
Personalized Dosimetry in Targeted Radiation Therapy: A Look to Methods, Tools and Critical Aspects

 ,
,  , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Radiopharmaceuticals in TRT
3. One Activity Does Not Fit All
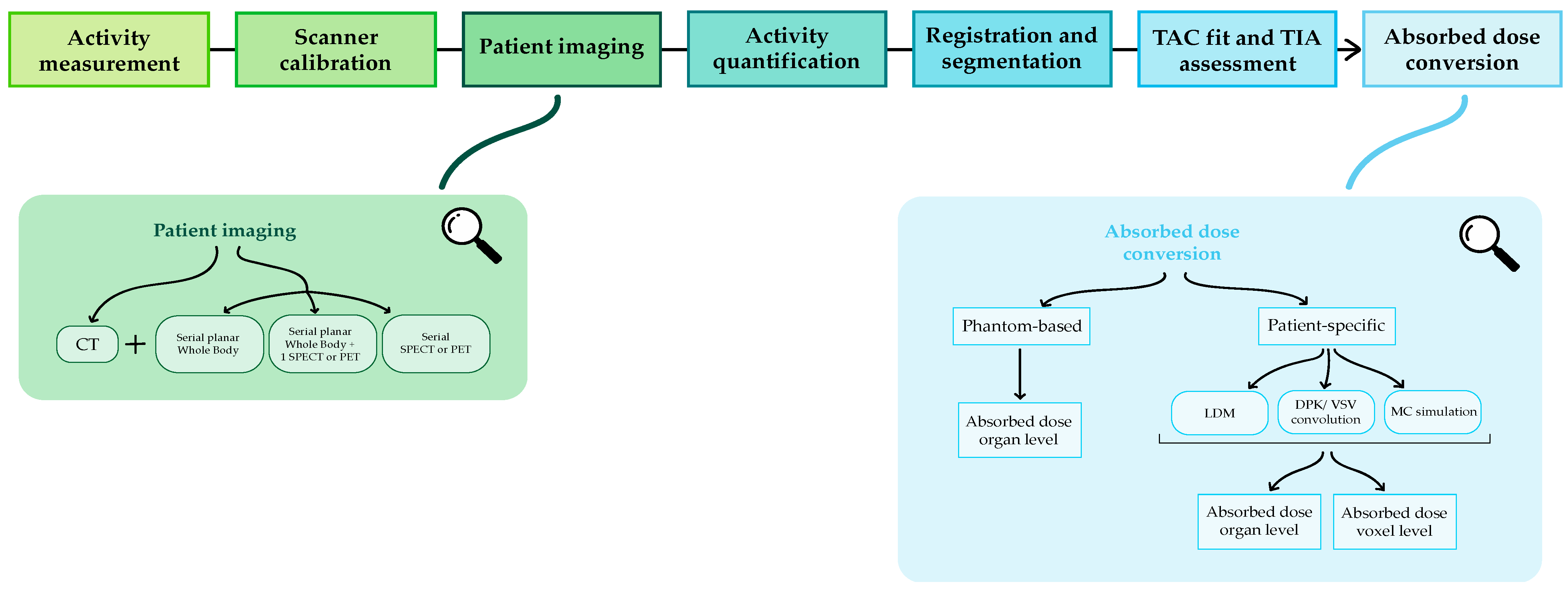
4. How to Calculate the Absorbed Dose
4.1. Activity Measurement
4.2. Scanner Calibration
4.3. Patient Image Acquisition
4.4. Activity Quantification
4.5. Registration and Segmentation
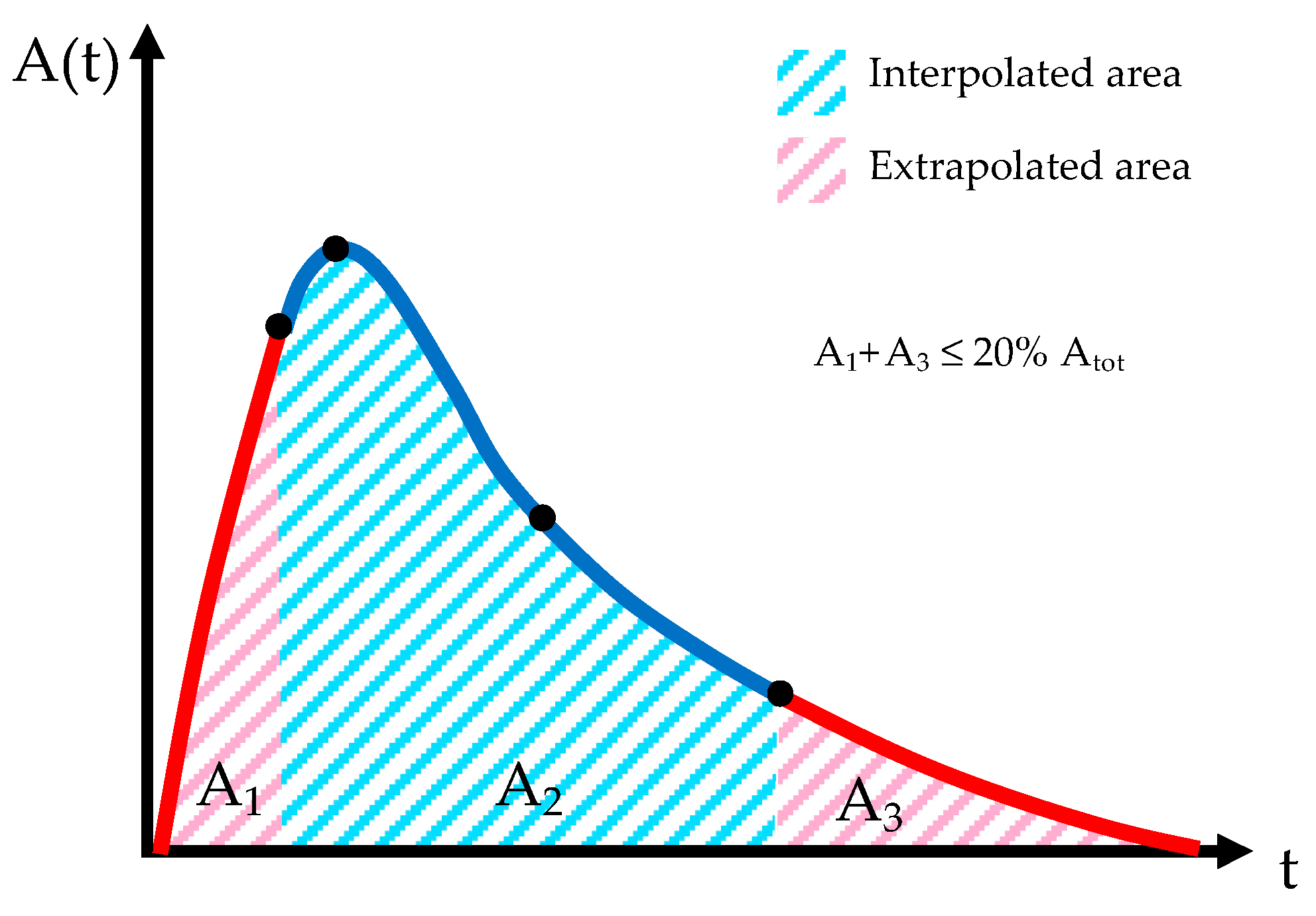
4.6. Time Activity Curve (TAC) Fit and Time Integrated Activity (TIA) Assessment
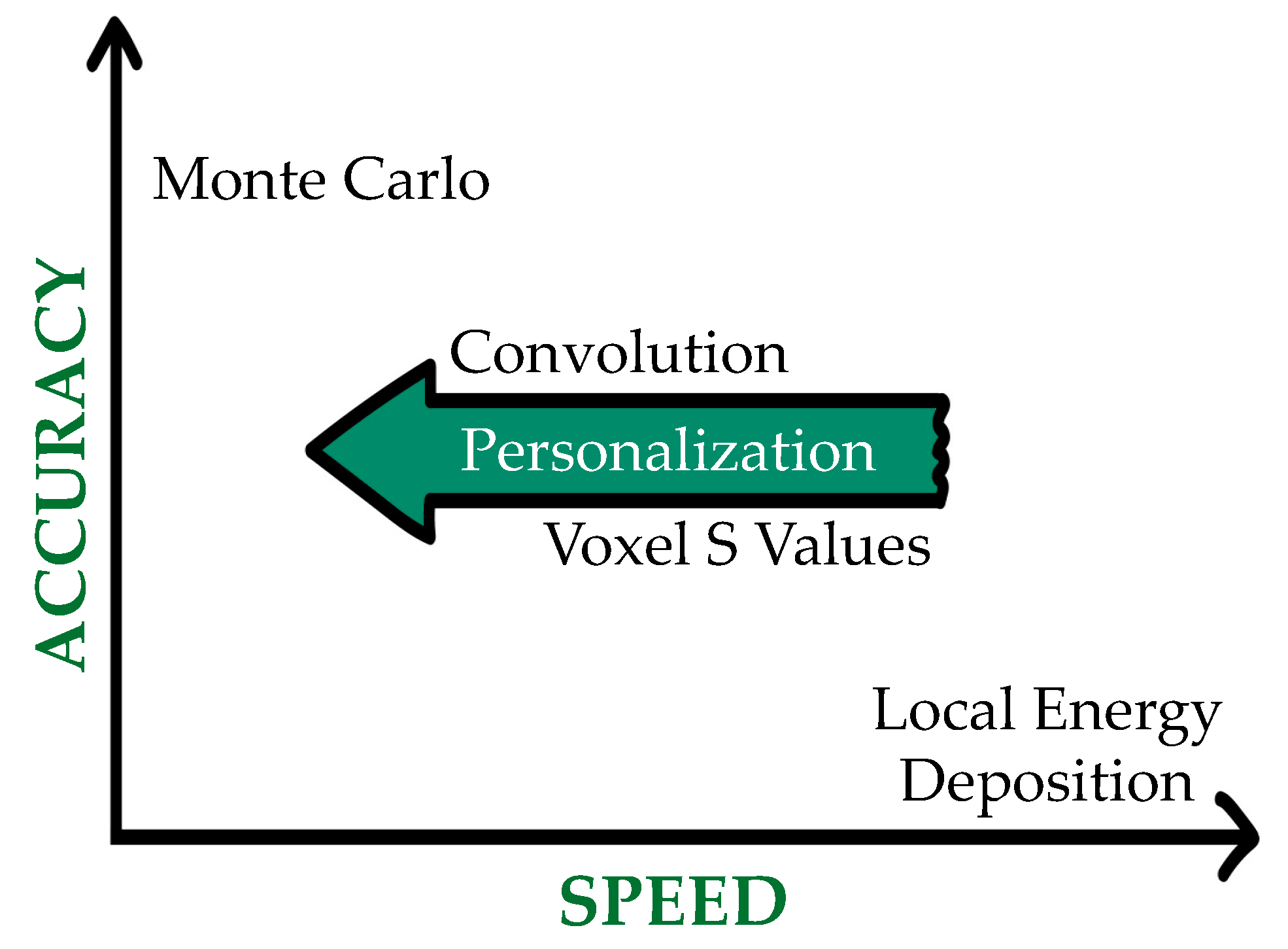
4.7. Absorbed Dose Conversion
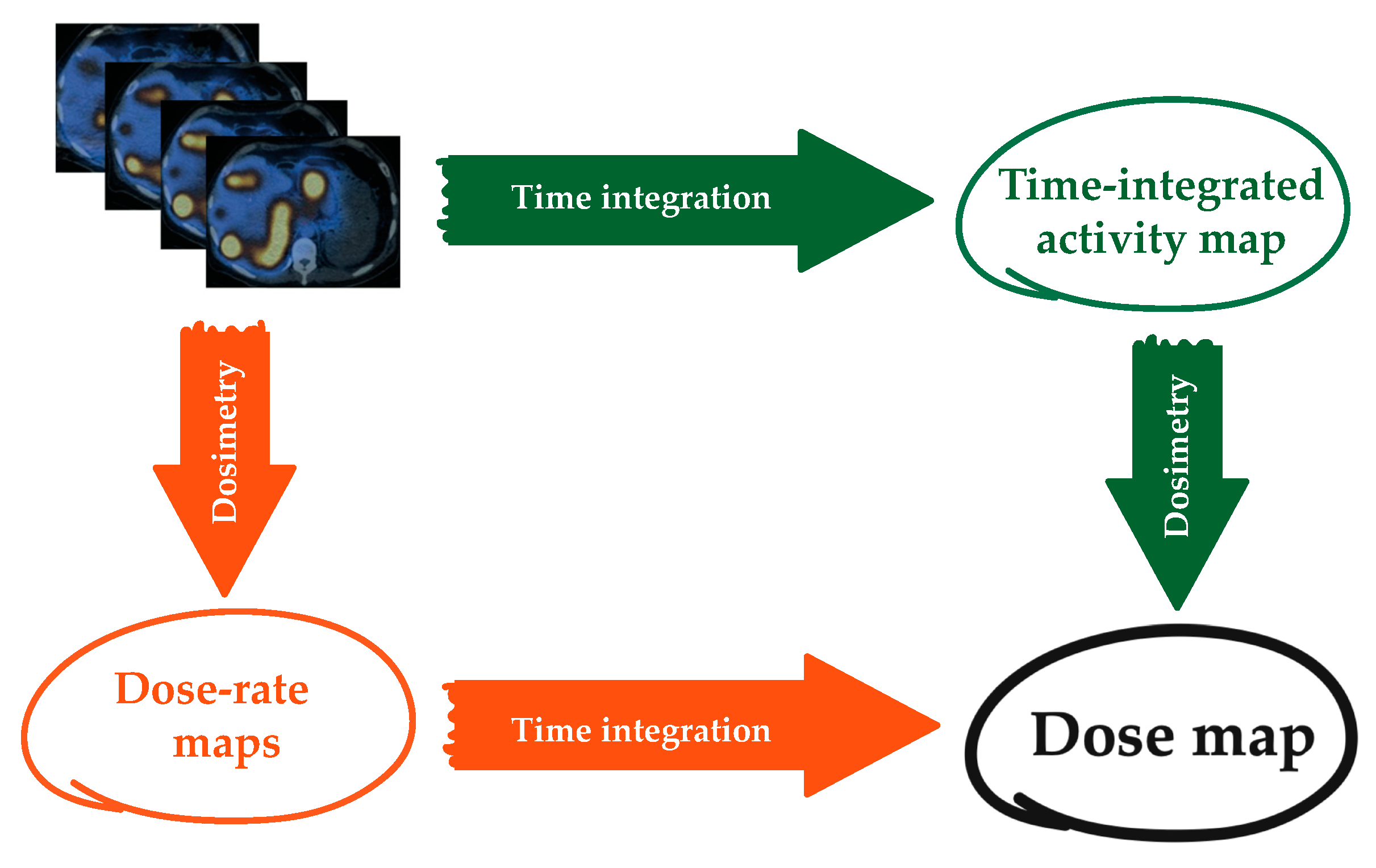
4.8. Dose-Rate Integration
4.9. Uncertainties
5. The Potential Role of Artificial Intelligence in TRT
6. Software Packages for Internal Dosimetry
6.1. Organ Level or Phantom-Based Software Packages
6.2. Voxel Level or Patient-Based Software Packages
7. Discussion
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Goldsmith, S.J. Targeted Radionuclide Therapy: A Historical and Personal Review. Semin. Nucl. Med. 2020, 50, 87–97. [Google Scholar] [CrossRef]
- Wadsley, J.; Flux, G. Molecular Radiotherapy Comes of Age. Clin. Oncol. 2021, 33, 65–67. [Google Scholar] [CrossRef]
- Alsultan, A.A.; Braat, A.; Smits, M.L.J.; Barentsz, M.W.; Bastiaannet, R.; Bruijnen, R.C.G.; de Keizer, B.; de Jong, H.; Lam, M.; Maccauro, M. Current Status and Future Direction of Hepatic Radioembolisation. Clin. Oncol. 2021, 33, 106–116. [Google Scholar] [CrossRef]
- Stokke, C.; Gabiña, P.M.; Solnỳ, P.; Cicone, F.; Sandström, M.; Gleisner, K.S.; Chiesa, C.; Spezi, E.; Paphiti, M.; Konijnenberg, M. Dosimetry-Based Treatment Planning for Molecular Radiotherapy: A Summary of the 2017 Report from the Internal Dosimetry Task Force. EJNMMI Phys. 2017, 4, 1–9. [Google Scholar] [CrossRef]
- Sgouros, G.; Kolbert, K.S.; Sheikh, A.; Pentlow, K.S.; Mun, E.F.; Barth, A.; Robbins, R.J.; Larson, S.M. Patient-Specific Dosimetry for 131I Thyroid Cancer Therapy Using 124I PET and 3-Dimensional-Internal Dosimetry (3D-ID) Software. J. Nucl. Med. 2004, 45, 1366–1372. [Google Scholar]
- Sandström, M.; Freedman, N.; Fröss-Baron, K.; Kahn, T.; Sundin, A. Kidney Dosimetry in 777 Patients during 177 Lu-DOTATATE Therapy: Aspects on Extrapolations and Measurement Time Points. EJNMMI Phys. 2020, 7, 1–15. [Google Scholar] [CrossRef]
- Strigari, L.; Konijnenberg, M.; Chiesa, C.; Bardies, M.; Du, Y.; Gleisner, K.S.; Lassmann, M.; Flux, G. The Evidence Base for the Use of Internal Dosimetry in the Clinical Practice of Molecular Radiotherapy. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 1976–1988. [Google Scholar] [CrossRef]
- Council, E.U. European Council Directive 2013/59/Euratom on Basic Safety Standards for Protection against the Dangers Arising from Exposure to Ionising Radiation and Repealing Directives 89/618/Euratom, 90/641/Euratom, 96/29/ Euratom, 97/43/Euratom and 2003/122/Euratom. Off. J. Eur. Union 2014, L13, 1–73. [Google Scholar]
- Murray, D.; McEwan, A.J. Radiobiology of Systemic Radiation Therapy. Cancer Biother. Radiopharm. 2007, 22, 1–23. [Google Scholar] [CrossRef]
- Sgouros, G.; Dewaraja, Y.K.; Escorcia, F.; Graves, S.A.; Hope, T.A.; Iravani, A.; Pandit-Taskar, N.; Saboury, B.; James, S.S.; Zanzonico, P.B. Tumor Response to Radiopharmaceutical Therapies: The Knowns and the Unknowns. J. Nucl. Med. 2021, 62, 12S–22S. [Google Scholar] [CrossRef]
- Wahl, R.L.; Sgouros, G.; Iravani, A.; Jacene, H.; Pryma, D.; Saboury, B.; Capala, J.; Graves, S.A. Normal-Tissue Tolerance to Radiopharmaceutical Therapies, the Knowns and the Unknowns. J. Nucl. Med. 2021, 62, 23S–35S. [Google Scholar] [CrossRef]
- Sgouros, G.; Bodei, L.; McDevitt, M.R.; Nedrow, J.R. Radiopharmaceutical Therapy in Cancer: Clinical Advances and Challenges. Nat. Rev. Drug Discov. 2020, 19, 589–608. [Google Scholar] [CrossRef]
- Lassmann, M.; Luster, M.; Hänscheid, H.; Reiners, C. Impact of 131I Diagnostic Activities on the Biokinetics of Thyroid Remnants. J. Nucl. Med. 2004, 45, 619–625. [Google Scholar]
- Walrand, S.; Hesse, M.; Jamar, F. Statistical and Radiobiological Analysis of the So-Called Thyroid Stunning. EJNMMI Res. 2015, 5, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Sapienza, M.T.; Willegaignon, J. Radionuclide Therapy: Current Status and Prospects for Internal Dosimetry in Individualized Therapeutic Planning. Clinics 2019, 74, e835. [Google Scholar] [CrossRef]
