
The Predictive Role of Systemic Inflammatory Markers in the Development of Acute Kidney Failure and Mortality in Patients with Abdominal Trauma
 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
2.3. Systemic Inflammatory Markers
- −
- MLR = monocytes/lymphocytes
- −
- NLR = neutrophils/lymphocytes
- −
- PLR = platelets/lymphocytes
- −
- SII = (neutrophils × platelets)/lymphocytes
- −
- SIRI = (monocytes × platelets)/lymphocytes
- −
- AISI = (neutrophils × monocytes × platelets)/lymphocytes
2.4. Study Outcomes
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ki, Y.-J.; Jo, Y.-G.; Park, Y.-C.; Kang, W.-S. The Efficacy and Safety of Laparoscopy for Blunt Abdominal Trauma: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 1853. [Google Scholar] [CrossRef]
- Ntundu, S.H.; Herman, A.M.; Kishe, A.; Babu, H.; Jahanpour, O.F.; Msuya, D.; Chugulu, S.G.; Chilonga, K. Patterns and Outcomes of Patients with Abdominal Trauma on Operative Management from Northern Tanzania: A Prospective Single Centre Observational Study. BMC Surg. 2019, 19, 69. [Google Scholar] [CrossRef] [PubMed]
- Gad, M.A.; Saber, A.; Farrag, S.; Shams, M.E.; Ellabban, G.M. Incidence, Patterns, and Factors Predicting Mortality of Abdominal Injuries in Trauma Patients. N. Am. J. Med. Sci. 2012, 4, 129. [Google Scholar] [CrossRef]
- Gönültaş, F.; Kutlutürk, K.; Gok, A.F.K.; Barut, B.; Sahin, T.T.; Yilmaz, S. Analysis of Risk Factors of Mortality in Abdominal Trauma. Turk. J. Trauma Emerg. Surg. 2020, 26, 43–49. [Google Scholar] [CrossRef]
- Parra-Romero, G.; Contreras-Cantero, G.; Orozco-Guibaldo, D.; Domínguez-Estrada, A.; de Mercado-Martín del Campo, J.J.; Bravo-Cuéllar, L. Trauma Abdominal: Experiencia de 4961 Casos En El Occidente de México. Cir. Cir. 2019, 87, 183–189. [Google Scholar] [CrossRef]
- Pekkari, P.; Bylund, P.-O.; Lindgren, H.; Öman, M. Abdominal Injuries in a Low Trauma Volume Hospital—A Descriptive Study from Northern Sweden. Scand. J. Trauma Resusc. Emerg. Med. 2014, 22, 48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrah, N.; Cameron, P.; Gabbe, B.; Fitzgerald, M.; Martin, K.; Beck, B. Trends in the Nature and Management of Serious Abdominal Trauma. World J. Surg. 2019, 43, 1216–1225. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.; Caldwell, E.; D’Amours, S.; Jalaludin, B.; Sugrue, M. Abdominal Trauma: A Disease in Evolution. ANZ J. Surg. 2005, 75, 790–794. [Google Scholar] [CrossRef] [PubMed]
- Raza, M.; Abbas, Y.; Devi, V.; Prasad, K.V.S.; Rizk, K.N.; Nair, P.P. Non Operative Management of Abdominal Trauma—A 10 Years Review. World J. Emerg. Surg. 2013, 8, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Menyar, A.; Abdelrahman, H.; Al-Hassani, A.; Peralta, R.; AbdelAziz, H.; Latifi, R.; Al-Thani, H. Single Versus Multiple Solid Organ Injuries Following Blunt Abdominal Trauma. World J. Surg. 2017, 41, 2689–2696. [Google Scholar] [CrossRef]
- García, I.C.; Villalba, J.S.; Iovino, D.; Franchi, C.; Iori, V.; Pettinato, G.; Inversini, D.; Amico, F.; Ietto, G. Liver Trauma: Until When We Have to Delay Surgery? A Review. Life 2022, 12, 694. [Google Scholar] [CrossRef] [PubMed]
