
The Influence of the Locus of Control Construct on the Efficacy of Physiotherapy Treatments in Patients with Chronic Pain: A Systematic Review

 and
and
Abstract
:1. Introduction
2. Materials and Methods
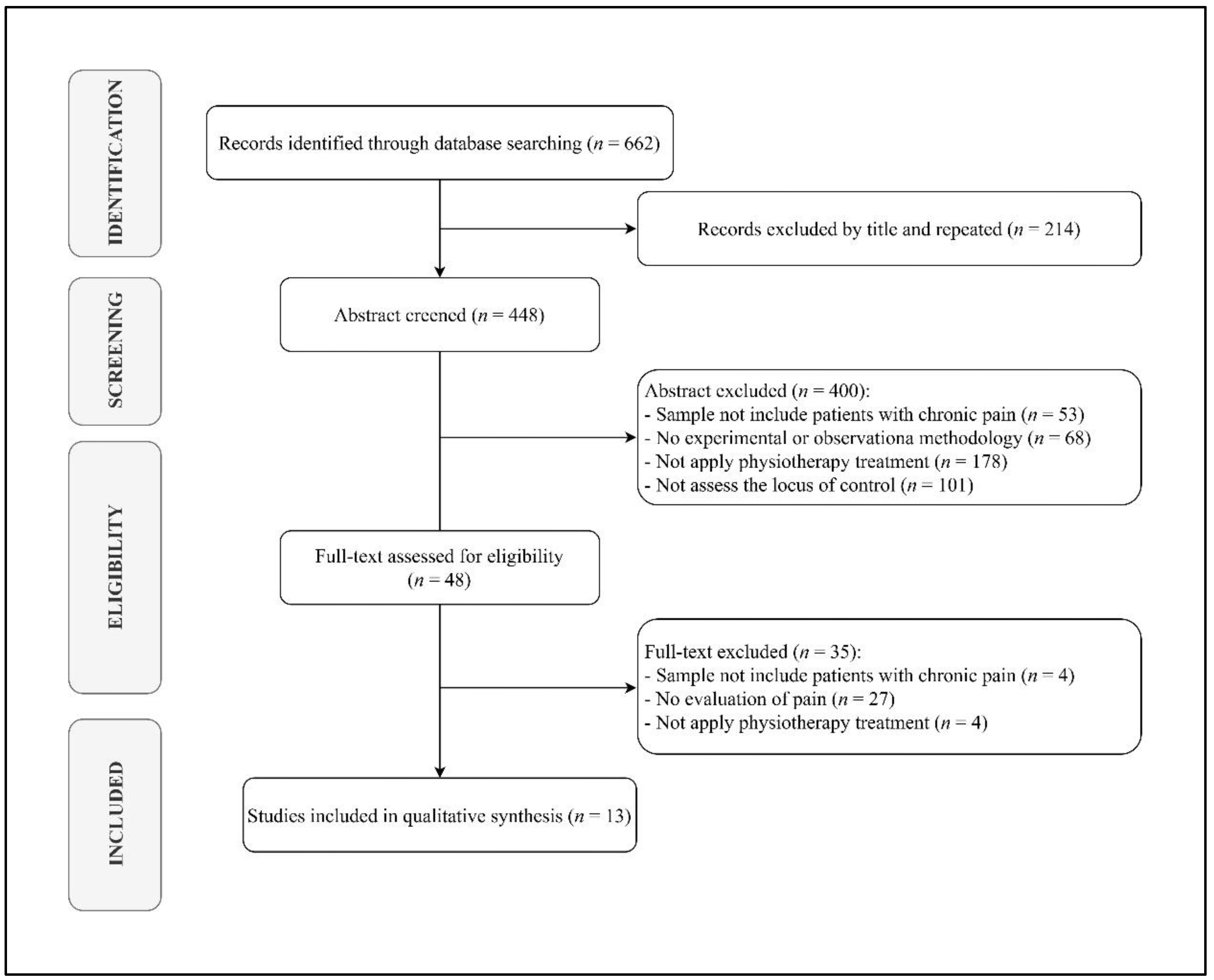
3. Results
3.1. Studies Included
3.2. Treatments Applied
3.3. Assessment Tools Used
3.4. Results Obtained
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Treede, R.-D.; Rief, W.; Barke, A.; Aziz, Q.; Bennett, M.I.; Benoliel, R.; Cohen, M.; Evers, S.; Finnerup, N.B.; First, M.B.; et al. A classification of chronic pain for ICD-11. Pain 2015, 156, 1003–1007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malfliet, A.; Coppieters, I.; Van Wilgen, P.; Kregel, J.; De Pauw, R.; Dolphens, M.; Ickmans, K. Brain changes associated with cognitive and emotional factors in chronic pain: A systematic review. Eur. J. Pain 2017, 21, 769–786. [Google Scholar] [CrossRef] [PubMed]
- Chapman, C.; Nakamura, Y. A Passion of the Soul: An Introduction to Pain for Consciousness Researchers. Conscious. Cogn. 1999, 8, 391–422. [Google Scholar] [CrossRef] [PubMed]
- Breivik, H.; Collett, B.; Ventafridda, V.; Cohen, R.; Gallacher, D. Survey of chronic pain in Europe: Prevalence, impact on daily life, and treatment. Eur. J. Pain 2006, 10, 287–333. [Google Scholar] [CrossRef]
- Gatchel, R.J.; McGeary, D.D.; McGeary, C.A.; Lippe, B. Interdisciplinary chronic pain management: Past, present, and future. Am. Psychol. 2014, 69, 119–130. [Google Scholar] [CrossRef]
- Gobina, I.; Villberg, J.; Välimaa, R.; Tynjälä, J.; Whitehead, R.; Cosma, A.; Brooks, F.; Cavallo, F.; Ng, K.; de Matos, M.G.; et al. Prevalence of self-reported chronic pain among adolescents: Evidence from 42 countries and regions. Eur. J. Pain 2018, 23, 316–326. [Google Scholar] [CrossRef]
- Andrews, P.; Steultjens, M.; Riskowski, J. Chronic widespread pain prevalence in the general population: A systematic review. Eur. J. Pain 2017, 22, 5–18. [Google Scholar] [CrossRef] [Green Version]
- Cimas, M.; Ayala, A.; Sanz, B.; Agulló-Tomás, M.; Escobar, A.; Forjaz, M. Chronic musculoskeletal pain in European older adults: Cross-national and gender differences. Eur. J. Pain 2017, 22, 333–345. [Google Scholar] [CrossRef]
- Herman, P.M.; Broten, N.; Lavelle, T.A.; Sorbero, M.E.; Coulter, I.D. Health Care Costs and Opioid Use Associated With High-impact Chronic Spinal Pain in the United States. Spine 2019, 44, 1154–1161. [Google Scholar] [CrossRef]
- Rudd, R.A.; Aleshire, N.; Zibbell, J.E.; Gladden, R.M. Increases in Drug and Opioid Overdose Deaths—United States, 2000–2014. MMWR. Morb. Mortal. Wkly. Rep. 2016, 64, 1378–1382. [Google Scholar] [CrossRef] [Green Version]
- Coronado, R.A.; Bialosky, J.E. Manual physical therapy for chronic pain: The complex whole is greater than the sum of its parts. J. Man. Manip. Ther. 2017, 25, 115–117. [Google Scholar] [CrossRef] [Green Version]
- Becker, W.C.; Dorflinger, L.; Edmond, S.N.; Islam, L.; Heapy, A.A.; Fraenkel, L. Barriers and facilitators to use of non-pharmacological treatments in chronic pain. BMC Fam. Pr. 2017, 18, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Clark, S.; Horton, R. Low back pain: A major global challenge. Lancet 2018, 391, 2302. [Google Scholar] [CrossRef]
