1. Introduction
As societies age, more and more people become affected with dementia [
1]. In Germany, according to the German Alzheimer Society e.V. [
2], the number of people with dementia will have risen to three million by 2050. In addition to the personal cost, the disease causes substantial economic and social burdens [
3]. However, these burdens can be alleviated by early diagnosis of dementia and its pre-stages, as such early detection can allow for more sustainable disease management and optimal health care for affected individuals [
1]. It is therefore important to identify people with pre-dementia (e.g., persons with mild cognitive impairments, or MCI) early enough so they can start programs that will help them maintain their personal lifestyle and that will continuously assess the course of the dementia as it progresses.
In many therapeutic areas, diseases and treatments are evaluated using patient-reported outcome (PRO) measures (subjective measures), collected, for example, via questionnaires [
4]. However, several barriers exist for using PRO measures in cognitive impairment. For example, disease-related disorders can impair memory and cause people to lose insight into how their disease is progressing [
4,
5]. In these cases, one must rely on the reports of clinicians or information from personal contacts, such as family members [
4,
6]. However, the accuracy of the information provided by family members may be suboptimal, as biases may interfere or caregivers may lack knowledge regarding the disease symptoms [
4,
7]. Therefore, the validity of PRO measurements is limited. Furthermore, the sensitivity of current PRO measures for patients with mild cognitive impaired individuals (MCI) and Alzheimer’s disease (AD) patients in the prodromal stage is limited, as they are not specifically designed for these milder conditions [
4]. A combination of several neuropsychological tests (e.g., MoCA [
8] and CERAD-NP [
9]) may improve classification (e.g., [
10,
11]) and additionally identify a transitional stage between cognitively healthy individuals (CHI) and MCI, possible MCI (pMCI) as recently defined as individuals with some signs of cognitive impairment [
1,
10].
AD and cognitively healthy individuals have been shown to differ in performance of movement tasks (e.g., finger tapping [
12]). Therefore, objective measurements, e.g., by technical systems that measure simple movements, are an alternative to PRO measurements because they are easy to use and inexpensive. For this purpose, researchers use computer-aided measuring systems that measure parameters of the movement by means of a keyboard [
13], force sensors [
12] or light beams [
14]. With these types of devices, studies have shown differences in finger tapping tasks between age-matched healthy subjects and people with AD [
12,
13,
14], MCI [
13,
14] and Parkinson’s disease [
14] in a mean age range of 71–82 years. These differences are mainly related to a slowing of the tapping rhythm and an increase in touch duration as well an increase in the variability of these parameters [
12,
13,
14]. Such a study on the finger tapping behavior of group pMCI has not been previously conducted. In general, it should be noted that tapping is a diadochokinetic movement consisting of flexion followed by extension of the fingers. The timing of the change in movement is controlled by proprioceptive signals that are triggered when the force sensor is touched [
15,
16,
17]. The tapping task therefore tests the ability to plan and execute rhythmically oppositely oriented movements. It is shown that the selected tap pace has an influence on the execution [
13].
Therefore, in this study we aimed to use tapping parameters to distinguish between participants over 80 years old who were either cognitively healthy individuals (CHI), mild cognitive impaired individuals (MCI) or had possible MCI (pMCI), in two different conditions: as consistently as possible at a self-selected pace or as fast as possible without considering consistency (fast pace). We expected that in addition to reproducing known differences in tapping parameter between CHI and MCI groups [
13,
14], we would also find differences between pMCI subjects and the other groups. In addition, a recent study has shown for this study group that sex has an effect on force control [
18]. It was therefore expected that sex differences in finger tapping parameters would be found. Based on these differences, we then developed a classifier to determine whether a subject belongs to a group.
