
Combined Motor and Cognitive Rehabilitation: The Impact on Motor Performance in Patients with Mild Cognitive Impairment. Systematic Review and Meta-Analysis

 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
1.1. Description of the Condition
1.2. Description of the Intervention
1.3. Why It Is Important to Do This Review
1.4. Objectives
1.4.1. Primary Objective
1.4.2. Secondary Objectives
2. Materials and Methods
2.1. Criteria for Considering Studies for This Review
2.1.1. Types of Studies
- Randomized controlled trial (RCT) or quasi-RCT, controlled clinical trial, or case–control study;
- Patients with MCI (diagnosed by psychologists or psychiatrists, based on criteria proposed by European Consortium on Alzheimer’s Disease Working Group on MCI or with standard clinical examinations in line with the criteria of ICD-9-CM);
- Studies investigating MCI and motor impairments;
- Interventions must involve combined PCT compared to PT alone, no intervention, or placebo;
- Outcomes include motor functions (mobility, balance, gait speed, gait endurance, upper limb functions).
- Study design set as case report, review, study protocol, or case series;
- CT provided alone or PT provided alone as main intervention;
- All forms of telerehabilitation;
- All outcomes not related to motor function domains.
2.1.2. Types of Participants and Interventions
2.1.3. Types of Outcome Measures
2.2. Search Methods for Identification of Studies
Electronic Searches
2.3. Data Collection and Analysis
2.3.1. Selection of Studies
2.3.2. Data Extraction and Management with Missing Data
2.3.3. Assessment of Risk of Bias in Included Studies
- Low: low risk of bias.
- High: high risk of bias.
- Some concerns: when the reporting was insufficient, and some concerns were raised.
2.3.4. Measures of Treatment Effect
2.3.5. Assessment of Heterogeneity
3. Results
