
Personalized Management of Myocarditis and Inflammatory Cardiomyopathy in Clinical Practice

 , , ,
, , ,
Abstract
:1. Background
2. Definitions
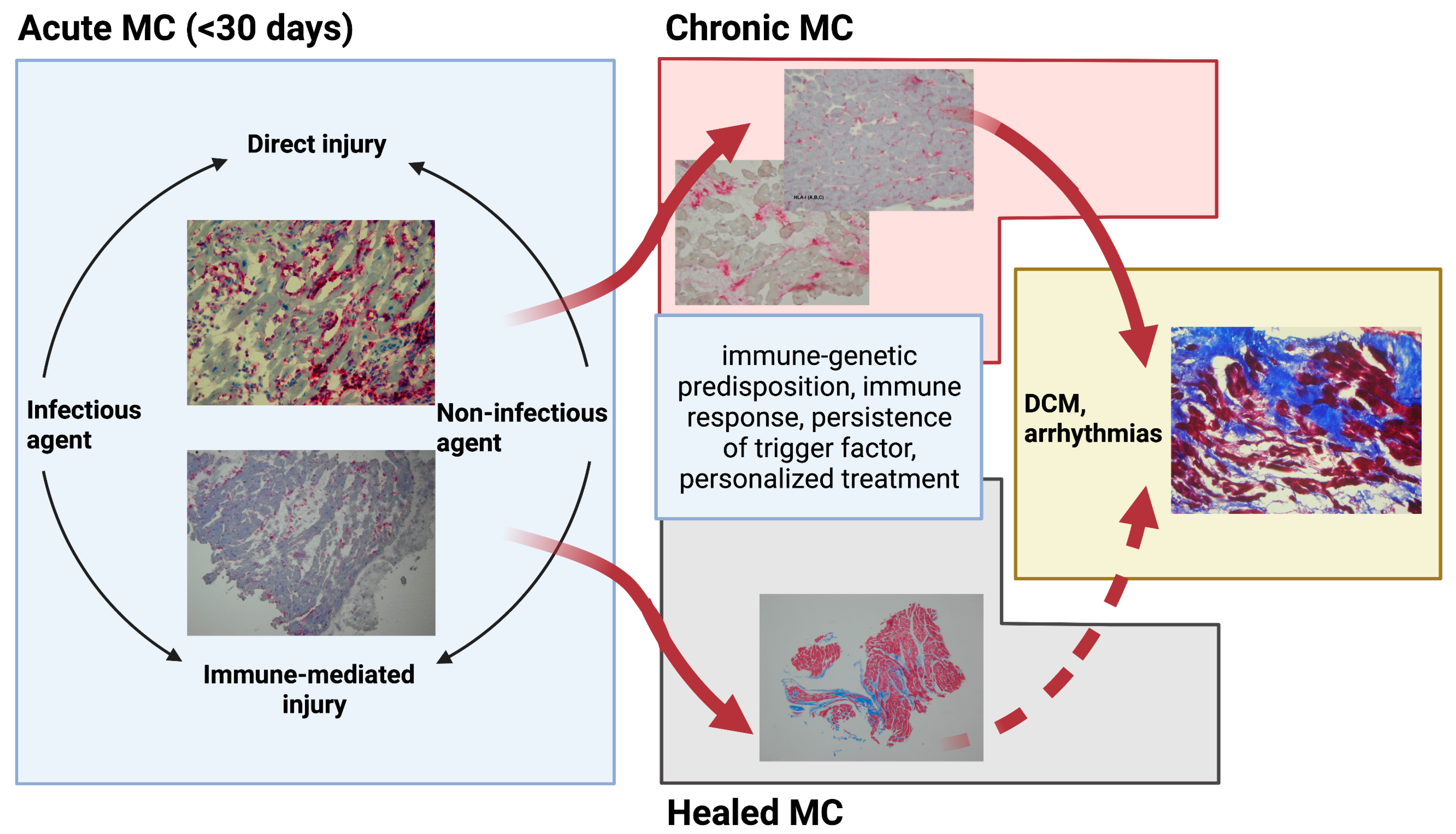
3. Emerging Etiologies and Pathophysiology of Myocarditis
4. Clinical Presentation and Complications in Patients with Myocarditis
5. Description of Diagnostic Methods
5.1. Biomarkers
5.2. Serum Anti-Heart Autoantibodies
5.3. Micro-RNA
5.4. Imaging
5.4.1. Echocardiography
5.4.2. Cardiac Magnetic Resonance
5.4.3. Nuclear Medicine
5.5. Endomyocardial Biopsy: Diagnostic Gold Standard
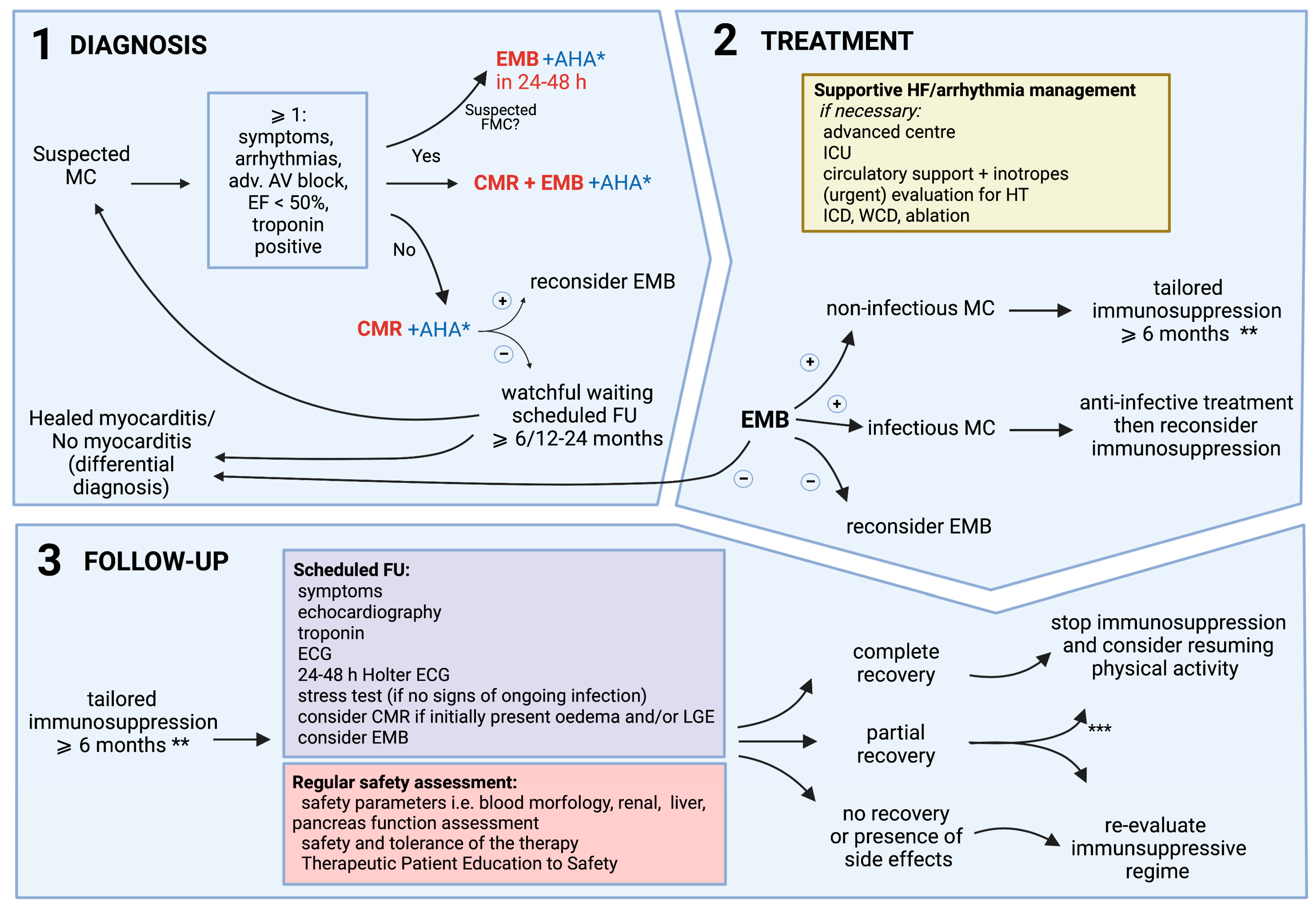
6. Diagnosis and Decision-Making Process
7. Personalized Treatment, Follow-Up, and Return to Activity
7.1. Personalized Treatment
7.2. Tailored Therapy and Follow-Up
7.3. Physical Activity
Author Contributions
Funding
Conflicts of Interest
References
- Ozierański, K.; Tymińska, A.; Kruk, M.; Koń, B.; Skwarek, A.; Opolski, G.; Grabowski, M. Occurrence, Trends, Management and Outcomes of Patients Hospitalized with Clinically Suspected Myocarditis-Ten-Year Perspectives from the MYO-PL Nationwide Database. J. Clin. Med. 2021, 10, 4672. [Google Scholar] [CrossRef] [PubMed]
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update from the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef] [PubMed]
- Caforio, A.L.; Pankuweit, S.; Arbustini, E.; Basso, C.; Gimeno-Blanes, J.; Felix, S.B.; Fu, M.; Heliö, T.; Heymans, S.; Jahns, R.; et al. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: A position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur. Heart J. 2013, 34, 2636–2648, 48a–48d. [Google Scholar] [CrossRef] [PubMed]
- Ozieranski, K.; Tyminska, A.; Jonik, S.; Marcolongo, R.; Baritussio, A.; Grabowski, M.; Filipiak, K.J.; Opolski, G.; Caforio, A.L.P. Clinically Suspected Myocarditis in the Course of Severe Acute Respiratory Syndrome Novel Coronavirus-2 Infection: Fact or Fiction? J. Card. Fail. 2021, 27, 92–96. [Google Scholar] [CrossRef] [PubMed]
- Tymińska, A.; Ozierański, K.; Caforio, A.L.P.; Marcolongo, R.; Marchel, M.; Kapłon-Cieślicka, A.; Baritussio, A.; Filipiak, K.J.; Opolski, G.; Grabowski, M. Myocarditis and inflammatory cardiomyopathy in 2021: An update. Pol. Arch. Intern. Med. 2021, 131, 594–606. [Google Scholar] [CrossRef]
- Kawai, C. From myocarditis to cardiomyopathy: Mechanisms of inflammation and cell death: Learning from the past for the future. Circulation 1999, 99, 1091–1100. [Google Scholar] [CrossRef] [Green Version]
- Maisch, B. Cardio-Immunology of Myocarditis: Focus on Immune Mechanisms and Treatment Options. Front. Cardiovasc. Med. 2019, 6, 48. [Google Scholar] [CrossRef] [Green Version]
- Tschöpe, C.; Ammirati, E.; Bozkurt, B.; Caforio, A.L.P.; Cooper, L.T.; Felix, S.B.; Hare, J.M.; Heidecker, B.; Heymans, S.; Hübner, N.; et al. Myocarditis and inflammatory cardiomyopathy: Current evidence and future directions. Nat. Rev. Cardiol. 2021, 18, 169–193. [Google Scholar] [CrossRef]
- Frustaci, A.; Russo, M.A.; Chimenti, C. Randomized study on the efficacy of immunosuppressive therapy in patients with virus-negative inflammatory cardiomyopathy: The TIMIC study. Eur. Heart J. 2009, 30, 1995–2002. [Google Scholar] [CrossRef]
- Kühl, U.; Lassner, D.; von Schlippenbach, J.; Poller, W.; Schultheiss, H.P. Interferon-Beta improves survival in enterovirus-associated cardiomyopathy. J. Am. Coll. Cardiol. 2012, 60, 1295–1296. [Google Scholar] [CrossRef] [Green Version]
- He, Y.; Chipman, P.R.; Howitt, J.; Bator, C.M.; Whitt, M.A.; Baker, T.S.; Kuhn, R.J.; Anderson, C.W.; Freimuth, P.; Rossmann, M.G. Interaction of coxsackievirus B3 with the full length coxsackievirus-adenovirus receptor. Nat. Struct. Biol. 2001, 8, 874–878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Badorff, C.; Lee, G.H.; Lamphear, B.J.; Martone, M.E.; Campbell, K.P.; Rhoads, R.E.; Knowlton, K.U. Enteroviral protease 2A cleaves dystrophin: Evidence of cytoskeletal disruption in an acquired cardiomyopathy. Nat. Med. 1999, 5, 320–326. [Google Scholar] [CrossRef] [PubMed]
- Dominguez, F.; Kühl, U.; Pieske, B.; Garcia-Pavia, P.; Tschöpe, C. Update on Myocarditis and Inflammatory Cardiomyopathy: Reemergence of Endomyocardial Biopsy. Rev. Esp. Cardiol. (Engl. Ed.) 2016, 69, 178–187. [Google Scholar] [CrossRef] [PubMed]