- Garkavij, M.; Nickel, M.; Sjögreen-Gleisner, K.; Ljungberg, M.; Ohlsson, T.; Wingårdh, K.; Strand, S.-E.; Tennvall, J. 177Lu-[DOTA0, Tyr3] Octreotate Therapy in Patients with Disseminated Neuroendocrine Tumors: Analysis of Dosimetry with Impact on Future Therapeutic Strategy. Cancer 2010, 116, 1084–1092. [Google Scholar] [CrossRef]
- Beauregard, J.-M.; Hofman, M.S.; Kong, G.; Hicks, R.J. The Tumour Sink Effect on the Biodistribution of 68 Ga-DOTA-Octreotate: Implications for Peptide Receptor Radionuclide Therapy. Eur. J. Nucl. Med. Mol. Imaging 2012, 39, 50–56. [Google Scholar] [CrossRef]
- Cremonesi, M.; Botta, F.; Di Dia, A.; Ferrari, M.; Bodei, L.; De Cicco, C.; Rossi, A.; Bartolomei, M.; Mei, R.; Severi, S. Dosimetry for Treatment with Radiolabelled Somatostatin Analogues. A Review. Q. J. Nucl. Med. Mol. Imaging 2010, 54, 37. [Google Scholar]
- Gnesin, S.; Canetti, L.; Adib, S.; Cherbuin, N.; Monteiro, M.S.; Bize, P.; Denys, A.; Prior, J.O.; Baechler, S.; Boubaker, A. Partition Model–Based 99mTc-MAA SPECT/CT Predictive Dosimetry Compared with 90Y TOF PET/CT Posttreatment Dosimetry in Radioembolization of Hepatocellular Carcinoma: A Quantitative Agreement Comparison. J. Nucl. Med. 2016, 57, 1672–1678. [Google Scholar] [CrossRef] [Green Version]
- Song, Y.S.; Paeng, J.C.; Kim, H.-C.; Chung, J.W.; Cheon, G.J.; Chung, J.-K.; Lee, D.S.; Kang, K.W. PET/CT-Based Dosimetry in 90Y-Microsphere Selective Internal Radiation Therapy: Single Cohort Comparison with Pretreatment Planning on 99mTc-MAA Imaging and Correlation with Treatment Efficacy. Medicine (Baltimore) 2015, 94, e945. [Google Scholar] [CrossRef]
- Belli, M.L.; Sarnelli, A.; Mezzenga, E.; Cesarini, F.; Caroli, P.; Di Iorio, V.; Strigari, L.; Cremonesi, M.; Romeo, A.; Nicolini, S. Targeted Alpha Therapy in MCRPC (Metastatic Castration-Resistant Prostate Cancer) Patients: Predictive Dosimetry and Toxicity Modeling of 225Ac-PSMA (Prostate-Specific Membrane Antigen). Front. Oncol. 2020, 10, 531660. [Google Scholar] [CrossRef]
- Kratochwil, C.; Bruchertseifer, F.; Rathke, H.; Bronzel, M.; Apostolidis, C.; Weichert, W.; Haberkorn, U.; Giesel, F.L.; Morgenstern, A. Targeted α-Therapy of Metastatic Castration-Resistant Prostate Cancer with (225)Ac-PSMA-617: Dosimetry Estimate and Empiric Dose Finding. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2017, 58, 1624–1631. [Google Scholar] [CrossRef] [Green Version]
- Van Nostrand, D.; Atkins, F.; Yeganeh, F.; Acio, E.; Bursaw, R.; Wartofsky, L. Dosimetrically Determined Doses of Radioiodine for the Treatment of Metastatic Thyroid Carcinoma. Thyroid Off. J. Am. Thyroid Assoc. 2002, 12, 121–134. [Google Scholar] [CrossRef]
- Giammarile, F.; Chiti, A.; Lassmann, M.; Brans, B.; Flux, G. EANM Procedure Guidelines for 131I-Meta-Iodobenzylguanidine (131I-MIBG) Therapy. Eur. J. Nucl. Med. Mol. Imaging 2008, 35, 1039–1047. [Google Scholar] [CrossRef]
- Bodei, L.; Kidd, M.; Paganelli, G.; Grana, C.M.; Drozdov, I.; Cremonesi, M.; Lepensky, C.; Kwekkeboom, D.J.; Baum, R.P.; Krenning, E.P.; et al. Long-Term Tolerability of PRRT in 807 Patients with Neuroendocrine Tumours: The Value and Limitations of Clinical Factors. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 5–19. [Google Scholar] [CrossRef]
- Giammarile, F.; Bodei, L.; Chiesa, C.; Flux, G.; Forrer, F.; Kraeber-Bodere, F.; Brans, B.; Lambert, B.; Konijnenberg, M.; Borson-Chazot, F.; et al. EANM Procedure Guideline for the Treatment of Liver Cancer and Liver Metastases with Intra-Arterial Radioactive Compounds. Eur. J. Nucl. Med. Mol. Imaging 2011, 38, 1393–1406. [Google Scholar] [CrossRef]
- Reinders, M.T.; Smits, M.L.; van Roekel, C.; Braat, A.J. Holmium-166 Microsphere Radioembolization of Hepatic Malignancies. Semin. Nucl. Med. 2019, 49, 237–243. [Google Scholar] [CrossRef]
- Tennvall, J.; Fischer, M.; Bischof Delaloye, A.; Bombardieri, E.; Bodei, L.; Giammarile, F.; Lassmann, M.; Oyen, W.; Brans, B. EANM Procedure Guideline for Radio-Immunotherapy for B-Cell Lymphoma with 90Y-Radiolabelled Ibritumomab Tiuxetan (Zevalin). Eur. J. Nucl. Med. Mol. Imaging 2007, 34, 616–622. [Google Scholar] [CrossRef]
- Dewaraja, Y.K.; Schipper, M.J.; Shen, J.; Smith, L.B.; Murgic, J.; Savas, H.; Youssef, E.; Regan, D.; Wilderman, S.J.; Roberson, P.L.; et al. Tumor-Absorbed Dose Predicts Progression-Free Survival Following (131)I-Tositumomab Radioimmunotherapy. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2014, 55, 1047–1053. [Google Scholar] [CrossRef] [Green Version]