- Qureshi, A.I.; Huang, W.; Lobanova, I.; Hanley, D.F.; Hsu, C.Y.; Malhotra, K.; Steiner, T.; Suarez, J.I.; Toyoda, K.; Yamamoto, H.; et al. Systolic Blood Pressure Reduction and Acute Kidney Injury in Intracerebral Hemorrhage. Stroke 2020, 51, 3030–3038. [Google Scholar] [CrossRef] [PubMed]
- Jalal, D.I.; Chonchol, M.; Targher, G. Disorders of Hemostasis Associated with Chronic Kidney Disease. Semin. Thromb. Hemost. 2010, 36, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Hoste, E.A.J.; Schurgers, M. Epidemiology of Acute Kidney Injury: How Big Is the Problem? Crit. Care Med. 2008, 36, S146–S151. [Google Scholar] [CrossRef] [PubMed]
- Awad, A.S.; Rouse, M.; Huang, L.; Vergis, A.L.; Reutershan, J.; Cathro, H.P.; Linden, J.; Okusa, M.D. Compartmentalization of Neutrophils in the Kidney and Lung Following Acute Ischemic Kidney Injury. Kidney Int. 2009, 75, 689–698. [Google Scholar] [CrossRef] [Green Version]
- Ávila Martínez, R.J.; Hernández Voth, A.; Marrón Fernández, C.; Hermoso Alarza, F.; Martínez Serna, I.; Mariscal de Alba, A.; Zuluaga Bedoya, M.; Trujillo, M.D.; Meneses Pardo, J.C.; Díaz Hellin, V.; et al. Evolution and Complications of Chest Trauma. Arch. Bronconeumol. 2013, 49, 177–180. [Google Scholar] [CrossRef] [PubMed]
- Letteri, J.M. Post Traumatic Acute Renal Failure. In Acute Renal Failure: Clinical and Experimental; Amerio, A., Coratelli, P., Campese, V.M., Massry, S.G., Eds.; Advances in Experimental Medicine and Biology; Springer: Boston, MA, USA, 1987; pp. 211–218. ISBN 978-1-4684-8240-9. [Google Scholar]
- Stene, J.K. Renal Failure in the Trauma Patient. Crit. Care Clin. 1990, 6, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Halmaciu, I.; Arbănași, E.M.; Kaller, R.; Mureșan, A.V.; Arbănași, E.M.; Bacalbasa, N.; Suciu, B.A.; Cojocaru, I.I.; Runcan, A.I.; Grosu, F.; et al. Chest CT Severity Score and Systemic Inflammatory Biomarkers as Predictors of the Need for Invasive Mechanical Ventilation and of COVID-19 Patients’ Mortality. Diagnostics 2022, 12, 2089. [Google Scholar] [CrossRef]
- Arbănași, E.M.; Halmaciu, I.; Kaller, R.; Mureșan, A.V.; Arbănași, E.M.; Suciu, B.A.; Coșarcă, C.M.; Cojocaru, I.I.; Melinte, R.M.; Russu, E. Systemic Inflammatory Biomarkers and Chest CT Findings as Predictors of Acute Limb Ischemia Risk, Intensive Care Unit Admission, and Mortality in COVID-19 Patients. Diagnostics 2022, 12, 2379. [Google Scholar] [CrossRef]
- Kaller, R.; Arbănași, E.M.; Mureșan, A.V.; Voidăzan, S.; Arbănași, E.M.; Horváth, E.; Suciu, B.A.; Hosu, I.; Halmaciu, I.; Brinzaniuc, K.; et al. The Predictive Value of Systemic Inflammatory Markers, the Prognostic Nutritional Index, and Measured Vessels’ Diameters in Arteriovenous Fistula Maturation Failure. Life 2022, 12, 1447. [Google Scholar] [CrossRef]
- Mureșan, A.V.; Hălmaciu, I.; Arbănași, E.M.; Kaller, R.; Arbănași, E.M.; Budișcă, O.A.; Melinte, R.M.; Vunvulea, V.; Filep, R.C.; Mărginean, L.; et al. Prognostic Nutritional Index, Controlling Nutritional Status (CONUT) Score, and Inflammatory Biomarkers as Predictors of Deep Vein Thrombosis, Acute Pulmonary Embolism, and Mortality in COVID-19 Patients. Diagnostics 2022, 12, 2757. [Google Scholar] [CrossRef] [PubMed]