4. Discussion
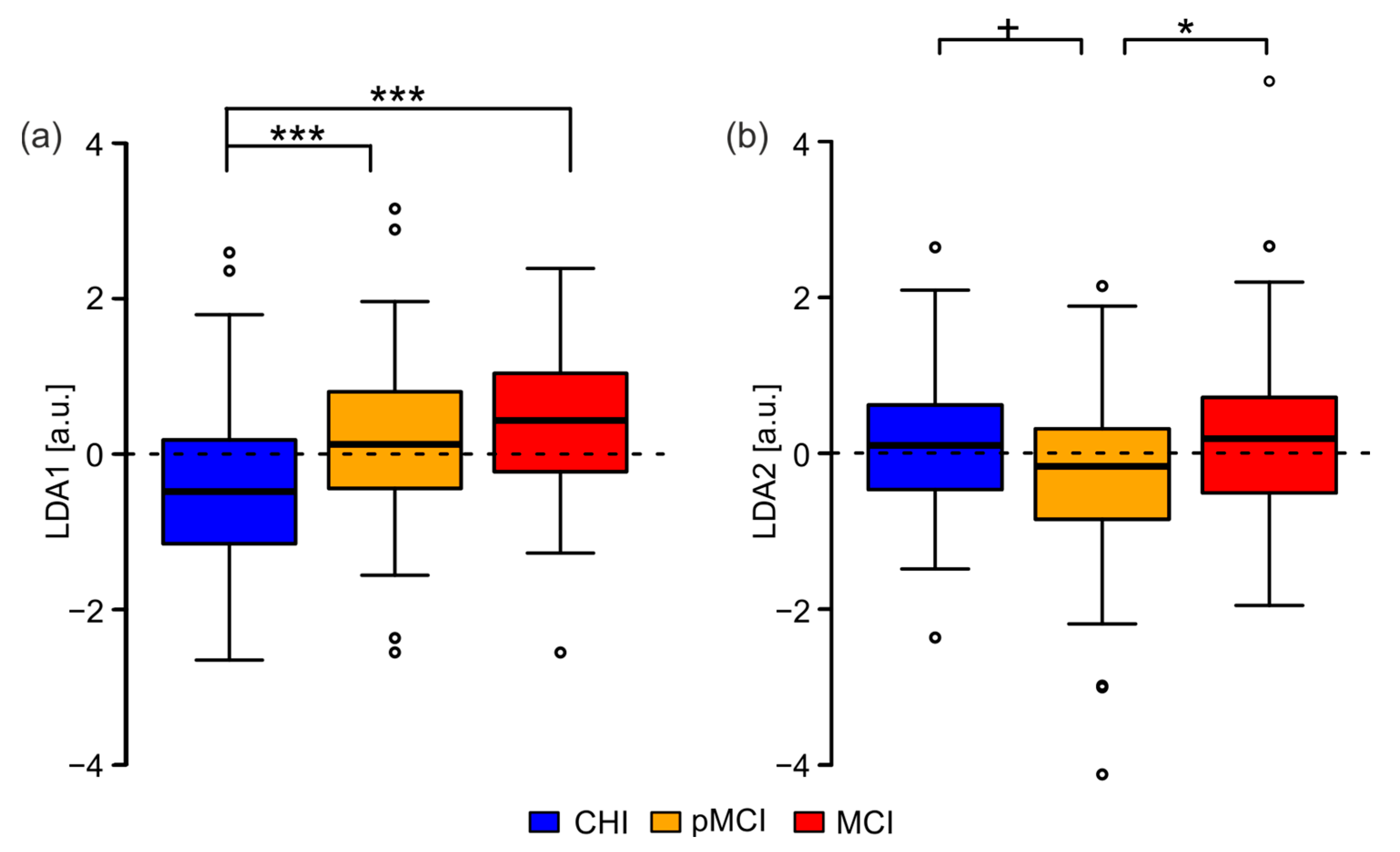
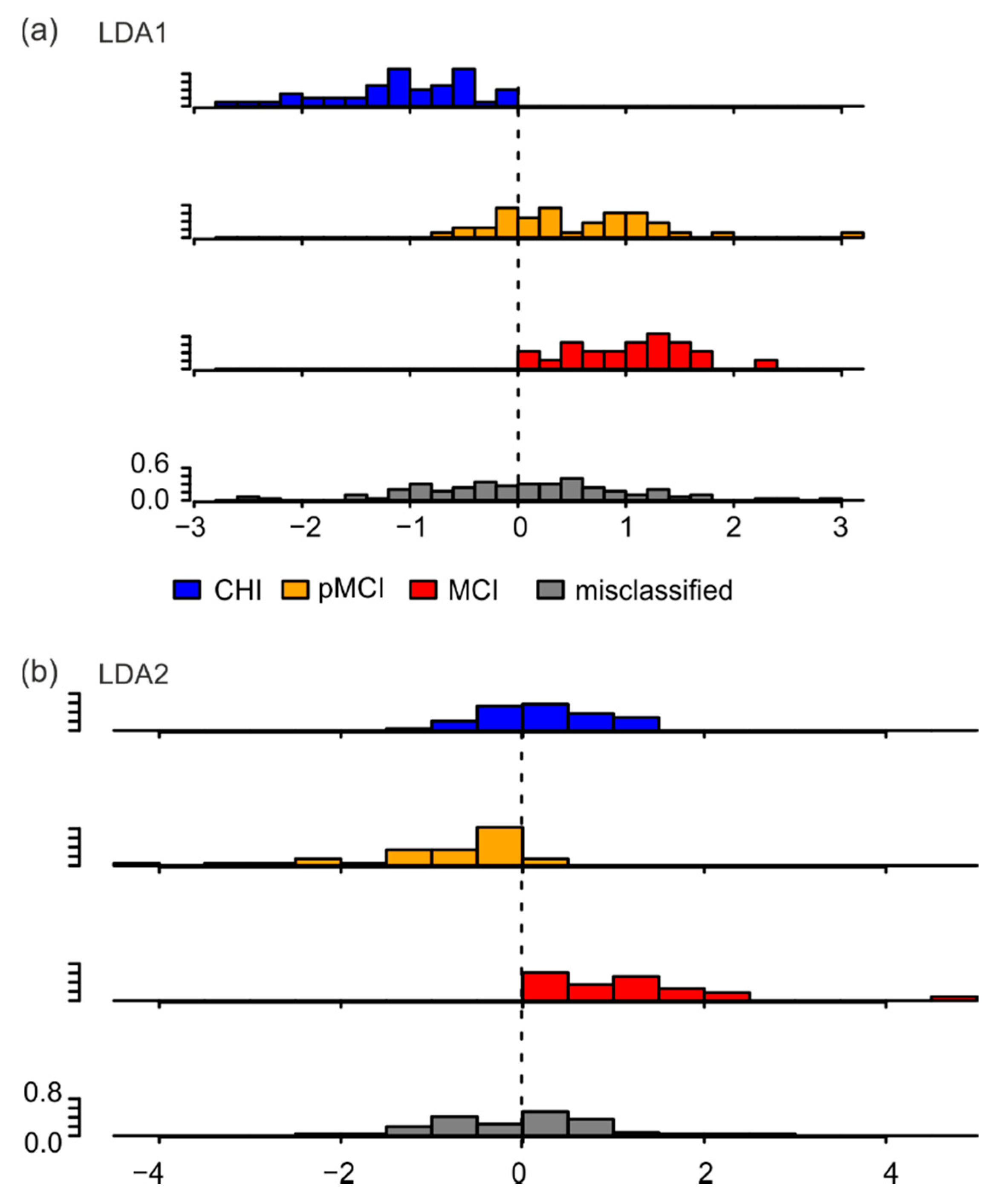
The aim of the study was to develop a system that uses tapping parameters in a self-selected and fast tapping mode to distinguish cognitively healthy individuals (CHI) from people with possible MCI (pMCI) and people with mild cognitive impairments (MCI), specifically for individuals over 80 years old. For this purpose, the finger tapping behavior of 225 subjects over 80 years old was analyzed. ANOVA revealed differences between groups (CHI, pMCI, MCI), sexes (male, female) and their interaction (group × sex) for the self-selected pace condition (four parameters) and for the fast pace condition (eight parameters). These parameters were used for classification by means of a linear discriminant analysis (LDA). The first LDA component showed significant differences between CHI and pMCI, CHI and MCI, and pMCI and MCI. Furthermore, the second LDA component showed significant differences between CHI and pMCI and between pMCI and MCI. Nevertheless, when the algorithm was used to classify individual participants, it was correct in only 50% of cases. This shows that tapping parameters were only partially useful for classification.