3.1. Description of the Studies
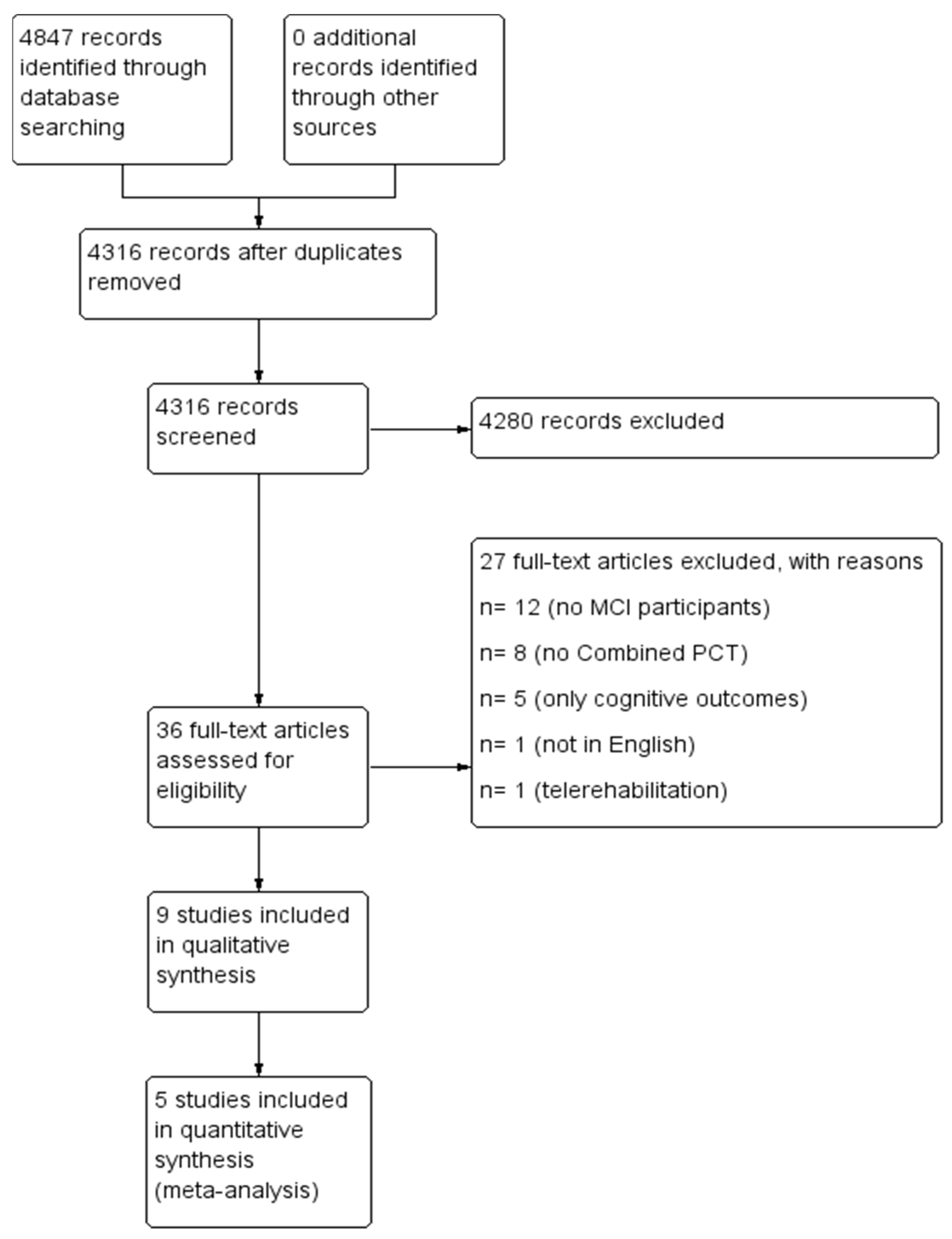
3.1.1. Results of the Search
3.1.2. Excluded Studies
3.1.3. Included Studies
3.2. Risk of Bias in Included Studies
- ➢
- Randomization process and allocation concealment (selection bias): Almost all studies were judged to have a low risk of bias. Studies by Combourieu Donnezan et al., Cintoli et al. and Simionatto et al. were found to have some concerns, as concealment is not mentioned and randomization is not detailed.
- ➢
- Deviation from intended intervention (performance bias): The studies by Hagovská (B) and Shimada et al. raised some concerns about the presence of bias, and Simionatto et al.’s study was classified as high risk due to absence of information about participants’ withdrawing, and no intention-to-treat analysis was performed. The six remaining studies showed a low risk of bias.
- ➢
- Missing outcome data (detection bias): A low risk of bias was found in all the included studies.
- ➢
- Measurement of the outcome (attrition bias): The study by Hagovská (B) was judged to raise some concerns. As Cintoli et al. (2019) did not provide information for outcome assessors and assessors’ knowledge of intervention received and Simionatto et al. (2021) did not detail the timeline of assessment and assessors were aware of intervention received, they were judged to have a high risk of bias. Furthermore, the study by Combourieu Donnezan et al. raised high risk of bias as measurement of the outcome have differed between intervention groups. The other five studies showed a low risk of bias.
- ➢
- Selection of the reporting result (reporting bias): The studies by Hagovska and Nagyova, Hagovská (B), Hagovská (A), Combourieu Donnezan et al. and Simionatto et al. were evaluated to have some concerns, whereas the four remaining studies were assessed to have a low risk of bias.