- Caforio, A.L.P. Myocarditis: Endomyocardial biopsy and circulating anti-heart autoantibodies are key to diagnosis and personalized etiology-directed treatment. Eur. Heart J. 2021, 42, 1618–1620. [Google Scholar] [CrossRef]
- Caforio, A.L.P.; Adler, Y.; Agostini, C.; Allanore, Y.; Anastasakis, A.; Arad, M.; Böhm, M.; Charron, P.; Elliott, P.M.; Eriksson, U.; et al. Diagnosis and management of myocardial in.nvolvement in systemic immune-mediated diseases: A position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Disease. Eur. Heart J. 2017, 38, 2649–2662. [Google Scholar] [CrossRef] [Green Version]
- Kociol, R.D.; Cooper, L.T.; Fang, J.C.; Moslehi, J.J.; Pang, P.S.; Sabe, M.A.; Shah, R.V.; Sims, D.B.; Thiene, G.; Vardeny, O. Recognition and Initial Management of Fulminant Myocarditis: A Scientific Statement From the American Heart Association. Circulation 2020, 141, e69–e92. [Google Scholar] [CrossRef]
- Palaskas, N.; Lopez-Mattei, J.; Durand, J.B.; Iliescu, C.; Deswal, A. Immune Checkpoint Inhibitor Myocarditis: Pathophysiological Characteristics, Diagnosis, and Treatment. J. Am. Heart Assoc 2020, 9, e013757. [Google Scholar] [CrossRef]
- Mahmood, S.S.; Fradley, M.G.; Cohen, J.V.; Nohria, A.; Reynolds, K.L.; Heinzerling, L.M.; Sullivan, R.J.; Damrongwatanasuk, R.; Chen, C.L.; Gupta, D.; et al. Myocarditis in Patients Treated with Immune Checkpoint Inhibitors. J. Am. Coll. Cardiol. 2018, 71, 1755–1764. [Google Scholar] [CrossRef]
- Hu, J.R.; Florido, R.; Lipson, E.J.; Naidoo, J.; Ardehali, R.; Tocchetti, C.G.; Lyon, A.R.; Padera, R.F.; Johnson, D.B.; Moslehi, J. Cardiovascular toxicities associated with immune checkpoint inhibitors. Cardiovasc. Res. 2019, 115, 854–868. [Google Scholar] [CrossRef] [Green Version]
- Caforio, A.L.P. Receipt of mRNA Vaccine against Covid-19 and Myocarditis. N. Engl. J. Med. 2021, 385, 2189–2190. [Google Scholar] [CrossRef]
- Mevorach, D.; Anis, E.; Cedar, N.; Bromberg, M.; Haas, E.J.; Nadir, E.; Olsha-Castell, S.; Arad, D.; Hasin, T.; Levi, N.; et al. Myocarditis after BNT162b2 mRNA Vaccine against Covid-19 in Israel. N. Engl. J. Med. 2021, 385, 2140–2149. [Google Scholar] [CrossRef] [PubMed]
- Witberg, G.; Barda, N.; Hoss, S.; Richter, I.; Wiessman, M.; Aviv, Y.; Grinberg, T.; Auster, O.; Dagan, N.; Balicer, R.D.; et al. Myocarditis after Covid-19 Vaccination in a Large Health Care Organization. N. Engl. J. Med. 2021, 385, 2132–2139. [Google Scholar] [CrossRef] [PubMed]
- Husby, A.; Hansen, J.V.; Fosbøl, E.; Thiesson, E.M.; Madsen, M.; Thomsen, R.W.; Sørensen, H.T.; Andersen, M.; Wohlfahrt, J.; Gislason, G.; et al. SARS-CoV-2 vaccination and myocarditis or myopericarditis: Population based cohort study. BMJ 2021, 375, e068665. [Google Scholar] [CrossRef] [PubMed]
- Ozierański, K.; Tymińska, A.; Skwarek, A.; Kruk, M.; Koń, B.; Biliński, J.; Opolski, G.; Grabowski, M. Sex Differences in Incidence, Clinical Characteristics and Outcomes in Children and Young Adults Hospitalized for Clinically Suspected Myocarditis in the Last Ten Years-Data from the MYO-PL Nationwide Database. J. Clin. Med. 2021, 10, 5502. [Google Scholar] [CrossRef]
- Ammirati, E.; Cipriani, M.; Moro, C.; Raineri, C.; Pini, D.; Sormani, P.; Mantovani, R.; Varrenti, M.; Pedrotti, P.; Conca, C.; et al. Clinical Presentation and Outcome in a Contemporary Cohort of Patients with Acute Myocarditis: Multicenter Lombardy Registry. Circulation 2018, 138, 1088–1099. [Google Scholar] [CrossRef]
- Caforio, A.L.; Calabrese, F.; Angelini, A.; Tona, F.; Vinci, A.; Bottaro, S.; Ramondo, A.; Carturan, E.; Iliceto, S.; Thiene, G.; et al. A prospective study of biopsy-proven myocarditis: Prognostic relevance of clinical and aetiopathogenetic features at diagnosis. Eur. Heart J. 2007, 28, 1326–1333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tschöpe, C.; Cooper, L.T.; Torre-Amione, G.; Van Linthout, S. Management of Myocarditis-Related Cardiomyopathy in Adults. Circ. Res. 2019, 124, 1568–1583. [Google Scholar] [CrossRef]
- Schultheiss, H.P.; Kühl, U.; Cooper, L.T. The management of myocarditis. Eur. Heart J. 2011, 32, 2616–2625. [Google Scholar] [CrossRef] [Green Version]