- Kratochwil, C.; Fendler, W.P.; Eiber, M.; Baum, R.; Bozkurt, M.F.; Czernin, J.; Delgado Bolton, R.C.; Ezziddin, S.; Forrer, F.; Hicks, R.J.; et al. EANM Procedure Guidelines for Radionuclide Therapy with (177)Lu-Labelled PSMA-Ligands ((177)Lu-PSMA-RLT). Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 2536–2544. [Google Scholar] [CrossRef]
- Sathekge, M.; Bruchertseifer, F.; Knoesen, O.; Reyneke, F.; Lawal, I.; Lengana, T.; Davis, C.; Mahapane, J.; Corbett, C.; Vorster, M.; et al. (225)Ac-PSMA-617 in Chemotherapy-Naive Patients with Advanced Prostate Cancer: A Pilot Study. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 129–138. [Google Scholar] [CrossRef] [Green Version]
- Pacilio, M.; Ventroni, G.; De Vincentis, G.; Cassano, B.; Pellegrini, R.; Di Castro, E.; Frantellizzi, V.; Follacchio, G.A.; Garkavaya, T.; Lorenzon, L.; et al. Dosimetry of Bone Metastases in Targeted Radionuclide Therapy with Alpha-Emitting (223)Ra-Dichloride. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 21–33. [Google Scholar] [CrossRef]
- Stabin, M.G. Update: The Case for Patient-Specific Dosimetry in Radionuclide Therapy. Cancer Biother. Radiopharm. 2008, 23, 273–284. [Google Scholar] [CrossRef]
- de Keizer, B.; Brans, B.; Hoekstra, A.; Zelissen, P.M.; Koppeschaar, H.P.; Lips, C.J.; van Rijk, P.P.; Dierckx, R.A.; de Klerk, J.M. Tumour Dosimetry and Response in Patients with Metastatic Differentiated Thyroid Cancer Using Recombinant Human Thyrotropin before Radioiodine Therapy. Eur. J. Nucl. Med. Mol. Imaging 2003, 30, 367–373. [Google Scholar] [CrossRef]
- DuBois, S.G.; Messina, J.; Maris, J.M.; Huberty, J.; Glidden, D.V.; Veatch, J.; Charron, M.; Hawkins, R.; Matthay, K.K. Hematologic Toxicity of High-Dose Iodine-131–Metaiodobenzylguanidine Therapy for Advanced Neuroblastoma. J. Clin. Oncol. 2004, 22, 2452–2460. [Google Scholar] [CrossRef]
- Roth, D.; Gustafsson, J.R.; Warfvinge, C.F.; Sundlöv, A.; Åkesson, A.; Tennvall, J.; Gleisner, K.S. Dosimetric Quantities of Neuroendocrine Tumors over Treatment Cycles with 177Lu-DOTA-TATE. J. Nucl. Med. 2021, 121, 262069. [Google Scholar] [CrossRef]
- Gulec, S.A.; Mesoloras, G.; Dezarn, W.A.; McNeillie, P.; Kennedy, A.S. Safety and Efficacy of Y-90 Microsphere Treatment in Patients with Primary and Metastatic Liver Cancer: The Tumor Selectivity of the Treatment as a Function of Tumor to Liver Flow Ratio. J. Transl. Med. 2007, 5, 15. [Google Scholar] [CrossRef] [Green Version]
- Wiseman, G.A.; White, C.A.; Sparks, R.B.; Erwin, W.D.; Podoloff, D.A.; Lamonica, D.; Bartlett, N.L.; Parker, J.A.; Dunn, W.L.; Spies, S.M.; et al. Biodistribution and Dosimetry Results from a Phase III Prospectively Randomized Controlled Trial of Zevalin Radioimmunotherapy for Low-Grade, Follicular, or Transformed B-Cell Non-Hodgkin’s Lymphoma. Crit. Rev. Oncol. Hematol. 2001, 39, 181–194. [Google Scholar] [CrossRef]
- Baum, R.P.; Kulkarni, H.R.; Schuchardt, C.; Singh, A.; Wirtz, M.; Wiessalla, S.; Schottelius, M.; Mueller, D.; Klette, I.; Wester, H.-J. 177Lu-Labeled Prostate-Specific Membrane Antigen Radioligand Therapy of Metastatic Castration-Resistant Prostate Cancer: Safety and Efficacy. J. Nucl. Med. 2016, 57, 1006–1013. [Google Scholar] [CrossRef] [Green Version]
- Chittenden, S.J.; Hindorf, C.; Parker, C.C.; Lewington, V.J.; Pratt, B.E.; Johnson, B.; Flux, G.D. A Phase 1, Open-Label Study of the Biodistribution, Pharmacokinetics, and Dosimetry of 223Ra-Dichloride in Patients with Hormone-Refractory Prostate Cancer and Skeletal Metastases. J. Nucl. Med. 2015, 56, 1304–1309. [Google Scholar] [CrossRef] [Green Version]
- Buckley, S.E.; Chittenden, S.J.; Saran, F.H.; Meller, S.T.; Flux, G.D. Whole-Body Dosimetry for Individualized Treatment Planning of 131I-MIBG Radionuclide Therapy for Neuroblastoma. J. Nucl. Med. 2009, 50, 1518–1524. [Google Scholar] [CrossRef] [Green Version]
- Bergsma, H.; Konijnenberg, M.W.; Kam, B.L.R.; Teunissen, J.J.M.; Kooij, P.P.; de Herder, W.W.; Franssen, G.J.H.; van Eijck, C.H.J.; Krenning, E.P.; Kwekkeboom, D.J. Subacute Haematotoxicity after PRRT with (177)Lu-DOTA-Octreotate: Prognostic Factors, Incidence and Course. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 453–463. [Google Scholar] [CrossRef] [Green Version]
- Del Prete, M.; Buteau, F.-A.; Arsenault, F.; Saighi, N.; Bouchard, L.-O.; Beaulieu, A.; Beauregard, J.-M. Personalized 177Lu-Octreotate Peptide Receptor Radionuclide Therapy of Neuroendocrine Tumours: Initial Results from the P-PRRT Trial. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 728–742. [Google Scholar] [CrossRef]