3.3. Effects of Intervention—Combined PCT Compared to Motor Treatment Alone
3.3.1. Mobility
3.3.2. Balance
3.3.3. Gait Speed
3.3.4. ADL
3.4. Effects of Intervention—Combined PCT Compared to No Intervention
3.4.1. Mobility
3.4.2. Gait Speed
4. Discussion
Summary of Main Results and Applicability of Evidence
5. Conclusions
- (a)
- Implications for practice
- (b)
- Implications for research
Limitations
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Appendix A
Appendix B
Appendix C
Appendix D
References
- Ziegler-Graham, K.; Brookmeyer, R.; Johnson, E.; Arrighi, H.M. Worldwide variation in the doubling time of Alzheimer’s disease incidence rates. Alzheimer’s Dement. 2008, 4, 316–323. [Google Scholar] [CrossRef] [PubMed]
- Huey, E.D.; Manly, J.J.; Tang, M.X.; Schupf, N.; Brickman, A.M.; Manoochehri, M.; Mez, J.; DeCarli, C.; Devanand, D.P.; Mayeux, R. Course and etiology of dysexecutive MCI in a community sample. Alzheimer’s Dement. 2013, 9, 632–639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gillis, C.; Mirzaei, F.; Potashman, M.; Ikram, M.A.; Maserejian, N. The incidence of mild cognitive impairment: A systematic review and data synthesis. Alzheimer’s Dement. 2019, 11, 248–256. [Google Scholar] [CrossRef] [PubMed]
- Firbank, M.J.; O’Brien, J.T.; Durcan, R.; Allan, L.M.; Barker, S.; Ciafone, J.; Donaghy, P.C.; Hamilton, C.A.; Lawley, S.; Lloyd, J.; et al. Mild cognitive impairment with Lewy bodies: Blood perfusion with arterial spin labelling. J. Neurol. 2021, 268, 1284–1294. [Google Scholar] [CrossRef]
- Palmer, K.; Di Iulio, F.; Varsi, A.E.; Gianni, W.; Sancesario, G.; Caltagirone, C.; Spalletta, G. Neuropsychiatric Predictors of Progression from Amnestic-Mild Cognitive Impairment to Alzheimer’s Disease: The Role of Depression and Apathy. J. Alzheimer’s Dis. 2010, 20, 175–183. [Google Scholar] [CrossRef] [Green Version]
- Petersen, R.C. Mild cognitive impairment as a diagnostic entity. J. Intern. Med. 2004, 256, 183–194. [Google Scholar] [CrossRef]
- Bradfield, N.I.; Ames, D. Mild cognitive impairment: Narrative review of taxonomies and systematic review of their prediction of incident Alzheimer’s disease dementia. BJPsych Bull. 2020, 44, 67–74. [Google Scholar] [CrossRef]
- Mangialasche, F.; Kivipelto, M.; Solomon, A.; Fratiglioni, L. Dementia prevention: Current epidemiological evidence and future perspective. Alzheimer’s Res. Ther. 2012, 4, 6. [Google Scholar] [CrossRef]
- Wimo, A.; Jonsson, L.; Gustavsson, A.; McDaid, D.; Ersek, K.; Georges, J.; Gulacsi, L.; Karpati, K.; Kenigsberg, P.; Valtonen, H. The economic impact of dementia in Europe in 2008-cost estimates from the Eurocode project. Int. J. Geriatr. Psychiatry 2011, 26, 825–832. [Google Scholar] [CrossRef] [Green Version]
- Albert, M.S.; DeKosky, S.T.; Dickson, D.; Dubois, B.; Feldman, H.H.; Fox, N.C.; Gamst, A.; Holtzman, D.M.; Jagust, W.J.; Petersen, R.C.; et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimer’s Dement. J. Alzheimer’s Assoc. 2011, 7, 270–279. [Google Scholar] [CrossRef] [Green Version]
- Nasreddine, Z.S.; Phillips, N.A.; Bedirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Arevalo-Rodriguez, I.; Smailagic, N.; Roque, I.F.M.; Ciapponi, A.; Sanchez-Perez, E.; Giannakou, A.; Pedraza, O.L.; Bonfill Cosp, X.; Cullum, S. Mini-Mental State Examination (MMSE) for the detection of Alzheimer’s disease and other dementias in people with mild cognitive impairment (MCI). Cochrane Database Syst. Rev. 2015, 3, 1–68. [Google Scholar] [CrossRef]
- Palumbo, R.; Di Domenico, A.; Piras, F.; Bazzano, S.; Zerilli, M.; Lorico, F.; Borella, E. Measuring global functioning in older adults with cognitive impairments using the Rasch model. BMC Geriatr. 2020, 20, 492. [Google Scholar] [CrossRef] [PubMed]