- Lassner, D.; Rohde, M.; Siegismund, C.S.; Kühl, U.; Gross, U.M.; Escher, F.; Tschöpe, C.; Schultheiss, H.-P. Myocarditis—personalized medicine by expanded endomyocardial biopsy diagnostics. World J. Cardiovasc. Dis. 2014, 2014, 46494. [Google Scholar] [CrossRef] [Green Version]
- Aquaro, G.D.; Perfetti, M.; Camastra, G.; Monti, L.; Dellegrottaglie, S.; Moro, C.; Pepe, A.; Todiere, G.; Lanzillo, C.; Scatteia, A.; et al. Cardiac MR With Late Gadolinium Enhancement in Acute Myocarditis with Preserved Systolic Function: ITAMY Study. J. Am. Coll. Cardiol. 2017, 70, 1977–1987. [Google Scholar] [CrossRef]
- Kasner, M.; Aleksandrov, A.; Escher, F.; Al-Saadi, N.; Makowski, M.; Spillmann, F.; Genger, M.; Schultheiss, H.P.; Kühl, U.; Pieske, B.; et al. Multimodality imaging approach in the diagnosis of chronic myocarditis with preserved left ventricular ejection fraction (MCpEF): The role of 2D speckle-tracking echocardiography. Int. J. Cardiol. 2017, 243, 374–378. [Google Scholar] [CrossRef] [PubMed]
- Mair, J.; Lindahl, B.; Hammarsten, O.; Müller, C.; Giannitsis, E.; Huber, K.; Möckel, M.; Plebani, M.; Thygesen, K.; Jaffe, A.S. How is cardiac troponin released from injured myocardium? Eur. Heart J. Acute Cardiovasc. Care 2018, 7, 553–560. [Google Scholar] [CrossRef] [PubMed]
- Mewton, N.; Dernis, A.; Bresson, D.; Zouaghi, O.; Croisille, P.; Flocard, E.; Douek, P.; Bonnefoy-Cudraz, E. Myocardial biomarkers and delayed enhanced cardiac magnetic resonance relationship in clinically suspected myocarditis and insight on clinical outcome. J. Cardiovasc Med. 2015, 16, 696–703. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Coronado, M.J.; Bruno, K.A.; Blauwet, L.A.; Tschöpe, C.; Cunningham, M.W.; Pankuweit, S.; van Linthout, S.; Jeon, E.S.; McNamara, D.M.; Krejčí, J.; et al. Elevated Sera sST2 Is Associated with Heart Failure in Men ≤ 50 Years Old with Myocarditis. J. Am. Heart Assoc. 2019, 8, e008968. [Google Scholar] [CrossRef] [Green Version]
- Tymińska, A.; Kapłon-Cieślicka, A.; Ozierański, K.; Budnik, M.; Wancerz, A.; Sypień, P.; Peller, M.; Maksym, J.; Balsam, P.; Opolski, G.; et al. Association of galectin-3 and soluble ST2 with in-hospital and 1-year outcomes in patients with ST-segment elevation myocardial infarction treated with primary percutaneous coronary intervention. Pol. Arch. Intern. Med. 2019, 129, 770–780. [Google Scholar] [CrossRef] [Green Version]
- Caforio, A.L.; Angelini, A.; Blank, M.; Shani, A.; Kivity, S.; Goddard, G.; Doria, A.; Schiavo, A.; Testolina, M.; Bottaro, S.; et al. Passive transfer of affinity-purified anti-heart autoantibodies (AHA) from sera of patients with myocarditis induces experimental myocarditis in mice. Int. J. Cardiol. 2015, 179, 166–177. [Google Scholar] [CrossRef]
- Caforio, A.L.; Mahon, N.G.; Baig, M.K.; Tona, F.; Murphy, R.T.; Elliott, P.M.; McKenna, W.J. Prospective familial assessment in dilated cardiomyopathy: Cardiac autoantibodies predict disease development in asymptomatic relatives. Circulation 2007, 115, 76–83. [Google Scholar] [CrossRef] [Green Version]
- Caforio, A.L.; Grazzini, M.; Mann, J.M.; Keeling, P.J.; Bottazzo, G.F.; McKenna, W.J.; Schiaffino, S. Identification of alpha- and beta-cardiac myosin heavy chain isoforms as major autoantigens in dilated cardiomyopathy. Circulation 1992, 85, 1734–1742. [Google Scholar] [CrossRef] [Green Version]
- Caforio, A.L.P.; Baritussio, A.; Marcolongo, R.; Cheng, C.Y.; Pontara, E.; Bison, E.; Cattini, M.G.; Gallo, N.; Plebani, M.; Iliceto, S.; et al. Serum Anti-Heart and Anti-Intercalated Disk Autoantibodies: Novel Autoimmune Markers in Cardiac Sarcoidosis. J. Clin. Med. 2021, 10, 2476. [Google Scholar] [CrossRef]
- Caforio, A.L.P.; De Luca, G.; Baritussio, A.; Seguso, M.; Gallo, N.; Bison, E.; Cattini, M.G.; Pontara, E.; Gargani, L.; Pepe, A.; et al. Serum Organ-Specific Anti-Heart and Anti-Intercalated Disk Autoantibodies as New Autoimmune Markers of Cardiac Involvement in Systemic Sclerosis: Frequency, Clinical and Prognostic Correlates. Diagnostics 2021, 11, 2165. [Google Scholar] [CrossRef]
