
Statins Associated with Better Long-Term Outcomes in Aged Hospitalized Patients with COPD: A Real-World Experience from Pay-for-Performance Program



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethical Considerations
2.2. Patient Enrollment, Grouping, and Definition
2.3. Data Collection, Assessment, and Outcome Measures
2.4. Statistics
3. Results
3.1. Clinical and Demographic Characteristics of Patients
3.2. Differences between Survival and Mortality Groups
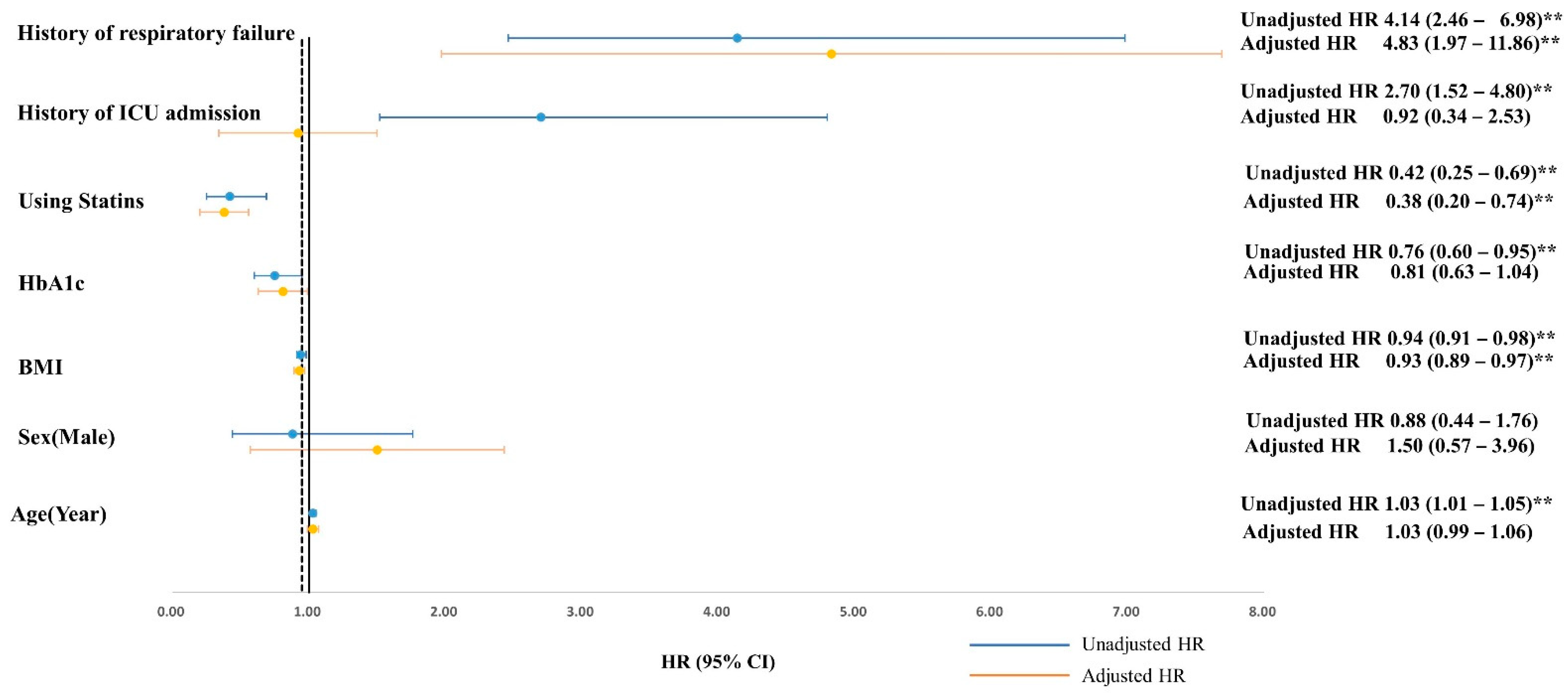
3.3. Factors Associated with Long-Term Mortality for Aged Patients with COPD Hospitalized due to AECOPD
3.4. Analysis of the Effect of Statin Prescription on Overall Mortality of Aged COPD Patients
3.5. Analysis of the Effect of Different Statins on Overall Mortality of Aged COPD Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chronic Obstructive Pulmonary Disease (COPD). Available online: https://www.who.int/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-(copd) (accessed on 10 November 2021).
