0.41 (−0.72 to −0.10) | −2.820 (0.012) | |||||
| Covariate | 476.447 | 12 | 39.704 | 89.906 (0.000) | |||||
| Group | 1.911 | 1 | 1.911 | 0.164 | 4.327 (0.049) | ||||
| Error | 9.716 | 22 | 0.442 | ||||||
| MMST (cm) | PNE + LSE | 3.51 (0.78) | 3.71 (0.74) | −0.20 (−0.27 to –0.12) | −5.532 (0.000) | ||||
| LSE | 3.23 (0.84) | 3.37 (0.83) | −0.14 (−0.19 to −0.08) | −5.470 (0.000) | |||||
| Covariate | 22.141 | 12 | 1.845 | 126.527 (0.000) | |||||
| Group | 0.050 | 1 | 0.050 | 0.077 | 3.451 (0.077) | ||||
| Error | 0.31 | 22 | 0.015 | ||||||
| Parameters | Pre-Test | Post-Test | Group Difference, Mean (95% CI) | SS | df | MS | Effect Size | t(p)/F(p) | |
|---|---|---|---|---|---|---|---|---|---|
| RMDQ (points) | PNE + LSE | 9.94 (1.58) | 6.06 (1.79) | 3.89 (3.13 to 4.65) | 10.786 (0.000) | ||||
| LSE | 10.94 (1.56) | 7.18 (1.97) | 3.76 (3.23 to 4.29) | 15.033 (0.000) | |||||
| Covariate | 80.019 | 12 | 6.668 | 3.032 (0.012) | |||||
| Group | 0.179 | 1 | 0.179 | 0.004 | 0.081 (0.778) | ||||
| Error | 48.381 | 22 | 2.199 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, K.-S.; An, J.; Kim, J.-O.; Lee, M.-Y.; Lee, B.-H. Effects of Pain Neuroscience Education Combined with Lumbar Stabilization Exercise on Strength and Pain in Patients with Chronic Low Back Pain: Randomized Controlled Trial. J. Pers. Med. 2022, 12, 303. https://doi.org/10.3390/jpm12020303
Kim K-S, An J, Kim J-O, Lee M-Y, Lee B-H. Effects of Pain Neuroscience Education Combined with Lumbar Stabilization Exercise on Strength and Pain in Patients with Chronic Low Back Pain: Randomized Controlled Trial. Journal of Personalized Medicine. 2022; 12(2):303. https://doi.org/10.3390/jpm12020303
Chicago/Turabian StyleKim, Ki-Sang, Jungae An, Ju-O Kim, Mi-Young Lee, and Byoung-Hee Lee. 2022. "Effects of Pain Neuroscience Education Combined with Lumbar Stabilization Exercise on Strength and Pain in Patients with Chronic Low Back Pain: Randomized Controlled Trial" Journal of Personalized Medicine 12, no. 2: 303. https://doi.org/10.3390/jpm12020303