- Shao, B.; Liu, X.; Li, H.; Song, G.; Di, L.; Jiang, H.; Yan, Y.; Zhang, R.; Ran, R.; Zhang, J.; et al. Prognostic Value of Pretreatment Neutrophil-to-Lymphocyte Ratio in HER2-Positive Metastatic Breast Cancer. Curr. Oncol. 2022, 29, 6154–6166. [Google Scholar] [CrossRef] [PubMed]
- Arbănași, E.M.; Mureșan, A.V.; Coșarcă, C.M.; Kaller, R.; Bud, T.I.; Hosu, I.; Voidăzan, S.T.; Arbănași, E.M.; Russu, E. Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio Impact on Predicting Outcomes in Patients with Acute Limb Ischemia. Life 2022, 12, 822. [Google Scholar] [CrossRef] [PubMed]
- Melinte, R.M.; Arbănași, E.M.; Blesneac, A.; Zolog, D.N.; Kaller, R.; Mureșan, A.V.; Arbănași, E.M.; Melinte, I.M.; Niculescu, R.; Russu, E. Inflammatory Biomarkers as Prognostic Factors of Acute Deep Vein Thrombosis Following the Total Knee Arthroplasty. Medicina 2022, 58, 1502. [Google Scholar] [CrossRef] [PubMed]
- Russu, E.; Mureșan, A.V.; Arbănași, E.M.; Kaller, R.; Hosu, I.; Voidăzan, S.; Arbănași, E.M.; Coșarcă, C.M. The Predictive Role of NLR and PLR in Outcome and Patency of Lower Limb Revascularization in Patients with Femoropopliteal Disease. J. Clin. Med. 2022, 11, 2620. [Google Scholar] [CrossRef] [PubMed]
- Arbănași, E.M.; Mureșan, A.V.; Arbănași, E.M.; Kaller, R.; Cojocaru, I.I.; Coșarcă, C.M.; Russu, E. The Neutrophil-to-Lymphocyte Ratio’s Predictive Utility in Acute Pulmonary Embolism: Systematic Review. J. Cardiovasc. Emergencies 2022, 8, 25–30. [Google Scholar] [CrossRef]
- Niculescu, R.; Russu, E.; Arbănași, E.M.; Kaller, R.; Arbănași, E.M.; Melinte, R.M.; Coșarcă, C.M.; Cocuz, I.G.; Sabău, A.H.; Tinca, A.C.; et al. Carotid Plaque Features and Inflammatory Biomarkers as Predictors of Restenosis and Mortality Following Carotid Endarterectomy. Int. J. Environ. Res. Public. Health 2022, 19, 13934. [Google Scholar] [CrossRef]
- Mureșan, A.V.; Russu, E.; Arbănași, E.M.; Kaller, R.; Hosu, I.; Arbănași, E.M.; Voidăzan, S.T. The Predictive Value of NLR, MLR, and PLR in the Outcome of End-Stage Kidney Disease Patients. Biomedicines 2022, 10, 1272. [Google Scholar] [CrossRef]
- Halmaciu, I.; Suciu, B.A.; Vunvulea, V.; Muresan, M.G.; Scarlat, F.C.; Molnar, C.; Bacalbasa, N.; Brinzaniuc, K.; Voidazan, S. The Importance of Neutrophil to Lymphocyte Ratio and Platelet to Lymphocyte Ratio in Predicting the Appearance of the Rectal Stenosis or Rectal Obstruction in Patients with Rectal Adenocarcinomas. Rev. Chim. 2020, 71, 239–247. [Google Scholar] [CrossRef]
- Festa, E.; Ascione, T.; Bernasconi, A.; Di Gennaro, D.; Basso, M.A.; Guarino, A.; Balato, G. Diagnostic Performance of Neutrophil to Lymphocyte Ratio, Monocyte to Lymphocyte Ratio, Platelet to Lymphocyte Ratio, and Platelet to Mean Platelet Volume Ratio in Periprosthetic Hip and Knee Infections: A Systematic Review and Meta-Analysis. Diagnostics 2022, 12, 2033. [Google Scholar] [CrossRef]
- Rau, C.-S.; Wu, S.-C.; Tsai, C.-H.; Chou, S.-E.; Su, W.-T.; Hsu, S.-Y.; Hsieh, C.-H. Association of White Blood Cell Subtypes and Derived Ratios with a Mortality Outcome in Adult Patients with Polytrauma. Healthcare 2022, 10, 1384. [Google Scholar] [CrossRef] [PubMed]