- Petersen, R.C.; Lopez, O.; Armstrong, M.J.; Getchius, T.S.D.; Ganguli, M.; Gloss, D.; Gronseth, G.S.; Marson, D.; Pringsheim, T.; Day, G.S.; et al. Practice guideline update summary: Mild cognitive impairment: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Neurology 2018, 90, 126–135. [Google Scholar] [CrossRef] [PubMed]
- Bahar-Fuchs, A.; Clare, L.; Woods, B. Cognitive training and cognitive rehabilitation for mild to moderate Alzheimer’s disease and vascular dementia. Cochrane Database Syst. Rev. 2013, 2013, 14651858. [Google Scholar] [CrossRef] [PubMed]
- Woods, B.; Aguirre, E.; Spector, A.E.; Orrell, M. Cognitive stimulation to improve cognitive functioning in people with dementia. Cochrane Database Syst. Rev. 2012, 2, CD005562. [Google Scholar] [CrossRef]
- Lobbia, A.; Carbone, E.; Faggian, S.; Gardini, S.; Piras, F.; Spector, A.; Borella, E. The efficacy of cognitive stimulation therapy (CST) for people with mild-to-moderate dementia: A review. Eur. Psychol. 2019, 24, 257–277. [Google Scholar] [CrossRef] [Green Version]
- Lauenroth, A.; Ioannidis, A.E.; Teichmann, B. Influence of combined physical and cognitive training on cognition: A systematic review. BMC Geriatr. 2016, 16, 141. [Google Scholar] [CrossRef] [Green Version]
- Zheng, G.; Xia, R.; Zhou, W.; Tao, J.; Chen, L. Aerobic exercise ameliorates cognitive function in older adults with mild cognitive impairment: A systematic review and meta-analysis of randomised controlled trials. Br. J. Sports Med. 2016, 50, 1443–1450. [Google Scholar] [CrossRef]
- Devenney, K.E.; Sanders, M.L.; Lawlor, B.; Olde Rikkert, M.G.M.; Schneider, S.; NeuroExercise Study, G. The effects of an extensive exercise programme on the progression of Mild Cognitive Impairment (MCI): Study protocol for a randomised controlled trial. BMC Geriatr. 2017, 17, 75. [Google Scholar] [CrossRef] [Green Version]
- Boecker, H.; Sprenger, T.; Spilker, M.E.; Henriksen, G.; Koppenhoefer, M.; Wagner, K.J.; Valet, M.; Berthele, A.; Tolle, T.R. The runner’s high: Opioidergic mechanisms in the human brain. Cereb. Cortex 2008, 18, 2523–2531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vogt, T.; Schneider, S.; Abeln, V.; Anneken, V.; Struder, H.K. Exercise, mood and cognitive performance in intellectual disability—A neurophysiological approach. Behav. Brain Res. 2012, 226, 473–480. [Google Scholar] [CrossRef] [PubMed]
- Chaddock, L.; Hillman, C.H.; Pontifex, M.B.; Johnson, C.R.; Raine, L.B.; Kramer, A.F. Childhood aerobic fitness predicts cognitive performance one year later. J. Sports Sci. 2012, 30, 421–430. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Pinilla, F.; Hillman, C. The influence of exercise on cognitive abilities. Compr. Physiol. 2013, 3, 403–428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erickson, K.I.; Voss, M.W.; Prakash, R.S.; Basak, C.; Szabo, A.; Chaddock, L.; Kim, J.S.; Heo, S.; Alves, H.; White, S.M.; et al. Exercise training increases size of hippocampus and improves memory. Proc. Natl. Acad. Sci. USA 2011, 108, 3017–3022. [Google Scholar] [CrossRef] [Green Version]
- Holzschneider, K.; Wolbers, T.; Roder, B.; Hotting, K. Cardiovascular fitness modulates brain activation associated with spatial learning. Neuroimage 2012, 59, 3003–3014. [Google Scholar] [CrossRef]
- Budde, H.; Brunelli, A.; Machado, S.; Velasques, B.; Ribeiro, P.; Arias-Carrion, O.; Voelcker-Rehage, C. Intermittent maximal exercise improves attentional performance only in physically active students. Arch. Med. Res. 2012, 43, 125–131. [Google Scholar] [CrossRef]
- Voss, M.W.; Chaddock, L.; Kim, J.S.; VanPatter, M.; Pontifex, M.B.; Raine, L.B.; Cohen, N.J.; Hillman, C.H.; Kramer, A.F. Aerobic fitness is associated with greater efficiency of the network underlying cognitive control in preadolescent children. Neuroscience 2011, 199, 166–176. [Google Scholar] [CrossRef] [Green Version]