Our results showed that pMCI, a group first described in the SENDA study [
10], differed from both CHI and MCI. Previous studies on tapping behavior were mainly conducted with Alzheimer’s patients (e.g., [
12]) or MCI patients, (e.g., the CDR. 5 group in [
13]). In this study, we additionally showed that in the self-selected pace condition, not only participants with MCI but also those with pMCI had a significantly slower tapping rhythm and prolonged touch duration compared to CHI (
Table 2: tap-cyle_median, tap-duration_median, and plateau-duration_median).
However, the planned goal of classifying individual participants based on tapping parameters was only partially achieved. Thus, while 49 of 79 CHI participants were correctly classified on the basis of their motor performance, 30 of these participants were classified as pMCI or MCI. Furthermore, 42 of 65 MCI patients were apparently classified as CHI or pMCI. An explanation for the misclassification might be the simplicity of the task. Previous work has shown that no age effects exist in tasks with simple planned anticipatory grasp control, such as in tapping [
29]; only tasks with higher complexity, such as activities of daily living, had recognizable differences [
29]. In a recent study with a subset of the subjects described here, it was shown that all participants were comparably able to perform anticipatory grip strength control regardless of group membership [
18]. It can therefore be assumed that the motor requirements of the tapping task were not sufficient to reliably separate between the groups.
In addition to the experimental condition, the neurological status of the participants must also be considered. All participants reported no neurological deficits (an exclusion criterion; see Methods). However, individuals may have had different degrees of age-related degeneration and in different relevant areas of the CNS (e.g., cortex, spinal cord, basal ganglia, cerebellum). Cortical activity can be measured via resting-state electroencephalography (EEG), usually performed with eyes closed and/or eyes open [
30]. It is a measure of tonic brain activity [
31] and this spontaneous EEG activity is thought to account for 80% of total brain activity [
30,
32]. Only a small additional percentage is accounted for by engagement in a task [
32]. Thus, resting-state EEG studies describe the functional state of the cortex. A recent study [
10] showed that in the subjects studied, cortical activity in resting-state EEG did not differ between groups. Therefore, group differences in tapping parameters cannot be derived from cortical differences between the groups.
For Parkinson’s disease, as an example disease of the basal ganglia, it is known that patients show a faster tapping rhythm than healthy subjects [
14]. In contrast, our data show that in the self-selected pace condition pMCI and MCI tapped significantly slower than CHI, and in the fast pace condition there was a significant difference between CHI and MCI for this parameter (
Table 2). This is consistent with behavior shown in MCI and Alzheimer’s patients [
12,
13,
14]. Therefore, it is reasonable to conclude that the group differences are not due to an influence of the basal ganglia.