- Soehnlein, O. Multiple Roles for Neutrophils in Atherosclerosis. Circ. Res. 2012, 110, 875–888. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacIsaac, R.J.; Ekinci, E.I.; Jerums, G. Markers of and Risk Factors for the Development and Progression of Diabetic Kidney Disease. Am. J. Kidney Dis. 2014, 63, S39–S62. [Google Scholar] [CrossRef]
- Bi, J.-B.; Zhang, J.; Ren, Y.-F.; Du, Z.-Q.; Wu, Z.; Lv, Y.; Wu, R.-Q. Neutrophil-to-Lymphocyte Ratio Predicts Acute Kidney Injury Occurrence after Gastrointestinal and Hepatobiliary Surgery. World J. Gastrointest. Surg. 2020, 12, 326–335. [Google Scholar] [CrossRef] [PubMed]
- Guangqing, Z.; Liwei, C.; Fei, L.; Jianshe, Z.; Guang, Z.; Yan, Z.; Jianjun, C.; Ming, T.; Hao, C.; Wei, L. Predictive Value of Neutrophil to Lymphocyte Ratio on Acute Kidney Injury after On-Pump Coronary Artery Bypass: A Retrospective, Single-Center Study. Gen. Thorac. Cardiovasc. Surg. 2022, 70, 624–633. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.; Chen, L.; Li, B.; Yang, L.; Ouyang, W.; Li, D. Preoperative Neutrophil-Lymphocyte Ratio for Predicting Surgery-Related Acute Kidney Injury in Non-Cardiac Surgery Patients under General Anaesthesia: A Retrospective Cohort Study. PLoS ONE 2022, 17, e0270066. [Google Scholar] [CrossRef]
- Ntalouka, M.P.; Nana, P.; Kouvelos, G.N.; Stamoulis, K.; Spanos, K.; Giannoukas, A.; Matsagkas, M.; Arnaoutoglou, E. Association of Neutrophil–Lymphocyte and Platelet–Lymphocyte Ratio with Adverse Events in Endovascular Repair for Abdominal Aortic Aneurysm. J. Clin. Med. 2021, 10, 1083. [Google Scholar] [CrossRef]
- Khwaja, A. KDIGO Clinical Practice Guidelines for Acute Kidney Injury. Nephron Clin. Pract. 2012, 120, c179–c184. [Google Scholar] [CrossRef]
- Søvik, S.; Isachsen, M.S.; Nordhuus, K.M.; Tveiten, C.K.; Eken, T.; Sunde, K.; Brurberg, K.G.; Beitland, S. Acute Kidney Injury in Trauma Patients Admitted to the ICU: A Systematic Review and Meta-Analysis. Intensive Care Med. 2019, 45, 407–419. [Google Scholar] [CrossRef] [Green Version]
- Haines, R.W.; Fowler, A.J.; Kirwan, C.J.; Prowle, J.R. The Incidence and Associations of Acute Kidney Injury in Trauma Patients Admitted to Critical Care: A Systematic Review and Meta-Analysis. J. Trauma Acute Care Surg. 2019, 86, 141–147. [Google Scholar] [CrossRef]
- Ishani, A.; Nelson, D.; Clothier, B.; Schult, T.; Nugent, S.; Greer, N.; Slinin, Y.; Ensrud, K.E. The Magnitude of Acute Serum Creatinine Increase after Cardiac Surgery and the Risk of Chronic Kidney Disease, Progression of Kidney Disease, and Death. Arch. Intern. Med. 2011, 171, 226–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bihorac, A.; Delano, M.J.; Schold, J.D.; Lopez, M.C.; Nathens, A.B.; Maier, R.V.; Layon, A.J.; Baker, H.V.; Moldawer, L.L. Incidence, Clinical Predictors, Genomics, and Outcome of Acute Kidney Injury among Trauma Patients. Ann. Surg. 2010, 252, 158–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaw, A. Update on Acute Kidney Injury after Cardiac Surgery. J. Thorac. Cardiovasc. Surg. 2012, 143, 676–681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grams, M.E.; Sang, Y.; Coresh, J.; Ballew, S.; Matsushita, K.; Molnar, M.Z.; Szabo, Z.; Kalantar-Zadeh, K.; Kovesdy, C.P. Acute Kidney Injury After Major Surgery: A Retrospective Analysis of Veterans Health Administration Data. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2016, 67, 872–880. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borthwick, E.; Ferguson, A. Perioperative Acute Kidney Injury: Risk Factors, Recognition, Management, and Outcomes. BMJ 2010, 341, c3365. [Google Scholar] [CrossRef] [Green Version]