- Ilan, E.; Sandström, M.; Wassberg, C.; Sundin, A.; Garske-Román, U.; Eriksson, B.; Granberg, D.; Lubberink, M. Dose Response of Pancreatic Neuroendocrine Tumors Treated with Peptide Receptor Radionuclide Therapy Using 177Lu-DOTATATE. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2015, 56, 177–182. [Google Scholar] [CrossRef] [Green Version]
- Jahn, U.; Ilan, E.; Sandström, M.; Lubberink, M.; Garske-Román, U.; Sundin, A. Peptide Receptor Radionuclide Therapy (PRRT) with 177Lu-DOTATATE; Differences in Tumor Dosimetry, Vascularity and Lesion Metrics in Pancreatic and Small Intestinal Neuroendocrine Neoplasms. Cancers 2021, 13, 962. [Google Scholar] [CrossRef]
- Garin, E.; Lenoir, L.; Rolland, Y.; Edeline, J.; Mesbah, H.; Laffont, S.; Porée, P.; Clément, B.; Raoul, J.-L.; Boucher, E. Dosimetry Based on 99mTc-Macroaggregated Albumin SPECT/CT Accurately Predicts Tumor Response and Survival in Hepatocellular Carcinoma Patients Treated with 90Y-Loaded Glass Microspheres: Preliminary Results. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2012, 53, 255–263. [Google Scholar] [CrossRef] [Green Version]
- Alsultan, A.A.; van Roekel, C.; Barentsz, M.W.; Smits, M.L.J.; Kunnen, B.; Koopman, M.; Braat, A.J.A.T.; Bruijnen, R.C.G.; de Keizer, B.; Lam, M.G.E.H. Dose-Response and Dose-Toxicity Relationships for Glass (90)Y Radioembolization in Patients with Liver Metastases from Colorectal Cancer. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2021, 62, 1616–1623. [Google Scholar] [CrossRef]
- Violet, J.; Jackson, P.; Ferdinandus, J.; Sandhu, S.; Akhurst, T.; Iravani, A.; Kong, G.; Kumar, A.R.; Thang, S.P.; Eu, P.; et al. Dosimetry of (177)Lu-PSMA-617 in Metastatic Castration-Resistant Prostate Cancer: Correlations Between Pretherapeutic Imaging and Whole-Body Tumor Dosimetry with Treatment Outcomes. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2019, 60, 517–523. [Google Scholar] [CrossRef] [Green Version]
- Pacilio, M.; Ventroni, G.; Basile, C.; Ialongo, P.; Becci, D.; Mango, L. Improving the Dose-Myelotoxicity Correlation in Radiometabolic Therapy of Bone Metastases with 153Sm-EDTMP. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 238–252. [Google Scholar] [CrossRef]
- Mínguez, P.; Rodeño, E.; Fernández, I.; Esteban, A.; Martínez-Indart, L.; Gómez de Iturriaga, A. A Retrospective Study on the Potential of (99m) Tc-HDP Imaging before Therapy for Individualizing Treatments with (223) Ra-Cl(2) for Metastatic Castration Resistant Prostate Cancer. Med. Phys. 2021, 48, 1395–1403. [Google Scholar] [CrossRef]
- Hänscheid, H.; Canzi, C.; Eschner, W.; Flux, G.; Luster, M.; Strigari, L.; Lassmann, M. EANM Dosimetry Committee Series on Standard Operational Procedures for Pre-Therapeutic Dosimetry II. Dosimetry Prior to Radioiodine Therapy of Benign Thyroid Diseases. Eur. J. Nucl. Med. Mol. Imaging 2013, 40, 1126–1134. [Google Scholar] [CrossRef] [PubMed]
- Zhao, W.; Esquinas, P.L.; Hou, X.; Uribe, C.F.; Gonzalez, M.; Beauregard, J.-M.; Dewaraja, Y.K.; Celler, A. Determination of Gamma Camera Calibration Factors for Quantitation of Therapeutic Radioisotopes. EJNMMI Phys. 2018, 5, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Bardies, M.; Buvat, I. Dosimetry in Nuclear Medicine Therapy: What Are the Specifics in Image Quantification for Dosimetry? Q. J. Nucl. Med. Mol. Imaging 2011, 55, 5. [Google Scholar] [PubMed]
- He, B.; Wahl, R.L.; Sgouros, G.; Du, Y.; Jacene, H.; Kasecamp, W.R.; Flinn, I.; Hammes, R.J.; Bianco, J.; Kahl, B. Comparison of Organ Residence Time Estimation Methods for Radioimmunotherapy Dosimetry and Treatment Planning—Patient Studies. Med. Phys. 2009, 36, 1595–1601. [Google Scholar] [CrossRef] [PubMed]
- Roth, D.; Gustafsson, J.; Sundlöv, A.; Sjögreen Gleisner, K. A Method for Tumor Dosimetry Based on Hybrid Planar-SPECT/CT Images and Semiautomatic Segmentation. Med. Phys. 2018, 45, 5004–5018. [Google Scholar] [CrossRef] [Green Version]
- Qi, J.; Leahy, R.M. Iterative Reconstruction Techniques in Emission Computed Tomography. Phys. Med. Biol. 2006, 51, R541. [Google Scholar] [CrossRef]
- Siegel, J.A.; Thomas, S.R.; Stubbs, J.B.; Stabin, M.G.; Hays, M.T.; Koral, K.F.; Robertson, J.S.; Howell, R.W.; Wessels, B.W.; Fisher, D.R.; et al. MIRD Pamphlet No. 16: Techniques for Quantitative Radiopharmaceutical Biodistribution Data Acquisition and Analysis for Use in Human Radiation Dose Estimates. J. Nucl. Med. 1999, 40, 37S–61S. [Google Scholar]