- Global Initiative for Chronic Obstructive Lung Disease 2021 Report. Available online: https://goldcopd.org/2021-gold-reports/ (accessed on 20 December 2021).
- Adeloye, D.; Chua, S.; Lee, C.; Basquill, C.; Papana, A.; Theodoratou, E.; Nair, H.; Gasevic, D.; Sridhar, D.; Campbell, H.; et al. Global and regional estimates of COPD prevalence: Systematic review and meta-analysis. J. Glob. Health 2015, 5, 020415. [Google Scholar] [CrossRef] [PubMed]
- van Eeden, S.F.; Sin, D.D. Chronic obstructive pulmonary disease: A chronic systemic inflammatory disease. Respiration 2008, 75, 224–238. [Google Scholar] [CrossRef] [PubMed]
- Lopez, A.D.; Shibuya, K.; Rao, C.; Mathers, C.D.; Hansell, A.L.; Held, L.S.; Schmid, V.; Buist, S. Chronic obstructive pulmonary disease: Current burden and future projections. Eur. Respir. J. 2006, 27, 397–412. [Google Scholar] [CrossRef] [Green Version]
- Mathers, C. Updated WHO Projection of Mortality and Causes of Death 2016–2060. Available online: https://www.who.int/healthinfo/global_burden_disease/projections_method.pdf (accessed on 15 November 2021).
- Sorge, R.; DeBlieux, P. Acute Exacerbations of Chronic Obstructive Pulmonary Disease: A Primer for Emergency Physicians. J. Emerg. Med. 2020, 59, 643–659. [Google Scholar] [CrossRef] [PubMed]
- Hillas, G.; Perlikos, F.; Tzanakis, N. Acute exacerbation of COPD: Is it the “stroke of the lungs”? Int. J. Chron. Obstruct. Pulm. Dis. 2016, 11, 1579–1586. [Google Scholar] [CrossRef] [Green Version]
- Crisafulli, E.; Barbeta, E.; Ielpo, A.; Torres, A. Management of severe acute exacerbations of COPD: An updated narrative review. Multidiscip. Respir. Med. 2018, 13, 36. [Google Scholar] [CrossRef]
- Han, M.K.; Martinez, F.J. Host, Gender, and Early-Life Factors as Risks for Chronic Obstructive Pulmonary Disease. Clin. Chest Med. 2020, 41, 329–337. [Google Scholar] [CrossRef]
- Sprooten, R.T.M.; Rohde, G.G.U.; Lawyer, G.; Leijte, W.T.; Wouters, E.F.M.; Franssen, F.M.E. Risk stratification for short-term mortality at hospital admission for acute exacerbations of COPD. Respirology 2019, 24, 765–776. [Google Scholar] [CrossRef]
- Cao, Y.; Xing, Z.; Long, H.; Huang, Y.; Zeng, P.; Janssens, J.P.; Guo, Y. Predictors of mortality in COPD exacerbation cases presenting to the respiratory intensive care unit. Respir. Res. 2021, 22, 77. [Google Scholar] [CrossRef]
- Ho, T.W.; Tsai, Y.J.; Ruan, S.Y.; Huang, C.T.; Lai, F.; Yu, C.J.; Group, H.S. In-hospital and one-year mortality and their predictors in patients hospitalized for first-ever chronic obstructive pulmonary disease exacerbations: A nationwide population-based study. PLoS ONE 2014, 9, e114866. [Google Scholar] [CrossRef] [Green Version]