- Bihorac, A.; Yavas, S.; Subbiah, S.; Hobson, C.E.; Schold, J.D.; Gabrielli, A.; Layon, A.J.; Segal, M.S. Long-Term Risk of Mortality and Acute Kidney Injury during Hospitalization after Major Surgery. Ann. Surg. 2009, 249, 851–858. [Google Scholar] [CrossRef]
- Hobson, C.E.; Yavas, S.; Segal, M.S.; Schold, J.D.; Tribble, C.G.; Layon, A.J.; Bihorac, A. Acute Kidney Injury Is Associated with Increased Long-Term Mortality after Cardiothoracic Surgery. Circulation 2009, 119, 2444–2453. [Google Scholar] [CrossRef] [Green Version]
- Younan, D.; Richman, J.; Zaky, A.; Pittet, J.-F. An Increasing Neutrophil-to-Lymphocyte Ratio Trajectory Predicts Organ Failure in Critically-Ill Male Trauma Patients. An Exploratory Study. Healthcare 2019, 7, 42. [Google Scholar] [CrossRef] [Green Version]
- Ke, R.-T.; Rau, C.-S.; Hsieh, T.-M.; Chou, S.-E.; Su, W.-T.; Hsu, S.-Y.; Hsieh, C.-H.; Liu, H.-T. Association of Platelets and White Blood Cells Subtypes with Trauma Patients’ Mortality Outcome in the Intensive Care Unit. Healthcare 2021, 9, 942. [Google Scholar] [CrossRef]
- Duchesne, J.C.; Tatum, D.; Jones, G.; Davis, B.; Robledo, R.; DeMoya, M.; O’Keeffe, T.; Ferrada, P.; Jacome, T.; Schroll, R.; et al. Multi-Institutional Analysis of Neutrophil-to-Lymphocyte Ratio (NLR) in Patients with Severe Hemorrhage: A New Mortality Predictor Value. J. Trauma Acute Care Surg. 2017, 83, 888–893. [Google Scholar] [CrossRef]
- Qiu, Y.; Fitzgerald, M.; Mitra, B. Association of the Neutrophil–Lymphocyte Ratio to Patient Outcomes after Trauma: A Systematic Review. Trauma 2022, 24, 195–203. [Google Scholar] [CrossRef]
- Li, W.; Deng, W. Platelet-to-Lymphocyte Ratio Predicts Short-Term Mortality in Patients with Moderate to Severe Traumatic Brain Injury. Sci. Rep. 2022, 12, 13976. [Google Scholar] [CrossRef] [PubMed]
- Abu Alfeilat, M.; Slotki, I.; Shavit, L. Single Emergency Room Measurement of Neutrophil/Lymphocyte Ratio for Early Detection of Acute Kidney Injury (AKI). Intern. Emerg. Med. 2018, 13, 717–725. [Google Scholar] [CrossRef] [PubMed]
- de Hond, T.A.P.; Ocak, G.; Groeneweg, L.; Oosterheert, J.J.; Haitjema, S.; Khairoun, M.; Kaasjager, K.A.H. Hematological Ratios Are Associated with Acute Kidney Injury and Mortality in Patients That Present with Suspected Infection at the Emergency Department. J. Clin. Med. 2022, 11, 1017. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | All Patients N = 364 | Survivors N = 283 | Non-Survivors N = 81 | p Value (OR; CI 95%) |
|---|---|---|---|---|
| Age mean ± SD (MIN–MAX) | 42.83 ± 18.24 (18–89) | 41.60 ± 17.61 (18–89) | 45.80 ± 20.53 (20–88) | 0.02 |
| Male/Female SEX NO. (%) | 258 (70.88%) 106 (29.12%) | 198 (69.96%) 85 (30.04%) | 60 (74.07%) 21 (25.93%) | 0.47 (1.22; 0.70–2.14) |
| Comorbidities and Risk Factors | ||||
| AH, no. (%) | 64 (17.58%) | 47 (16.60%) | 17 (20.98%) | 0.36 (1.33; 0.71–2.7) |