- Dewaraja, Y.K.; Frey, E.C.; Sgouros, G.; Brill, A.B.; Roberson, P.; Zanzonico, P.B.; Ljungberg, M. MIRD Pamphlet No. 23: Quantitative SPECT for Patient-Specific 3-Dimensional Dosimetry in Internal Radionuclide Therapy. J. Nucl. Med. 2012, 53, 1310–1325. [Google Scholar] [CrossRef] [Green Version]
- Buvat, I.; Frey, E.; Green, A.; Ljungberg, M. Quantitative Nuclear Medicine Imaging: Concepts, Requirements and Methods; Human Health Reports; International Atomic Energy Agency: Vienna, Austria, 2014.
- Glatting, G.; Kletting, P.; Reske, S.N.; Hohl, K.; Ring, C. Choosing the Optimal Fit Function: Comparison of the Akaike Information Criterion and the F-Test. Med. Phys. 2007, 34, 4285–4292. [Google Scholar] [CrossRef]
- Guerriero, F.; Ferrari, M.E.; Botta, F.; Fioroni, F.; Grassi, E.; Versari, A.; Sarnelli, A.; Pacilio, M.; Amato, E.; Strigari, L. Kidney Dosimetry in 177Lu and 90Y Peptide Receptor Radionuclide Therapy: Influence of Image Timing, Time-Activity Integration Method, and Risk Factors. BioMed Res. Int. 2013, 2013, 935351. [Google Scholar] [CrossRef] [Green Version]
- Hindorf, C.; Glatting, G.; Chiesa, C.; Lindén, O.; Flux, G. EANM Dosimetry Committee Guidelines for Bone Marrow and Whole-Body Dosimetry. Eur. J. Nucl. Med. Mol. Imaging 2010, 37, 1238–1250. [Google Scholar] [CrossRef] [PubMed]
- Bolch, W.E.; Eckerman, K.F.; Sgouros, G.; Thomas, S.R. MIRD Pamphlet No. 21: A Generalized Schema for Radiopharmaceutical Dosimetry—Standardization of Nomenclature. J. Nucl. Med. 2009, 50, 477–484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bolch, W.E.; Bouchet, L.G.; Robertson, J.S.; Wessels, B.W.; Siegel, J.A.; Howell, R.W.; Erdi, A.K.; Aydogan, B.; Costes, S.; Watson, E.E. MIRD Pamphlet No. 17: The Dosimetry of Nonuniform Activity Distributions—Radionuclide S Values at the Voxel Level. J. Nucl. Med. 1999, 40, 11S–36S. [Google Scholar] [PubMed]
- Ljungberg, M.; Sjögreen-Gleisner, K. The Accuracy of Absorbed Dose Estimates in Tumours Determined by Quantitative SPECT: A Monte Carlo Study. Acta Oncol. 2011, 50, 981–989. [Google Scholar] [CrossRef]
- Jan, S.; Santin, G.; Strul, D.; Staelens, S.; Assie, K.; Autret, D.; Avner, S.; Barbier, R.; Bardies, M.; Bloomfield, P.M. GATE: A Simulation Toolkit for PET and SPECT. Phys. Med. Biol. 2004, 49, 4543. [Google Scholar] [CrossRef] [PubMed]
- Kawrakow, I. The EGSnrc Code System, Monte Carlo Simulation of Electron and Photon Transport. NRCC Rep. Pirs-701 2001. [Google Scholar]
- Briesmeister, J.F. MCNP-A General Monte Carlo Code for Neutron and Photon Transport. 7396-M 1986, 10003403588. [Google Scholar]
- Forster, R.A.; Cox, L.J.; Barrett, R.F.; Booth, T.E.; Briesmeister, J.F.; Brown, F.B.; Bull, J.S.; Geisler, G.C.; Goorley, J.T.; Mosteller, R.D. MCNPTM Version 5. Nucl. Instrum. Methods Phys. Res. Sect. B Beam Interact. Mater. At. 2004, 213, 82–86. [Google Scholar] [CrossRef]
- Battistoni, G.; Cerutti, F.; Fasso, A.; Ferrari, A.; Muraro, S.; Ranft, J.; Roesler, S.; Sala, P.R. The FLUKA Code: Description and Benchmarking. In AIP Conference Proceedings; American Institute of Physics: College Park, MD, USA, 2007; Volume 896, pp. 31–49. [Google Scholar]
- Lanconelli, N.; Pacilio, M.; Meo, S.L.; Botta, F.; Di Dia, A.; Aroche, L.T.; Pérez, M.C.; Cremonesi, M. A Free Database of Radionuclide Voxel S Values for the Dosimetry of Nonuniform Activity Distributions. Phys. Med. Biol. 2012, 57, 517. [Google Scholar] [CrossRef]
- Dieudonné, A.; Hobbs, R.F.; Bolch, W.E.; Sgouros, G.; Gardin, I. Fine-Resolution Voxel S Values for Constructing Absorbed Dose Distributions at Variable Voxel Size. J. Nucl. Med. 2010, 51, 1600–1607. [Google Scholar] [CrossRef] [Green Version]
- Amato, E.; Minutoli, F.; Pacilio, M.; Campennì, A.; Baldari, S. An Analytical Method for Computing Voxel S Values for Electrons and Photons. Med. Phys. 2012, 39, 6808–6817. [Google Scholar] [CrossRef] [PubMed]
- Franquiz, J.M.; Chigurupati, S.; Kandagatla, K. Beta Voxel S Values for Internal Emitter Dosimetry. Med. Phys. 2003, 30, 1030–1032. [Google Scholar] [CrossRef] [PubMed]
- Pasciak, A.S.; Bourgeois, A.C.; Bradley, Y.C. A Comparison of Techniques for 90Y PET/CT Image-Based Dosimetry Following Radioembolization with Resin Microspheres. Front. Oncol. 2014, 4, 121. [Google Scholar] [CrossRef] [Green Version]
- Pacilio, M.; Amato, E.; Lanconelli, N.; Basile, C.; Torres, L.A.; Botta, F.; Ferrari, M.; Diaz, N.C.; Perez, M.C.; Fernández, M.; et al. Differences in 3D Dose Distributions Due to Calculation Method of Voxel S-Values and the Influence of Image Blurring in SPECT. Phys. Med. Biol. 2015, 60, 1945. [Google Scholar] [CrossRef]