- Brown, H.; Dodic, S.; Goh, S.S.; Green, C.; Wang, W.C.; Kaul, S.; Tiruvoipati, R. Factors associated with hospital mortality in critically ill patients with exacerbation of COPD. Int. J. Chron. Obstruct. Pulm. Dis 2018, 13, 2361–2366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia-Sanz, M.T.; Canive-Gomez, J.C.; Senin-Rial, L.; Aboal-Vinas, J.; Barreiro-Garcia, A.; Lopez-Val, E.; Gonzalez-Barcala, F.J. One-year and long-term mortality in patients hospitalized for chronic obstructive pulmonary disease. J. Thorac. Dis. 2017, 9, 636–645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Celli, B.R.; Cote, C.G.; Marin, J.M.; Casanova, C.; Montes de Oca, M.; Mendez, R.A.; Pinto Plata, V.; Cabral, H.J. The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. N. Engl. J. Med. 2004, 350, 1005–1012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riley, C.M.; Sciurba, F.C. Diagnosis and Outpatient Management of Chronic Obstructive Pulmonary Disease: A Review. JAMA 2019, 321, 786–797. [Google Scholar] [CrossRef]
- Vieira, E.B.; Degani-Costa, L.H.; Amorim, B.C.; Oliveira, L.B.; Miranda-Silva, T.; Sperandio, P.C.; Medeiros, W.M.; Arbex, F.F.; Ramos, R.P.; Nery, L.E. Modified BODE Index to Predict Mortality in Individuals With COPD: The Role of 4-Min Step Test. Respir. Care 2020, 65, 977–983. [Google Scholar] [CrossRef]
- Yang, C.J.; Liao, W.I.; Tang, Z.C.; Wang, J.C.; Lee, C.H.; Chang, W.C.; Hsu, C.W.; Tang, S.E.; Tsai, S.H. Glycated hemoglobin A1c-based adjusted glycemic variables in patients with diabetes presenting with acute exacerbation of chronic obstructive pulmonary disease. Int. J. Chron. Obstruct. Pulm. Dis. 2017, 12, 1923–1932. [Google Scholar] [CrossRef] [Green Version]
- Almagro, P.; Boixeda, R.; Diez-Manglano, J.; Gomez-Antunez, M.; Lopez-Garcia, F.; Recio, J. Insights into Chronic Obstructive Pulmonary Disease as Critical Risk Factor for Cardiovascular Disease. Int. J. Chron. Obstruct. Pulm. Dis. 2020, 15, 755–764. [Google Scholar] [CrossRef] [Green Version]
- Citgez, E.; van der Palen, J.; Koehorst-Ter Huurne, K.; Movig, K.; van der Valk, P.; Brusse-Keizer, M. Statins and morbidity and mortality in COPD in the COMIC study: A prospective COPD cohort study. BMJ Open Respir. Res. 2016, 3, e000142. [Google Scholar] [CrossRef] [Green Version]
- WMA—The World Medical Association-WMA Declaration of Helsinki–Ethical Principles for Medical Research Involving Human Subjects. Available online: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/ (accessed on 20 December 2021).
- Ritchie, A.I.; Wedzicha, J.A. Definition, Causes, Pathogenesis, and Consequences of Chronic Obstructive Pulmonary Disease Exacerbations. Clin. Chest Med. 2020, 41, 421–438. [Google Scholar] [CrossRef]
- Kim, V.; Aaron, S.D. What is a COPD exacerbation? Current definitions, pitfalls, challenges and opportunities for improvement. Eur. Respir. J. 2018, 52, 1801261. [Google Scholar] [CrossRef]
- Fu, P.K.; Yang, M.C.; Wang, C.Y.; Lin, S.P.; Kuo, C.T.; Hsu, C.Y.; Tung, Y.C. Early Do-Not-Resuscitate Directives Decrease Invasive Procedures and Health Care Expenses during the Final Hospitalization of Life of COPD Patients. J. Pain Symptom Manag. 2019, 58, 968–976. [Google Scholar] [CrossRef] [PubMed]
- Global Initiative for Chronic Obstructive Lung Disease 2022 Report. Available online: https://goldcopd.org/2022-gold-reports/ (accessed on 20 December 2021).