- Foster, N.E.; Anema, J.R.; Cherkin, D.; Chou, R.; Cohen, S.P.; Gross, D.P.; Ferreira, P.H.; Fritz, J.M.; Koes, B.W.; Peul, W.; et al. Prevention and treatment of low back pain: Evidence, challenges, and promising directions. Lancet 2018, 391, 2368–2383. [Google Scholar] [CrossRef]
- Náfrádi, L.; Nakamoto, K.; Schulz, P.J. Is patient empowerment the key to promote adherence? A systematic review of the relationship between self-efficacy, health locus of control and medication adherence. PLoS ONE 2017, 12, e0186458. [Google Scholar] [CrossRef] [Green Version]
- Galvin, B.M.; Randel, A.E.; Collins, B.J.; Johnson, R.E. Changing the focus of locus (of control): A targeted review of the locus of control literature and agenda for future research. J. Organ. Behav. 2018, 39, 820–833. [Google Scholar] [CrossRef]
- Edwards, R.R.; Dworkin, R.H.; Sullivan, M.D.; Turk, D.C.; Wasan, A.D. The Role of Psychosocial Processes in the Development and Maintenance of Chronic Pain. J. Pain 2016, 17, T70–T92. [Google Scholar] [CrossRef] [Green Version]
- Toscano, A.; Blanchin, M.; Bourdon, M.; Antignac, A.B.; Sébille, V. Longitudinal associations between coping strategies, locus of control and health-related quality of life in patients with breast cancer or melanoma. Qual. Life Res. 2020, 29, 1271–1279. [Google Scholar] [CrossRef]
- Berglund, E.; Lytsy, P.; Westerling, R. The influence of locus of control on self-rated health in context of chronic disease: A structural equation modeling approach in a cross sectional study. BMC Public Health 2014, 14, 492. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Howick, J.; Chalmers, I.; Glasziou, P.; Greenhalgh, T.; Heneghan, C.; Liberati, A.; Moschetti, I.; Phillips, B.; Thornton, H. The 2011 Oxford CEBM Evidence Levels of Evidence (Introductory Document). Oxford Centre for Evidence-Based Medicine. Available online: https://www.cebm.ox.ac.uk/resources/levels-of-evidence/ocebm-levels-of-evidence (accessed on 17 January 2020).
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Groeneweg, R.; Haanstra, T.; Bolman, C.A.; Oostendorp, R.A.; van Tulder, M.W.; Ostelo, R.W. Treatment success in neck pain: The added predictive value of psychosocial variables in addition to clinical variables. Scand. J. Pain 2017, 14, 44–52. [Google Scholar] [CrossRef]
- Linden, M.; Scherbe, S.; Cicholas, B. Randomized controlled trial on the effectiveness of cognitive behavior group therapy in chronic back pain patients. J. Back Musculoskelet. Rehabilitation 2014, 27, 563–568. [Google Scholar] [CrossRef]
- Farin, E.; Gramm, L.; Schmidt, E. The patient–physician relationship in patients with chronic low back pain as a predictor of outcomes after rehabilitation. J. Behav. Med. 2012, 36, 246–258. [Google Scholar] [CrossRef]
- Xu, J.; Twiggs, J.; Parker, D.; Negus, J. The Association Between Anxiety, Depression, and locus of control With Patient Outcomes Following Total Knee Arthroplasty. J. Arthroplast. 2019, 35, 720–724. [Google Scholar] [CrossRef] [Green Version]
- Musich, S.; Wang, S.S.; Slindee, L.; Kraemer, S.; Yeh, C.S. The association of pain locus of control with pain outcomes among older adults. Geriatr. Nurs. 2020, 41, 521–529. [Google Scholar] [CrossRef]
- Zuercher-Huerlimann, E.; Stewart, J.A.; Egloff, N.; von Känel, R.; Studer, M.; Holtforth, M.G. Internal health locus of control as a predictor of pain reduction in multidisciplinary inpatient treatment for chronic pain: A retrospective study. J. Pain Res. 2019, 12, 2095–2099. [Google Scholar] [CrossRef] [Green Version]