- Gear, J.I.; Cox, M.G.; Gustafsson, J.; Gleisner, K.S.; Murray, I.; Glatting, G.; Konijnenberg, M.; Flux, G.D. EANM Practical Guidance on Uncertainty Analysis for Molecular Radiotherapy Absorbed Dose Calculations. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 2456–2474. [Google Scholar] [CrossRef] [Green Version]
- Finocchiaro, D.; Gear, J.I.; Fioroni, F.; Flux, G.D.; Murray, I.; Castellani, G.; Versari, A.; Iori, M.; Grassi, E. Uncertainty Analysis of Tumour Absorbed Dose Calculations in Molecular Radiotherapy. EJNMMI Phys. 2020, 7, 1–16. [Google Scholar] [CrossRef]
- Taprogge, J.; Leek, F.; Flux, G.D. Physics Aspects of Setting up a Multicenter Clinical Trial Involving Internal Dosimetry of Radioiodine Treatment of Differentiated Thyroid Cancer. Q. J. Nucl. Med. Mol. Imaging 2019, 63, 271–277. [Google Scholar] [CrossRef]
- Avanzo, M.; Trianni, A.; Botta, F.; Talamonti, C.; Stasi, M.; Iori, M. Artificial Intelligence and the Medical Physicist: Welcome to the Machine. Appl. Sci. 2021, 11, 1691. [Google Scholar] [CrossRef]
- Arabi, H.; AkhavanAllaf, A.; Sanaat, A.; Shiri, I.; Zaidi, H. The Promise of Artificial Intelligence and Deep Learning in PET and SPECT Imaging. Phys. Med. 2021, 83, 122–137. [Google Scholar] [CrossRef]
- Brosch-Lenz, J.; Yousefirizi, F.; Zukotynski, K.; Beauregard, J.-M.; Gaudet, V.; Saboury, B.; Rahmim, A.; Uribe, C. Role of Artificial Intelligence in Theranostics: Toward Routine Personalized Radiopharmaceutical Therapies. PET Clin. 2021, 16, 627–641. [Google Scholar] [CrossRef]
- Tang, X.; Rangraz, E.J.; Coudyzer, W.; Bertels, J.; Robben, D.; Schramm, G.; Deckers, W.; Maleux, G.; Baete, K.; Verslype, C. Whole Liver Segmentation Based on Deep Learning and Manual Adjustment for Clinical Use in SIRT. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 2742–2752. [Google Scholar] [CrossRef]
- Jackson, P.; Hardcastle, N.; Dawe, N.; Kron, T.; Hofman, M.S.; Hicks, R.J. Deep Learning Renal Segmentation for Fully Automated Radiation Dose Estimation in Unsealed Source Therapy. Front. Oncol. 2018, 8, 215. [Google Scholar] [CrossRef] [Green Version]
- Klyuzhin, I.; Chausse, G.; Bloise, I.; Ferres, J.L.; Uribe, C.; Rahmim, A. Automated Deep Segmentation of Healthy Organs in PSMA PET/CT Images. J. Nucl. Med. 2021, 62 (Suppl. 1), 1410. [Google Scholar]
- Akhavanallaf, A.; Shiri, I.; Arabi, H.; Zaidi, H. Whole-Body Voxel-Based Internal Dosimetry Using Deep Learning. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 670–682. [Google Scholar] [CrossRef] [PubMed]
- Götz, T.I.; Lang, E.W.; Schmidkonz, C.; Kuwert, T.; Ludwig, B. Dose Voxel Kernel Prediction with Neural Networks for Radiation Dose Estimation. Z. Für Med. Phys. 2021, 31, 23–36. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.S.; Hwang, D.; Kim, J.H.; Lee, J.S. Deep-Dose: A Voxel Dose Estimation Method Using Deep Convolutional Neural Network for Personalized Internal Dosimetry. Sci. Rep. 2019, 9, 10308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Götz, T.I.; Schmidkonz, C.; Chen, S.; Al-Baddai, S.; Kuwert, T.; Lang, E.W. A Deep Learning Approach to Radiation Dose Estimation. Phys. Med. Biol. 2020, 65, 035007. [Google Scholar] [CrossRef]
- Xue, S.; Gafita, A.; Afshar-Oromieh, A.; Eiber, M.; Rominger, A.; Shi, K. Voxel-Wise Prediction of Post-Therapy Dosimetry for 177 Lu-PSMA I&T Therapy Using Deep Learning. J. Nucl. Med. 2020, 61, 1424. [Google Scholar]
- Stabin, M.G.; Xu, X.G.; Emmons, M.A.; Segars, W.P.; Shi, C.; Fernald, M.J. RADAR Reference Adult, Pediatric, and Pregnant Female Phantom Series for Internal and External Dosimetry. J. Nucl. Med. 2012, 53, 1807–1813. [Google Scholar] [CrossRef] [Green Version]
- Menzel, H.-G.; Clement, C.; DeLuca, P. ICRP Publication 110. Realistic Reference Phantoms: An ICRP/ICRU Joint Effort. A Report of Adult Reference Computational Phantoms. Ann. ICRP 2009, 39, 1–164. [Google Scholar] [CrossRef] [Green Version]
- Bolch, W.E.; Eckerman, K.; Endo, A.; Hunt, J.G.S.; Jokisch, D.W.; Kim, C.H.; Kim, K.-P.; Lee, C.; Li, J.; Petoussi-Henss, N.; et al. ICRP Publication 143: Paediatric Reference Computational Phantoms. Ann. ICRP 2020, 49, 5–297. [Google Scholar] [CrossRef] [PubMed]
- Eckerman, K.; Endo, A. ICRP Publication 107. Nuclear Decay Data for Dosimetric Calculations. Ann. ICRP 2008, 38, 7–96. [Google Scholar] [CrossRef]
- RADAR—The Decay Data. Available online: https://www.doseinfo-radar.com/RADARDecay.html (accessed on 5 December 2021).