- Fu, P.K.; Tung, Y.C.; Wang, C.Y.; Hwang, S.F.; Lin, S.P.; Hsu, C.Y.; Chen, D.R. Early and late do-not-resuscitate (DNR) decisions in patients with terminal COPD: A retrospective study in the last year of life. Int. J. Chron. Obstruct. Pulm. Dis. 2018, 13, 2447–2454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glaser, S.; Kruger, S.; Merkel, M.; Bramlage, P.; Herth, F.J. Chronic obstructive pulmonary disease and diabetes mellitus: A systematic review of the literature. Respiration 2015, 89, 253–264. [Google Scholar] [CrossRef] [PubMed]
- Mirrakhimov, A.E. Chronic obstructive pulmonary disease and glucose metabolism: A bitter sweet symphony. Cardiovasc. Diabetol. 2012, 11, 132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andre, S.; Conde, B.; Fragoso, E.; Boleo-Tome, J.P.; Areias, V.; Cardoso, J.; GI DPOC-Grupo de Interesse na Doença Pulmonar Obstrutiva Crónica. COPD and Cardiovascular Disease. Pulmonology 2019, 25, 168–176. [Google Scholar] [CrossRef]
- Cavailles, A.; Brinchault-Rabin, G.; Dixmier, A.; Goupil, F.; Gut-Gobert, C.; Marchand-Adam, S.; Meurice, J.C.; Morel, H.; Person-Tacnet, C.; Leroyer, C.; et al. Comorbidities of COPD. Eur. Respir. Rev. 2013, 22, 454–475. [Google Scholar] [CrossRef]
- Lin, L.; Shi, J.; Kang, J.; Wang, Q. Analysis of prevalence and prognosis of type 2 diabetes mellitus in patients with acute exacerbation of COPD. BMC Pulm. Med. 2021, 21, 7. [Google Scholar] [CrossRef]
- Gunasekaran, K.; Murthi, S.; Elango, K.; Rahi, M.S.; Thilagar, B.; Ramalingam, S.; Voruganti, D.; Paramasivam, V.K.; Kolandaivel, K.P.; Arora, A.; et al. The Impact of Diabetes Mellitus in Patients with Chronic Obstructive Pulmonary Disease (COPD) Hospitalization. J. Clin. Med. 2021, 10, 235. [Google Scholar] [CrossRef]
- Ho, T.W.; Huang, C.T.; Ruan, S.Y.; Tsai, Y.J.; Lai, F.; Yu, C.J. Diabetes mellitus in patients with chronic obstructive pulmonary disease-The impact on mortality. PLoS ONE 2017, 12, e0175794. [Google Scholar] [CrossRef]
- Mao, X.; Liang, C.; Niu, H.; Dong, F.; Huang, K.; Chen, Y.; Huang, K.; Zhan, Q.; Zhang, Y.; Huang, Y.; et al. Outcomes associated with comorbid diabetes among patients with COPD exacerbation: Findings from the ACURE registry. Respir. Res. 2021, 22, 7. [Google Scholar] [CrossRef]
- Wang, Y.F.; Tang, Z.; Guo, J.; Tao, L.X.; Liu, L.; Li, H.B.; Li, D.T.; Guo, X.H.; Yang, X.H. BMI and BMI Changes to All-cause Mortality among the Elderly in Beijing: A 20-year Cohort Study. Biomed Environ. Sci. 2017, 30, 79–87. [Google Scholar] [CrossRef] [PubMed]
- DeLapp, D.A.; Glick, C.; Furmanek, S.; Ramirez, J.A.; Cavallazzi, R. Patients with Obesity Have Better Long-Term Outcomes after Hospitalization for COPD Exacerbation. COPD 2020, 17, 373–377. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes, A. 12. Older Adults: Standards of Medical Care in Diabetes-2021. Diabetes Care 2021, 44, S168–S179. [Google Scholar] [CrossRef] [PubMed]
- Soyseth, V.; Brekke, P.H.; Smith, P.; Omland, T. Statin use is associated with reduced mortality in COPD. Eur. Respir. J. 2007, 29, 279–283. [Google Scholar] [CrossRef] [Green Version]