- Stewart, J.A.; Aebischer, V.; Egloff, N.; Wegmann, B.; Von Känel, R.; Vögelin, E.; Holtforth, M.G. The Role of Health locus of control in Pain Intensity Outcome of Conservatively and Operatively Treated Hand Surgery Patients. Int. J. Behav. Med. 2018, 25, 374–379. [Google Scholar] [CrossRef]
- Pereira, M.G.; Roios, E. Functional disability in patients with low back pain: The mediator role of suffering and beliefs about pain control in patients receiving physical and chiropractic treatment. Braz. J. Phys. Ther. 2017, 21, 465–472. [Google Scholar] [CrossRef]
- Keedy, N.H.; Keffala, V.J.; Altmaier, E.M.; Chen, J.J. Health locus of control and Self-Efficacy Predict Back Pain Rehabilitation Outcomes. Iowa Orthop. J. 2014, 34, 158–165. [Google Scholar]
- Oliveira, T.H.; Oliveira, V.C.; Melo, R.C.; Melo, R.M.; Freitas, A.E.; Ferreira, P.H. Patients in treatment for chronic low back pain have higher externalised beliefs: A cross-sectional study. Rev. Bras. J. Fisioter. 2012, 16, 35–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopez-Olivo, M.A.; Landon, G.C.; Siff, S.J.; Edelstein, D.; Pak, C.; Kallen, M.A.; Stanley, M.; Zhang, H.; Robinson, K.C.; E Suarez-Almazor, M. Psychosocial determinants of outcomes in knee replacement. Ann. Rheum. Dis. 2011, 70, 1775–1781. [Google Scholar] [CrossRef] [PubMed]
- Dhurve, K.; Scholes, C.; El-Tawil, S.; Shaikh, A.; Weng, L.K.; Levin, K.; Fritsch, B.; Parker, D.; Coolican, M. Multifactorial analysis of dissatisfaction after primary total knee replacement. Knee 2017, 24, 856–862. [Google Scholar] [CrossRef]
- de Souza-Batista, A.A.; Rezende-Diniz, L.S.; Cunha-Oliveira, V.; Venturini, C. Locus of control in active physical therapy treatment for non-specific chronic low back pain. Phys. Ther. Mov. 2015, 28, 495–500. [Google Scholar] [CrossRef]
- Musich, S.; Wang, S.S.; Slindee, L.; Kraemer, S.; Yeh, C.S. The impact of internal locus of control on healthcare utilization, expenditures, and health status across older adult income levels. Geriatr. Nurs. 2019, 41, 274–281. [Google Scholar] [CrossRef] [PubMed]
- O’Keeffe, M.; O’Sullivan, P.; Purtill, H.; Bargary, N.; O’Sullivan, K. Cognitive functional therapy compared with a group-based exercise and education intervention for chronic low back pain: A multicentre randomised controlled trial (RCT). Br. J. Sports Med. 2019, 54, 782–789. [Google Scholar] [CrossRef] [PubMed]
- Kinney, M.; Seider, J.; Beaty, A.F.; Coughlin, K.; Dyal, M.; Clewley, D. The impact of therapeutic alliance in physical therapy for chronic musculoskeletal pain: A systematic review of the literature. Physiother. Theory Pr. 2018, 36, 886–898. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Nogueira, O.; Botella-Rico, J.; Martínez-González, M.C.; Leal-Clavel, M.; Morera-Balaguer, J.; Moreno-Poyato, A.R. Construction and content validation of a measurement tool to evaluate person-centered therapeutic relationships in physiotherapy services. PLoS ONE. 2020, 15, e0228916. [Google Scholar] [CrossRef]
- Wahl, A.K.; Opseth, G.; Nolte, S.; Osborne, R.H.; Bjørke, G.; Mengshoel, A.M. Is regular use of physiotherapy treatment associated with health locus of control and self-management competency? A study of patients with musculoskeletal disorders undergoing physiotherapy in primary health care. Musculoskelet. Sci. Pract. 2018, 36, 43–47. [Google Scholar] [CrossRef]