- Lauer, B.; Schannwell, M.; Kühl, U.; Strauer, B.E.; Schultheiss, H.P. Antimyosin autoantibodies are associated with deterioration of systolic and diastolic left ventricular function in patients with chronic myocarditis. J. Am. Coll. Cardiol. 2000, 35, 11–18. [Google Scholar] [CrossRef] [Green Version]
- Caforio, A.L.P.; Re, F.; Avella, A.; Marcolongo, R.; Baratta, P.; Seguso, M.; Gallo, N.; Plebani, M.; Izquierdo-Bajo, A.; Cheng, C.Y.; et al. Evidence From Family Studies for Autoimmunity in Arrhythmogenic Right Ventricular Cardiomyopathy: Associations of Circulating Anti-Heart and Anti-Intercalated Disk Autoantibodies with Disease Severity and Family History. Circulation 2020, 141, 1238–1248. [Google Scholar] [CrossRef] [PubMed]
- Aleshcheva, G.; Pietsch, H.; Escher, F.; Schultheiss, H.P. MicroRNA profiling as a novel diagnostic tool for identification of patients with inflammatory and/or virally induced cardiomyopathies. ESC Heart Fail. 2021, 8, 408–422. [Google Scholar] [CrossRef]
- Xu, H.F.; Ding, Y.J.; Shen, Y.W.; Xue, A.M.; Xu, H.M.; Luo, C.L.; Li, B.X.; Liu, Y.L.; Zhao, Z.Q. MicroRNA- 1 represses Cx43 expression in viral myocarditis. Mol. Cell Biochem. 2012, 362, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Besler, C.; Urban, D.; Watzka, S.; Lang, D.; Rommel, K.P.; Kandolf, R.; Klingel, K.; Thiele, H.; Linke, A.; Schuler, G.; et al. Endomyocardial miR-133a levels correlate with myocardial inflammation, improved left ventricular function, and clinical outcome in patients with inflammatory cardiomyopathy. Eur. J. Heart Fail. 2016, 18, 1442–1451. [Google Scholar] [CrossRef] [Green Version]
- Iftikhar, H.; Carney, G.E. Evidence and potential in vivo functions for biofluid miRNAs: From expression profiling to functional testing: Potential roles of extracellular miRNAs as indicators of physiological change and as agents of intercellular information exchange. Bioessays 2016, 38, 367–378. [Google Scholar] [CrossRef]
- Small, E.M.; Olson, E.N. Pervasive roles of microRNAs in cardiovascular biology. Nature 2011, 469, 336–342. [Google Scholar] [CrossRef] [Green Version]
- Blanco-Domínguez, R.; Sánchez-Díaz, R.; de la Fuente, H.; Jiménez-Borreguero, L.J.; Matesanz-Marín, A.; Relaño, M.; Jiménez-Alejandre, R.; Linillos-Pradillo, B.; Tsilingiri, K.; Martín-Mariscal, M.L.; et al. A Novel Circulating MicroRNA for the Detection of Acute Myocarditis. N. Engl. J. Med. 2021, 384, 2014–2027. [Google Scholar] [CrossRef]
- Wang, J.; Han, B. Dysregulated CD4+ T Cells and microRNAs in Myocarditis. Front. Immunol. 2020, 11, 539. [Google Scholar] [CrossRef]
- Ferreira, V.M.; Schulz-Menger, J.; Holmvang, G.; Kramer, C.M.; Carbone, I.; Sechtem, U.; Kindermann, I.; Gutberlet, M.; Cooper, L.T.; Liu, P.; et al. Cardiovascular Magnetic Resonance in Nonischemic Myocardial Inflammation: Expert Recommendations. J. Am. Coll. Cardiol. 2018, 72, 3158–3176. [Google Scholar] [CrossRef] [PubMed]
- Felker, G.M.; Boehmer, J.P.; Hruban, R.H.; Hutchins, G.M.; Kasper, E.K.; Baughman, K.L.; Hare, J.M. Echocardiographic findings in fulminant and acute myocarditis. J. Am. Coll. Cardiol. 2000, 36, 227–232. [Google Scholar] [CrossRef] [Green Version]
- Hsiao, J.F.; Koshino, Y.; Bonnichsen, C.R.; Yu, Y.; Miller, F.A., Jr.; Pellikka, P.A.; Cooper, L.T., Jr.; Villarraga, H.R. Speckle tracking echocardiography in acute myocarditis. Int. J. Cardiovasc. Imaging 2013, 29, 275–284. [Google Scholar] [CrossRef]
- Kasner, M.; Sinning, D.; Escher, F.; Lassner, D.; Kühl, U.; Schultheiss, H.P.; Tschöpe, C. The utility of speckle tracking imaging in the diagnostic of acute myocarditis, as proven by endomyocardial biopsy. Int. J. Cardiol. 2013, 168, 3023–3024. [Google Scholar] [CrossRef]
- Erley, J.; Genovese, D.; Tapaskar, N.; Alvi, N.; Rashedi, N.; Besser, S.A.; Kawaji, K.; Goyal, N.; Kelle, S.; Lang, R.M.; et al. Echocardiography and cardiovascular magnetic resonance based evaluation of myocardial strain and relationship with late gadolinium enhancement. J. Cardiovasc. Magn Reson. 2019, 21, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plana, J.C.; Galderisi, M.; Barac, A.; Ewer, M.S.; Ky, B.; Scherrer-Crosbie, M.; Ganame, J.; Sebag, I.A.; Agler, D.A.; Badano, L.P.; et al. Expert consensus for multimodality imaging evaluation of adult patients during and after cancer therapy: A report from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr 2014, 27, 911–939. [Google Scholar] [CrossRef] [Green Version]