- Lawes, C.M.; Thornley, S.; Young, R.; Hopkins, R.; Marshall, R.; Chan, W.C.; Jackson, G. Statin use in COPD patients is associated with a reduction in mortality: A national cohort study. Prim. Care Respir. J. 2012, 21, 35–40. [Google Scholar] [CrossRef]
- Lu, Y.; Chang, R.; Yao, J.; Xu, X.; Teng, Y.; Cheng, N. Effectiveness of long-term using statins in COPD—A network meta-analysis. Respir. Res. 2019, 20, 17. [Google Scholar] [CrossRef]
- Smith, M.C.; Ashdown, H.F.; Sheppard, J.P.; Butler, C.C.; Bankhead, C. Statin prescription in patients with chronic obstructive pulmonary disease and risk of exacerbations: A retrospective cohort study in the Clinical Practice Research Datalink. BMJ Open 2021, 11, e050757. [Google Scholar] [CrossRef]
- Chen, C.Y.; Wu, W.T.; Wang, Y.L.; Liao, K.M. Statins for the Treatment of Pulmonary Hypertension in Patients with Chronic Obstructive Pulmonary Disease. Front. Pharmacol. 2020, 11, 613761. [Google Scholar] [CrossRef]
- Crouse, J.R., 3rd; Raichlen, J.S.; Riley, W.A.; Evans, G.W.; Palmer, M.K.; O’Leary, D.H.; Grobbee, D.E.; Bots, M.L.; Group, M.S. Effect of rosuvastatin on progression of carotid intima-media thickness in low-risk individuals with subclinical atherosclerosis: The METEOR Trial. JAMA 2007, 297, 1344–1353. [Google Scholar] [CrossRef] [Green Version]
- Ridker, P.M.; Danielson, E.; Fonseca, F.A.; Genest, J.; Gotto, A.M., Jr.; Kastelein, J.J.; Koenig, W.; Libby, P.; Lorenzatti, A.J.; MacFadyen, J.G.; et al. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N. Engl. J. Med. 2008, 359, 2195–2207. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variables | Median | IQR |
|---|---|---|
| Age (year) | 80.0 | 70.0–87.0 |
| Gender-Male (n, %) | 259 | 87.5% |
| Body mass index (kg/m2) | 23.7 | 20.6–27.2 |
| HbA1c | 6.5 | 5.9–7.5 |
| Pulmonary function test | ||
| FEV1 (%) | 68.0 | 53.0–87.0 |
| FVC (%) | 86.0 | 72.0–108.0 |
| FEV1/FVC (%) | 63.0 | 53.0–71.0 |
| GOLD classification | ||
| Category C (n, %) | 193 | 65.2% |
| Category D (n, %) | 103 | 34.8% |
| Comorbidity Status (Deyo Score ≥ 1) | 190 | 64.2% |
| Coronary artery disease (CAD) (n, %) | 49 | 16.6% |
| Cerebrovascular disease (CVA) (n, %) | 47 | 15.9% |
| With DM history (n, %) | 167 | 56.4% |
| Using Insulin or OHA (n, %) | 99 | 33.5% |
| Using Statins (n, %) | 93 | 31.4% |
| Outcomes | ||
| ICU admission (n, %) | 69 | 23.3% |
| Respiratory failure (n, %) | 104 | 35.1% |
| Hospital mortality (n, %) | 39 | 13.2% |
| 1-year mortality (n, %) | 100 | 33.8% |
| Overall mortality (n, %) | 152 | 51.4% |
| Follow-up years | 3.0 | 2.6–3.5 |
| Variables | Total (n = 296) | Mortality (n = 152) | Survival (n = 144) | p Value |
|---|---|---|---|---|
| Median (IQR); (n, %) | ||||
| Age (year) | 80.0 (70.0–87.0) | 81.0 (74.0–88.0) | 78.0 (68.0–86.0) | 0.051 |
| Sex-Male c | 259 (87.5%) | 134 (88.2%) | 125 (86.8%) | 0.725 |
| BMI (kg/m2) | 23.7 (20.6–27.2) | 22.0 (20.0–26.1) | 25.1 (21.2–27.9) | 0.003 ** |
| HbA1c (%) | 6.5 (5.9–7.5) | 6.4 (5.9–7.3) | 6.9 (6.0–7.7) | 0.3949 |