- Jackson, P.A.; Pialoux, V.; Corbett, D.; Drogos, L.; Erickson, K.I.; Eskes, G.A.; Poulin, M.J. Promoting brain health through exercise and diet in older adults: A physiological perspective. J. Physiol. 2016, 594, 4485–4498. [Google Scholar] [CrossRef]
- Bamidis, P.D.; Vivas, A.B.; Styliadis, C.; Frantzidis, C.; Klados, M.; Schlee, W.; Siountas, A.; Papageorgiou, S.G. A review of physical and cognitive interventions in aging. Neurosci. Biobehav. Rev. 2014, 44, 206–220. [Google Scholar] [CrossRef]
- Priest, A.W.; Salamon, K.B.; Hollman, J.H. Age-related differences in dual task walking: A cross sectional study. J. Neuroeng. Rehabil. 2008, 5, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaefer, S.; Schumacher, V. The interplay between cognitive and motor functioning in healthy older adults: Findings from dual-task studies and suggestions for intervention. Gerontology 2011, 57, 239–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simionatto, J.; Cruz, A.D.F.C.; Campos, A.P.S.M.; Bottini, D.A.M.C.; Ansai, J.H.; de Souza Pegorare, A.B.G.; Barbosa, S.R.M. Effects of manual motor and cognitive training on functionality and cognition of institutionalized elderly people. Mundo da Saúde 2021, 44, 539–549. [Google Scholar] [CrossRef]
- Shimada, H.; Makizako, H.; Doi, T.; Park, H.; Tsutsumimoto, K.; Verghese, J.; Suzuki, T. Effects of Combined Physical and Cognitive Exercises on Cognition and Mobility in Patients with Mild Cognitive Impairment: A Randomized Clinical Trial. J. Am. Med. Dir. Assoc. 2018, 19, 584–591. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Cintoli, S.; Radicchi, C.; Noale, M.; Maggi, S.; Meucci, G.; Tognoni, G.; Bonuccelli, U.; Sale, A.; Berardi, N.; Maffei, L.; et al. Effects of combined training on neuropsychiatric symptoms and quality of life in patients with cognitive decline. Aging Clin. Exp. Res. 2019, 33, 1249–1257. [Google Scholar] [CrossRef]
- Combourieu Donnezan, L.; Perrot, A.; Belleville, S.; Bloch, F.; Kemoun, G. Effects of simultaneous aerobic and cognitive training on executive functions, cardiovascular fitness and functional abilities in older adults with mild cognitive impairment. Ment. Health Phys. Act. 2018, 15, 78–87. [Google Scholar] [CrossRef] [Green Version]
- Hagovská, M.; Takáč, P.; Dzvoník, O. Effect of a combining cognitive and balanced training on the cognitive, postural and functional status of seniors with a mild cognitive deficit in a randomized, controlled trial. Eur. J. Phys. Rehabil. Med. 2016, 52, 101–109. [Google Scholar]
- Hagovská, M.; Olekszyová, Z. Impact of the combination of cognitive and balance training on gait, fear and risk of falling and quality of life in seniors with mild cognitive impairment. Geriatr. Gerontol. Int. 2016, 16, 1043–1050. [Google Scholar] [CrossRef]
- Hagovska, M.; Nagyova, I. The transfer of skills from cognitive and physical training to activities of daily living: A randomised controlled study. Eur. J. Ageing 2017, 14, 133–142. [Google Scholar] [CrossRef]
- Lipardo, D.S.; Tsang, W.W.N. Effects of combined physical and cognitive training on fall prevention and risk reduction in older persons with mild cognitive impairment: A randomized controlled study. Clin. Rehabil. 2020, 34, 773–782. [Google Scholar] [CrossRef] [PubMed]
- Middleton, L.E.; Ventura, M.I.; Santos-Modesitt, W.; Poelke, G.; Yaffe, K.; Barnes, D.E. The Mental Activity and eXercise (MAX) trial: Effects on physical function and quality of life among older adults with cognitive complaints. Contemp. Clin. Trials 2018, 64, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions Version 6.2; Cochrane Training: London, UK, February 2021; Available online: www.training.cochrane.org/handbook (accessed on 26 November 2021).