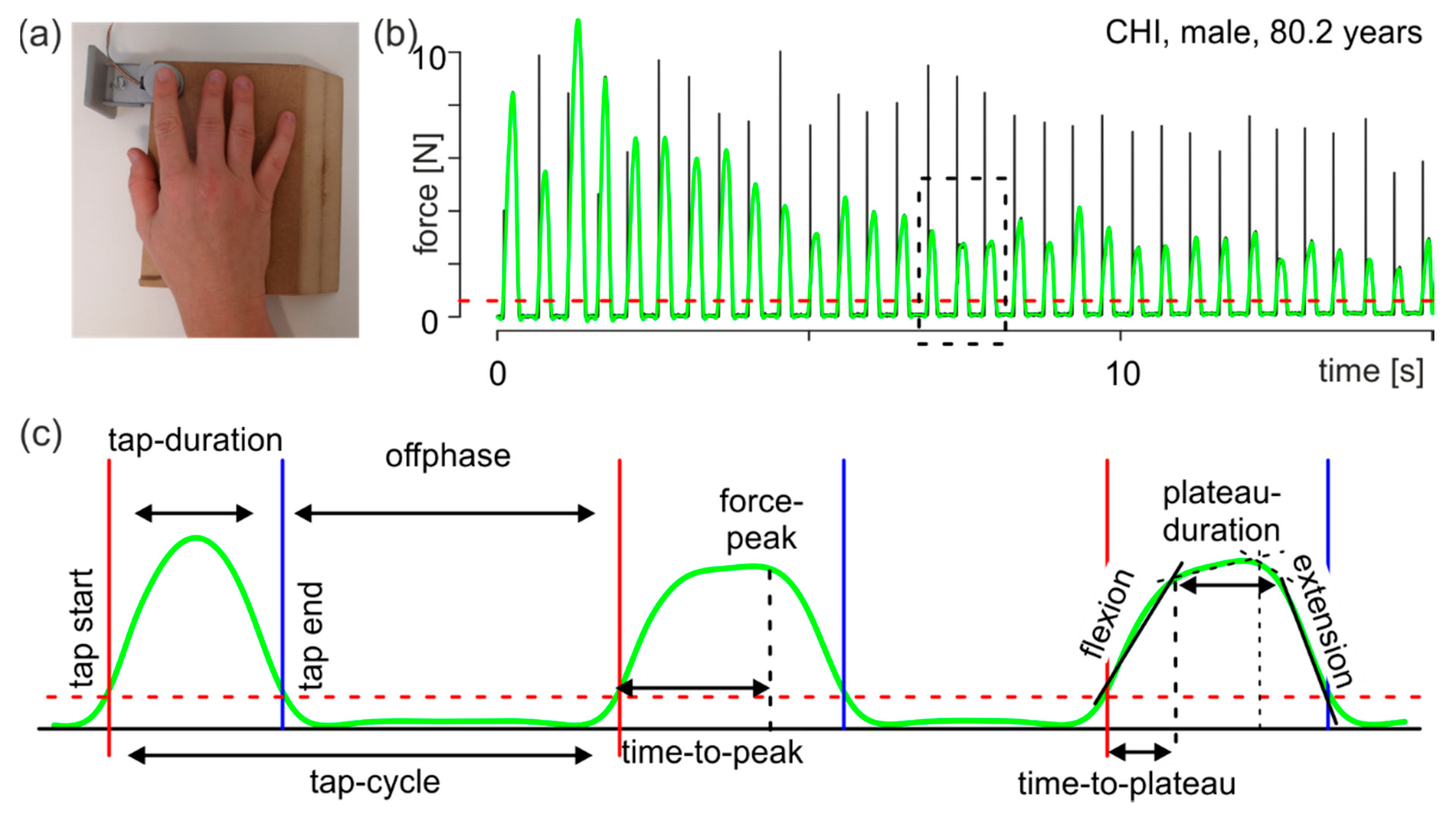
The influence of spinal cord control can be derived from the parameter time-to-plateau (
Figure 1). Tapping can be described as a diadochokinetic task. It consists of finger flexion followed by finger extension. The time to stop flexion and start extension is controlled by proprioceptive signals. The mean size of the parameter time-to-plateau gives information on the planned movement (the shorter the time to plateau, the faster the movement), and its variability gives information on the participant’s proprioceptive control at the spinal cord level (the smaller the better). The parameter time-to-plateau was determined by the current speed of the movement (
Figure 1, flexion) and the sensory feedback at touch, which could lead to deceleration of the movement and onset of the reverse movement (
Figure 1, extension). If sensory feedback is insufficient, the stopping of the movement is delayed and much more variable. Thus, group differences can be inferred from the variability and mean magnitude of this parameter. For the self-selected pace condition, no group differences existed in either mean magnitude (
Table 2 time-to-plateau_median) or variability (
Table 2 time-to-plateau_iqr). In the fast pace condition, only one significant difference was found between CHI and pMCI or MCI for the parameter time-to-plateau_median. Therefore, in the fast pace condition, CHI performed a significantly faster motor program than the other groups. Because the variability of the time-to-plateau parameter was the same between groups in both pace conditions, it can be assumed that the degree of degeneration at the spinal cord level can be considered comparable between the groups.