- Murtagh, G.; Laffin, L.J.; Patel, K.V.; Patel, A.V.; Bonham, C.A.; Yu, Z.; Addetia, K.; El-Hangouche, N.; Maffesanti, F.; Mor-Avi, V.; et al. Improved detection of myocardial damage in sarcoidosis using longitudinal strain in patients with preserved left ventricular ejection fraction. Echocardiography 2016, 33, 1344–1352. [Google Scholar] [CrossRef] [Green Version]
- Escher, F.; Kasner, M.; Kühl, U.; Heymer, J.; Wilkenshoff, U.; Tschöpe, C.; Schultheiss, H.P. New echocardiographic findings correlate with intramyocardial inflammation in endomyocardial biopsies of patients with acute myocarditis and inflammatory cardiomyopathy. Mediat. Inflamm. 2013, 2013, 875420. [Google Scholar] [CrossRef] [Green Version]
- Medvedofsky, D.; Maffessanti, F.; Weinert, L.; Tehrani, D.M.; Narang, A.; Addetia, K.; Mediratta, A.; Besser, S.A.; Maor, E.; Patel, A.R.; et al. 2D and 3D Echocardiography-Derived Indices of Left Ventricular Function and Shape: Relationship with Mortality. JACC Cardiovasc. Imaging 2018, 11, 1569–1579. [Google Scholar] [CrossRef]
- Friedrich, M.G.; Sechtem, U.; Schulz-Menger, J.; Holmvang, G.; Alakija, P.; Cooper, L.T.; White, J.A.; Abdel-Aty, H.; Gutberlet, M.; Prasad, S.; et al. Cardiovascular magnetic resonance in myocarditis: A JACC White Paper. J. Am. Coll. Cardiol. 2009, 53, 1475–1487. [Google Scholar] [CrossRef] [Green Version]
- Vermes, E.; Childs, H.; Faris, P.; Friedrich, M.G. Predictive value of CMR criteria for LV functional improvement in patients with acute myocarditis. Eur. Heart J. Cardiovasc. Imaging 2014, 15, 1140–1144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thavendiranathan, P.; Walls, M.; Giri, S.; Verhaert, D.; Rajagopalan, S.; Moore, S.; Simonetti, O.P.; Raman, S.V. Improved detection of myocardial involvement in acute inflammatory cardiomyopathies using T2 mapping. Circ. Cardiovasc. Imaging 2012, 5, 102–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lagan, J.; Schmitt, M.; Miller, C.A. Clinical applications of multi-parametric CMR in myocarditis and systemic inflammatory diseases. Int. J. Cardiovasc. Imaging 2018, 34, 35–54. [Google Scholar] [CrossRef] [PubMed]
- Amsallem, M.; Saito, T.; Tada, Y.; Dash, R.; McConnell, M.V. Magnetic Resonance Imaging and Positron Emission Tomography Approaches to Imaging Vascular and Cardiac Inflammation. Circ. J. 2016, 80, 1269–1277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ozierański, K.; Tymińska, A.; Kobylecka, M.; Caforio, A.L.P.; Šobić-Šaranović, D.; Ristić, A.D.; Maksimović, R.; Seferović, P.M.; Marcolongo, R.; Królicki, L.; et al. Positron emission tomography in clinically suspected myocarditis—STREAM study design. Int. J. Cardiol. 2021, 332, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Dec, G.W.; Palacios, I.; Yasuda, T.; Fallon, J.T.; Khaw, B.A.; Strauss, H.W.; Haber, E. Antimyosin antibody cardiac imaging: Its role in the diagnosis of myocarditis. J. Am. Coll. Cardiol. 1990, 16, 97–104. [Google Scholar] [CrossRef] [Green Version]
- Chareonthaitawee, P.; Beanlands, R.S.; Chen, W.; Dorbala, S.; Miller, E.J.; Murthy, V.L.; Birnie, D.H.; Chen, E.S.; Cooper, L.T.; Tung, R.H.; et al. Joint SNMMI-ASNC expert consensus document on the role of (18)F-FDG PET/CT in cardiac sarcoid detection and therapy monitoring. J. Nucl. Cardiol. 2017, 24, 1741–1758. [Google Scholar] [CrossRef] [Green Version]
- Ozawa, K.; Funabashi, N.; Daimon, M.; Takaoka, H.; Takano, H.; Uehara, M.; Kobayashi, Y. Determination of optimum periods between onset of suspected acute myocarditis and ¹⁸F-fluorodeoxyglucose positron emission tomography in the diagnosis of inflammatory left ventricular myocardium. Int. J. Cardiol. 2013, 169, 196–200. [Google Scholar] [CrossRef]
- Nensa, F.; Kloth, J.; Tezgah, E.; Poeppel, T.D.; Heusch, P.; Goebel, J.; Nassenstein, K.; Schlosser, T. Feasibility of FDG-PET in myocarditis: Comparison to CMR using integrated PET/MRI. J. Nucl Cardiol. 2018, 25, 785–794. [Google Scholar] [CrossRef]
- Niederkohr, R.D.; Daniels, C.; Raman, S.V. Concordant findings on myocardial perfusion SPECT and cardiac magnetic resonance imaging in a patient with myocarditis. J. Nucl. Cardiol. 2008, 15, 466–468. [Google Scholar] [CrossRef]