- Hartvigsen, J.; Hancock, M.J.; Kongsted, A.; Louw, Q.; Ferreira, M.L.; Genevay, S.; Hoy, D.; Karppinen, J.; Pransky, G.; Sieper, J.; et al. What low back pain is and why we need to pay attention. Lancet 2018, 391, 2356–2367. [Google Scholar] [CrossRef] [Green Version]
- Zusman, M. Belief reinforcement: One reason why costs for low back pain have not decreased. J. Multidiscip. Health 2013, 6, 197–204. [Google Scholar] [CrossRef] [Green Version]
- Hruschak, V.; Cochran, G. Psychosocial predictors in the transition from acute to chronic pain: A systematic review. Psychol. Health Med. 2017, 23, 1151–1167. [Google Scholar] [CrossRef]
- Darlow, B.; Fullen, B.M.; Dean, S.; Hurley, D.A.; Baxter, G.D.; Dowell, A. The association between health care professional attitudes and beliefs and the attitudes and beliefs, clinical management, and outcomes of patients with low back pain: A systematic review. Eur. J. Pain 2012, 16, 3–17. [Google Scholar] [CrossRef]


{kind=link}
| Database | Search Equation |
|---|---|
| Scopus | (MH “Physical therapy modalities”) AND (MH “Chronic pain”) AND (MH “Internal-external control”) (MH “Physical therapy modalities”) AND (MH “Chronic pain”) AND (MH “Self-management”) (MH “Chronic pain”) AND (MH “Internal-external control”) AND “Physical therapy” (MH “Chronic pain”) AND (MH “Internal-external control”) AND “Physiotherapy” (MH “Chronic pain”) AND (MH “Self-management”) AND “Physical therapy” (MH “Chronic pain”) AND (MH “Self-management”) AND “Physiotherapy” |
| Pubmed | (“Physical therapy modalities”(Mesh)) AND (“Chronic pain”(Mesh)) AND (“Internal-external control”(Mesh)) (“Physical therapy modalities”(Mesh)) AND (“Chronic pain”(Mesh)) AND (“Self-management”(Mesh)) (“Chronic pain”(Mesh)) AND (“Internal-external control”(Mesh)) AND “Physical therapy” (“Chronic pain”(Mesh)) AND (“Internal-external control”(Mesh)) AND “Physiotherapy” (“Chronic pain”(Mesh)) AND (“Self-management”(Mesh)) AND “Physical therapy” (“Chronic pain”(Mesh)) AND (“Self-management”(Mesh)) AND “Physiotherapy” |
| Web of Science | TOPIC: (“Physical therapy modalities”) AND TOPIC: (“Chronic pain”) AND TOPIC: (“Internal-external control”) TOPIC: (“Physical therapy modalities”) AND TOPIC: (“Chronic pain”) AND TOPIC: (“Self-management”) TOPIC: (“Chronic pain”) AND TOPIC: (“Internal-external control”) AND TOPIC: (“Physical therapy”) TOPIC: (“Chronic pain”) AND TOPIC: (“Internal-external control”) AND TOPIC: (“Physiotherapy”) TOPIC: (“Chronic pain”) AND TOPIC: (“Self-management”) AND TOPIC: (“Physical therapy”) TOPIC: (“Chronic pain”) AND TOPIC: (“Self-management”) AND TOPIC: (“Physiotherapy”) |
| Science Direct | (MH “Physical therapy modalities”) AND (MH “Chronic pain”) AND (MH “Internal external locus of control”) (MH “Physical therapy modalities”) AND (MH “Chronic pain”) AND (MH “Self management”) (MH “Chronic pain”) AND (MH “Internal external locus of control”) AND (MH “Physical therapy” OR “Physiotherapy” OR “Rehabilitation”) (MH “Chronic pain”) AND (MH “Self management”) AND (MH “Physical therapy” OR “Physiotherapy” OR “Rehabilitation”) |
| Authors | Design | Sample Size | Inclussion Criteria | Exclussion Criteria | JADAD Scale | LE | |||