- Valentin, J. Basic Anatomical and Physiological Data for Use in Radiological Protection: Reference Values. A Report of Age- and Gender-Related Differences in the Anatomical and Physiological Characteristics of Reference Individuals. ICRP Publication 89. Ann. ICRP 2002, 32, 5–265. [Google Scholar]
- Cremonesi, M.; Ferrari, M.; Grana, C.M.; Vanazzi, A.; Stabin, M.; Bartolomei, M.; Papi, S.; Prisco, G.; Ferrucci, P.F.; Martinelli, G.; et al. High-Dose Radioimmunotherapy with 90Y-Ibritumomab Tiuxetan: Comparative Dosimetric Study for Tailored Treatment. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2007, 48, 1871–1879. [Google Scholar] [CrossRef] [PubMed]
- Kesner, A.; Olguin, E.; Zanzonico, P.; Bolch, W. MIRDCalc V 1.0—A Community Spreadsheet Tool for Organ-Level Radiopharmaceutical Absorbed Dose Calculations. J. Nucl. Med. 2018, 59, 473. [Google Scholar]
- Carter, L.; Ramos, J.O.; Zanzonico, P.; Bolch, W.; Kesner, A. Comparative Evaluation of the New MIRDcalc Dosimetry Software across a Compendium of Radiopharmaceuticals. J. Nucl. Med. 2021, 62, 1581. [Google Scholar]
- Cristy, M.; Eckerman, K.F. Specific Absorbed Fractions of Energy at Various Ages from Internal Photon Sources; Oak Ridge National Lab: Oak Ridge, TN, USA, 1987.
- Stabin, M.G.; Watson, E.E.; Cristy, M.; Ryman, J.C.; Eckerman, K.F.; Davis, J.L.; Marshall, D.; Gehlen, M.K. Mathematical Models and Specific Absorbed Fractions of Photon Energy in the Nonpregnant Adult Female and at the End of Each Trimester of Pregnancy; Oak Ridge National Lab: Oak Ridge, TN, USA, 1995.
- Stabin, M.G.; Sparks, R.B.; Crowe, E. OLINDA/EXM: The Second-Generation Personal Computer Software for Internal Dose Assessment in Nuclear Medicine. J. Nucl. Med. 2005, 46, 1023–1027. [Google Scholar]
- Stabin, M.; Farmer, A. OLINDA/EXM 2.0: The New Generation Dosimetry Modeling Code. J. Nucl. Med. 2012, 53, 585. [Google Scholar]
- Chauvin, M.; Borys, D.; Botta, F.; Bzowski, P.; Dabin, J.; Denis-Bacelar, A.M.; Desbrée, A.; Falzone, N.; Lee, B.Q.; Mairani, A. OpenDose: Open-Access Resource for Nuclear Medicine Dosimetry. J. Nucl. Med. 2020, 61, 1514–1519. [Google Scholar] [CrossRef] [Green Version]
- OpenDose. Open Access Resources for Radiopharmaceutical Dosimetry. Available online: https://www.opendose.org (accessed on 5 December 2021).
- Finocchiaro, D.; Berenato, S.; Bertolini, V.; Castellani, G.; Lanconelli, N.; Versari, A.; Spezi, E.; Iori, M.; Fioroni, F.; Grassi, E. Comparison of Different Calculation Techniques for Absorbed Dose Assessment in Patient Specific Peptide Receptor Radionuclide Therapy. PLoS ONE 2020, 15, e0236466. [Google Scholar] [CrossRef]
- Mora-Ramirez, E.; Santoro, L.; Cassol, E.; Ocampo-Ramos, J.C.; Clayton, N.; Kayal, G.; Chouaf, S.; Trauchessec, D.; Pouget, J.-P.; Kotzki, P.-O. Comparison of Commercial Dosimetric Software Platforms in Patients Treated with 177Lu-DOTATATE for Peptide Receptor Radionuclide Therapy. Med. Phys. 2020, 47, 4602–4615. [Google Scholar] [CrossRef] [PubMed]
- Santoro, L.; Pitalot, L.; Trauchessec, D.; Mora-Ramirez, E.; Kotzki, P.-O.; Bardiès, M.; Deshayes, E. Clinical Implementation of PLANET® Dose for Dosimetric Assessment after [177 Lu] Lu-DOTA-TATE: Comparison with Dosimetry Toolkit® and OLINDA/EXM® V1.0. EJNMMI Res. 2021, 11, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Gleisner, K.S.; Spezi, E.; Solny, P.; Gabina, P.M.; Cicone, F.; Stokke, C.; Chiesa, C.; Paphiti, M.; Brans, B.; Sandström, M. Variations in the Practice of Molecular Radiotherapy and Implementation of Dosimetry: Results from a European Survey. EJNMMI Phys. 2017, 4, 1–20. [Google Scholar]
- Mínguez, P.; Gustafsson, J.; Flux, G.; Gleisner, K.S. Biologically Effective Dose in Fractionated Molecular Radiotherapy—Application to Treatment of Neuroblastoma with (131)I-MIBG. Phys. Med. Biol. 2016, 61, 2532–2551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levillain, H.; Bagni, O.; Deroose, C.M.; Dieudonné, A.; Gnesin, S.; Grosser, O.S.; Kappadath, S.C.; Kennedy, A.; Kokabi, N.; Liu, D.M.; et al. International Recommendations for Personalised Selective Internal Radiation Therapy of Primary and Metastatic Liver Diseases with Yttrium-90 Resin Microspheres. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 1570–1584. [Google Scholar] [CrossRef]
- Ljungberg, M.; Celler, A.; Konijnenberg, M.W.; Eckerman, K.F.; Dewaraja, Y.K.; Sjögreen-Gleisner, K.; Bolch, W.E.; Brill, A.B.; Fahey, F.; Fisher, D.R.; et al. MIRD Pamphlet No. 26: Joint EANM/MIRD Guidelines for Quantitative 177Lu SPECT Applied for Dosimetry of Radiopharmaceutical Therapy. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2016, 57, 151–162. [Google Scholar] [CrossRef] [Green Version]
- Call for Nominations: EFOMP Special Interest Group in Radionuclide Dosimetry. Available online: https://www.efomp.org/index.php?r=news/view&id=209%20EFOMP%20Special%20Interest%20Group%20in%20Radionuclide%20Dosimetry (accessed on 5 December 2021).