| Pulmonary function test | ||||
| FEV1 (%) | 68.0 (53.0–87.0) | 70.5 (55.0–87.0) | 65.0 (53.0–87.0) | 0.755 |
| FVC (%) | 86.0 (72.0–108.0) | 86.5 (77.0–108.0) | 85.0 (67.0–102.0) | 0.533 |
| FEV1/FVC (%) | 63.0 (53.0–71.0) | 60.5 (52.0–69.0) | 64.0 (55.0–72.0) | 0.189 |
| GOLD classification | ||||
| Category C (n, %) | 193 (65.2%) | 99 (65.1%) | 94 (65.3%) | 0.979 |
| Category D (n, %) | 103 (34.8%) | 53 (34.9%) | 50 (34.7%) | |
| Comorbidity Status | ||||
| Deyo Score ≥ 1 | 190 (64.2%) | 92 (60.5.0%) | 98 (68.1%) | 0.178 |
| CAD (n, %) | 49 (16.6%) | 28 (18.4%) | 21 (14.6%) | 0.375 |
| CVA (n, %) | 47 (15.9%) | 21 (13.8%) | 26 (18.1%) | 0.319 |
| With DM history c | 167 (56.4%) | 82 (54.0%) | 85 (59.0%) | 0.379 |
| Using Insulin or OHA c | 99 (33.5%) | 51 (33.6%) | 48 (33.3%) | 0.968 |
| Using Statins c | 93 (31.4%) | 34 (22.4%) | 59 (41.0%) | <0.001 ** |
| History of ICU admission c | 69 (23.3%) | 48 (31.6%) | 21 (14.6%) | 0.001 ** |
| History of respiratory failure c | 104 (35.1%) | 76 (50.0%) | 28 (19.4%) | <0.001 ** |
| Variables | Univariate Analysis HR (95% CI) | Multivariate Analysis HR (95% CI) |
|---|---|---|
| Age (year) | 1.03 (1.01–1.05) ** | 1.03 (0.99–1.06) |
| Sex-Male | 0.88 (0.44–1.76) | 1.50 (0.57–3.96) |
| BMI | 0.94 (0.91–0.98) ** | 0.93 (0.89–0.97) ** |
| HbA1c | 0.76 (0.60–0.95) ** | 0.81 (0.63–1.04) |
| Deyo Score ≥ 1 | 0.72 (0.45–1.16) | |
| With DM history | 0.81 (0.51–1.29) | |
| CAD | 1.32 (0.71–2.45) | |
| CVA | 0.73 (0.39–1.36) | |
| Using Insulin or OHA | 1.01 (0.62–1.64) | |
| Using Statins | 0.42 (0.25–0.69) ** | 0.38 (0.20–0.74) ** |
| History of ICU admission | 2.70 (1.52–4.80) ** | 0.92 (0.34–2.53) |
| History of respiratory failure | 4.14 (2.46–6.98) ** | 4.83 (1.97–11.86) ** |
| Statin Type and Dose (n = 93) | n (%) | Univariate Analysis HR (95% CI) |
|---|---|---|
| Rosuvastatin 10 mg | 30 (32.3%) | 0.44 (0.20–0.97) * |
| Pravastatin 40 mg | 15 (16.1%) | 0.33 (0.10–1.05) |
| Atorvastatin 10 mg | 13 (14.0%) | 0.80 (0.26–2.45) |
| Atorvastatin 20 mg | 34 (36.5%) | 0.63 (0.31–1.30) |
| Atorvastatin 40 mg | 1 (1.1%) | n/a |
| Atorvastatin all dose | 48 (52%) | 0.70 (0.37–1.29) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.-Y.; Li, T.-C.; Li, C.-I.; Lin, S.-P.; Fu, P.-K. Statins Associated with Better Long-Term Outcomes in Aged Hospitalized Patients with COPD: A Real-World Experience from Pay-for-Performance Program. J. Pers. Med. 2022, 12, 299. https://doi.org/10.3390/jpm12020299
Chen Y-Y, Li T-C, Li C-I, Lin S-P, Fu P-K. Statins Associated with Better Long-Term Outcomes in Aged Hospitalized Patients with COPD: A Real-World Experience from Pay-for-Performance Program. Journal of Personalized Medicine. 2022; 12(2):299. https://doi.org/10.3390/jpm12020299
Chicago/Turabian StyleChen, Ying-Yi, Tsai-Chung Li, Chia-Ing Li, Shih-Pin Lin, and Pin-Kuei Fu. 2022. "Statins Associated with Better Long-Term Outcomes in Aged Hospitalized Patients with COPD: A Real-World Experience from Pay-for-Performance Program" Journal of Personalized Medicine 12, no. 2: 299. https://doi.org/10.3390/jpm12020299