|---|---|---|---|---|---|---|---|---|---|
| RD * | BD ** | WD *** | FS | ||||||
| Groeneweg et al. (2017) | RCT | 181 | Patients included were aged 18–70, with nonspecific subacute and chronic neck pain, with or without radiation to the shoulder region or the upper extremities, and with or without headache | Presence of red flags, pregnancy, whiplash trauma as cause, and treatment for neck pain in the previous three months | 1 | 0 | 1 | 2 | 1 |
| Pereira et al. (2017) | RCT | 338 | Age between 18 and 65, a diagnosis of common chronic lower back pain for a period of more than three months being attributed to muscle ligaments and mechanical and degenerative causes (according to the diagnostic criteria defined by the Portuguese Association of Rheumatology | Critical limitation on movement or diagnosis of severe psychiatric illness according to the patient’s medical chart | 0 | 0 | 0 | 0 | 2 |
| de Souza et al. (2015) | CSS | 28 | Age between 18 and 55 years, presenting low back pain for more than three months, currently undergoing active treatment with low back stabilization exercises and educational guidance with emphasis on self-treatment and control of their health condition | Patients presenting specific diagnosis for low back pain, such as tumors, trauma, infections, inflammatory disorders and motor and/or cognitive neurological deficit, nor being pregnant or in six months or less of postpartum | 0 | 0 | 0 | 0 | 2 |
| Keedy et al. (2014) | RS | 61 | Patients completing the two-week chronic spine rehabilitation program involving an interdisciplinary treatment approach including physical therapy, cognitive-behavioral group therapy, vocational rehabilitation, and group discussions with a physiatrist. Participants were at least 18 years old and English-speaking. | Not specified | 0 | 0 | 0 | 0 | 2 |
| Linden et al. (2017) | RCT | 103 | Patients were suffering from back pain for at least six months according to the medical records and the assessment of the treating physicians. | Patients excluded if they were applying for early retirement | 1 | 0 | 1 | 2 | 1 |
| Oliveira et al. (2012) | CSS | 100 | Patients with symptoms of nonspecific LBP, with symptom duration of 3 months and over, between 18 and 60 years old and being treated or awaiting treatment with a physical therapist for LBP. | Patients with fracture, tumor, infectious or inflammatory diseases of the spine and sciatica | 0 | 0 | 0 | 0 | 2 |
| Musich et al. (2020) | CSS | 3824 | Patients over 65 years of age with a minimum of 12 months’ continuous medical and drug plan enrollment with back pain, osteoarthritis or rheumatoid arthritis | Patients with cancer, trauma or drug abuse | 0 | 0 | 0 | 0 | 2 |
| López-Olivo et al. (2011) | PS | 241 | Patients with radiological diagnosis of knee osteoarthritis; first knee replacement (previous hip replacement was allowed); adequate cognitive status; living in the community (not in long-term care facilities) and with ability to communicate in English | Patients in revision surgery; with inflammatory arthropathies; neurological disorders; Paget’s syndrome or bone disorders; litigation process related to surgery and patients seeking or receiving workers’ compensation benefits. | 0 | 0 | 1 | 1 | 2 |