| IHD, no. (%) | 48 (13.18%) | 30 (10.60%) | 18 (22.22%) | 0.007 (2.40; 1.26–4.59) |
| AF, no. (%) | 14 (3.84%) | 8 (2.82%) | 6 (7.40%) | 0.06 (2.75; 0.92–8.17) |
| CHF, no. (%) | 24 (6.59%) | 17 (6.007%) | 7 (8.64%) | 0.40 (148; 0.59–3.70) |
| MI, no. (%) | 12 (3.29%) | 4 (1.41%) | 8 (9.87%) | 0.002 (6.11; 1.94–19.24) |
| DM, no. (%) | 38 (10.43%) | 27 (9.54%) | 11 (13.58%) | 0.29 (1.48; 0.70–3.15) |
| COPD, no. (%) | 10 (2.74%) | 8 (2.82%) | 2 (2.46%) | 0.86 (0.87; 0.18–4.18) |
| PAD, no. (%) | 8 (2.19%) | 3 (1.06%) | 5 (6.12%) | 0.01 (6.14; 1.43–26.27) |
| CKD, no. (%) | 20 (5.49%) | 11 (3.88%) | 9 (11.11%) | 0.01 (2.55; 1.46–4.46) |
| Tobacco, no. (%) | 16 (4.39%) | 6 (2.12%) | 10 (12.34%) | 0.0004 (6.50; 2.28–18.49) |
| Obesity, no. (%) | 17 (4.67%) | 5 (1.76%) | 12 (14.81%) | <0.0001 (9.66; 3.29–28.36) |
| Injured Organs | ||||
| Liver, no. (%) | 130 (35.71%) | 103 (36.39%) | 27 (33.33%) | 0.61 (0.87; 0.51–1.47) |
| Spleen, no. (%) | 201 (55.21%) | 160 (56.53%) | 41 (50.61%) | 0.34 (0.78; 0.48–1.29) |
| Pancreas, no. (%) | 18 (4.94%) | 14 (4.94%) | 4 (4.93%) | 0.99 (0.99; 0.31–3.12) |
| Large bowel, no. (%) | 23 (6.31%) | 17 (6.007%) | 6 (7.40%) | 0.64 (1.25; 0.47–3.28) |
| Small bowel, no. (%) | 25 (6.86%) | 20 (7.06%) | 5 (6.17%) | 0.77 (0.86; 0.31–2.38) |
| Kidney, no. (%) | 23 (6.31%) | 12 (4.24%) | 11 (13.58%) | 0.003 (3.54; 1.50–8.38) |
| Hemoperitoneum, no. (%) | 191 (52.47%) | 138 (48.76%) | 53 (65.43%) | 0.008 (1.98; 1.18–3.32) |
| Laboratory Data | ||||
| Hemoglobin g/dL median (Q1–Q3) | 11.91 (10.47–13.36) | 12.2 (10.5–13.55) | 11.50 (10.4–12.7) | 0.03 |
| Hematocrit % median (Q1–Q3) | 35.9 (31.4–39.98) | 36.6 (31.36–40.66) | 33.86 (31.6–37.2) | 0.01 |
| Glucose mg/dL median (Q1–Q3) | 109 (93–140.75) | 105 (92.5–132.9) | 143 (104.25–170.5) | 0.02 |
| Sodium median (Q1–Q3) | 138 (135–141) | 138 (135–141) | 138 (135–140.7) | 0.35 |
| Potassium median (Q1–Q3) | 4.25 (3.74–5.0) | 4.21 (3.72–5.19) | 4.36 (3.9–4.74) | 0.37 |
| Uric acid median (Q1–Q3) | 6.45 (5.1–8.2) | 6.2 (5.0–7.95) | 6.90 (5.5–8.6) | 0.02 |
| Bun mg/dL median (Q1–Q3) | 67 (38.47–194.42) | 56.5 (35.85–163.22) | 145.5 (51–247.98) | <0.0001 |
| Creatinine mg/dL median (Q1–Q3) | 1.55 (0.86–6.1) | 1.22 (0.84–5.68) | 4.41 (1.36–9.57) | <0.0001 |
| GFR (mL/min/1.73 m2) median (Q1–Q3) | 74.17 (56.02–90.5) | 76.72 (57.84–92.56) | 66.52 (54.74–85.15) | 0.004 |
| Neutrophils ×10³/µL median (Q1–Q3) | 8.24 (5.58–12.98) | 7.43 (5.25–11.06) | 12.94 (8.03–17.25) | <0.0001 |
| Lymphocytes ×10³/µL median (Q1–Q3) | 1.96 (1.47–2.66) | 2.13 (1.68–2.88) | 1.26 (0.98–1.89) | <0.0001 |
| Monocyte ×10³/µL median (Q1–Q3) | 0.9 (0.61–1.62) | 0.8 (0.59–1.38) | 1.29 (0.73–2.23) | <0.0001 |
| PLT ×10³/µL median (Q1–Q3) | 245.5 (200.6–303.85) | 238.7 (193.15–300.4) | 272 (222.7–316.1) | 0.001 |
| MLR, median (Q1–Q3) | 4.15 (2.39–7.31) | 3.36 (2.17–5.62) | 9.79 (6.06–13.96) | <0.0001 |
| NLR, median (Q1–Q3) | 0.47 (0.30–0.94) | 0.40 (0.28–0.68) | 0.98 (0.67–1.80) | <0.0001 |
| PLR, median (Q1–Q3) | 120.03 (91.08–168.92) | 110.66 (82.79–147.27) | 224.05 (166.67–288.37) | <0.0001 |
| SII, median (Q1–Q3) | 1013.22 (583.19–1750.97) | 757.46 (532.12–1392.7) | 2725.15 (1697.4–3840) | <0.0001 |