- Tymińska, A.; Ozierański, K.; Caforio, A.L.P.; Kobylecka, M.; Matsibora, V.; Kowalik, R.; Grabowski, M.; Opolski, G. Emerging nuclear medicine modalities to improve diagnostic accuracy in myocarditis. Kardiol. Pol. 2020, 78, 1297–1298. [Google Scholar] [CrossRef] [PubMed]
- Francone, M.; Chimenti, C.; Galea, N.; Scopelliti, F.; Verardo, R.; Galea, R.; Carbone, I.; Catalano, C.; Fedele, F.; Frustaci, A. CMR sensitivity varies with clinical presentation and extent of cell necrosis in biopsy-proven acute myocarditis. JACC Cardiovasc. Imaging 2014, 7, 254–263. [Google Scholar] [CrossRef] [PubMed]
- Peix, A.; Mesquita, C.T.; Paez, D.; Pereira, C.C.; Felix, R.; Gutierrez, C.; Jaimovich, R.; Ianni, B.M.; Soares, J., Jr.; Olaya, P.; et al. Nuclear medicine in the management of patients with heart failure: Guidance from an expert panel of the International Atomic Energy Agency (IAEA). Nucl. Med. Commun. 2014, 35, 818–823. [Google Scholar] [CrossRef] [Green Version]
- Caforio, A.L.P.; Malipiero, G.; Marcolongo, R.; Iliceto, S. Myocarditis: A Clinical Overview. Curr. Cardiol. Rep. 2017, 19, 63. [Google Scholar] [CrossRef] [PubMed]
- Chimenti, C.; Frustaci, A. Contribution and risks of left ventricular endomyocardial biopsy in patients with cardiomyopathies: A retrospective study over a 28-year period. Circulation 2013, 128, 1531–1541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seferović, P.M.; Tsutsui, H.; McNamara, D.M.; Ristić, A.D.; Basso, C.; Bozkurt, B.; Cooper, L.T., Jr.; Filippatos, G.; Ide, T.; Inomata, T.; et al. Heart Failure Association of the ESC, Heart Failure Society of America and Japanese Heart Failure Society Position statement on endomyocardial biopsy. Eur. J. Heart Fail. 2021, 23, 854–871. [Google Scholar] [CrossRef]
- Kawakatsu, N.; Suzuki, A.; Serizawa, N.; Suzuki, T.; Ejima, K.; Shiga, T.; Fukushima, K.; Momose, M.; Uto, K.; Shoda, M.; et al. Isolated cardiac sarcoidosis diagnosed by electroanatomic voltage mapping-guided endomyocardial biopsy combined with magnetic resonance imaging and positron emission tomography. J. Cardiol. Cases 2016, 14, 107–110. [Google Scholar] [CrossRef] [Green Version]
- Borchert, B.; Lawrenz, T.; Bartelsmeier, M.; Röthemeyer, S.; Kuhn, H.; Stellbrink, C. Utility of endomyocardial biopsy guided by delayed enhancement areas on magnetic resonance imaging in the diagnosis of cardiac sarcoidosis. Clin. Res. Cardiol. 2007, 96, 759–762. [Google Scholar] [CrossRef]
- Mahrholdt, H.; Goedecke, C.; Wagner, A.; Meinhardt, G.; Athanasiadis, A.; Vogelsberg, H.; Fritz, P.; Klingel, K.; Kandolf, R.; Sechtem, U. Cardiovascular magnetic resonance assessment of human myocarditis: A comparison to histology and molecular pathology. Circulation 2004, 109, 1250–1258. [Google Scholar] [CrossRef] [Green Version]
- Vaidya, V.R.; Abudan, A.A.; Vasudevan, K.; Shantha, G.; Cooper, L.T.; Kapa, S.; Noseworthy, P.A.; Cha, Y.M.; Asirvatham, S.J.; Deshmukh, A.J. The efficacy and safety of electroanatomic mapping-guided endomyocardial biopsy: A systematic review. J. Interv. Card Electrophysiol. 2018, 53, 63–71. [Google Scholar] [CrossRef]
- Holzmann, M.; Nicko, A.; Kühl, U.; Noutsias, M.; Poller, W.; Hoffmann, W.; Morguet, A.; Witzenbichler, B.; Tschöpe, C.; Schultheiss, H.P.; et al. Complication rate of right ventricular endomyocardial biopsy via the femoral approach: A retrospective and prospective study analyzing 3048 diagnostic procedures over an 11-year period. Circulation 2008, 118, 1722–1728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wojnicz, R.; Nowalany-Kozielska, E.; Wojciechowska, C.; Glanowska, G.; Wilczewski, P.; Niklewski, T.; Zembala, M.; Polonski, L.; Rozek, M.M.; Wodniecki, J. Randomized, placebo-controlled study for immunosuppressive treatment of inflammatory dilated cardiomyopathy: Two-year follow-up results. Circulation 2001, 104, 39–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, C.Y.; Cheng, G.Y.; Shan, Z.G.; Baritussio, A.; Lorenzoni, G.; Tyminska, A.; Ozieranski, K.; Iliceto, S.; Marcolongo, R.; Gregori, D.; et al. Efficacy of immunosuppressive therapy in myocarditis: A 30-year systematic review and meta analysis. Autoimmun Rev. 2021, 20, 102710. [Google Scholar] [CrossRef] [PubMed]