| Farin et al. (2011) | PS | 668 | Patients with chronic lower back pain for at least 6 months | Patients with specific low back pain due to tumors or inflammatory diseases | 0 | 0 | 0 | 0 | 2 |
| Xu et al. (2020) | CSS | 136 | Patients over 18 years old, primary unilateral or bilateral total knee arthroplasty, and English speakers | Previous septic joint, revision surgery, dementia, or were unable to return for all extra follow-up visits. | 0 | 0 | 0 | 0 | 2 |
| Zuerche-Huerlimn et al. (2019) | RS | 225 | Patients with somatoform pain disorder or suffering from a comorbid chronic pain condition with a mental or behavioral disorder confirmed by a clinician | Not specified | 0 | 0 | 0 | 0 | 2 |
| Stewart et al. (2018) | PS | 125 | Patients admitted to a tertiary hand surgery center with at least 18 years old | No selection criteria were implemented regarding pain levels at entry or comorbid diagnoses | 0 | 0 | 1 | 1 | 2 |
| Dhurve et al. (2017) | CSS | 301 | Patients underwent a primary unilateral total knee replacement using computer navigation, operated by two consultant orthopedic surgeons with a follow-up period ranging from one to five years. | Patients with bilateral total knee replacement or revision cases were excluded. | 0 | 0 | 0 | 0 | 2 |
| Authors | Intervention | Assessment Tools | Outcomes | |
|---|---|---|---|---|
| Experimental Group | Control Group | |||
| Xu et al. (2020) | Not described | --- | Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), Medical Outcomes Study SF-12 – Mental Score, Hospital Anxiety and Depression Scales and LoC Questionnaire | Higher scores in preoperative depression and anxiety worse WOMAC score at 6 and 18 months. Low SF-12 score worst total WOMAC score at 6 weeks. Highest internal LOC less pain and better score in WOMAC at 18 weeks. Higher external LoC was not correlated with lower WOMAC scores. Patients with preoperative internal LOC, total WOMAC better at one year than internal LOC patients who switched to external |
| Musich et al. (2020) | Not described | --- | Pain, Enjoyment and General Activity Assessment Scale (PEG), Veterans Rand 12, Patient Health Quesionnaire-2, Pittsburgh Sleep Quality Index, Multidimensional Health LoC and Six-item Brief Resilience Scale | The prevalence of internal LoC was 30%, external LoC (others) 34% and external LoC (chance or luck) 36%. The internal LOC was protective, reducing the likelihood of moderate pain by 30% and severe pain by 50%. The internal LOC was as protective of pain severity as having high resilience and diverse social networks. External LOC was associated with a 10% increase in moderate pain, while the external LOC subscale associated with luck was associated with a 50% increase in the likelihood of severe pain |
| Zuercher-Huerlimn et al. (2019) | Not described | --- | German Health and Illness Related Control Beliefs and Numerical Rating Scale | High values of internal LoC showed less pain at the end of treatment. Internal LoC showed predictive value of decreased pain intensity |
| Stewart et al. (2018) | Not described | --- | German Health and Illness Related Control Beliefs, Hospital Anxiety and Depression Scales and Visual Analogue Scale | Decrease in pain intensity, predominantly in subjects with severe pain. High levels of external LoC dependent on health professionals favour a decrease in pain intensity |