| SIRI, median (Q1–Q3) | 4.96 (1.89–11.32) | 3.44 (1.62–7.54) | 15.56 (7.92–23.74) | <0.0001 |
| AISI, median (Q1–Q3) | 1163.85 (461.48–2874.06) | 849.73 (377.96–1767.38) | 3956.66 (2561.89–6192.3) | <0.0001 |
| Outcomes | ||||
| AKI, no. (%) | 84 (23.07%) | 27 (9.54%) | 57 (70.37%) | <0.0001 (5.57; 2.77–11.22) |
| AKI + Mortality, no. (%) | 57 (15.65%) | 0 | 57 (70.37%) | <0.0001 (5.57; 2.77–11.22) |
| Length of hospital stay, MEAN ± SD | 9 (7–13) | 9 (6–12) | 10 (7–16) | <0.0001 |
| Length of ICU stay, mean ± SD | 7 (5–8.25) | 6 (5–8) | 8 (7–11) | <0.0001 |
| AKI stage KDIGO | ||||
| 0, no. (%) | 280 (76.92%) | 256 (90.45%) | 24 (29.62%) | <0.0001 |
| I, no. (%) | 26 (7.14%) | 18 (6.36%) | 8 (9.87%) | 0.26 |
| II, no. (%) | 31 (8.51%) | 7 (2.47%) | 24 (29.62%) | <0.0001 |
| III, no. (%) | 27 (7.41%) | 2 (0.7%) | 25 (30.86%) | <0.0001 |
| Variables | Cut-off | AUC | Std. Error | 95% CI | Sensitivity | Specificity | p-Value |
|---|---|---|---|---|---|---|---|
| AKI | |||||||
| NLR | 4.40 | 0.777 | 0.028 | 0.722–0.831 | 79.8% | 64.6% | <0.0001 |
| MLR | 0.51 | 0.744 | 0.030 | 0.685–0.803 | 77.4% | 62.9% | <0.0001 |
| PLR | 158.82 | 0.751 | 0.032 | 0.689–0.813 | 60.7% | 78.9% | <0.0001 |
| SII | 1295.99 | 0.796 | 0.027 | 0.744–0.849 | 75.0% | 69.3% | <0.0001 |
| SIRI | 5.57 | 0.790 | 0.027 | 0.738–0.843 | 78.6% | 64.3% | <0.0001 |
| AISI | 1657.92 | 0.802 | 0.026 | 0.750–0.853 | 72.6% | 69.6% | <0.0001 |
| Mortality | |||||||
| NLR | 4.98 | 0.870 | 0.021 | 0.828–0.911 | 80.2% | 73.1% | <0.0001 |
| MLR | 0.57 | 0.800 | 0.025 | 0.752–0.848 | 82.7% | 70.3% | <0.0001 |
| PLR | 161.07 | 0.865 | 0.025 | 0.816–0.914 | 76.5% | 85.2% | <0.0001 |
| SII | 1559.39 | 0.893 | 0.020 | 0.853–0.933 | 80.2% | 81.6% | <0.0001 |
| SIRI | 7.85 | 0.846 | 0.024 | 0.798–0.894 | 75.3% | 76% | <0.0001 |
| AISI | 2131.74 | 0.859 | 0.023 | 0.814–0.905 | 79% | 79.5% | <0.0001 |
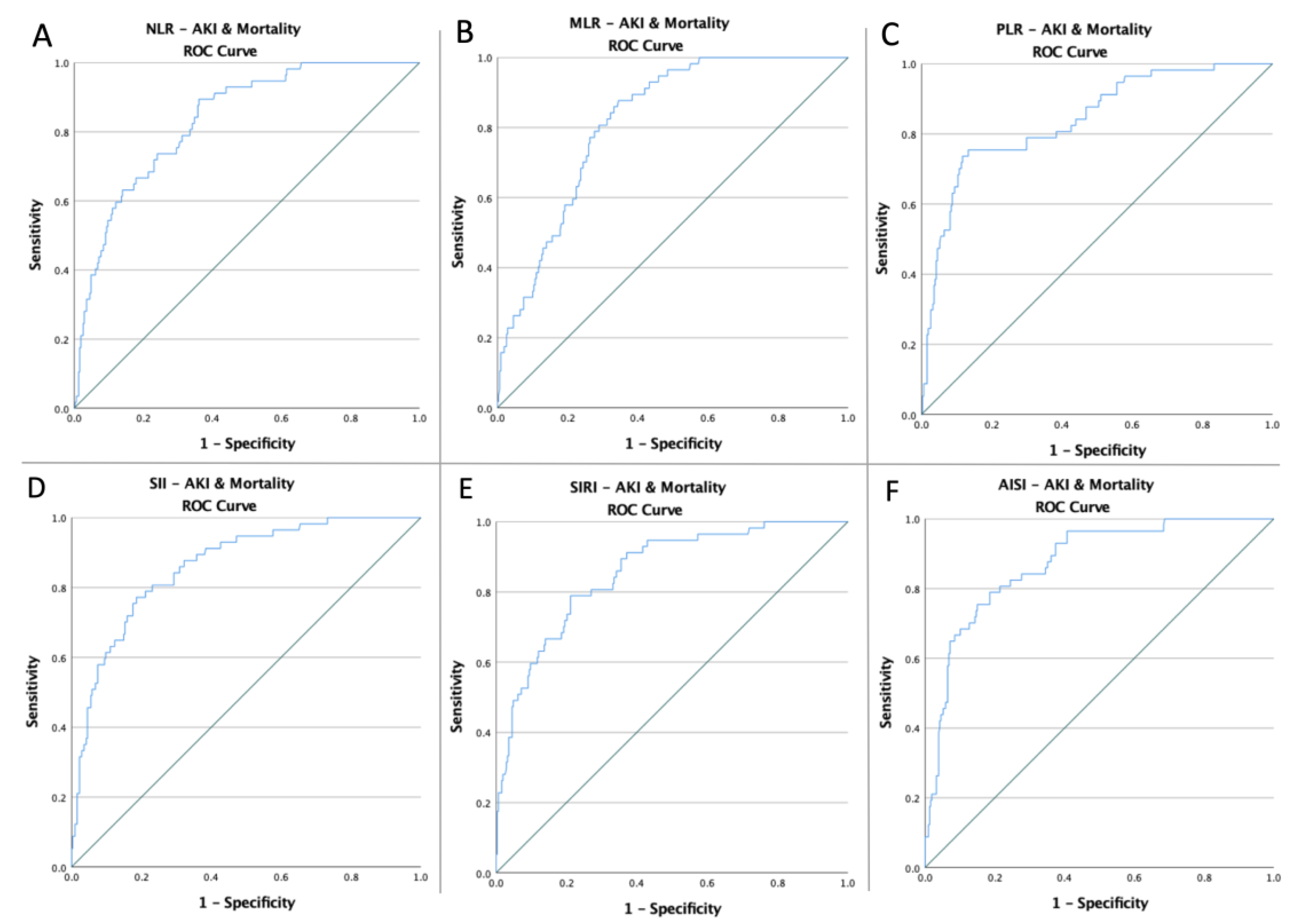
| AKI and Mortality | |||||||
| NLR | 4.49 | 0.835 | 0.026 | 0.783–0.886 | 89.5% | 63.8% | <0.0001 |
| MLR | 0.67 | 0.817 | 0.025 | 0.768–0.865 | 80.7% | 71% | <0.0001 |
| PLR | 176.14 | 0.841 | 0.029 | 0.783–0.898 | 75.4% | 86.6% | <0.0001 |
| SII | 1559.39 | 0.862 | 0.025 | 0.813–0.911 | 80.7% | 76.9% | <0.0001 |
| SIRI | 10.08 | 0.855 | 0.026 | 0.804–0.906 | 78.9% | 78.8% | <0.0001 |
| AISI | 2530.35 | 0.873 | 0.024 | 0.827–0.920 | 80.7% | 78.5% | <0.0001 |
| AKI | Mortality | AKI and Mortality | |
|---|---|---|---|
| Low-NLR vs. high-NLR | 17/197 (8.63%) vs. 67/167 (40.12%) p < 0.0001 | 16/223 (7.17%) vs. 65/141 (46.10%) p < 0.0001 | 6/202 (2.97%) vs. 51/162 (31.48%) p < 0.0001 |
| Low-MLR vs. high-MLR | 19/195 (9.74%) vs. 65/169 (38.46%) p < 0.0001 | 14/212 (6.60%) vs. 67/152 (44.08%) p < 0.0001 | 11/228 (4.82%) vs. 46/136 (33.82%) p < 0.0001 |
| Low-PLR vs. high-PLR | 33/254 (12.9%) vs. 51/110 (46.36%) p < 0.0001 | 19/260 (7.31%) vs. 62/104 (59.62%) p < 0.0001 | 14/280 (5.00%) vs. 43/84 (51.19%) p < 0.0001 |
| Low-SII vs. high-SII | 21/215 (9.77%) vs. 63/149 (42.28%) p < 0.0001 | 16/247 (6.48%) vs. 65/117 (55.56%) p < 0.0001 | 16/247 (6.48%) vs. 65/117 (55.56%) p < 0.0001 |
| Low-SIRI vs. high-SIRI | 19/200 (9.50%) vs. 65/164 (39.63%) p < 0.0001 | 20/235 (8.51%) vs. 61/129 (47.29%) p < 0.0001 | 12/254 (4.72%) vs. 45/110 (40.91%) p < 0.0001 |