- Lassmann, M.; Chiesa, C.; Flux, G.; Bardiès, M. EANM Dosimetry Committee Guidance Document: Good Practice of Clinical Dosimetry Reporting. Eur. J. Nucl. Med. Mol. Imaging 2011, 38, 192–200. [Google Scholar] [CrossRef]
- Sarnelli, A.; Guerriero, F.; Botta, F.; Ferrari, M.; Strigari, L.; Bodei, L.; D’Errico, V.; Grassi, E.; Fioroni, F.; Paganelli, G.; et al. Therapeutic Schemes in 177Lu and 90Y-PRRT: Radiobiological Considerations. Q. J. Nucl. Med. Mol. Imaging 2017, 61, 216–231. [Google Scholar] [CrossRef]
- Garske-Román, U.; Sandström, M.; Fröss Baron, K.; Lundin, L.; Hellman, P.; Welin, S.; Johansson, S.; Khan, T.; Lundqvist, H.; Eriksson, B.; et al. Prospective Observational Study of (177)Lu-DOTA-Octreotate Therapy in 200 Patients with Advanced Metastasized Neuroendocrine Tumours (NETs): Feasibility and Impact of a Dosimetry-Guided Study Protocol on Outcome and Toxicity. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 970–988. [Google Scholar] [CrossRef] [Green Version]
- Garin, E.; Tzelikas, L.; Guiu, B.; Chalaye, J.; Edeline, J.; De Baere, T.; Tacher, V.; Robert, C.; Assenat, E.; Terroir-Cassou-Mounat, M.; et al. Major Impact of Personalized Dosimetry Using 90Y Loaded Glass Microspheres SIRT in HCC: Final Overall Survival Analysis of a Multicenter Randomized Phase II Study (DOSISPHERE-01). J. Clin. Oncol. 2020, 38, 516. [Google Scholar] [CrossRef]
- Lassmann, M.; Eberlein, U. The Relevance of Dosimetry in Precision Medicine. J. Nucl. Med. 2018, 59, 1494–1499. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Therapeutic Application | RP for Therapy | Activity Typically Administered | RP for Dosimetry |
|---|---|---|---|
| Thyroid cancer | 131I | 1.1 to 5.5 GBq (thyroid remnant ablation) 5.5–11 GBq (treatment of metastases) single administration [23] | 123I, 124I, 131I |
| Neuroblastoma | (131I)mIBG | 3.7–11.2 GBq per cycle; multiple cycles [24] | (131I)mIBG |
| PRRT for NET and other somatostatin receptor expressing tumors | 90Y-DOTATOC * | 2.8–3.7 GBq per cycle; 4 cycles [25] | 111In-DOTATOC |
| 177Lu-DOTATATE | 7.4 GBq per cycle; 4 cycles [6] | 177Lu-DOTATATE | |
| Radioembolization of primary and secondary liver tumors | 90Y resin or glass microspheres | 2–4 GBq (resin) 3–20 GBq (glass) single administration [26] | 99mTc-MAA, 90Y microspheres |
| 166Ho poly-L-lactic acid microspheres | 3.8 GBq/kg (liver weight) single administration [27] | 166Ho microspheres | |
| Radioimmunotherapy for hematologic malignancies (leukemia, MDS, myeloma, lymphoma) | 90Y-MoAbs (Zevalin®) | 11–14 MBq/kg (body weight) single administration [28] | 111In-MoAbs |
| 131I-MoAbs (Bexxar®) | 2.2–5.7 GBq single administration [29] | 131I-MoAbs | |
| Prostate cancer | 177Lu-PSMA | 3.7–9.3 GBq; 2 to six cycles [30] | 177Lu-PSMA |
| 225Ac-PSMA * | 4–13.4 MBq per cycle; 2–6 cycles [31] | imaging not possible, extrapolation from 177Lu-PSMA data | |
| Bone metastases from breast and prostate cancers | 223Ra | 55 kBq/kg (body weight) per cycle; 6 cycles [32] | 223Ra |
| Therapy | No. of Patients | Administered Activity | Absorbed Dose Range | Reference |
|---|---|---|---|---|
| 131I for thyroid cancer | 16 | 7.4 GBq | Tumor: 1–368 Gy | [34] |
| (131I)mIBG | 53 | 666 MBq/kg | Red marrow: 2–5 Gy | [35] |
| 177Lu-DOTATATE | 777 | 7.4 GBq | Kidneys: 1–10 Gy | [6] |
| 177Lu-DOTATATE | 41 | 7.4 GBq | Tumor: 2–77 Gy | [36] |
| 90Y resin or glass microspheres | 40 | 0.4–2.4 GBq (according to empiric or BSA method) | Tumor: 40–495 Gy Healthy Liver: 1–100 Gy | [37] |
| 90Y-MoAbs (Zevalin®) | 72 | 15 MBq/kg up to a maximum of 1.2 GBq | Red marrow: 0.1–2.0 mGy/MBq | [38] |
| 177Lu-PSMA | 30 | 3.6–8.7 GBq per cycle | Parotid glands: 0.3–10 mGy/MBq Lesions: 0.03–78 mGy/MBq | [39] |
| 223Ra (Xofigo®) | 6 | 100 kBq/kg per cycle | Red Marrow: 177–994 mGy/MBq (from bone surface) 1–5 mGy/MBq (from blood) | [40] |
| Therapy | No. of Patients | Clinical Endpoint | Correlation Found | Reference |
|---|---|---|---|---|
| (131I)mIBG | 26 | Hematological toxiticy (Neutropenia) | Whole-body absorbed dose | [41] |
| 177Lu-DOTATATE | 14 | Hematological toxicity (PLT 1 and WBC 2 variation) | Cumulative bone marrow absorbed dose | [42] |
| 177Lu-DOTATATE | 52 | Hematological toxicity (PLT variation) | Per-cycle bone marrow absorbed dose | [43] |
| 177Lu-DOTATATE | 24 | Tumor response (RECIST 3 criteria) | Tumor absorbed dose | [44] |
| 177Lu-DOTATATE | 48 | Tumor response (CT) | Tumor absorbed dose | [45] |
| 90Y microspheres | 36 | Tumor response (EASL 4 criteria) PFS OS | Tumor absorbed dose | [46] |
| 90Y microspheres | 24 | Tumor response (18F-FDG PET/CT) | Tumor absorbed dose | [47] |
| 177Lu-PSMA (mCRPC) | 30 | Tumor response (PSA, 68Ga-PET/CT) | “Whole-body” tumor absorbed dose | [48] |
| 153Sm-EDTMP (bone metastases) | 27 | Hematological toxicity (CTCAE 5, PLT and WBC variation) | Bone marrow absorbed dose rescaled in terms of patient-specific trabecular volume | [49] |
| 223Ra-Cl2 (mCRPC) | 14 | Tumor response (99mTc-HDP) | Tumor absorbed dose in the first cycle | [50] |
| Name | Availability | Decay Data | Number of Radionuclides | Phantoms | Specific Organ Models |
|---|---|---|---|---|---|
| OLINDA /EXM 1 | Distributed by Vanderbilt University, presently withdrawn from the market | RADAR website [95] | Over 800 | Cristy and Eckerman [100] + pregnant female series [101] | Peritoneal cavity, prostate gland, head and brain, kidney and spheres |
| Organ DosimetryTM with Olinda/EXM® 2.0 | Distributed by Hermes Medical | RADAR website [95] | Over 1000 | RADAR phantoms [91] + animal phantoms | Peritoneal cavity, prostate gland, head and brain, kidney and spheres |
| IDAC 2.1 | Free | ICRP 107 [94] | 1252 | ICRP 110 [92] | Spheres |
| 3D-RD-S | Distributed by Rapid, LLC | ICRP 107 [94] | 1252 | ICRP 110 [92] and ICRP 143 [93] | Spheres |
| MIRDcalc | Free | ICRP 107 [94] | 333 | ICRP 110 [92], ICRP 143 [93] and weight-based phantoms | Spheres |
| Name | Manufacturer | Dose Conversion Method | Supported Therapy Radionuclides | CE/FDA Approval |
|---|---|---|---|---|
| SurePlan™ MRT | MIM Software Inc. | VSV | 177Lu, 131I 1 | CE/FDA |
| Planet® Dose | DOSIsoft | VSV/LDM | 177Lu, 131I | CE/FDA |
| Voxel DosimetryTM | Hermes Medical solutions | Semi-MC | 68Ga, 123I, 131I, 111In, 177Lu, 99mTc, 90Y, 89Zr, 223Ra, 166Ho | CE/FDA |
| QDOSE® | ABX-CRO | VSV | 11C, 15O, 18F, 44Sc, 64Cu, 68Ga, 86Y, 89Zr, 90Y, 124I, 89Sr, 99mTc, 111In, 131I, 153Sm, 166Ho, 177Lu, 186Re, 188Re | CE |
| SurePlan™ LiverY90 | MIM Software Inc. | VSV/LDM | 90Y microspheres 1 | CE/FDA |
| Planet® Dose | DOSIsoft | VSV/LDM | 90Y microspheres | CE/FDA |
| Hybrid3DTM SIRT | Hermes Medical solutions | LDM | 90Y microspheres | CE/FDA |
| Simplicit90YTM v2.4 | Mirada Medical | LDM | 90Y microspheres | CE/FDA |
| VelocityTM Varian RapidSphere v4.1 | Varian | DPK/LDM | 90Y microspheres | CE/FDA |
| Q-Suite v2.0 | QUIREM Medical BV | LDM | 166Ho microspheres | CE |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Danieli, R.; Milano, A.; Gallo, S.; Veronese, I.; Lascialfari, A.; Indovina, L.; Botta, F.; Ferrari, M.; Cicchetti, A.; Raspanti, D.; et al. Personalized Dosimetry in Targeted Radiation Therapy: A Look to Methods, Tools and Critical Aspects. J. Pers. Med. 2022, 12, 205. https://doi.org/10.3390/jpm12020205
Danieli R, Milano A, Gallo S, Veronese I, Lascialfari A, Indovina L, Botta F, Ferrari M, Cicchetti A, Raspanti D, et al. Personalized Dosimetry in Targeted Radiation Therapy: A Look to Methods, Tools and Critical Aspects. Journal of Personalized Medicine. 2022; 12(2):205. https://doi.org/10.3390/jpm12020205
Chicago/Turabian StyleDanieli, Rachele, Alessia Milano, Salvatore Gallo, Ivan Veronese, Alessandro Lascialfari, Luca Indovina, Francesca Botta, Mahila Ferrari, Alessandro Cicchetti, Davide Raspanti, and et al. 2022. "Personalized Dosimetry in Targeted Radiation Therapy: A Look to Methods, Tools and Critical Aspects" Journal of Personalized Medicine 12, no. 2: 205. https://doi.org/10.3390/jpm12020205