- Ozierański, K.; Tymińska, A.; Marchel, M.; Januszkiewicz, Ł.; Maciejewski, C.; Główczyńska, R.; Marcolongo, R.; Caforio, A.L.; Wojnicz, R.; Mizia-Stec, K.; et al. A multicenter, randomized, double-blind, placebo-controlled study to evaluate the efficacy of immunosuppression in biopsy-proven virus-negative myocarditis or inflammatory cardiomyopathy (IMPROVE-MC). Cardiol. J. 2021. [Google Scholar] [CrossRef] [PubMed]
- Rose, N.R.; Bona, C. Defining criteria for autoimmune diseases (Witebsky’s postulates revisited). Immunol. Today 1993, 14, 426–430. [Google Scholar] [CrossRef]
- Marcolongo, R.; Baritussio, A.; Gianstefani, S.; Cheng, C.-Y.; Iliceto, S.; Caforio, A.L. Clinical management and follow-up of myocarditis patients on immunosuppressive therapy. In Myocarditis: Pathogenesis, Diagnosis and Treatment; Springer: Cham, Switzerland, 2020; pp. 285–296. [Google Scholar]
- Baritussio, A.; Giordani, A.S.; Rizzo, S.; Masiero, G.; Iliceto, S.; Marcolongo, R.; Caforio, A.L. Management of myocarditis in clinical practice. Minerva Cardiol. Angiol. 2021. [Google Scholar] [CrossRef]
- Pelliccia, A.; Sharma, S.; Gati, S.; Bäck, M.; Börjesson, M.; Caselli, S.; Collet, J.P.; Corrado, D.; Drezner, J.A.; Halle, M.; et al. 2020 ESC Guidelines on Sports Cardiology and Exercise in Patients with Cardiovascular Disease. Rev. Esp. Cardiol. (Engl. Ed.) 2021, 74, 545. [Google Scholar] [CrossRef]
- Pelliccia, A.; Solberg, E.E.; Papadakis, M.; Adami, P.E.; Biffi, A.; Caselli, S.; La Gerche, A.; Niebauer, J.; Pressler, A.; Schmied, C.M.; et al. Recommendations for participation in competitive and leisure time sport in athletes with cardiomyopathies, myocarditis, and pericarditis: Position statement of the Sport Cardiology Section of the European Association of Preventive Cardiology (EAPC). Eur. Heart J. 2019, 40, 19–33. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Definite Diagnosis of Myocarditis Based on Endomyocardial Biopsy | |
|---|---|
| Myocarditis |
|
| Infective myocarditis |
|
| Myocarditis temporarily associated with infective agent |
|
| Immune-mediated myocarditis |
|
| Autoimmune myocarditis |
|
| Clinically suspected myocarditis |
|
| Inflammatory cardiomyopathy |
|
| Clinical Presentation and Diagnostic Tests | Method/Characteristic | Recommendation | ||
|---|---|---|---|---|
| Acute Cardiac Signs/Symptoms | Chronic Cardiac Signs/Symptoms | Follow-Up | ||
| Diagnosis of clinically suspected myocarditis: new unexplained signs/symptoms and ≥1 non-invasive test being positive from diagnostic categories (ECG, troponin(s), cardiac imaging (echo/CMR), tissue characterization), if patient is asymptomatic ≥2 positive non-invasive tests [3] * | ||||
| Evaluation of medical history and physical examination | Low sensitivity and specificity. Mandatory evaluation for:
| ++ | ++ | ++ |
| Coronary angiography (invasive or CT) | Mandatory for exclusion of:
| ++ | ++ | - |
| Laboratory evaluation | Intermediate sensitivity and low specificity. Mandatory evaluation for:
| ++ | ++ | ++ |
| -AHA | Intermediate sensitivity and intermediate specificity. Evaluation valuable for:
| ++ | ++ | ++ |
| ECG | High sensitivity and low specificity. Mandatory evaluation for:
| ++ | ++ | ++ |
| Echocardiography | High sensitivity and low specificity. Mandatory evaluation for:
| ++ | ++ | ++ |
| CMR | High sensitivity and intermediate specificity **. Mandatory evaluation for ***:
| ++ | ++ | ++ |
| PET-CT/MR | May be useful when:
| (+) | (+) | (+) |
| Confirmation of myocarditis: clinically suspected myocarditis + EMB | ||||
| EMB | High-intermediate sensitivity and high specificity. Mandatory evaluation for:
May be used for follow-up. | ++ | ++ | ++ |
| Treatment | Recommendation |
|---|---|
| Standard and/or supportive treatment | |
| Standard HF medications (ACE-I/ARNI, beta-blocker, MRA, ivabradine, SGLT2-I, diuretic, etc.) | Management according to the current appropriate guidelines. |
| Therapy of end-stage or acute HF with hemodynamic compromise | Treatment in experienced intensive (cardiac) care unit. Advanced cardio-pulmonary support may be needed as a bridge to heart transplantation or recovery. If possible, referral for a heart transplant/LV assist device implantation should be deferred for at least 3–6 months. |