| Dhurve et al. (2017) | Not described | --- | Pain Catastrophizing Scale, 21-Question Depression, Anxiety and Stress Scale, Multidimensional Health LoC, Oxford Knee Score (OKS) and Veterans Rand 12. | Persistent pain was the most common reason for dissatisfaction. Dissatisfied patients reported a significantly higher mean PCS score, higher depression component and lower internal locus of control. The dissatisfied group exhibited reduced improvement in OKS and range of movement, as well as a lower preoperative grade of osteoarthritis compared to satisfied patients |
| Groeneweg et al. (2017) | Passive mobilization techniques very gently and generally pain-free | Active exercises, improving strength, mobility, movement coordination, and relaxation, manual traction for pain reduction, and massage therapy for relaxation. | Credibility Expectancy Questionnaire, Multidimensional Health LoC, Fear Avoidance Belief Questionnaire, Neck Disability Index, Numeric Rating Scale on Pain, Medical Outcomes Study Short Form 36 and Global Perceived Effect | Treatment outcome expectancy predicted outcome success, in addition to clinical and demographic variables. Expectancy explained additional variance, ranging from 6% (pain) to 17% (functioning) at 7 weeks, and 8% (pain) to 16% (functioning) at 26 weeks. Locus of control and fear avoidance beliefs did not add significantly to predicting outcome |
| Pereira et al. (2017) | Physiotherapy treatment | Chiropractic treatment | Sociodemographic questionnaire, Beliefs about Pain Control Questionnaire, Illness Subjective Suffering Inventory, Oswestry Disability Questionnaire and Hospital Anxiety and Depression Scales | Suffering was a mediator in the relationship between depression and functional disability in both treatment groups. Only beliefs related to external chance events mediated the relationship between depression and functional disability in the physical therapy group, but not in the chiropractic treatment group |
| De Souza et al. (2015) | Not described | --- | Oswestry Disability Index, McGill Pain Questionnaire, Multidimensional Health LoC | Participants presented a mean of 26 points scale for disability and 6.39 for pain. 82.1% of the participants presented higher rates for internal locus of control. Patients undergoing active treatment for chronic low back pain believe they are responsible for their own condition |
| Keedy et al. (2014) | Not described | --- | Multidimensional Health LoC, Chronic Pain Self-Efficacy Scale, Medical Outcomes Study Short Form 36, Oswestry Disability Index and Beck Depression Inventory-II | Higher internal and lower doctor health locus of control, and higher self-efficacy at baseline predicted higher lift scores one month after treatment. Higher baseline self-efficacy also predicted better physical functioning and lower disability at one month |
| Linden et al. (2014) | Cognitive behavior group therapy for back pain | General orthopedic inpatient treatment, sport therapy and physiotherapy, balneotherapy, massages, or electrotherapy | Fear Avoidance Beliefs Questionnaire (FABQ), Visual Analogue Scale for Pain, Pain Disability Index and Symptom Checklist | In both groups there was a significant improvement in Symptom Checklist, the Rating of Health LoC Attributions, FABQ and Visual Analogue Scale for Pain. There are significant interactions between treatment group and Visual Analogue Scale for Pain and the FABQ, showing a superior improvement in the intervention group |