The cerebellum is known to be generally important for coordinating motor performance, such as diadochokinesis, and it is additionally important for associating sensory information with movements as well as for adapting movements [
33]. Some studies have highlighted the cerebellum’s importance in the context of participants’ associative learning of grip forces [
34,
35]. For example, in precision finger tasks such as the raspberry task [
36,
37], half of the young participants showed a conditioned change in force at just the second presentation of the conditioning stimulus [
35] and personal observation of DFK. In contrast, cerebellar patients were significantly worse than control subjects at learning the necessary association [
34]. For a successful association between the conditioned stimulus and the motor action, participants needed a well-planned and controlled execution of the task [
35]; in cerebellar patients, this execution was impaired [
25]. It is therefore possible that restrictions in tapping behavior can be explained not only by cognitive impairments, but also by age-related decline of the cerebellum. This is accompanied by a reduced ability to associate sensory information with the necessary timing of tapping. As they are spatially separated from the regions related to manual motor performance, parts of the cerebellum are also correlated with cognitive performance [
38,
39,
40,
41]. The anterior lobe and the top of the superior posterior lobe are correlated with motor skills, and the bottom parts of the posterior superior lobe and the inferior lobe are correlated with cognition [
39]. Degeneration of cerebellar regions associated with the somatomotor network is more pronounced than that of regions associated with dorsal attention, ventral attention, or frontoparietal networks [
38]. Furthermore, age-related degeneration of the motor cerebellum is comparable to the degeneration found in cerebellar diseases [
38]. In contrast, Alzheimer’s patients show degeneration of the cognitive part of the cerebellum without concomitant increased degeneration in the motor cerebellum [
41]. Notably, the cerebellum is generally considered to be resistant to the neurotoxic effects of soluble amyloid-beta (Aβ), which is helpful in the early stages of AD [
42]. However, assuming that a proportion of participants classified as MCI are in a precursor phase to AD, it is still reasonable to hypothesize that the influence of the cerebellum on tapping behavior should be considered an age-related limitation rather than an effect of the developing disease.
In conclusion, the 30 misclassified participants in the CHI group may have had more degeneration of the motor cerebellum than those correctly classified into the CHI group (n = 49). Indicators for this difference are the values for the tap-cycle (correctly classified CHI: −0.697 ± 0.008; misclassified CHI: −0.422 ± 0.013; mean ± SEM in log [s]) and tap-duration (correctly classified CHI: −1.825 ± 0.007; misclassified CHI: −1.448 ± 0.016; mean ± SEM in log [s]) parameters in the self-selected condition. Thus, in this condition, the correctly classified CHI showed a significantly faster tapping rhythm with a shorter tapping duration (p < 0.005, Bonferroni corrected, both parameters). Similarly, it can be hypothesized that the 42 misclassified MCI participants had less degeneration of the cerebellum than the correctly classified MCI patients (n = 23). This can be seen from the values for the tap-cycle (correctly classified MCI: −1,289 ± 0.012; misclassified MCI: −1.407 ± 0.005; mean ± SEM in log [s]) and tap-duration (correctly classified MCI: −2.017 ± 0.012; misclassified MCI: −2.213 ± 0.004; mean ± SEM in log [s]) parameters in the fast pace condition. In this condition, the correctly classified MCI showed a slower tap rhythm (p < 0.1, Bonferroni corrected) with a significantly longer tap duration (p < 0.004, Bonferroni corrected).
Overall, when investigating whether cognitive state can be assessed based on simple finger movements (such as tapping), one must also consider the possible degeneration of relevant motor systems (e.g., the cerebellum). To establish tapping as a good classifier, researchers need to perform additional motor tests to specifically determine the degeneration of the aforementioned areas and adequately assess their impact on tapping behavior.


 ,
, 



{kind=link}
{kind=link}
{kind=link}