| Low-AISI vs. high-AISI | 23/218 (10.5%) vs. 61/146 (41.78%) p < 0.0001 | 17/242 (7.02%) vs. 64/122 (52.46%) p < 0.0001 | 11/252 (4.37%) vs. 46/112 (41.07%) p < 0.0001 |
| AKI | Mortality | AKI AND Mortality | |||||||
|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p Value | OR | 95% CI | p Value | OR | 95% CI | p Value | |
| Age > 45 | 1.25 | 0.76–2.05 | 0.36 | 1.55 | 0.94–2.55 | 0.08 | 1.21 | 0.68–2.15 | 0.50 |
| IHD | 1.62 | 0.83–3.16 | 0.15 | 2.41 | 1.26–4.59 | 0.008 | 2.29 | 1.12–4.67 | 0.02 |
| AF | 2.61 | 0.88–7.76 | 0.08 | 2.75 | 0.92–8.17 | 0.06 | 3.18 | 1.02–9.87 | 0.04 |
| MI | 3.51 | 1.10–11.19 | 0.03 | 7.64 | 2.24–26.08 | 0.001 | 5.90 | 1.83–19.01 | 0.003 |
| PAD | 5.84 | 1.36–24.98 | 0.01 | 6.14 | 1.43–26.27 | 0.01 | 9.74 | 2.26–24.09 | 0.002 |
| CKD | 2.55 | 1.46–4.46 | <0.001 | 3.09 | 1.23–7.74 | 0.01 | 3.21 | 1.97–6.50 | 0.001 |
| Tobacco | 2.73 | 0.98–7.58 | 0.053 | 6.50 | 2.28–18.49 | <0.001 | 3.49 | 1.21–10.03 | 0.02 |
| Obesity | 9.16 | 3.12–26.86 | <0.001 | 9.67 | 3.29–28.36 | <0.001 | 9.11 | 3.30–25.12 | <0.001 |
| Kidney injury | 2.77 | 1.17–5.68 | 0.02 | 3.54 | 1.50–8.38 | 0.004 | 3.17 | 1.28–7.89 | 0.01 |
| Hemoperitoneum | 1.27 | 0.78–2.08 | 0.32 | 1.98 | 1.19–3.32 | 0.009 | 2.20 | 1.21–4.03 | 0.01 |
| high-NLR | 7.09 | 3.94–12.74 | <0.001 | 11.06 | 6.03–20.30 | <0.001 | 15.09 | 6.24–36.09 | <0.001 |
| high-MLR | 5.78 | 3.28–10.19 | <0.001 | 11.14 | 5.94–20.92 | <0.001 | 10.08 | 4.99–20.35 | <0.001 |
| high-PLR | 5.89 | 3.42–9.77 | <0.001 | 18.72 | 10.17–34.44 | <0.001 | 19.92 | 10.02–39.60 | <0.001 |
| high-SII | 6.76 | 3.88–11.79 | <0.001 | 18.04 | 9.66–33.69 | <0.001 | 13.90 | 6.83–28.25 | <0.001 |
| high-SIRI | 6.25 | 3.54–11.02 | <0.001 | 9.64 | 5.43–17.11 | <0.001 | 13.96 | 6.98–27.92 | <0.001 |
| high-AISI | 6.08 | 3.53–10.47 | <0.001 | 14.60 | 7.95–25.81 | <0.001 | 15.27 | 7.49–31.12 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vunvulea, V.; Budișcă, O.A.; Arbănași, E.M.; Mureșan, A.V.; Arbănași, E.M.; Brînzaniuc, K.; Niculescu, R.; Cocuz, I.G.; Ivănescu, A.D.; Hălmaciu, I.; et al. The Predictive Role of Systemic Inflammatory Markers in the Development of Acute Kidney Failure and Mortality in Patients with Abdominal Trauma. J. Pers. Med. 2022, 12, 2045. https://doi.org/10.3390/jpm12122045
Vunvulea V, Budișcă OA, Arbănași EM, Mureșan AV, Arbănași EM, Brînzaniuc K, Niculescu R, Cocuz IG, Ivănescu AD, Hălmaciu I, et al. The Predictive Role of Systemic Inflammatory Markers in the Development of Acute Kidney Failure and Mortality in Patients with Abdominal Trauma. Journal of Personalized Medicine. 2022; 12(12):2045. https://doi.org/10.3390/jpm12122045
Chicago/Turabian StyleVunvulea, Vlad, Ovidiu Aurelian Budișcă, Emil Marian Arbănași, Adrian Vasile Mureșan, Eliza Mihaela Arbănași, Klara Brînzaniuc, Raluca Niculescu, Iuliu Gabriel Cocuz, Adrian Dumitru Ivănescu, Ioana Hălmaciu, and et al. 2022. "The Predictive Role of Systemic Inflammatory Markers in the Development of Acute Kidney Failure and Mortality in Patients with Abdominal Trauma" Journal of Personalized Medicine 12, no. 12: 2045. https://doi.org/10.3390/jpm12122045