| Oliveira et al. (2012) | Patients undergoing physiotherapy treatment (at least one session) | Participants awaiting treatment recruited from waiting lists or from first consultations | Multidimensional Health LoC, Visual Analogue Scale and Roland Morris Disability Questionnaire | Health locus of control was found to be different between treatment and control groups. Participants being treated had higher external LoC and lower internal LoC than control group |
| López-Olivo et al. (2011) | Not described | --- | Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), Knee Society Rating System (KSRS), Coping Responses to Stressors Inventory, Multidimensional Health LoC, Arthritis Self-Efficacy Scale and Life Orientation Test | Higher pain scores were associated with lower education and problem-solving skills, higher dysfunction and lower internal health LoC. Worse WOMAC scores were associated with less support, depression and decreased coping skills for problem solving. Older age, less education, depression, and less coping skills were significantly associated with lower total KSRS scores. A worse pain, range of movement, and knee stability score was predicted by lower problem-solving ability |
| Farin et al. (2011) | Not described | --- | Perceived Involvement in Care Scale, Trust in Physician, General Patient Satisfaction, Communication Behavior Questionnaire, Visual Analogue Scale, Oswestry Disability Questionnaire, Fear Avoidance Beliefs Questionnaire, Control Beliefs Concerning Illness and Health and Illness perception questionnaire | The patient–physician relationship is significantly associated with the outcome. In the medium term (6 months after rehabilitation), the effect of the patient–physician relationship is clearer than in the short term (end of rehabilitation). In addition, risk factors for less improvement are female gender, higher age, low income, comorbidity, low treatment motivation, fear avoidance beliefs, and external locus of control. Future studies should examine the causal paths between the relationship variables and the outcome variables |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Álvarez-Rodríguez, J.; Leirós-Rodríguez, R.; Morera-Balaguer, J.; Marqués-Sánchez, P.; Rodríguez-Nogueira, Ó. The Influence of the Locus of Control Construct on the Efficacy of Physiotherapy Treatments in Patients with Chronic Pain: A Systematic Review. J. Pers. Med. 2022, 12, 232. https://doi.org/10.3390/jpm12020232
Álvarez-Rodríguez J, Leirós-Rodríguez R, Morera-Balaguer J, Marqués-Sánchez P, Rodríguez-Nogueira Ó. The Influence of the Locus of Control Construct on the Efficacy of Physiotherapy Treatments in Patients with Chronic Pain: A Systematic Review. Journal of Personalized Medicine. 2022; 12(2):232. https://doi.org/10.3390/jpm12020232
Chicago/Turabian StyleÁlvarez-Rodríguez, Julia, Raquel Leirós-Rodríguez, Jaume Morera-Balaguer, Pilar Marqués-Sánchez, and Óscar Rodríguez-Nogueira. 2022. "The Influence of the Locus of Control Construct on the Efficacy of Physiotherapy Treatments in Patients with Chronic Pain: A Systematic Review" Journal of Personalized Medicine 12, no. 2: 232. https://doi.org/10.3390/jpm12020232