| Standard antiarrhythmic medications (i.e., amiodarone) | The management of arrhythmias should mainly be supportive, as in myocarditis, arrhythmias often diminish or disappear following the resolution of acute myocardial inflammation. Patients with life-threatening arrhythmias should be referred to experienced centers. |
| Nonsteroidal anti-inflammatory drugs (i.e., ibuprofen) and colchicine | Patients with mild myocarditis and predominant associated pericarditis (pericarditic chest pain, pericardial effusion, high C-reactive protein) with preserved or nearly preserved LV function. Potentially harmful in other groups, but data is lacking. |
| Anticoagulation | Patients with acute/fulminant myocarditis with reduced LVEF until resolution of the acute inflammatory phase may require anticoagulation. Patients with intracardiac thrombosis and peripheral embolization, particularly if biopsy-proven eosinophilic myocarditis. |
| Catheter ablation | No indication in acute myocarditis. If necessary, it may be considered in selected patients with drug-refractory or scar-related arrhythmias or arrhythmic storms (i.e., in giant cell myocarditis). |
| ICD/CRT | Indications for ICD/CRT implantation should be evaluated individually; however, urgent ICD implantation in primary SCD prevention is not recommended for patients with recent-onset myocarditis. The decision regarding ICD/CRT implantation should be deferred for at least 3–6 months. A wearable cardioverter defibrillator can provide protection as a bridge to ICD or transplant decision, or to recovery after immunosuppressive therapy, particularly in patients with high arrhythmic risk and/or severe left ventricular dysfunction. |
| Disease-specific treatment | |
| Withdrawal of potential triggering factors (i.e., clozapine, immune-checkpoint inhibitors) | Myocardial damage induced by toxic substances or drugs may progress if treatment is not stopped immediately. |
| Anti-infectious treatment | Therapy (anti-viral, antibiotics, antifungal, antiparasitic) directed against specific infectious agents (i.e., HIV, HHV6, Parvovirus B19, Borrelia). |
| Immunosuppressive treatment in specific infectious-negative forms | Recommended for immune-mediated forms confirmed with EMB (and AHA if available).
|
| Use of the safety checklist is intended to rule out potential general and individual risks related to immunosuppressive therapy. |
| Before starting Patients who are candidates to immunosuppressive therapy should be screened for: |
|
| During treatment |
|
| Factors Affecting the Resumption of Training |
|---|
| Relief of symptoms |
| Normalization of LV systolic function on echocardiography and CMR |
| Normal troponin and biomarkers of inflammation |
Absence of:
|
| Good clinical status and functional capacity |
| Patient Group | Individuals with Presumed or Biopsy-Proven Healed Myocarditis |
|---|---|
| Aim of the test | For routine control evaluation, in order to assess the risk of exercise-related SCD |
| Recommended modalities |
|
| When/how often | At 3–6 months after the acute phase of the disease and then annually |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tymińska, A.; Ozierański, K.; Skwarek, A.; Kapłon-Cieślicka, A.; Baritussio, A.; Grabowski, M.; Marcolongo, R.; Caforio, A.L. Personalized Management of Myocarditis and Inflammatory Cardiomyopathy in Clinical Practice. J. Pers. Med. 2022, 12, 183. https://doi.org/10.3390/jpm12020183
Tymińska A, Ozierański K, Skwarek A, Kapłon-Cieślicka A, Baritussio A, Grabowski M, Marcolongo R, Caforio AL. Personalized Management of Myocarditis and Inflammatory Cardiomyopathy in Clinical Practice. Journal of Personalized Medicine. 2022; 12(2):183. https://doi.org/10.3390/jpm12020183
Chicago/Turabian StyleTymińska, Agata, Krzysztof Ozierański, Aleksandra Skwarek, Agnieszka Kapłon-Cieślicka, Anna Baritussio, Marcin Grabowski, Renzo Marcolongo, and Alida LP Caforio. 2022. "Personalized Management of Myocarditis and Inflammatory Cardiomyopathy in Clinical Practice" Journal of Personalized Medicine 12, no. 2: 183. https://doi.org/10.3390/jpm12020183