- Melsen, W.G.; Bootsma, M.C.J.; Rovers, M.M.; Bonten, M.J.M. The effects of clinical and statistical heterogeneity on the predictive values of results from meta-analyses. Clin. Microbiol. Infect. 2014, 20, 123–129. [Google Scholar] [CrossRef] [Green Version]
- Woollacott, M.; Shumway-Cook, A. Attention and the control of posture and gait: A review of an emerging area of research. Gait Posture 2002, 16, 1–14. [Google Scholar] [CrossRef]
- Perin, C.; Bolis, M.; Limonta, M.; Meroni, R.; Ostasiewicz, K.; Cornaggia, C.M.; Alouche, S.R.; da Silva Matuti, G.; Cerri, C.G.; Piscitelli, D. Differences in Rehabilitation Needs after Stroke: A Similarity Analysis on the ICF Core Set for Stroke. Int. J. Environ. Res. Public Health 2020, 17, 4291. [Google Scholar] [CrossRef] [PubMed]
- Cornelis, E.; Gorus, E.; Beyer, I.; Bautmans, I.; De Vriendt, P. Early diagnosis of mild cognitive impairment and mild dementia through basic and instrumental activities of daily living: Development of a new evaluation tool. PLoS Med. 2017, 14, e1002250. [Google Scholar] [CrossRef]








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kiper, P.; Richard, M.; Stefanutti, F.; Pierson-Poinsignon, R.; Cacciante, L.; Perin, C.; Mazzucchelli, M.; Viganò, B.; Meroni, R. Combined Motor and Cognitive Rehabilitation: The Impact on Motor Performance in Patients with Mild Cognitive Impairment. Systematic Review and Meta-Analysis. J. Pers. Med. 2022, 12, 276. https://doi.org/10.3390/jpm12020276
Kiper P, Richard M, Stefanutti F, Pierson-Poinsignon R, Cacciante L, Perin C, Mazzucchelli M, Viganò B, Meroni R. Combined Motor and Cognitive Rehabilitation: The Impact on Motor Performance in Patients with Mild Cognitive Impairment. Systematic Review and Meta-Analysis. Journal of Personalized Medicine. 2022; 12(2):276. https://doi.org/10.3390/jpm12020276
Chicago/Turabian StyleKiper, Pawel, Michelle Richard, Françoise Stefanutti, Romain Pierson-Poinsignon, Luisa Cacciante, Cecilia Perin, Miryam Mazzucchelli, Barbara Viganò, and Roberto Meroni. 2022. "Combined Motor and Cognitive Rehabilitation: The Impact on Motor Performance in Patients with Mild Cognitive Impairment. Systematic Review and Meta-Analysis" Journal of Personalized Medicine 12, no. 2: 276. https://doi.org/10.3390/jpm12020276